
Abstract
Children and youth with physical disabilities face significant psychosocial challenges compared to their able-bodied peers. Medical specialty camps provide space where children can enjoy a typical camp experience alongside peers with similar conditions, offering programming and support tailored toward various levels of ability. This paper aimed to assess the impact of such camps on the psychosocial well-being of children with physical disabilities. A literature search performed in PubMed and Science Direct uncovered n = 33 research articles meeting the inclusion criteria. The existing literature consists of a mixture of qualitative and quantitative studies, collectively suggesting that medical specialty camps can lead to measurable improvements in children's quality of life, self-esteem, and self-perception, while also fostering positive social connections, enjoyment, belonging, and empowerment. However, questions remain about the long-term benefits of these camps, with extinguishing effects potentially being offset by follow-up programming. The absence of control data limits the strength of the conclusions that can be drawn. This review builds on the body of literature suggesting that medical specialty camps offer positive improvements to the lives of children and youth with illnesses and disabilities. Also, it suggests key components of effective research in this field, as well as avenues for future study.
Introduction
Physical disabilities (PD) impact the lives of hundreds of thousands of children and youth each year. While it is challenging to find data on the prevalence of PD as an encompassing category, statistics on the prevalence of specific conditions in the United States can provide an indication of how common PD in children and youth are (Table 1). However, this is only a subset of PD and does not take other countries into account, which only further highlights the significant local and global impact of PD on the lives of children.
Incidence or prevalence of physical disabilities in youth in the United States.
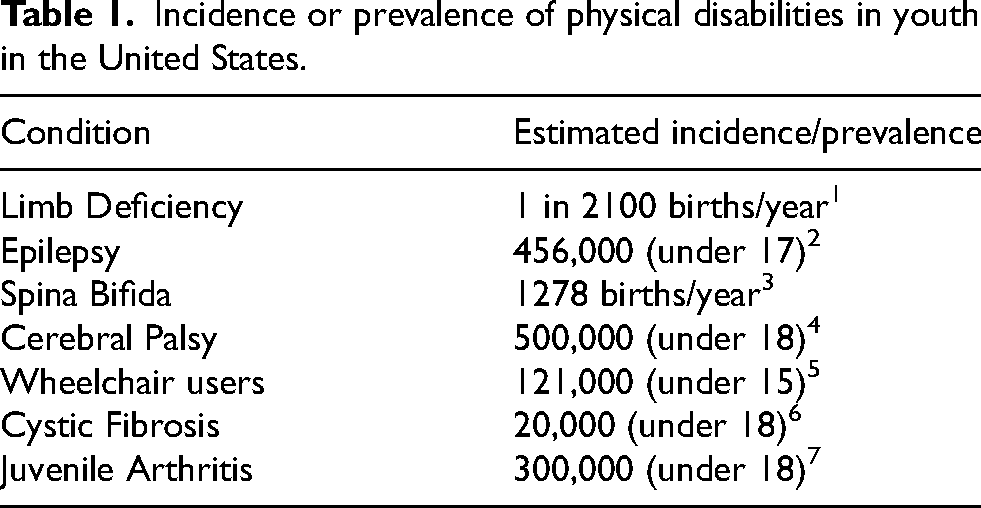
Furthermore, disabilities have significant psychological effects on young people. Youth with disabilities have prolonged adolescence and lower self-esteem, are more vulnerable to negative experiences, and are at a higher risk for bullying compared to their peers.1,2 Children with PD in particular have been found to have greater functional impairment socially, academically, and physically, and are at higher risk of psychosocial issues when compared to children without visible, physical differences.3,4 Youth are also at a higher risk socially due to being less involved in social activities because of health-related barriers.4–6 Children with visible facial conditions are more likely to have lower self-esteem, poor body image, higher stigma, and less social acceptance.7–9 Young people with spina bifida and epilepsy report a lower health-related quality of life and poorer psychosocial adaptation than youth with other chronic health conditions.10,11
One response to these problems has been the creation of medical specialty camps (sometimes called therapeutic recreation camps). The first organized camp in America was founded in the late 1800s, offering outdoor programming to teach boys how to live the life of a soldier. 12 By the early 1900s, physical-illness specific camps, also known as “medical specialty camps,” began to appear. These camps incorporated learning and social activities for children who often were previously isolated, while under medical supervision. 13
According to Cushner-Weinstein et al., there now exist “approximately 138 asthma camps, 91 muscular dystrophy camps, 65 diabetes camps, 60 cancer camps, 47 hemophilia camps, 40 sickle cell anemia camps, 26 renal disease camps, 17 obesity or weight management camps, 13 Crohn's disease camps, 7 burn camps, 3 neurofibromatosis camps, 3 Tourette's syndrome camps, and 25 camps for children with epilepsy.” 14 Haberman reports that “there are over 400 camps in the USA specifically serving children with chronic illness or disability.” 15
A significant research effort has been devoted to understanding how camps have provided a setting for social-emotional learning and character development for children. 16 The intended outcomes of many of these camps include the further development of self-confidence, independence, new friendships, group identity, new skills and new interests. 17 While many studies and review papers have evaluated the effects of involvement in medical specialty camps in children with burns, diabetes, cancer, visual impairment, and chronic illnesses,18–25 among others, there is a paucity of data available for children with PD (e.g., limb differences). 17 No study has yet been performed to gather the qualitative and quantitative results of recreational camps for children with PD. Given the large number of youths currently living with such conditions, and the psychosocial and medical differences between PD and chronic illnesses, this is a significant discrepancy in the existing literature regarding the experiences of a substantial pediatric population.
Therefore, due to the unique challenges faced by youth with PD and the lack of collected data focusing on the effect of camps on this population, the goal of this review was to systematically chart the research in this area and identify existing gaps in knowledge, as well as provide commentary on any insights and issues observed. The following research question was formulated: what is known in the literature about the impact of medical specialty camps on the psychosocial well-being of children and youth with PD?
Methods
For this review, the reporting guidelines from the PRISMA extension for scoping reviews (PRISMA-ScR) were used, but protocol registration was performed after the literature search. 26 A review protocol was discussed with all authors prior to the literature search and iterated upon throughout the search process. The final protocol was registered with the Open Science Framework on August 14, 2025 (https://osf.io/dq452).
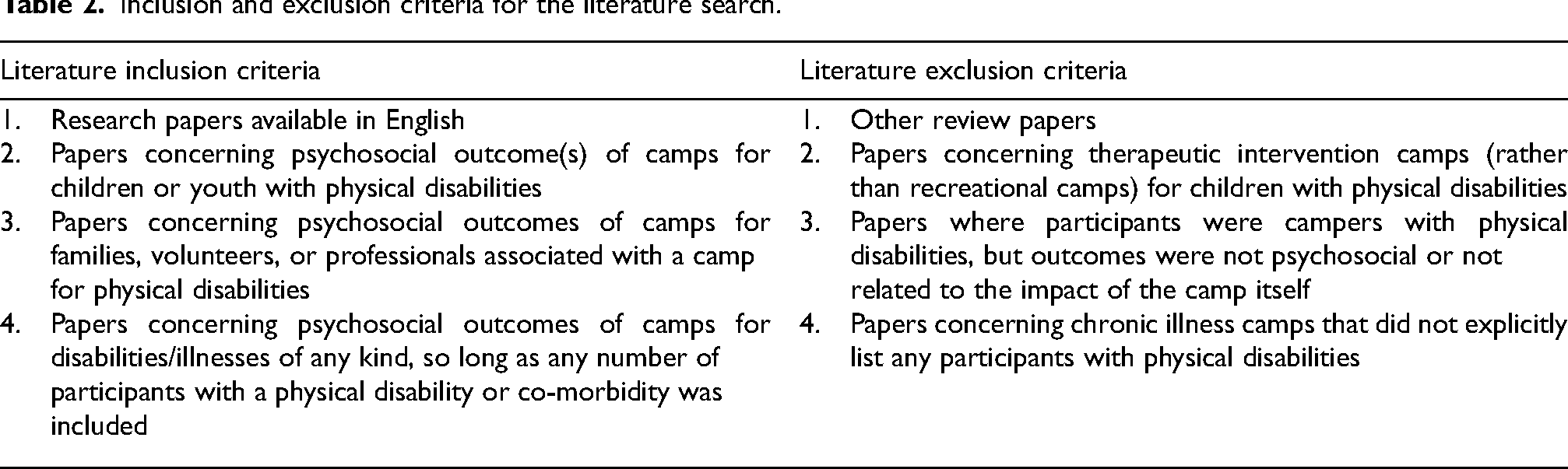
Inclusion and exclusion criteria are shown in Table 2. No restrictions were made regarding publication date. Both qualitative and quantitative studies were included.
Inclusion and exclusion criteria for the literature search.
Literature search
A literature search was performed in PubMed and Science Direct in June 2024 and updated in December 2025, using the search terms “(pediatric OR paediatric [Text Word]) AND (camp [Text Word])” as well as “Medical* [Text Word] AND special* [Text Word] AND camp [Text Word]”. These search terms were developed by the authors after a preliminary review of the literature for keywords. Citations within relevant research articles and review papers were scanned for additional references. The resulting 3305 papers (including 36 references from other sources and not including duplicates) were evaluated for relevance independently by both reviewers using Covidence systematic review software. Discrepancies between decisions were discussed between the authors until a consensus was reached.
PD were defined broadly using several sources and refined throughout the review process as new conditions came up. The United Spinal Association states: “Physical disability is often the result of a medical condition, such as muscular dystrophy, multiple sclerosis, arthritis or epilepsy. Some disabilities are present at birth, such as cerebral palsy, spina bifida and partially formed/not fully functional limb or extremity. Physical disability also can result from an injury, such as loss/reduction of use of a limb or spinal cord injury.”
