
Abstract
Female pelvic organ prolapse is a common condition associated with significant impact on women’s lives from a biopsychosocial perspective. The aim of this systematic review is to identify, appraise and summarize the biopsychosocial profile of women with pelvic organ prolapse. Searches were completed from inception to October 2022 from PubMed, Web of Science, EMBASE, CINAHL, Cochrane, PsycINFO and PEDro using a search string and in line with the Preferred Reporting Information for Systematic reviews and Meta-Analyses protocol. English language studies (randomized controlled trials, cohort studies, case–control studies, qualitative research) investigating female pelvic organ prolapse and using a validated patient-reported outcome measure and validated pelvic organ prolapse objective measurement were examined. Two reviewers independently screened titles, abstracts and full articles for eligibility. Data extraction included participant characteristics, pelvic organ prolapse grading and outcome measures. Risk of bias was assessed using the appropriate Joanna Briggs Institute Tool. Baseline mean score for each questionnaire or questionnaire domain in each category was presented in tertiles (low, moderate and high impact) to allow simple classification of impact. Of 8341 articles identified, 18 were included (n = 2075 women, age range = 22–85 years, parity range = 0–10). One objective outcome measure graded pelvic organ prolapse: Pelvic Organ Prolapse Quantification measurement. Eleven validated patient-reported outcome measures were utilized; two pelvic organ prolapse-specific (Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire, Pelvic Organ Prolapse Quality of Life Questionnaire), the remainder pelvic health (International Consultation on Incontinence Questionnaire–Vaginal Symptoms, International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form, Pelvic Floor Distress Inventory-20, Incontinence Impact Questionnaire-7, Female Sexual Function Index, Urinary Distress Inventory-6, Kings Health Questionnaire, Pelvic Floor Impact Questionnaire-7) or general health questionnaires (Short Form-36). Patient-reported outcome measures included in the review reported moderate levels of pain with sexual intercourse and low levels of bodily pain. Pelvic organ prolapse had a low to moderate impact in sleep/energy and quality of life and sexual function domains. Its impact on physical symptoms and general health perception domains was low. Patient-reported outcome measures results for physical functioning varied from low to high impact. More impact was demonstrated when using pelvic organ prolapse-specific patient-reported outcome measures. There are opportunities for improvement in the use of patient-reported outcome measures in clinical research which would facilitate increased understanding of the biopsychosocial profile of women with pelvic organ prolapse.
Keywords
Introduction
Female pelvic organ prolapse (POP) is defined by the International Urogynecological Association (IUGA) and International Continence Society (ICS) as ‘the descent of one or more of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix) or the apex of the vagina (vaginal vault or cuff scar after hysterectomy)’. POP symptoms are described as ‘a departure from normal sensation, structure or function, experienced by the woman in reference to the position of her pelvic organs’. 1
A broad range of symptoms are commonly reported including sensation of a bulge or fullness in the vagina, feeling ‘like a tampon is falling out’, pelvic pressure, groyne pain, low back pain, painful intercourse, difficult bowel movements, urinary or faecal incontinence, sexual dysfunction, 2 difficulty achieving orgasm and lack of vaginal sensation. 3
These symptoms have a significant impact on women’s lives from a biopsychosocial perspective 4 : impinging on sexual health, restricting daily and sports activities and affecting women’s ability to fulfil everyday parental duties. 5 Women report negative changes in body image,5,6 annoyance, frustration and irritation, unhappiness, depression, anxiety and sadness. 7 They also report feeling they were not listened to, given information or counselled on the options for treatment of their symptoms.2,7
A number of validated patient-reported outcome measures (PROMs) have been developed to quantify POP symptom bother. These PROMs assess quality of life (QOL), distress, bladder and bowel difficulties, vaginal symptoms and sexual function. Given the impact of biopsychosocial factors of POP on women’s lives, it is important that they are quantified and included in a battery of outcomes measures during surgical or conservative management of female POP.
This systematic review aims to identify, appraise and summarize the biopsychosocial profile of women with POP who participate in POP research. Previous enquiry has investigated the biopsychosocial profile of women with dyspareunia, finding more psychological distress, sexual dysfunction and relationship problems, 8 but to our knowledge, no research to date has examined the biopsychosocial profile of women with POP.
Methods
This review was carried out in line with the Preferred Reporting Information for Systematic reviews and Meta-Analyses (PRISMA) guidelines. 9 The review protocol was published in Prospero (CRD42021222457). The research question was elucidated using the Population, Intervention, Comparator and Outcomes (PICO) Framework as follows: population: adult women with POP; intervention: none; comparison: none; outcome: biopsychosocial factors such as pain, mood, sleep and QOL.
