
Abstract
Real-time continuous glucose monitoring (RT-CGM) provides real time glucose readings to participants wearing the device. The ability to see changes in glucose has the potential to provide immediate feedback to users on food choices and physical activity. The National Diabetes Prevention Program is currently the only reimbursable intervention for diabetes prevention and weight loss. The purpose of this article is to review the CGM literature on measurements other than Hemoglobin A1c (HbA1c) changes and hypoglycemia and discuss RT-CGM potential use as a behavior modification tool for lifestyle changes and weight reduction in people with prediabetes and type 2 diabetes (T2D).
A literature search from January 2008 to January 2018 was conducted in PUBMED using CGM and T2D or prediabetes in search. Eligible studies were prospective CGM studies which evaluated glycemic control on participants with T2D or prediabetes with duration of study of >8 weeks and was further refined to studies using CGM to promote or highlight a lifestyle change. Studies were excluded if CGM was used primarily to assess glycemic effect after a medication intervention or only used as part of the assessment tool for a behavior change. Out of 761 articles reviewed for CGM in T2D only 4 authors and 5 studies met the criteria. Given limited CGM studies on lifestyle modification both RT and professional/retrospective CGM studies were included. Of note there was only one published pilot study for the prediabetes population with 36 citations reviewed but it did not meet inclusion criteria given HbA1c was not reported.
In the United States, more than 30.3 million people have diabetes and 84.1 million adults have prediabetes. 1 Annual medical costs for persons with diagnosed diabetes average $13 700. 2 Many comprehensive lifestyle intervention programs such as the Diabetes Prevention Program (DPP) 3 and behavior change strategies (alone or in combination) have been used to promote weight loss in obese, high-risk individuals with variable effects. These strategies include motivational interviewing, accountability/self-monitoring programs, food journals,4-6 pedometers,7,8 and mobile phone apps 9 for weight loss.
There is widespread acknowledgment that lifestyle behavior change is critical for weight and glucose regulation. The DPP trial demonstrated that lifestyle changes (diet and physical activity aimed at weight loss) were more effective than metformin in preventing diabetes among those with prediabetes; 3 however, the DPP lifestyle intervention involved frequent visits and coaching over several years, which is costly and labor intensive. More scalable adaptations for community translation, such as a group-based program called Group Lifestyle Balance™ (GLB) have been shown to be effective in community settings. A meta-analysis conducted in 2012 reviewing 28 National DPP translational interventions showed an average weight loss of 4%. However, the attrition rate or drop-out rate was as high as 50% in some programs. The weight loss achieved in these interventions was highly dependent on number of core sessions attended, 10 highlighting the challenges of engaging patients in ongoing weekly group sessions and the need to evaluate alternative, self-directed behavioral change methods to promote weight loss and glycemic managment.
Several studies have demonstrated that encouraging patient engagement enhances self-care behaviors such as healthy eating.11-15 Patients are more likely to engage in healthy behaviors when they are given appropriate tools and are supported by their clinicians. For example, structured self-monitoring of blood glucose (SMBG) by 7-8 fingersticks a day has been shown to improve glycemic control in patients with diabetes by helping them understand glycemic response to food and activity. 15 However, this is nearly impossible to reproduce in a real-world setting because of the inconvenience and discomfort associated with multiple fingersticks. CGM technology previously required multiple daily calibrations but now has advanced to a no-calibration model in both the RT-CGM and newer intermittent CGM or “flash” technology.