27
Victory Junction Camp includes on their website a list of PD including “spina bifida, muscular dystrophy, spinal muscle atrophy, arthrogryposis, myasthenia gravis, skeletal dysplasia, and … amputations.” 28 Camp Barnabas categorizes their campers by distinguishing PD from developmental disabilities, posttraumatic burn injuries, blood diseases and cancer, medical disabilities, and visual or hearing impairments. 29 These examples were used as guidance for the inclusion criteria in this review regarding which conditions could be classified as a ‘physical disability’. Articles were excluded if they encompassed camps for behavioral issues, addiction, diabetes, obesity, asthma, autism, attention-deficit/hyperactivity disorder, organ disease and transplants, HIV/AIDS, celiac disease, victims of violence, sickle cell disease, migraines, inflammatory bowel disease, urinary incontinence, hemophilia, phenylketonuria, and sensory impairments.
After reviewing titles and abstracts, 3100 studies were excluded. Following full-text review of the remaining 205 papers, a total of 33 studies that met the inclusion criteria were included in this review.
Data analysis
A data-charting form was developed and is shown in Table 3, summarizing the data and main findings of the 33 research articles included. This included the author, year of publication, country of study, illness or disability studied, study design and timepoints, participant data (i.e., demographics), an overview of the camp, psychosocial outcome measure/s used, key findings, and sources of funding. Data was extracted jointly by both reviewers and cross-checked at separate time points through iterative review to enhance accuracy and inter-rater reliability.
Review of camp programs and their effects on the psychosocial wellbeing of children and youth with physical disabilities.
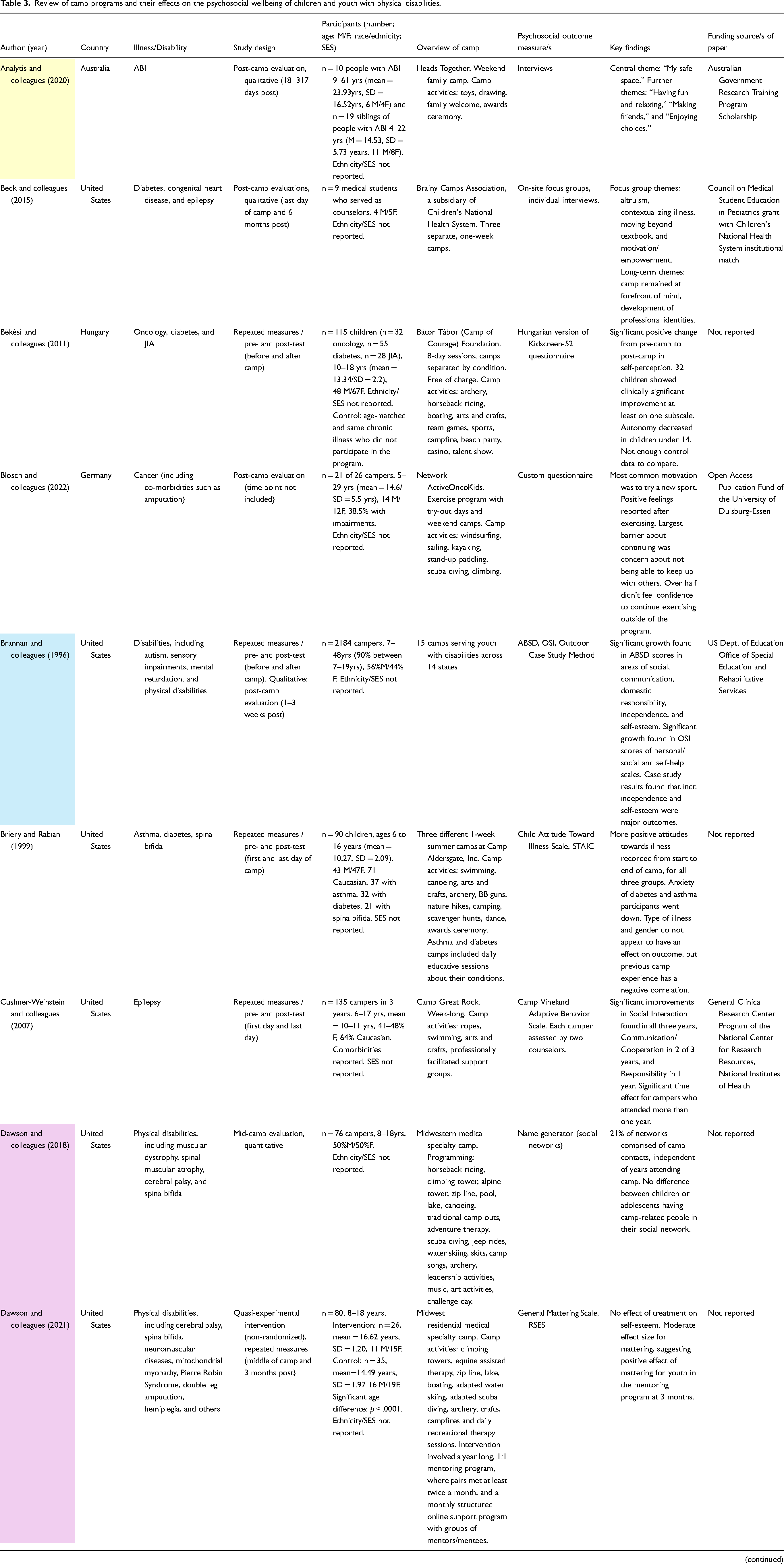
Color groupings indicate papers with shared authors and/or studies evaluating the same camp.
ABI: acquired brain injury; ABSD: Affective Behavior Scales for the Disabled; Dept.: department; F: female; GA: Goal Attainment; incr.: increased; JIA: juvenile immune arthritis; LLC: life-limiting conditions; M: male; OSI: Outdoor Skills Inventory; PedsQL: Pediatric Quality of Life Inventory; RSES: Rosenberg Self-Esteem Scale; SA: Social Acceptance; SBIS: Spina Bifida Independence Survey; SD: standard deviation; SES: socioeconomic status; SOSBMR: Sharing of Spina Bifida Management Responsibilities; STAIC: State-Trait Anxiety Inventory for Children.
Custom surveys or evaluations were classified as quantitative if there were numerical results that were statistically analyzed, and qualitative if the results were summarized only by graphs and/or descriptions. Quantitative results were organized by effect—positive, negative, neutral (non-significant), or static (one-time measurements). Outcome measures were gathered, listed, and tallied. Within-text citations and external searches were used to determine if each of the measures was validated.
A thematic qualitative analysis was performed to summarize the results of all papers which utilized semi-structured interviews, focus studies, or qualitative custom surveys. This was performed following similar methods as Neville et al. 20 After reading and highlighting results sections, a variety of sub-themes was identified, then grouped and placed under broader theme labels.
Results
The search uncovered 33 studies (Table 3) which evaluated psychosocial outcomes of camps for children with PD. Several groups of papers had shared authors, with some evaluating the same camp using different metrics, and others evaluating different camps with the same metrics. These connections are indicated in the table by shared colors. Not all studies included the name of the camp(s) investigated, so other unknown connections may exist.
Characteristics of camps and participants
The literature search uncovered studies conducted at camps that took place around the world, with 20 papers in the United States (several studying the same camp or multiple camps), five in Canada (two reviewing the same camp),30–34 three in Australia (two evaluating the same camp),35–37 and one each in the United Kingdom, 38 Germany, 39 Ireland, 40 and Hungary. 41 One paper surveyed camp alumni across eight countries. 42
The number of study participants (either individual campers with disabilities or whole families) ranged from five to 178 at the start of camp, with a median of 43 participants. This excludes Brannan et al.'s 1996 report which studied 2184 campers across 15 camps and Gillard et al.'s 2023 study evaluating 2245 alumni from 16 camps.42,43 Seven studies had over 100 participants.14,38,41,44–47 Where retainment was reported, dropout rates significantly increased the longer the study went on. While Yang et al. retained 59% of participants from pre- to post-camp, they only retained 18% of the original participants all the way to the three-month follow-up. 38 Other long-term retainment rates were 23.5% (three months), 48 61% (three months), 45 66% (one month), 49 and 87% (one month). 46 For pre- and post-camp study designs, retainment ranged from 21.9% for Békési et al.'s control group 41 to Ohanian et al.'s 62.3%. 50 Four studies reported no significant differences between participants who were retained and those who declined to finish the study.41,45,49,50 Yang et al. found a decrease in proportion of females in the post-camp surveys, 38 and Meltzer et al. found that dropouts reported less camp experience, fewer caregiving duties, and lower subjective stress. 46
The programming of the camps was generally similar, with the largest difference being the length of camp and whether families were involved. Some camps lasted a weekend (n = 5),36,37,39,51,52 while others were a whole week (n = 21)8,14,15,31–35,38,44–50,53–57 or longer (n = 3).30,41,58 A portion of the camps allowed family and/or friends to attend (n = 11),31,36–40,46,48,49,51,53 while most were just for youths. When activities were reported, there was abundant overlap across camps including archery, arts and crafts, swimming, and horseback riding. Many camps were free or had financial assistance available if needed (n = 11).30,32,34,36,38,41,42,44–46,51,56,57 Several camps provided specific programming for discussions or workshops surrounding youth's disabilities or coping (n = 6).14,45,50,54,55,58 Note that some of these counts include separate studies assessing the same camp, so overlap may exist.