The review comprised four stages. In stage 1, following consultation with a medical librarian, a search of the electronic databases Cochrane, Embase, PubMed, CINAHL, PsycINFO and PEDro (from inception to October 2022) was made on 7 November 2022 using a search string (Supplemental Appendix 1). Inclusion criteria stipulated qualitative or quantitative studies written in the English language, published in peer-reviewed journals, on adult women, examining one or more biopsychosocial factors using a validated subjective questionnaire, who had not had prior pelvic surgery for POP and with a validated objective POP quantification system included.
Exclusion criteria were studies examining cancer, fistula and children. Studies that did not differentiate between subjects with a history of prior incontinence, POP surgery or hysterectomy were excluded as these surgeries may be associated with de novo post-op symptoms such as constipation, stress urinary incontinence (SUI) and overactive bladder (OAB), de novo POP in an untreated compartment, dyspareunia and possible increased risk of anxiety and depression after hysterectomy.10 –14
In stage 2, all studies were screened by title and abstract using the Rayyan systematic review platform by three blinded reviewers as per the inclusion criteria. 15 Where disagreements arose, a third person reviewed the potentially relevant paper. Full-text papers of included studies were reviewed. At this stage, in order to identify all studies of relevance, citation searching using bidirectional citation searching to completion (BCSC) was used. 16
In stage 3, study data were extracted from the research by one reviewer and checked by another. A data proforma was created to record author, year of publication country, study methodology, sample size, POP type and outcome measures used.
A second proforma recorded baseline data obtained in each study for all outcome measures used. If necessary, senior authors of potentially relevant studies would be contacted if data relevant to the review were not reported.
Questionnaires and components of questionnaires were summarized according to biopsychosocial categories. These categories were developed based on biopsychosocial factors that were most often screened for in the PROMs used. Baseline data from the studies (demographic information, i.e. age, body mass index (BMI) and parity as well as mean and standard deviation of questionnaire scores) were then screened and entered in the appropriate biopsychosocial category.
The biological category included pain (both bodily pain and pain specific to the abdominal, pelvic and vaginal areas) and sleep/energy. Although the authors recognize that physical functioning and the impact of physical symptoms can be strongly influenced by psychological and other factors,17,18 it was decided to include these categories under the biological domain. Emotions, QOL and general health perception were summarized under the psychological domain, while social functioning, relationships and sexual functioning were summarized under the social domain.
Interpretation of the included PROMs characteristics are summarized in Table 2. Baseline mean score for each PROM or PROM domain in each category is presented in tertiles (where low is <33%, moderate is 33%–66% and high impact is >66% of max possible score). For randomized controlled trials (RCTs), the pooled mean score and standard deviation (SD) were calculated for intervention and control groups at baseline.
In stage 4, studies meeting the inclusion criteria were critically appraised using the Joanna Briggs Institute (JBI) tool appropriate to the study design.19−21 and included as an appendix (Supplemental Appendix 2).
Results
Study selection
The initial search electronic search generated 6627 potentially relevant studies which were screened by title and abstract by two independent authors. During this phase, disagreements arose regarding n = 68 studies. Following review by a third researcher, 15 of these papers were subsequently included for full-text review. The full text of 334 potentially relevant studies was then screened by two independent reviewers.
Senior authors of 12 studies were contacted requesting further information. Two authors responded; both studies were subsequently excluded as they did not meet the inclusion criteria (participants without prior POP surgery). Studies carried out by authors who did not respond (n = 10) were excluded from the review.
Following full-text review, 20 studies fulfilled the inclusion criteria (Figure 1). Two studies were subsequently excluded during the data extraction stage as they did not include baseline data. Eighteen articles were included in the review after full-paper screening (see PRISMA diagram).

PRISMA diagram.
Study characteristics
The majority of studies were RCTs (n = 9), followed by cohort studies (n = 6 prospective, n = 1 retrospective) and case series (n = 2). No eligible qualitative studies were identified. Twelve of the studies compared either two interventions or an intervention and a control group (n = 2). Study characteristics are summarized in Table 1.
Summary of studies included.