Multiple studies have demonstrated that RT-CGM can be used in adults and children with type 1 diabetes (T1D) and result in improvement in HbA1c and/or a reduced frequency of hypoglycemia.16-18 One recent study in T2D using multiple daily insulin injections (MDI) and CGM showed significantly reduced HbA1c, CGM-measured hypoglycemia, CGM-measured hyperglycemia with a high degree of CGM perseverance over 6 months. 19 In none of these studies was there comment on food or exercise changes in these individuals.16-19 In the case of “flash” CGM technology in patients with T2D on MDI therapy for 6 months there was no change in HbA1c but slight improvement in hypoglycemia. Similar to other CGM research the only additional endpoint assessed in this study was patient satisfaction. 20 CGM studies in patients with T2D not on MDI are very limited. Our study showed that intermediate use of RT-CGM serially over 3 months improved HbA1c by average of 1.0% in subjects with T2D on no prandial insulin. 21 Nutrition and activity changes were not measured, but the 3-month HbA1c improvement was sustained for another 9 months without further RT-CGM intervention. 22
There has been little direct examination of RT-CGM or retrospective CGM as a behavior modification/weight loss tool, as most studies have focused on HbA1c changes but available studies are summarized in Table 1. Yoo et al did show that intermittent use (3 days of RT- CGM every month for 12 weeks) produced a significant decrease in calorie consumption, increase in physical activity, improvement of weight, and a 1% decrease in HbA1c in poorly controlled patients with T2D. 23 Allen et al found that the data from a single three-day session of blinded CGM when combined with subsequent counseling and review of the CGM glucose data with the patient resulted in an increase in physical activity and a decrease in HbA1c by 1.2% and BMI by 0.5 kg/m2. 24 A recent small pilot study by Cox et al 25 that focused on glycemic index reduction using RT-CGM and newly diagnosed T2D not on insulin showed decrease in HbA1c by 1% over 3 months. They reported average weight loss of 7.2 kilograms, decreased intake in high glycemic index food, total carbohydrate intake, and increase in fiber. There has been only one community-based study looking at CGM. This study using retrospective CGM with two sessions over 3 months in 181 T2D at 11 health clinics in India showed improvement of HbA1c by 0.6% and noted that in their participants 67.6% made dietary and 48.6% made exercise changes although specifics of these changes were not qualified. 26 A study using RT-CGM in patients with prediabetes showed significant glycemic variability at baseline but did not show decreased glycemic variability or improvement in weight after 6 months, and diet and activity levels were not measured (unpublished data, Vigersky RA 2014 and Warnock A 2016). The reasons for the failure to achieve weight reduction in that study may have been due to the lack of specific lifestyle counseling and/or instructions on use/interpretation of RT-CGM to the subjects. In addition, the rigorous RT-CGM schedule in the protocol (2 weeks of RT-CGM wear on 4 occasions over 3 months) may have been too intensive for patients with prediabetes who do not perform fingerstick blood glucose measurements. Finally, the idea that CGM facilitates self-monitoring behavior has been assessed only in 2 small pilot CGM studies all on exercise. The one pilot RT-CGM study on exercise which included both participants with prediabetes and diabetes did not report HbA1c but not only showed positive changes in body composition and increased fitness but also assessed and showed improved ability for goal setting, self-efficacy to self-monitor, higher attendance, and more registration for additional exercise sessions than those in the standard exercise group. 27 Interestingly, in the second pilot in T2D which attempted to assess CGM as a tool for theory-based behavioral counseling, both groups received CGM and counseling on CGM. However, one group received only diabetes education and the other received additional problem-solving skills. Both groups had improvement in physical activity, HbA1c, and weight but the CGM/problem solving skills group’s results were slightly although not statistically better. 28 These pilots hint at CGM’s potential, highlighting that perhaps CGM does more than record glucose. Further research needs to both assess outcomes such as HbA1c, weight, activity, and nutrition and also how CGM use modifies lifestyle behavior.
Changes in HbA1c, Body Mass Index (BMI), and CGM Intervention for Behavioral Changes.