The camps studied served youth with a variety of disabilities or conditions, as shown in Figure 1. Many studies evaluated camps that served a broad range of diagnoses, with six camps for PD,32–34,48,55,58 two for chronic illnesses and disabilities,15,38 two for any disabilities,31,35 one for life-limiting conditions, 40 and one for multiple disabilities. 47
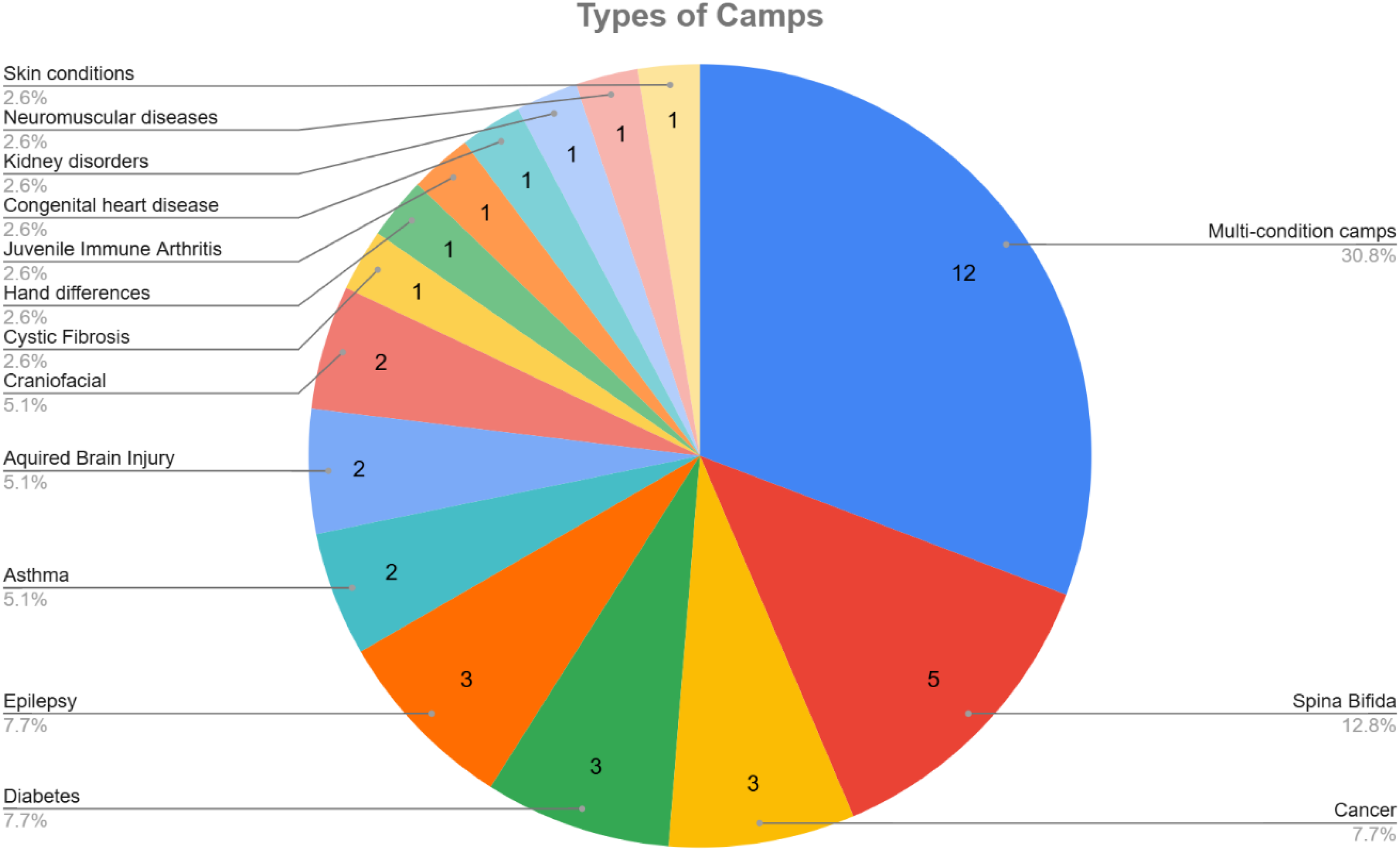
Representation of conditions served by each camp in this review, excluding Brannan et al. and Fullerton et al.'s larger studies of 15 camps each.
Other papers evaluated multiple camps that each served a specific condition, such as Meltzer et al. who investigated camps for the following: asthma, cancer, epilepsy, and kidney. 46 These were all tallied separately, causing several camps that were not specifically in the inclusion criteria (e.g., diabetes) to be represented. Brannan et al., Fullerton et al., and Gillard et al. were not included in the graphic because they studied 15–16 separate camps whose specialties were not elaborated on explicitly.42,43,59
Where data was available, there were an equal number of studies with more male or more female participants. Brannan et al.'s extremely high sample size (n = 2184) was 56% male, whereas Gillard et al. had 59.29% female respondents. The rest of the studies had more female participants represented than male participants (48.3% male and 51.7% female of 1700 total reported). Four papers did not report gender demographics.15,40,50,56 The age of child campers ranged from 4–19 years old, with five camps extending beyond this range into adult campers or alumni,36,39,42,45,49,50 and one study including mothers of infants as young as five months. 46 Five papers did not report age demographics, though four evaluated adults related to the camp.15,40,53,56,59 Ethnicity or race was reported by 12 of the 33 papers. Of those, 63% to 100% of participants identified as White or Caucasian. Socioeconomic status or employment was reported by only six papers. Holbein et al. classified 56% of families as middle to upper class (>30k $USD/yr). 45 Luzinat et al. and Ohanian et al. reported average incomes of 63k ± 31k $AUD and 95k ± 49k $USD respectively.37,50 Meltzer et al. reported that 70% of mothers interviewed were employed. 46 Gillard et al. reported education and employment, with 19% of responding alumni having a Bachelor's degree or above, and 81% being employed or students. 42 And lastly, O’Mahar et al. reported a mean Hollingshead score (a measure of socioeconomic status ranging from 8–66 where higher scores generally indicate higher status) of 41 ± 14.5. 49 Altogether, these results indicate that the average camp attendee tended to be middle class or above.
Study designs and outcome measures
A variety of study designs and outcome measures were used in the papers examined to collect both quantitative and qualitative data on the psychosocial outcomes of the camps. The most common study design was a single post-camp or mid-camp evaluation (n = 17). There were also seven pre- and post-test designs,14,30,41,43,50,54,57 and eight repeated measures studies,8,34,38,45,46,49,52,56 with time points ranging from a few weeks before camp to 12 months post-camp. There was a single, non-randomized, quasi-experimental intervention with a repeated measures design. 55
A list of all outcome measures employed in the studies is shown in Table 4. A ‘Partial’ rating for validation indicated that some initial reliability or validation measure was reported within the study but not outside of it,43,45 or that psychometric measures have been tested with mixed results.60–63 A ‘No’ rating for validation indicated that no reliability or validation information could be found (either generally or for children), even if other studies have used that measure in a related context or population. Gillard et al.'s survey was the sole exception within custom surveys, adapted from the American Camp Association's Youth Outcomes Battery and Youth Impact Study Survey, and reporting high reliability via Cronbach's alpha. Other non-psychosocial outcome measures, such as pulmonary function or physical activity time, were excluded from this count.
Outcome measures used by studies, frequency of use, and whether there is validated documentation for the assessment, both in general and for children or youth.
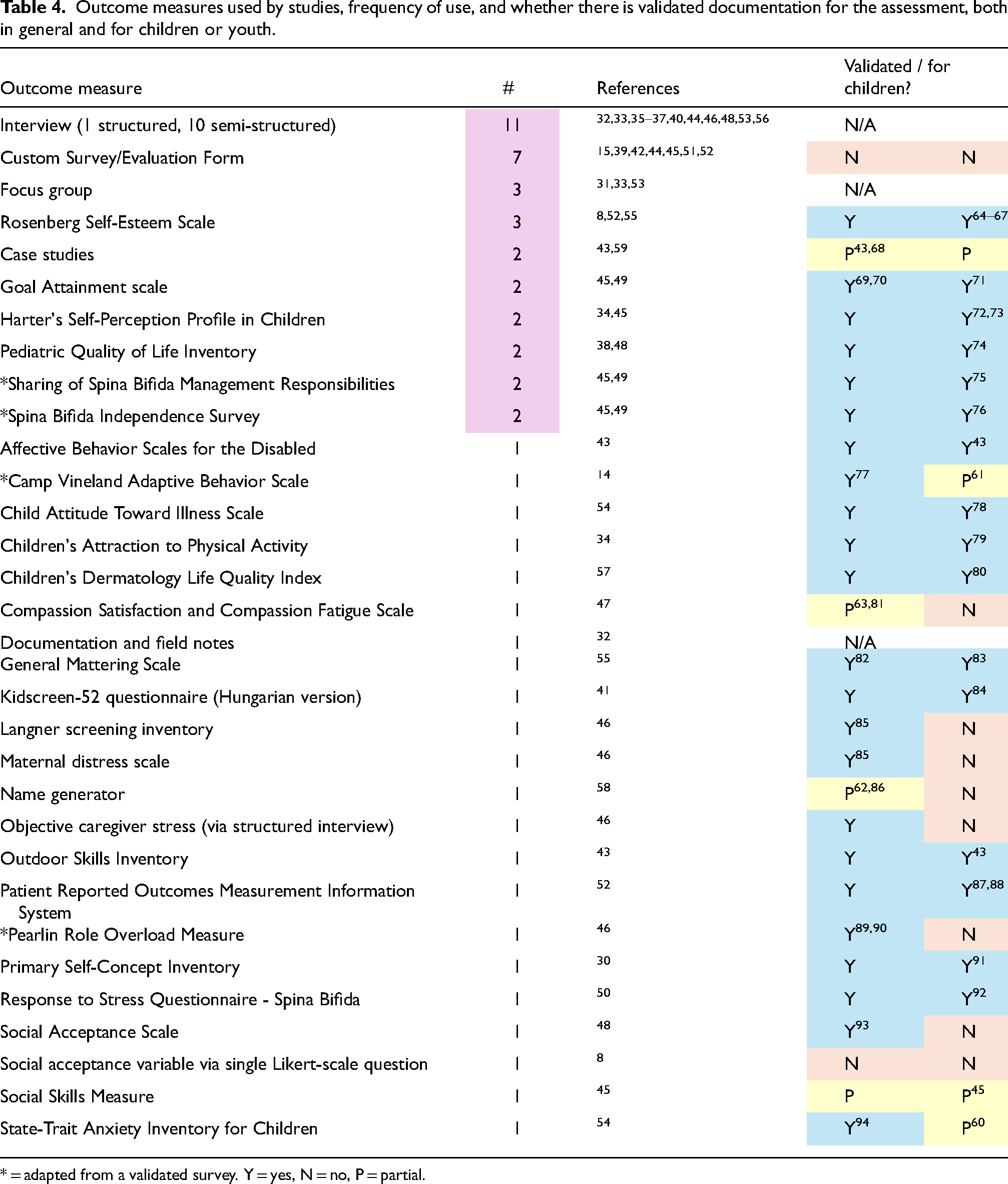
* = adapted from a validated survey. Y = yes, N = no, P = partial.