POP: pelvic organ prolapse; PROMs: patient-reported outcome measures; BMI: body mass index; SD: standard deviation; RCT: randomized controlled trial; C: control; I: intervention; PFDI-20: Pelvic Floor Distress Inventory-20; UDI: Urinary Distress Inventory-6; PFIQ: Pelvic Floor Impact Questionnaire; ICIQ-VS: International Consultation on Incontinence Questionnaire–Vaginal Symptoms; FSFI: Female Sexual Function Index; PQOL: Pelvic Organ Prolapse Quality of Life Questionnaire; PISQ: Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire; IIQ: Incontinence Impact Questionnaire; SF-36: Short Form-36; KHQ: Kings Health Questionnaire; ICIQ-UI SF: International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form; ICIQ-SF: International Consultation on Incontinence Questionnaire–Short Form; CRADI-8: Colorectal-Anal Distress Inventory-8; POPDI-6: Pelvic Organ Prolapse Distress Inventory-6; N/A: not available; DDI: Defecation Distress Inventory.
Critical appraisal of studies
The Joanna Briggs Checklist for Randomized Control Trials was used to appraise RCTs, 19 for case series, the Checklist for Case–Control Studies 21 was employed, and the Checklist for Cohort Studies 20 was utilized to appraise cohort studies (Table 2 and Supplemental Appendix 2).
Summary of critical appraisal of included studies.

JBI: Joanna Briggs Institute; RCT: randomized control trial; SD: standard deviation.
For the RCT studies (n = 9), JBI scores ranged from 4 to 10 out of a maximum possible score of 13. The mean (95% confidence interval (CI)) score was 6.67 (5.47–7.87). RCTs with below average quality (56%, n = 5) had mainly methodological limitations, most often lack of blinding of treating healthcare professionals (HCPs), patients and/or outcome assessors.
For cohort studies (n = 7), quality JBI scores ranged from 7 to 9 out of a maximum score of 11 with a mean (95% CI) score of 7.7 (7.15–8.27). Those studies falling below average quality (43%, n = 3) were mostly due to issues regarding completeness of follow-up or failure to address incomplete follow-up.
The case series studies (n = 2) had a JBI Score of 7 where maximum possible score is 10; mean score (95% CI) = 7 (7–7). Lack of clarity regarding type of inclusion was an issue common to both studies.
Overall, 50.5% of studies were of below average quality when appraised. No studies were excluded on the basis of being categorized as low quality given the limited number of studies fulfilling the inclusion criteria and the reviewers did not want to present a restricted picture of the data. In addition, quality issues were more often due to blinding or completeness of follow-up rather than recruitment and selection; therefore, the reviewers considered the baseline data as generally good quality and somewhat comparable.
Patient characteristics
Age data from the complete sample of 2075 women from 18 studies was 22–85 years (mean ± SD = 60 ± 11 years). Parity of the women ranged from 0 to 10 children. Fifteen studies (1780 women) had complete data on parity with women having a mean of 3 children ± 3 overall. Where women’s BMI was reported (n = 13 studies, 1745 women) and their BMI was mean ± SD = 27.12 ± 4.61 (range = 19 to >40). A BMI of 25–29.9 is considered overweight, with BMI 20–24.9 considered healthy weight.
The majority of studies (n = 11 studies) did not specify the women’s menopausal status. Three of these 11 studies26,28,36 included data on age at menopause but were unclear regarding menopausal status of the sample. One study indicated whether participants were pre-menopausal, menopausal or post-menopausal 29 ; the remaining six studies23,25,30,35,37,39 indicated either pre- or post-menopause. Data on menopausal status were available for 897 women; overall 423 women were menopausal or post-menopausal and 409 women were pre-menopausal.
All studies included POP across different stages; POP stages II, III and IV (n = 10 studies); POP stages I and II (n = 1 study); POP stages I, II and III (n = 1 study); POP stages II and III (n = 3 studies); POP stages III and IV (n = 2 studies) and all five POP stages (n = 1 study). The questionnaires and components of questionnaires were summarized according to biopsychosocial categories (Table 3).
Baseline data summarized per biopsychosocial category.