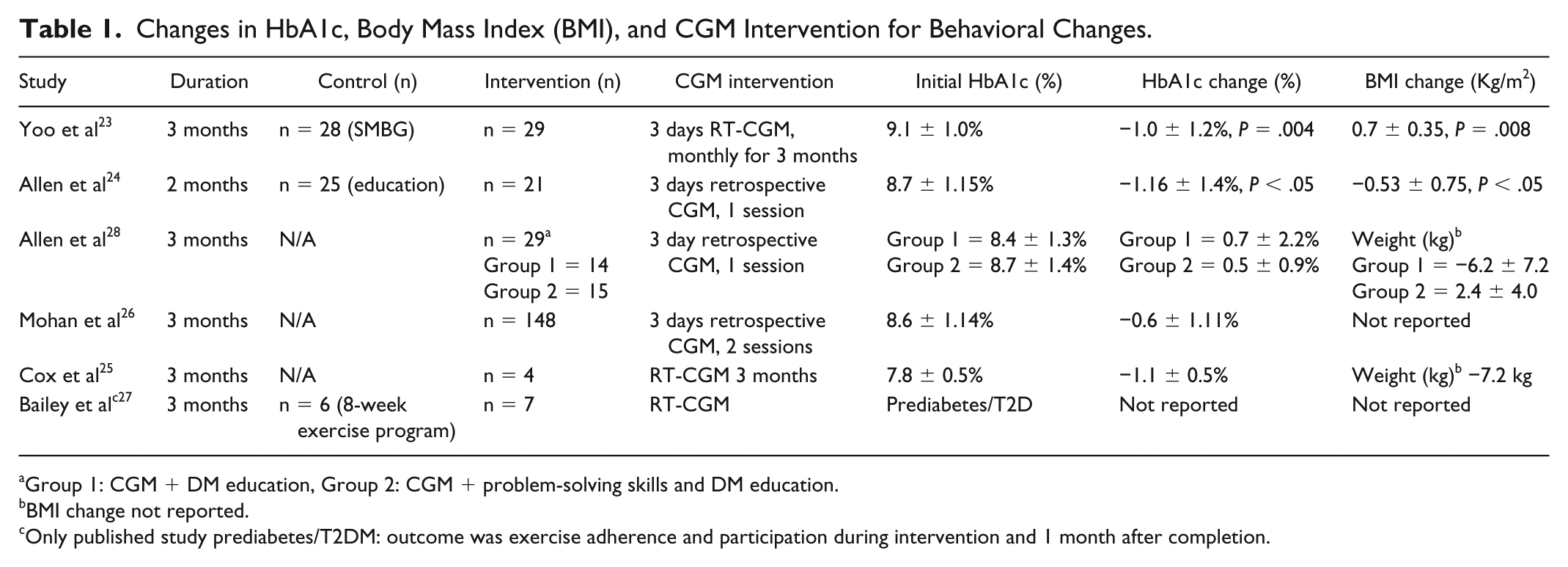
Group 1: CGM + DM education, Group 2: CGM + problem-solving skills and DM education.
BMI change not reported.
Only published study prediabetes/T2DM: outcome was exercise adherence and participation during intervention and 1 month after completion.
Recently the Diabetes Technology Working Group called for “greater investment in trials to provide evidence of CGM value and reliability for all patient groups” and noted the lack of “training available either to providers or users on how to react to the measurement results.” 29 This “value” may be in CGM use as an adjunct for lifestyle changes, specifically nutrition and exercise, which has yet to be well studied. Food intake and activity level affect weight and glycemic control in all types of diabetes and prediabetes; however, as current CGM use is primarily in patients with T1DM, we conducted a survey in 40 patients to evaluate overall perception of CGM in the population currently using this technology. Overall 94.7% reported “a healthier lifestyle” (unpublished data, Al Zaghal E, Ehrhardt NM), highlighting the need for further evaluation of how/if RT-CGM causes behavioral changes.