Of the studies that utilized one or two outcome measures, there was a nearly equal split between those using only quantitative or qualitative outcomes. All qualitative measures were gathered after interviewees attended the camp, ranging from several weeks to several years post-camp. Meltzer et al. applied five quantitative measures, including a structured interview used to discern stress and distress. 46 Holbein et al. utilized six quantitative measures, including a custom, Likert-scale survey to evaluate camper satisfaction with the program. 45 Knapp et al. (2015) and Brannan et al. were the only studies to employ both quantitative measures and qualitative interviews/case studies.43,48
Of the studies using quantitative measures, there were six surveys employed by more than one study. These were the Rosenberg Self-Esteem Scale (
Nearly all of the quantitative assessments had been validated, including for children or adolescents. Only initial validation was accomplished on the outdoor case study method employed by Brannan, 43 and only the compassion satisfaction subscale of the Compassion Satisfaction and Compassion Fatigue Scale (CSCFS) has been validated, although an updated, fully validated version has since been published. 63 Holbein et al. developed a custom social skills measure for their study and reported adequate internal consistency. 45 Most of the measures from this review which had been validated for adults but not for children were explicitly aimed towards caregivers. 46
Qualitative themes (n = 15)
Fifteen papers utilized semi-structured interviews, focus groups, and/or a qualitative, custom survey.31–33,35–37,39,40,43,44,48,51,53,56,59 Seven common themes were identified across all papers: connections, fun, belonging, empowerment, understanding, future-shaping, and improved outlook. Figure 2 summarizes the number of studies that included results that fit into each theme. Eight papers also reported some areas for improvement.
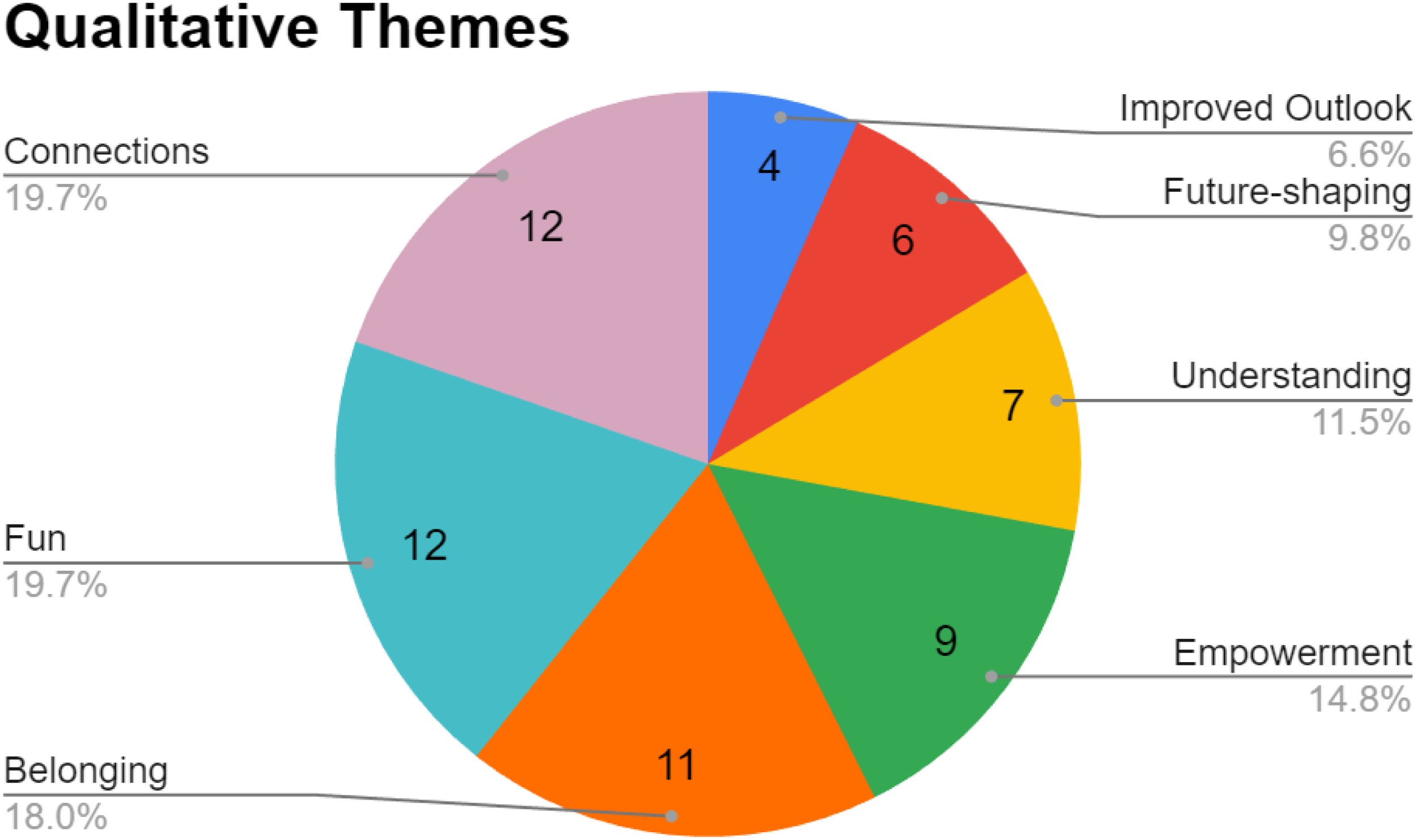
Camp outcome themes across all qualitative studies, by number of papers reporting each theme.
Connections (n=12)
A significant theme cited by nearly all papers was the importance of connections formed at the camp.31–33,35–37,39,40,44,48,51,56 The most prominent examples of this are friendships formed by campers, noting that this may include making friends as a new camper or maintaining or growing friendships among returning campers. These connections were often long-lasting, with several studies mentioning friendships between campers that continued past the duration of the camp itself.32,40,51 The connections also contributed to a positive peer pressure at the camps, in which youth were encouraged by the presence of their friends to do more than they may have been able to on their own. 32 The connections made at camp also served as a source of information sharing, both between youth and between parents at family camps.31,37,40 Children and caregivers alike were able to learn from one another's experiences and benefit from that relationship.
In the family camps, another positive outcome was the improvement of within-family relationships. The chance to be able to participate in activities together in a less stressful environment proved beneficial for parents connecting to their children and for siblings connecting with one another. Numerous papers found that families were closer to one another and stronger as a result of the camp.31,36,37,40
Finally, the connections made with counselors and camp staff appeared to be another positive aspect of the camps. Parents trusted the staff to take care of their children, and professional volunteers appreciated the chance to grow more familiar with patients outside of a hospital context. The situation fostered trust between hospital staff and patients, leading families to be more comfortable approaching staff.33,40,44,56,56
Fun (n = 12)
Nearly all studies also found that everyone involved in the camps had fun.31–33,35–37,39,40,44,48,51,56 Campers enjoyed a variety of activities such as horseback riding, swimming, and arts and crafts. The fact that facilities and activities were all accessible was a positive factor compared to the disable-ism often faced in everyday life.31,51 Those who often participated in physical activities solely in a therapeutic environment found exercising to be fun in itself. 33 Children often stated they wanted to return, and could recall many camp activities in detail months after the fact.48,51,56 From a family perspective, caregivers found the camp to be relaxing and a break from worrying.31,37,40 They saw the camp as a safe place for their children, so they could simply rest and enjoy themselves.31,40 Families were energized and joyful as a result of the camp.31,36,40
Belonging (n = 11)
Many papers included results describing the sense in which the campers felt accepted for who they were.31–33,35–37,40,44,48,51,56 They no longer felt alone but rather understood by others who were going through similar experiences.31,36,40,44,56 The camps were seen as an emotionally safe space for the children, where judgmentalism or bullying was not a problem, and they were free to be themselves.32,35,48 There was an overall sense of normalcy and equality at the camps that was uniquely refreshing. 33 Campers felt they could talk honestly about anything, or alternatively, be in a space where they didn’t have to explain their differences.36,40
Empowerment (n = 9)
Many campers enjoyed a greater level of choice, independence, and self-confidence as a result of the camps.31–33,35,36,39,44,51,59 Children were able to choose in which activities they wanted to take part, how to take part, and with whom to take part.33,35,36,44,59 Whether at a family camp or on their own, they were able to exercise confidence by trying new things and experiencing the resulting pride at the level of their accomplishments.31–33,35,39 Campers were challenged to push their limits and overcome their doubts, and as a result, parents found their children to be bolder and more willing to try new experiences or continue participating in activities after the camps.32,33,39,44 This self-confidence was not limited to physical activities, but also to being more willing to speak up about their disabilities and needs. 33
Understanding (n = 7)
Camps also served as a place of learning and increased understanding of disabilities.31–33,35,36,44,53 Campers learned more about their disability and how to adapt as a result of the connections they made at camp.32,33,36 Volunteers were especially impacted in this way. Medical students felt that they moved beyond the textbook to be more sensitive to people's needs and the social aspects of health. 53 They and other camp staff found they had a better understanding of the daily impact of diseases and saw patients as more than their condition.44,53 Even parents echoed these thoughts, gaining a better understanding of their children's experiences and capabilities, as well as the resources available to them.33,44
Future-Shaping (n = 6)
The camp experience had a meaningful impact on volunteers and campers’ perspectives of the future.31–33,40,44,53 Medical volunteers found that their camp experiences motivated them to work harder. 53 They found that the skills they developed, such as listening, leadership, and interacting with children would serve them well in their future careers. Other staff found the camp to have a meaningful impact on their work, even resulting in better support of patients beyond the program.40,44 Parents were more comfortable with the idea of participating in future programs. 31 And lastly, the confidence and skills that campers developed served as a practical learning experience for their future transition into independent adulthood.32,33
Improved outlook (n = 4)
Several papers cited the way that the camp contextualized families’ situations and left them feeling more positive, thankful, and optimistic about their outcomes.32,33,37,40 Additionally, youth were able to reframe therapeutic exercises as sports and view therapy equipment in a more positive light. 33
Areas for improvement
The largest area of improvement that many of the studies highlighted was a lack of transference of the skills or activities in the camp to similar opportunities when campers returned home.32,39,48 While one study cited a lack of self-confidence as being an impediment, 39 most participants simply lacked available resources or opportunities close enough to home to pursue their desired activities after returning from camp.32,48 Another paper brought up that lack of knowledge is a big barrier to finding adaptive children's sports programs to continue their physical involvement locally. 33 There were requests for a resource list or for follow-up programs.