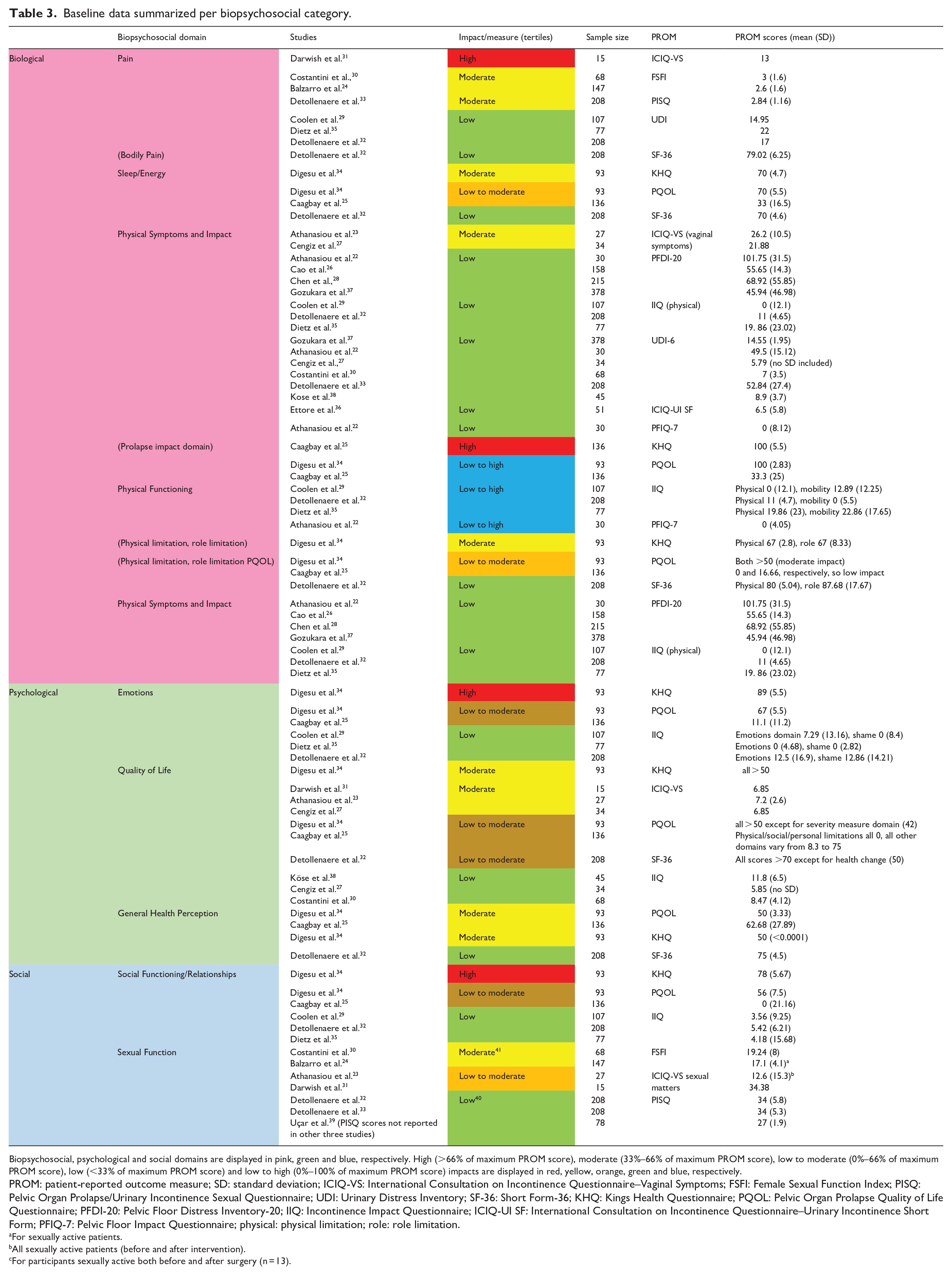

Biopsychosocial, psychological and social domains are displayed in pink, green and blue, respectively. High (>66% of maximum PROM score), moderate (33%–66% of maximum PROM score), low to moderate (0%–66% of maximum PROM score), low (<33% of maximum PROM score) and low to high (0%–100% of maximum PROM score) impacts are displayed in red, yellow, orange, green and blue, respectively.
PROM: patient-reported outcome measure; SD: standard deviation; ICIQ-VS: International Consultation on Incontinence Questionnaire–Vaginal Symptoms; FSFI: Female Sexual Function Index; PISQ: Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire; UDI: Urinary Distress Inventory; SF-36: Short Form-36; KHQ: Kings Health Questionnaire; PQOL: Pelvic Organ Prolapse Quality of Life Questionnaire; PFDI-20: Pelvic Floor Distress Inventory-20; IIQ: Incontinence Impact Questionnaire; ICIQ-UI SF: International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form; PFIQ-7: Pelvic Floor Impact Questionnaire; physical: physical limitation; role: role limitation.
For sexually active patients.
All sexually active patients (before and after intervention).
For participants sexually active both before and after surgery (n = 13).