As shown by the above review, the CGM data is significantly limited on CGM as a behavior modification tool with many clinical questions still unanswered, including ability to aid in weight loss and behavior changes in the patients with all types of diabetes and prediabetes, best technology for lifestyle effect, duration of use, and overall cost. With the limited data available in the T2D population on MDI for the RT-CGM versus “flash” technology, it currently appears RT-CGM maybe be preferred since there was no HbA1c reduction in the recent study in the T2D population on MDI but was in the RT-CGM.19,20 In addition, in our CGM in patients with T2D study, which excluded those on premeal insulin, we saw a reduction in HbA1c so there did seem to be some effect outside of insulin use. Unfortunately we can only speculate that some of the changes may have been from lifestyle changes. We can also only speculate that since "Flash" technology requires user participation to “swipe” to see glucose that perhaps the “out of sight out of mind” may blunt the effect for behavior modification.
In general, the large prospective studies in the T2D population have been with CGM used continuously over a 6-month period.19-20 Our study cycled patients two weeks on CGM then 1 week off for 12 weeks. There are only very limited small studies using CGM for a shorter duration (3-7 days and 1-4 sessions).21-28 However, their results are promising as they did show HbA1c, weight reduction, and some behavioral changes. Again we can only postulate, but interventions may have been more effective for behavior changes since they also included patient education about CGM, nutrition, and activity. In addition, the technology has advanced so that sensors now last 10-14 days and require no calibration, which should also improve patient use and adherence.
Intermittent RT-CGM use would make the cost more affordable. It is difficult to assess/compare costs but translational DPP group classes median cost was $424 per person for a year-long intervention and as high as $5881 per person for individual programs. 30 Intensive lifestyle intervention (ILI) with a target of 7% weight loss in patients with diabetes did decrease medical costs and hospitalizations in the LOOK AHEAD study but the cost per person was $2864 per ILI participant compared with $202 per control/traditional diabetes support and education (DSE) in the first year. A large part of the cost was the ILI meal replacement which were $798 per participant31,32 in the first year. Estimated costs of individual sessions, group intervention, meal replacement for lifestyle changes, and weight loss are not directly comparable to medical device cost but rather used as a broad comparison since Medicare is currently reimbursing for DPP group intervention. For gross comparison, cash cost of the personal CGM sensors range from approximately $35.99-43.00 for one FreeStyle Libre sensor and $87.25 for Dexcom G5-G6 for 7-10 days of use (package information and personal communication Dexcom and FreeStyle Libre). Medicare reimbursement per CGM session with insertion currently averages $157.77 for health care providers. 33 So if two to four sessions were performed assuming average sensor cost of $63.13, the potential cost would be $442.79 for 2 educational sessions and 2 sensors and $883.60 for four sessions with 4 CGM sensors. Although it is unknown if long-term behavior change will occur with intermittent short-term CGM coupled to nutrition and physical activity counseling, the cost would be comparable to other lifestyle interventions for diabetes and prediabetes and less time intensive for the patient.
The heart of diabetes prevention and diabetes management is lifestyle changes and weight reduction. Currently the National DPP is the only reimbursable mechanism for diabetes prevention, but it is time-intensive with many not reaching a 5% weight loss goal, despite the greater than year-long intervention. 34 CGM technology has now advanced to no-calibration systems that potentially allow expansion of use to those with diabetes not on insulin and those with prediabetes. Objective measurements of changes in food and exercise in patients on RT-CGM in patients and standardized training materials for providers and users need to be developed. Duration of user utilization (indefinite versus finite “educational” period) needs to be better defined.
Rather than being used as a “reactionary device” for hypoglycemia prevention and glycemic management, RT-CGM should be assessed for its use as a prevention tool. Its potential role as an adjunct to lifestyle changes, weight reduction, and potential to decrease overall use of insulin and other medications in patients with T1D, T2D, and prediabetes calls for further evaluation.
Footnotes
Abbreviations
BMI, body mass index; CGM, continuous glucose monitoring; DPP, Diabetes Prevention Program; DSE, diabetes support and education; GLB, Group Lifestyle Balance; HbA1c, hemoglobin A1c; ILI, intensive lifestyle intervention; MDI, multiple daily insulin injections; RT, real time; SMBG, structured self-monitoring of blood glucose; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.