Fullerton et al. found that roughly half of counselors and parents saw no change in their child's behavior before and after camp. 59 The authors suggested that this finding may have been partly due to the interview protocol, which framed growth using examples of changes in the child's abilities.
A few sources referenced an initial nervousness on the part of campers, families, and volunteers before attending camp.33,37,44 For families and campers, being in an unfamiliar place with new people seemed intimidating. Staff were concerned about not being prepared enough to take care of campers with more complex needs. However, in all cases, those concerns were found to be short-lived. Families and campers ended up enjoying themselves. For volunteers, having a thorough training program before the camp prepared them well.
Other papers mentioned homesickness or family strife as factors that contributed to a negative experience in the camp setting.36,44 One study also described a camper with behavioral challenges that created difficulties, along with challenges when staffing was insufficient. 44
Finally, Youngblood et al. evaluated the impact that the COVID-19 pandemic had on families when the camp program was no longer available for them. 31 They found that COVID put more pressure on mothers, worsened isolation, reduced the family's ability to do things together, and made siblings more impatient with one another. All of this was in direct contrast to the benefits that the camp had provided to the families prior.
Quantitative results (n = 20)
Twenty studies employed quantitative outcome measures and data analysis.8,14,15,30,34,38,41–43,45–50,52,54,55,57,58 Most employed a repeated measures design, with at least a pre- and post-test, while four studies investigated a single time-point.15,42,47,58 Nearly all papers used some form of survey or questionnaire to obtain their data. Meltzer et al. used a structured interview to quantitatively assess caregiver stress, 46 and Dawson et al. (2018) used a name generator method to establish camper's social networks. 58 The results of these studies are summarized in Table 5.
Quantitative outcome results.
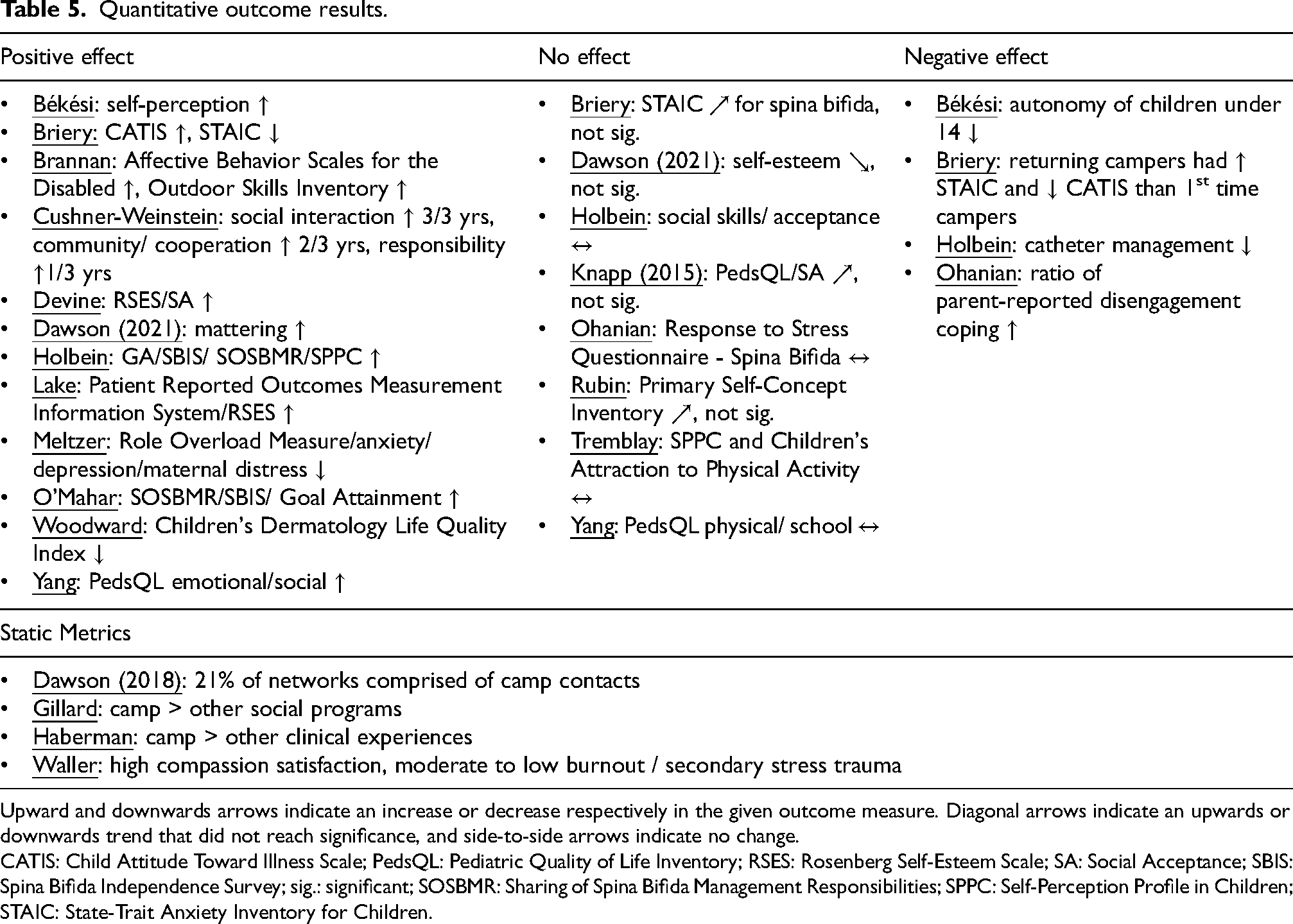
Upward and downwards arrows indicate an increase or decrease respectively in the given outcome measure. Diagonal arrows indicate an upwards or downwards trend that did not reach significance, and side-to-side arrows indicate no change.
CATIS: Child Attitude Toward Illness Scale; PedsQL: Pediatric Quality of Life Inventory; RSES: Rosenberg Self-Esteem Scale; SA: Social Acceptance; SBIS: Spina Bifida Independence Survey; sig.: significant; SOSBMR: Sharing of Spina Bifida Management Responsibilities; SPPC: Self-Perception Profile in Children; STAIC: State-Trait Anxiety Inventory for Children.
The study by Ohanian et al. was the only one that found exclusively negative and neutral outcomes, where campers’ response to stress did not change before and after the camp, and parent-reported disengagement coping increased. However, their primary focus was documenting stress and coping mechanisms rather than assessing the impact of the camp as an intervention. 50 The other three papers reporting negative outcomes saw positive results in other metrics.41,45,54
The static metrics contained results from four quantitative papers that did not use a repeated measures design, but rather a single time-point evaluation.15,42,47,58 Although not directly examining the effect of the camp, they pointed to a positive experience, in which campers connected and made lasting friendships, student volunteers enjoyed their experience more than other clinical experiences, camp staff did not suffer from compassion fatigue, and alumni found their camp experiences to be more influential in their lives than other social programs.
Control groups (n = 4)
Only four studies attempted to use a control group for outcome comparison.41,46,54,55 Békési et al. reached out to age-matched children with the same chronic illness who did not attend camp, 41 and Briery et al. sought to compare families still on the wait list for camp. 54 However, neither study received enough responses to evaluate their control data.
Meltzer et al. compared parents of children undergoing treatment to parents of children who had recovered from cancer and found that the control group maintained a decrease in maternal distress for up to a month after the camp, while the treatment group's distress returned to baseline after the camp. 46 However, this control group is only effective in comparing the cancer groups, and the study lacked a control group of chronically ill children not attending camp.
Dawson et al. (2021) utilized a non-random intervention to investigate the effect of a continued mentoring program after the camp. 55 The control group consisted of camp attendees who did not participate in the mentoring program, although they noted that there was a statistically significant difference in age between the two groups, with the intervention group being about two years older on average. They found a small positive impact on participants’ sense of mattering in the program compared to the control, but no effect on self-esteem.
Mixed effects (n = 8)
A few factors may influence who benefits most from medical specialty camps. Of the 18 quantitative studies, 11 investigated how various factors affected their reported outcomes. Results are summarized in Table 6.