Pelvic organ prolapse staging
Of the outcome measures used only POP stage (using the Pelvic Organ Prolapse Quantification System (POP-Q)) was uniformly assessed and reported (n = 18 studies). The POP-Q stage was reported in three ways: as a grouping of 2 or more stages (i.e. women with POP stage 2–4),27,30,31,34,37,38 separately reporting POP-Q stage for each compartment for each participant 23 or separately reporting the dominant compartment POP-Q stage.22,24 –26,28,29,32,33,35,36,39
It was therefore not possible to report on the numbers of the various prolapse stages except for those studies (n = 7 studies) who reported the dominant compartment POP-Q stage.22 –26,32,33,36 These studies included 1020 women; POP-Q stage 0 (n = 1 woman), stage I (n = 80 women), stage II (n = 434 women), stage III (n = 338 women) and stage IV POP (n = 167 women).
All included studies were investigating the effects of an intervention, mostly surgical repair; no study reported subjective outcome measures by POP-Q stage. All reported POP-Q and subjective outcome measures per intervention or control group or as a cohort, grouping all included POP-Q stages together.
Patient-reported outcome measures
Table 4 summarises the patient-reported outcome measures, their charac used in the included studies. Eleven validated patient-reported outcome measure questionnaires were utilized: two POP-specific (Pelvic Organ Prolapse/Urinary Incontinence Sexual Questionnaire-12 (PISQ-12), Pelvic Organ Prolapse Quality of Life Questionnaire (PQOL)), the remainder pelvic health (International Consultation on Incontinence Questionnaire–Vaginal Symptoms Module (ICIQ-VS), International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form (ICIQ-UI SF), Pelvic Floor Distress Inventory-20 (PFDI-20), Incontinence Impact Questionnaire-7 (IIQ-7), Female Sexual Function Index (FSFI), Urinary Distress Inventory-6 (UDI-6), Kings Health Questionnaire (KHQ), Pelvic Floor Impact Questionnaire-7 (PFIQ-7)) or general health questionnaires (Short Form-36 (SF-36)). In the case of the PFDI-20, some investigators used the complete symptom scale (n = 4),22,26,28,37 while others used the UDI subscale only (n = 7).27,29,30,32,33,35,38 Some focus primarily on physical symptoms experienced by participants; others explore QOL, emotional health and impact as well as physical symptoms; other questionnaires focus primarily on QOL and impact on the patient rather than physical symptoms.
Summary of patient-reported outcome measures used and their characteristics.


Shaded areas denote POP-specific PROMs.
PROM: patient-reported outcome measure; POPDI-6: Pelvic Organ Prolapse Distress Inventory-6; CRADI-8: Colorectal-Anal Distress Inventory-8.
Biological
Pain
Sixteen of the 18 studies (n = 1038 women) used a scale with a component (question or domain) that assesses pain.
Twelve studies used a questionnaire with a domain focusing on pain during sexual activity (FSFI, PISQ, ICIQ-VS, International Consultation on Incontinence Questionnaire–Short Form (ICIQ-SF)). Thirteen used a questionnaire investigating pain or soreness relating to the pelvis, abdomen or genital area: ICIQ-VS22,27,29,30,32,33,35,37,38 and UDI-6.23,27,31,36 One study used a questionnaire assessing bodily pain (SF-36). 32
Of the three studies using the ICIQ-VS (n = 128 women), two22,31 reported all three domain scores with Cengiz et al. 27 reporting on the VS and QOL domains only. Darwish et al. 31 also reported all items for each domain.
Overall, women with POP included in the studies reported moderate levels of pain with sexual intercourse (n = 3 studies, n = 423)24,30,33 and low scores with regard to bodily pain (n = 1 study, n = 208). 32 There was a wide distribution of pain rating in the pelvic, abdomen or genital area (measured by the UDI-6 and ICIQ-VS) ranging from low to high impact (n = 4 studies, n = 407 women).29,31,32,35
In the one study, which reported scores for the ICIQ-VS pain domain, women in the sample had a younger mean age 19 (38 years) compared to women in the other studies reporting on pain whose mean ages were all in the fifties and sixties.29,31,32,35 This study reported a high level of pain with POP; however, the study sample of 15 women was very small.
Sleep/energy
Sleep/energy was assessed in three studies (n = 437 women),25,32,34 using three PROMs (KHQ, PQOL and SF-36). Of these questionnaires, only PQOL is POP-specific; KHQ is a urinary incontinence(UI)–specific measure and SF-36 is a general health PROM.
SF-36 32 (n = 1 study, n = 208 women) showed a low impact of POP on sleep, with the PQOL (n = 2 studies, n = 229 women)32,34 and KHQ 34 (n = 1 study, n = 93 women) demonstrating low to moderate impact.