Mixed effects results.
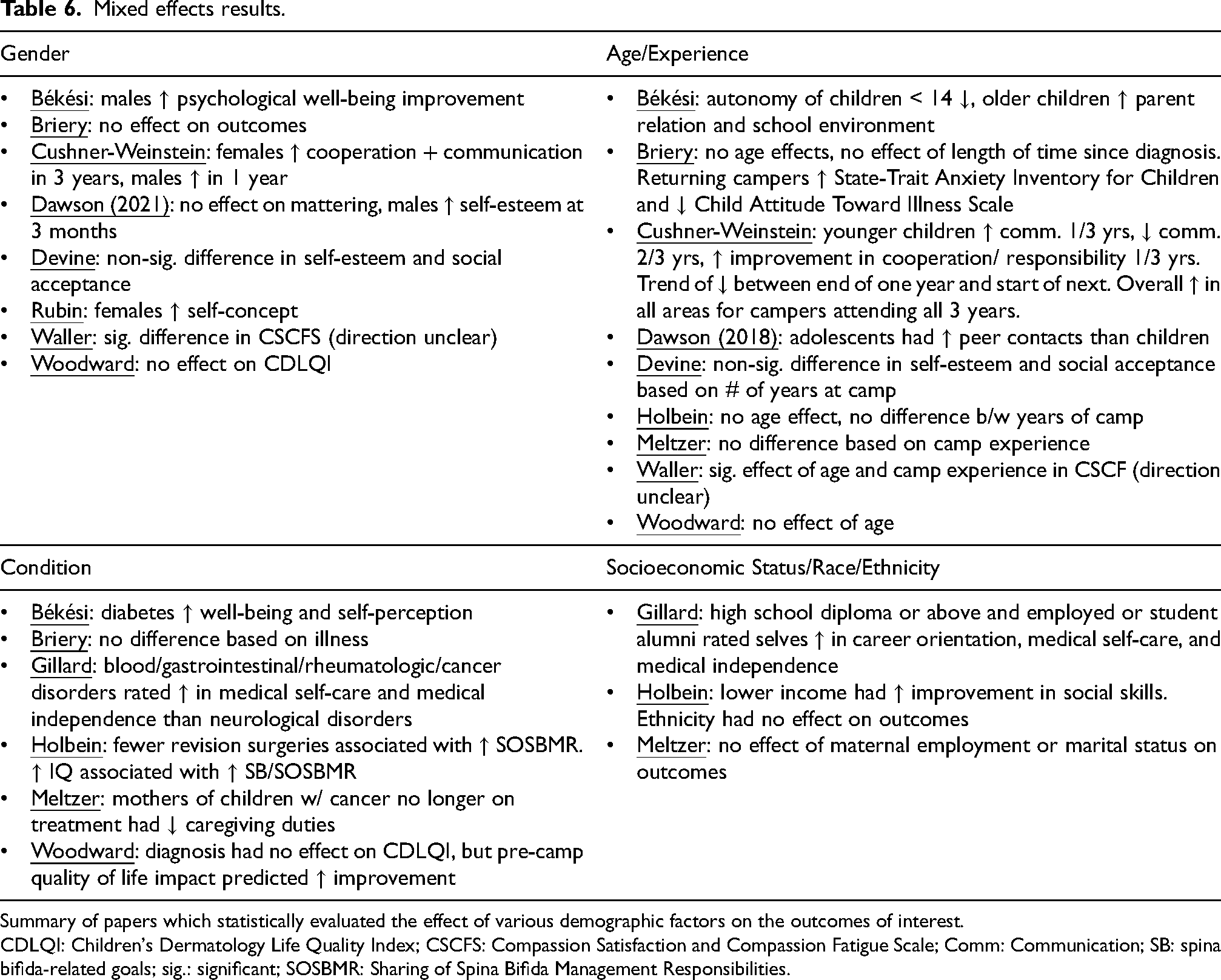
Summary of papers which statistically evaluated the effect of various demographic factors on the outcomes of interest.
CDLQI: Children's Dermatology Life Quality Index; CSCFS: Compassion Satisfaction and Compassion Fatigue Scale; Comm: Communication; SB: spina bifida-related goals; sig.: significant; SOSBMR: Sharing of Spina Bifida Management Responsibilities.
Gender: There was no clear consensus regarding gender. Briery et al. found no differences in campers’ attitudes toward illness or anxiety, and Woodward et al. reported no differences in quality of life. Dawson et al. (2021) likewise found no differences in mattering, but did report higher self-esteem in males at three months. Rubin and Geiger found females had higher subscale and global self-concept scores than males at both time points. Békési et al. reported psychological well-being improvements only in males. Lastly, Cushner-Weinstein et al. found that females rated higher than males in cooperation, responsibility, and communication for two separate years of camp, and also improved more in cooperation and communication over one year. In a different year, males improved more across all domains. Devine and Dawson found nonsignificant differences in self-esteem and social acceptance based on gender. Waller et al. found significant gender effects on compassion, satisfaction, and fatigue in volunteers. Altogether, this indicates that no strong conclusions can be made about the differences in psychosocial effects of a therapeutic camp experience on males versus females.
Age/Camp Experience: There were mixed reports on the effects of age or camp experience. Briery et al. found no age effects or effect of the length of time since diagnosis. However, returning campers reported more anxiety and worse attitude towards illness. Woodward et al. and Holbein et al. found no age effect, and the latter also found no difference in results between years of camp. Békési found that autonomy for children under the age of 14 decreased, whereas older children's autonomy did not change. Parent relation scores and school environment scores increased only for older children. Cushner-Weinstein found conflicting results depending on the year: younger children (<12) rated higher in communication in Year 1, but lower across multiple domains in Years 2 and 3. Older campers improved their communication skills in one year, whereas younger campers declined. In another year, younger campers improved more in cooperation and responsibility. Meltzer found no effects of camp experience. Dawson et al. (2018) reported that adolescents had more non-relative peer contacts in their ‘important matters’ networks than children, a developmentally typical but novel finding for youth with PD. Devine and Dawson found nonsignificant differences in self-esteem and social acceptance based on number of years at camp. Waller et al. found significant age and experience effects on compassion satisfaction and fatigue in volunteers. These mixed results highlight the unclear impact of age and repeated attendance on psychosocial outcomes.
Condition/Intelligence: Briery et al. found no pre-camp difference in results based on illness (asthma, diabetes, spina bifida). Holbein et al. unexpectedly found that fewer ventriculoperitoneal shunt revision surgeries were associated with better outcomes for managing spina bifida-related tasks. They also found that higher intelligence scores predicted better outcomes for spina bifida goals and tasks. Gillard et al. found that alumni with blood, gastrointestinal, rheumatologic, and cancer disorders rated themselves higher in medical self-care and medical independence than those with neurological disorders. Békési et al. found that the diabetes group had higher scores on physical well-being and self-perception compared to the cancer and arthritis group. Woodward et al. found that diagnosis did not significantly predict quality of life index. However, pre-camp scores did; that is, campers whose condition had a more severe impact on their lives before camp reported the greatest improvements in quality of life after camp. Lastly, Meltzer et al. found that mothers of cancer survivors had significantly fewer and shorter caregiving duties than other illness groups (cancer, kidney, epilepsy, asthma). Ohanian et al. found relationships between coping style and IQ, but this was not studied in relation to the camp as an intervention.
Socioeconomic Status: Holbein et al. found that lower income was associated with a greater improvement in social skills. Meltzer et al. found no effect of maternal employment or marital status on outcomes. Ohanian et al. found relationships between coping style and income, but this was not studied in relation to the camp as an intervention. Gillard found that alumni with a high school diploma or above rated themselves higher on responsibility, career orientation, medical-related self-care, and medical independence. Gillard also found that alumni who were employed or students rated themselves higher in career orientation, medical-related self-care, and medical independence.
Race/Ethnicity: Although 13 studies reported race and ethnicity,8,14,30,31,35,42,45–47,49–52,54 mixed effects were only statistically analyzed by Holbein et al., who found no effect based on ethnicity. Most papers could not perform analysis due to insufficient datapoints.47,54 Gillard did not examine race or gender variables due to international differences in definitions. 42
Long-term impact
If medical specialty camps do have a positive effect on youth, the question of how long this effect lasts remains unanswered. Previous reviews have reported either inconclusive results or a diminishing effect of positive outcomes for burn camps 95 and chronic illness camps.18,96,97
This review found similar inconclusive results, summarized in Table 7. Five studies reported that some positive effects remained in place for three weeks, 43 one month,46,49 three months, 55 or six months. 52 However, four studies found that other positive effects did not last at one month,38,46 six weeks, 8 or six months. 52 Of note, two studies found a lasting effect in one area but a temporary effect in another, potentially pointing to the variables that are more likely to see long-term impacts.46,52 A limitation lies in the fact that these studies did not aim to follow the long-term effects until they faded. Instead, they assessed participants at only one or a few predetermined follow-up time points; thus, the true duration of effects cannot be assumed with confidence.
Long-term outcomes of camps.
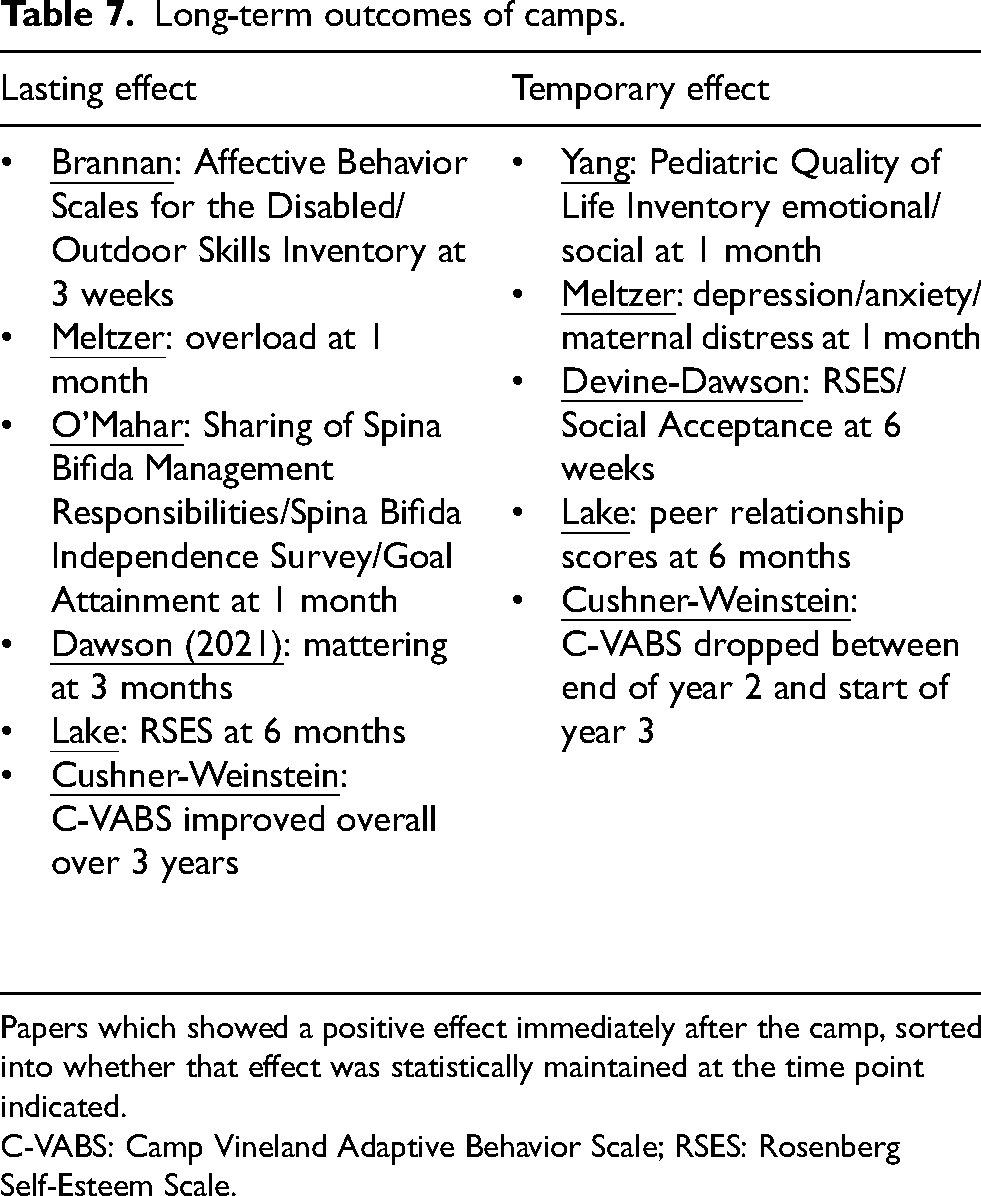
Papers which showed a positive effect immediately after the camp, sorted into whether that effect was statistically maintained at the time point indicated.
C-VABS: Camp Vineland Adaptive Behavior Scale; RSES: Rosenberg Self-Esteem Scale.
In evaluating adaptive behaviors in campers over the course of two or three years, Cushner-Weinstein et al. noted a drop in scores between the end of year two and the start of year three, potentially indicating diminishing effects over the course of a year. However, they also found an overall positive trend over the course of three years, suggesting that repeated camp attendance may result in an accumulation of benefits.
The qualitative studies offered a more conclusive picture. Many focused on in-camp experiences rather than lasting effects. However, lasting friendships and connections were a common theme. Children stayed in touch beyond the camp via texts and letters.32,40,51 Additionally, campers who attended for multiple years displayed excitement to see their friends again.36,56 Another effect Youngblood et al. found is that families had increased confidence to try new experiences after the camp, leading to trips previously considered unimaginable for their child. 31 This theme of opening families’ eyes to more possibilities was repeated in numerous papers, yet a lack of resources or opportunities in camper's hometowns dampened that optimism. Fullerton et al. found mixed long-term effects, where some participants had no lasting behavioral changes, while others described persistent efforts towards independence. 59 Gillard et al.'s survey of over 2000 camp alumni reported that the most impactful camp elements that contributed to personal improvement were feeling accepted and not judged, feeling a sense of freedom and possibility, and being able to try new things.
Discussion
The aim of this review was to gather and report on the psychosocial outcomes of recreational camps for children and youth with PD. Similar reviews have been conducted on the following camps: cancer, burn, diabetes, visual impairment, and chronic illness. The last of these has the most overlap with this study (three papers), but is over 10 years old. It could be argued that PD have very different psychosocial effects on children than chronic illnesses. PD present a unique challenge to the children they effect, as they often require lifelong accommodation and management, and can present in a physically obvious manner that can result in higher rates of bullying and lower self-esteem. Thirty-three research studies addressing this subset of campers were identified and here the results are discussed in broader contexts of research quality and other review papers.
On an important note, safety is a critical factor for parents in determining whether to send their child to a recreational camp. Hesitation may arise as these campers may have significant medical needs. However, there were no adverse events reported by any study in this review,39,44 nor in other review papers in children with chronic illnesses.98,99 Given parents’ hesitations revolving around their children's health, this should serve as reassurance that most specialty camps are well-equipped and prepared to handle all levels of care.
Outcome measures
Nearly all outcome measures employed in this review's studies were validated, including most for youth or children. However, this review did not assess age-specific validation. Arnoldo et al. notes in their 2006 burn camp study that the RSES was originally intended for adolescent age groups and has not been validated for younger children. Additionally, this review did not investigate validity for disabilities, i.e., whether an assessment tool has been validated only in an able-bodied youth population versus in youth with specific PD and conditions. The fact that most studies did not use a control group inherently reduces their internal validity and ability to generalize results. For the numerous papers using custom surveys or questionnaires,15,39,44,45,51,52 the risk of measurement bias remains unknown due to lack of validation. Psychometric properties of even validated outcome measures were inconsistently reported or cited.
Across related literature, some overlap in outcome measures can be found. Neville et al.'s cancer camp review found the PedsQL was the only validated outcome used in multiple sudies. 20 Focus groups and interviews were also common, found in at least five studies. Rea et al.'s systematic review of chronic illness camps reported studies using the PedsQL, SPP, and RSES. 19 Seven studies used semi-structured interviews. Burn camps most commonly used the RSES. 95 A review of congenital upper limb anomaly management recorded use of the PedsQL, State-Trait Anxiety Inventory for Children (STAIC), and RSES. 4 Most used boutique Likert scales, novel questionnaires, or visual analog scales to obtain the data of interest. An assessment tool used by several excluded studies100,101 was the Children's Hope Scale, geared towards chronic or life-threatening illnesses, rather than disabilities.
This review found 16 fully validated outcome measures whose domains of assessment spanned self-perception, quality of life, independence, self-esteem, mattering, self-concept, stress, anxiety, social acceptance, and more. Some studies asserted that investigating more specific factors (such as confidence or mattering) may provide a greater magnitude of results than general concepts (such as self-esteem).55,66 Additionally, camps that define themselves as interventions with specific psychosocial goals may achieve stronger improvements in the targeted outcomes for their campers.18,45,50,55
Quantitative and qualitative results
Despite varied methodologies and diverse populations, most findings showed that camps have positive psychosocial effects on youth with PD. The qualitative studies were unanimous: children and families enjoyed the camps, describing them as safe, socially connective, and fun. Most negative comments pointed to the fact that there weren’t good ways to keep participating in similar activities at home, implying that the value gained from these camps is worth maintaining. Dawson et al.'s 2018 paper found 21% of youth's social networks consisted of peers they met at camp, 58 and Zimmerman et al. found that 93% of families stayed in touch with other families 51 ; this indicates that camps foster valuable connections. Given that youth with PD can struggle with isolation and loneliness, 58 this effect cannot be discounted. 50
Nearly all quantitative studies reported improvements found in the areas of self-perception, quality of life, attitude towards illness, anxiety, self-esteem, social acceptance, mattering, responsibility management, and more. Only four studies reported no significant improvements in any domain, though two saw positive trends that did not reach significance.30,34,48,50 Studies which found no significant effect could have a few explanations. One is the timing of baseline assessments: scores collected on the first day of camp may be inflated due to arrival excitement and seeing friends. Alternatively, youths could already have a high sense of self. Tremblay notes that participants’ global self-worth scores were consistently above 3.0 out of 4.0, indicating a positive self-worth in children with PD. Other studies corroborate this fact in children with cerebral palsy, suggesting that although youth may feel less competent in certain aspects, the overall self-concept of youth with PD may not be lower than youth without impairment. 102 Similarly, Rubin and Geiger noted that their cerebral palsy campers’ intellectual self-concept scores were “more than 2 [standard deviations] higher than published scores for healthy children of a similar age” and their overall self-concept was not significantly lower than normal.
A further factor to consider is that many measurements were taken immediately post-camp, yet results related to coping mechanisms or social acceptance may not change enough to be statistically significant over such a short period of time. Similarly, factors such as self-esteem and coping are seen to be relatively stable over time. 50 Thus, consistent scores across time should not be viewed as a failure of camps to help their participants.
This also highlights the lack of appropriate control data. To accurately assess the effects of these camps, the psychosocial baseline of the population of interest must be well characterized. Validated comparison models that include able-bodied and impaired children, both with and without camp participation, are essential for understanding why outcomes may improve for some children or domains but not others.