Physical functioning and limitations
Physical functioning was assessed in six studies (n = 726 women),22,25,29,32,34,35 using five PROMs (IIQ, PFIQ-7, PQOL, KHQ, SF-36). To determine impact on physical functioning, questionnaire domains investigating physical functioning or physical limitations were examined. One study used the PFIQ (n = 30 women). 22 It did not include subscale scores for physical and social function so was excluded.
Six studies used the IIQ27,29,30,32,35,38 and three of these studies reported a score for each domain.29,32,35 For the PQOL, KHQ and SF-36, the physical limitations or physical function domain (depending on the questionnaire) was examined. The IIQ incorporates a ‘physical functioning’ domain, while the PQOL and KHQ questionnaires include a ‘physical limitations’ domain. For all the questionnaires, higher score means higher impact on physical functioning, except for the SF-36 where lower scores indicate higher impact of physical functioning.
IIQ physical functioning scores ranged from low to high (n = 3 studies, n = 392 women).29,32,35 Scores for the PQOL (n = 2 studies, n = 229 women) and KHQ physical limitations domains indicated moderate impact (n = 1 study, n = 93 women), while on the SF-36, low impact was noted (n = 1 study, n = 208 women).
The SF-36 is a general QOL questionnaire and as such does not specifically capture information regarding pelvic dysfunction. Impact on physical functioning varied considerably between studies from low to high.
Physical symptoms and impact
Five PROMs reported both physical symptoms and their impact on activities of daily living (ADLs) and/or QOL (ICIQ-VS, PFIQ, PFDI-20, IIQ, UDI-6).23, 26−30,32,35,37,38 Some studies used the complete PFDI questionnaire and reported each subscale while others used the UDI-6 subscale only. Of studies using the complete PFDI scale (n = 4 studies, n = 789 women),22,26,28,37 two (n = 381 women)26,28 reported only a total PFDI scale score and two (n = 408 women)22,28 reported a score for each PFDI subscale. Eight studies (n = 815 women) used the UDI-6 questionnaire, with five (n = 182 women) reporting a UDI-6 total score22,27,30,37,38 and three reporting a score for each question in the UDI-6 (n = 392 women).29,33,35
Only two studies (n = 408 women) using the PFDI reported individual domain scores.22,37 The POP-specific Pelvic Organ Prolapse Distress Inventory (POPDI) domain scores for these studies indicated low to moderate impact of POP symptom distress. Total PFDI scores for all studies using PFDI are shown in Table 4.
Of the six studies using the IIQ,27,30,38 three reported a score for each domain,29,32,35 with the other three reporting total score only. IIQ domain and total scores are shown in Table 4. One study (n = 30 women) used PFIQ 38 and reported on Pelvic Organ Prolapse Impact Questionnaire (POPIQ), which is the POP-specific domain. This questionnaire indicating low impact of physical symptoms in women with POP.
ICIQ-VS (used in one study) 23 has three domains: vaginal symptoms and associated bother, sexual matters and associated bother and QOL. The vaginal symptoms domain was included in the assessment of physical symptoms and impact in this review.
The impact of physical symptoms was generally low (n = 11 studies, n = 1365 women)22,27 –30,32,33,35,37,38 with moderate impact of physical symptoms noted in the one study (n = 27) using ICIQ-VS, 25 which is more specific to vaginal symptoms than the other questionnaires used in studies which reported domain scores.
Psychological
QOL
Eight studies (n = 683 women)23,25,27,30 –32,34,38 using n = 5 PROMs assessed QOL or included a QOL domain (IIQ,25,27,30 KHQ, 21 PQOL,25,37 ICIQ-VS,23,27,31 SF-36 32 ). When assessing QOL profiles, overall total scores of QOL questionnaires (IIQ, KHQ, PQOL and SF-36) were used, as well as the QOL domain of the ICIQ-VS. Results (shown in Table 4) demonstrate a low to moderate effect of POP on QOL at baseline.
General health perception
General health perception was examined in three studies (n = 437 women),25,32,34 using three questionnaires (PQOL,25,34 KHQ, 20 SF-36 32 ). Impact on general health perception was found to be low to moderate as shown in Table 4.
Social
Social functioning
Social functioning was assessed in five studies (n = 621 women)25,29,32,34,35 using three questionnaires (PQOL,25,34 IIQ,29,32,35 KHQ 34 ). Impact was found to be low or moderate on the PQOL and IIQ (n = 5 studies, n = 621).25,29,32,34,35
One study 34 (n = 93 women) using the KHQ found impact on social functioning to be high. This would seem contradictory in that the same n = 93 women demonstrating moderate impact on the PQOL were shown to be highly impacted on the KHQ questionnaire. As the KHQ is a UI-specific questionnaire, this may indicate that these women were more impacted by urinary symptoms associated with POP than by the POP itself.