While many questionnaires were filled out directly by the campers, several assessments were performed by counselors14,43 or caregivers43,45 on the campers’ behalf, and some studies relied on a mixture of respondent types.45,49,50 In multiple studies, parents reported greater magnitude of effects than campers in outcome measures, both positive and negative.10,45,50 Ohanian et al.'s parent report of disengagement coping increased, but the youth report did not, pointing to a potential mismatch between parent and youth perceptions. In broader literature, a study by Huang et al. investigated caregiver-child survey discrepancies in children with chronic conditions. They found statistical differences in perception of medication adherence, disease knowledge, and readiness to transition to adult care, supporting the point that including parent and child feedback may be valuable for obtaining a whole picture. 103 Future studies would benefit from incorporating feedback from both parties, which may result in a clearer perspective on certain psychosocial aspects.
Negative effects were minimal and typically outweighed by positives. Holbein et al. saw child-reported management of catheterization decrease over time, but saw improvements in many other areas. Békési et al. saw a decrease in the autonomy of children under the age of 14, but lacked control data to draw strong conclusions about what this may mean for those with disabilities. Briery et al. found that returning campers had higher anxiety and worse attitudes toward their illness than new campers, but those attitudes still improved over the course of the camp. However, they lacked baseline data for returning campers. Of additional interest is that anxiety decreased overall across all three camps while anxiety increased slightly, but not significantly, for the spina bifida patients.
Although the long-term outcomes of the camps were not conclusive, this does not imply that camps offer limited benefit, but rather reflects a lack of understanding of which factors affect a camper's experience, and which assessment tools are best able to capture longer-term outcomes. Quantitative tools allow for easier comparison but may miss the camper's lived experience and may be harder for younger children to understand.20,104,105 Qualitative interviews can better capture the personal outcomes that matter most to campers, but they may be less suitable for younger children with more limited language skills and are more difficult to generalize or compare with a control group. 20 Mixed methods may be best to capture camp effects. The fact that many qualitative interviews were conducted up to a year after camp, yet attendees still recalled the experience so fondly, suggests that camp can be a lasting positive experience for youth with PD.
Overall, findings from both qualitative and quantitative measures suggest that medical specialty camps for children with PD are positive environments. Youth enjoy traditional camp activities, form lasting friendships, and experience a sense of belonging. Some psychosocial improvements also appear to persist for several weeks to many months.
Camp demographics
The scope of this study focused on recreational camps and thus excluded numerous publications reporting on intensive therapeutic camps which served children with PD. This predominantly included studies on therapeutic techniques for children with hemiparesis and cerebral palsy.106–108 Although some of these studies did include psychosocial outcomes, such camps were excluded due to their emphasis on therapy over recreation. However, these programs still aim to be enjoyable for children, and have displayed psychosocial benefits.
Inclusion and exclusion criteria were not always easy to ascertain due to imprecise reporting of participant disabilities, sometimes grouping up to a quarter of participants in a general ‘other’ category.42,100,101,104 Similarly, there was sparse information available regarding campers’ race, ethnicity, and socioeconomic status, leaving the question of whether there is a discrepancy in access or psychosocial outcome based on these factors unanswered. The lack of reporting was sometimes a deliberate measure to maintain confidentiality due to the limited sample size, but in general this is an under-researched aspect of camps. When information was provided, minorities were underrepresented, a status also reflected in diabetes camps. 109 There may also be a higher proportion of middle- and upper-class representation at these camps, despite many of the camps being free or offering scholarships. Richmond et al. notes that cost is not the only barrier—transportation, childcare needs, and logistics such as proximity to home matter as well. 110 Blundell et al. reported that geography and childcare were barriers to families regardless of income. 111
The studies included in this review do not represent all PD, nor all specialty camps available to children. For example, only one study investigated the impact of camp experiences on children with limb differences, despite over 2000 individuals born with or acquiring such conditions each year in the US, and the existence of numerous limb difference camps, 112 such as Camp No Limits, which offers dozens of programs annually across the country. This review only represents camps and conditions that have had their psychosocial outcomes studied and reported in peer reviewed literature and is thus subject to any biases influencing which groups are investigated.
Studying these camps is important not only to understand their impact, but also because evidence-based outcomes can play a critical role in securing funding and sustaining program development. The more research that is published on the beneficial nature of medical specialty camps, the more justification an organization can have for proposing a new one. Similarly, stronger evidence of lasting psychosocial benefits could provide justification for supporting these camps as a valuable component of broader patient care. This may influence organizations and agencies involved in a child's care to endorse and facilitate participation.
With this in mind, an effective study in this field should be grounded in a specific conceptual framework and use well-validated outcome measures 113 It should also incorporate both qualitative and quantitative feedback. In addition, it should include comparisons with an able-bodied or non-camp control group, report demographic characteristics thoroughly, and assess long-term outcomes. Qualities of a good camp will include programming to support specific psychosocial outcome goals and a way to follow up with campers throughout the year. Knowledge of resources was cited as a significant barrier for camp attendance and continued growth. Therefore, providing lists of local resources for their patients from different regions may be a way for camps and hospitals to ensure that youth can keep participating in inclusive programs beyond the scope of the camp.
Camp inclusion
Medical specialty camps benefit from having low camper to counselor ratios, well-trained professional staff, and the adaptive tools needed to care for and involve campers of all levels of disability. Additionally, results indicate that being surrounded by youth who are experiencing similar health needs results in campers feeling accepted, safe, less alone, and more normal.14,32,44,48,114 Knapp et al. (2017) and Goodwin et al. emphasize the importance of camp segregation for children who often experience disability isolation. Parents also feel reassured that their child will be accepted, safe, and have peer support. 44 Other studies, however, indicate that integrated camp programs may also offer benefits, improving outdoor skills and social development in equal measure for children with and without disabilities, and helping able-bodied children develop greater understanding and respect for others.59,115 This effect could be seen in this review's family camps, where parents and siblings showed increased empathy and understanding for their family member with a disability, as well as with able-bodied camp staff who became more comfortable working with youth with disabilities. 33 Effective inclusive practices for non-specialized camps are elaborated upon by Brannan et al. (2002). 115
No study was found that compares the effects of children with disabilities going to a non-specialized camp versus a specialized camp. In other words, are the positive psychosocial effects a result of socialization and fun activities in general, or is a camp of peers a necessity to see those same improved outcomes? Gillard et al. came the closest to assessing this, by asking alumni of the camps to compare their medical specialty camp experience to other settings such as sports or support groups in retrospect. The study found that participants rated the camps to be highly influential compared to other settings in fostering a willingness to try new things, appreciation of diversity, and self-identity. However, they also found that the more experiences campers participated in outside of camp, the higher they rated camp's influence on outcomes. Baseline data directly comparing specialized to non-specialized camps is still a missing factor that could assist the field in understanding the mixed results that studies tend to find on camp outcomes, especially long-term. Both camp models appear to have clear benefits, and a camper's choice may depend on simple preference or availability.
Long-term maintenance
Gillard et al.'s survey taken many years after camp attendance pointed to some of the most lasting, memorable factors of a medical specialty camp experience. This may be a good place to start when considering which camp factors should be intentionally fostered to encourage lasting effects. Cushner-Weinstein's results following campers over three years of attendance suggested that repeated attendance may stack positive results, recovering psychosocial gains lost over the year. Similarly, Youngblood et al. shared that families noticed the positive impacts of camp declining when they missed camp during COVID-19, implying that effects may last up to a year but require regular reinforcement. Other reviews note that attending camp over a longer period of time may lead to enhanced psychosocial benefits for children. 20 Multiple papers emphasized the need for follow-up programs between camp sessions, and Dawson et al.'s (2021) mentorship program may help minimize the extinguishing effects of short-term programs and extend the benefits throughout the year. Another review article for chronic illness camps suggests that reinforcing the ‘camp philosophy’ during patient's regular clinic visits can facilitate long-term positive psychosocial change. 18 Taken together, these findings suggest that the benefits of camp are not only meaningful but potentially cumulative—strengthened through repeated participation and sustained through thoughtful follow-up. For camps to provide lasting psychosocial interventions, future programming and research should prioritize year-round engagement strategies and explore models that extend the camp's impact beyond its physical boundaries.
Limitations
The primary limitation of this review is that the database searching process was inherently biased to miss studies that research condition-specific camps due to a lack of consistent terminology use across literature. The keywords were kept broad to encompass as many camp-related research articles as possible, as attempting to search for every individual physical disability was considered to be unreasonable. However, it was for this reason that a large number of included studies were identified through scanning citations. This makes reproduction of the final set of 33 articles challenging, and also means that other relevant research may have been inadvertently omitted. Additionally, sources written in languages other than English may provide more insight that this review did not capture. Finally, data was extracted jointly by researchers rather than independently, which may lead to bias or error in results.
Conclusions
Medical specialty camps are places where youth with PD can enjoy typical camp experiences surrounded by peers experiencing similar health conditions. Most studies showed improvements in a range of psychosocial outcome measures, including self-esteem, quality of life, and self-perception, though long-term benefits remain elusive. Qualitative studies indicate that the most prominent themes of these camps are having fun, making connections, and feeling a sense of belonging and empowerment. The findings from this review reflect those seen in camps for youth with cancer, burns, and chronic illnesses, adding to the growing body of literature concluding that medical specialty camps provide a positive psychosocial impact for children with PD. Future research should focus on obtaining relevant control data, investigating accessibility factors to ensure equal access and outcomes, and pursuing follow-up programming to offset any diminishing long-term effects.
Footnotes
Acknowledgements
The authors would like to recognize the hard work that camp organizers and volunteers put in to make these camps a reality for kids with disabilities.
Ethical approval and informed consent
This study did not involve human participants or the collection of new data, and therefore ethical approval and informed consent were not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by NSF CAREER Award 2339965, NIH NIAMS T32 AR079099, NSF NRT Award 2152260, NIH 1F31HD118671-01, and NSF HCC Award 128621.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data supporting the findings of this review are available in the cited literature.