Sexual function
Sexual functioning was assessed in nine studies (n = 873 women)23,24,26,28,30−33,39 using three questionnaires (FSFI,24,30 PISQ26,28,32,33,39 and ICIQ-VS sexual matters domain23,27,31). Two studies26,28 did not report PISQ scores. PISQ scores for the remaining three studies (n = 494 women) generally reported low impact of POP on sexual function, while the FSFI (n = 2 studies, n = 215 women) found moderate impact. The ICIQ-VS (n = 3 studies, n = 128 women) reported low to moderate impact. Overall, low to moderate impact of POP on sexual function was reported.
Discussion
To our knowledge, this is the first review undertaken with the aim of systematically identifying, appraising and summarizing the biopsychosocial profile of women with POP participating in clinical research. Eighteen quantitative studies were identified: nine RCTs, seven cohort studies and two case series. Study design (especially for the RCTs) while generally pragmatic poses problems in terms of assessing outcomes in women with POP depending on their POP stage. Most included studies recruited women with a range of POP stages and reported PROM total scores rather than per stage.
Collecting and reporting PROMs per stage of POP could establish biological, psychological or social domains which may influence symptom bother in women with POP. Stratification could also be useful also to predict prognosis; research has shown that women with POP stage I and II (and possibly stage III) may respond well to conservative treatment, with most studies reporting improvements in bothersome POP symptoms.42,43 Other research has reported that individuals with cognitive or sensory impairment (CSI) compared to those without are more likely to have post-surgical complications or poor outcomes.44 –46
Predicting which variables affect patient response to interventions for POP may guide the introduction of effective biopsychosocial interventions as an adjunct to traditional POP treatment and help to enhance effective conservative care pathways for women with POP, reducing waiting times for assessment and treatment of women who require surgical intervention. It may also help to identify women who are at increased risk of poor outcomes, particularly post-surgery. This is important given between 19% and 48% regression of stage 1 and 2 prolapse without intervention over 3–8 years. 47
Studies in the current review incorporated women with a broad age range (from 22 to 84 years). It is widely accepted that POP increases with age, with one-third of women with symptomatic POP aged 50–59 and half aged 80 years or older. 48 This means younger women with symptomatic POP are likely under-represented in the sample.
Physical factors, environment and levels of activity among women are likely to differ with age. Younger women are reported as being more likely to be engaged in sports but have described caring for small children as a barrier to exercise. Women between the ages of 60 and 69years are more likely to take regular exercise than younger women, while a general decline in physical activity and social engagement has been observed among older women (over age 70 years).49 –52 Therefore, differences in type and level of bother associated with POP might be expected. Reporting PROMs by age as well as stage or time living with the condition seems sensible to better interpret impact and adaptation to the perceived limitations. Further research is needed to investigate potential differences in POP impact in women of differing ages.
There was a wide distribution of abdominal, genital and pelvic pain rating in women across the studies included in the review. This may be because while one PROM used (ICIQ-VS) is specific to the evaluation of vaginal symptoms, the other (UDI-6) is UI specific, asks only one question about pain and therefore may not capture pain data for all women with POP-associated pain. Many HCPs are taught that women with POP tend to present with symptoms of bulge or pelvic pressure and rarely with pain, 53 and some research has found that low back and pelvic pain are not associated 54 ; however recent studies have identified pelvic floor myofascial pain (PFMP) as a possible contributor to patient-reported POP symptoms.55,56 A recent systematic review recommended standardized physical vaginal examination of pelvic floor muscles to detect tenderness be utilized to detect PFMP in the absence of a questionnaire designed to identify PFMP. 55 The development of a questionnaire is also suggested. 57 Further research is required to elucidate the role of PFMP in POP symptom bother, particularly in women with grades I and II POP reporting severe symptom bother.
The International Classification of Functioning, Disability and Health (ICF) model includes environmental and personal factors, as well as disease-related factors as important in how disability is experienced by an individual. 58 The ongoing development of core outcome sets for the assessment of POP currently being undertaken by CHORUS and including input from HCPs, researchers and women with lived experience of pelvic floor disorders should include measures to assess all aspects of POP impact, particularly psychosocial, to reflect the significant impact of psychosocial factors in patient coping and response to treatment in other health conditions. 59
This review suggests that condition-specific PROMs may be more likely to demonstrate impact in some areas; for example, in studies using a PROM assessing general health perception, the two condition-specific PROMs showed moderate impact of POP on general health perception, while the generic PROM indicated low impact. This may indicate that because of low levels of knowledge, a societal culture of acceptance, trivialization of symptoms by HCPs and successful adaptation to their impairment, many women consider pelvic health issues to be a normal consequence of childbirth or an inevitable result of the ageing process60 –62 and therefore do not consider pelvic health issues an important aspect of general health unless it is specifically asked about.
On the contrary, PROMs which are too specific may fail to highlight important biopsychosocial impacts of the wide range of symptoms which may accompany POP, for example, UI. In the current review, some POP-specific PROMs demonstrated low to moderate social impact of POP. This contrasted with UI-specific PROMs which indicated a greater negative social impact of UI. This may demonstrate that additional urinary and other symptoms related to POP are more socially impactful than symptoms typically associated with POP, such as vaginal bulge and pressure.
There is a very small body of research to confirm this hypothesis; Porto et al. 63 observed strategies to manage UI and UI-related beliefs were significant predictors of social isolation. Self-stigmatizing beliefs have been shown to result in people with UI concealing their condition from family, friends and HCPs, thus cutting themselves off from potential support of their social circle. 64 In addition, people suffering from UI have reported reducing social interactions because of fear and embarrassment regarding potential odours associated with urine leakage. 65
Improved biopsychosocial profiling of women participating in POP research is needed to elucidate the possible impact of various factors including sleep, pain, central sensitisation, mood, general health perception, health literacy and physical and social function as well as others on the experiences of women with POP and their prognosis with conservative and surgical POP interventions.
Clinical implications of this review
This review suggests that consideration of the biopsychosocial context of POP may be useful to guide treatment choice, predict prognosis and identify women with POP at risk of poor treatment outcomes.
Limitations
This review could only profile women based on the biopsychosocial variables investigated in the PROMs used in the included studies. Because the inclusion criteria stipulated the use of an objective and subjective validated measurement tool, no qualitative studies were included in the review. Qualitative research may have captured more biopsychosocial domains that are not included in the PROMs used in the quantitative research.
Studies were carried out on several continents and countries. This raises a question of ethnic, cultural and healthcare system differences which may influence women’s reporting of POP and POP symptoms.66–68
The studies included in the review are mainly RCTs and intervention-based cohort studies. This means that the sample of women in the review had sought treatment for their condition. Although the RCTs included control groups, in many cases, these were women receiving a different type of surgery or intervention, not necessarily women with POP receiving no intervention. In addition, the recruitment of women mainly from tertiary care and from populations either considering or awaiting surgery is a consideration when interpreting patient-reported outcome measures, as symptom distress has been shown to increase the likelihood of women to opt for surgical management. 69
Therefore, there may be a bias in this review towards women who experience more bother from their symptoms.
Conclusion
This systematic review highlighted opportunities for improvement in the use of PROMs in POP clinical research, in particular the agreement on a set of PROMs to be used, incorporating PROMs measuring psychosocial domains such as mood, health perceptions, sleep and physical and social functioning, choosing disease-specific tools over generic tools to measure health-related quality of life (HRQL) and disease-specific physical functioning and stratified reporting by POP stage and age groups.
This comprehensive review also identified areas of knowledge gaps including the understanding of sleep disturbances in women living with POP as well as the role of PFMP in POP symptom bother.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231181012 – Supplemental material for Biopsychosocial profile of women with pelvic organ prolapse: A systematic review
Supplemental material, sj-docx-1-whe-10.1177_17455057231181012 for Biopsychosocial profile of women with pelvic organ prolapse: A systematic review by Louise Carroll, Cliona O’ Sullivan, Carla Perrotta and Brona M Fullen in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231181012 – Supplemental material for Biopsychosocial profile of women with pelvic organ prolapse: A systematic review
Supplemental material, sj-docx-2-whe-10.1177_17455057231181012 for Biopsychosocial profile of women with pelvic organ prolapse: A systematic review by Louise Carroll, Cliona O’ Sullivan, Carla Perrotta and Brona M Fullen in Women’s Health
Supplemental Material
sj-docx-3-whe-10.1177_17455057231181012 – Supplemental material for Biopsychosocial profile of women with pelvic organ prolapse: A systematic review
Supplemental material, sj-docx-3-whe-10.1177_17455057231181012 for Biopsychosocial profile of women with pelvic organ prolapse: A systematic review by Louise Carroll, Cliona O’ Sullivan, Carla Perrotta and Brona M Fullen in Women’s Health
Footnotes
Acknowledgements
The authors thank Catherine Doody (Associate Professor, School of Public Health, Physiotherapy and Sports Science, University College Dublin) for her guidance in carrying out this review.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.