
Abstract
PURPOSE:
Snoezelen is an environment that provides sensory stimulation to individuals in health care and rehabilitative settings. With the presentation of various instruments and materials, individuals can encounter a range of sensory experiences including visual, tactile, and auditory with the purpose of inducing relaxation and restoration. Little is known about how children and adolescents experience this form of sensory stimulation, particularly those in complex continuing care who may have limited verbal and mobility capacity.
METHODS:
This pilot study examined autonomic physiological responses and observational data on five children and adolescents in complex continuing care within a large rehabilitation hospital. Responses to Snoezelen and watching television were compared against baseline data collected during pre-intervention phases.
RESULTS:
Using a single-subject design, this preliminary study found that individual participant responses varied considerably. Four of the five participants exhibited significant changes between sessions on one or two distinct physiological measures. The authors call on additional studies that apply unique and multiple methods capable of accessing the preferences of children and adolescent in rehabilitative care.
CONCLUSIONS:
As an outcome, contributions to evidence-based practice can be made while supporting children’s participation rights in health care decision making.
Introduction
Snoezelen,1
Snoezelen
Most research about Snoezelen focuses on adult participants with developmental delays and various forms of dementia, although the findings from this body of research are inconsistent. According to some studies involving adults with developmental disabilities, Snoezelen is associated with decreases in challenging behaviours [9, 10, 11]; others have concluded that Snoezelen does not reduce challenging behaviours but does promote positive affect and relaxation [12, 13, 14]. Some studies have reported that Snoezelen has a positive effect on the mental states and comportment of persons with dementia [6, 15, 16, 17, 18]; others have found that Snoezelen has minimal or no effect on mood and behaviour among dementia patients [19, 20].
Very little research has focused on multisensory therapy for children. Some studies involving children with intellectual disabilities have suggested that multisensory interventions can help lower the number and duration of stereotypic self-stimulating [21, 22] and increase the incidence of appropriate responsive and interactive behaviours [22]. Other studies involving children undergoing or recovering from medical procedures have reported that Snoezelen can reduce physiological arousal, agitation, and anxiety [5, 23] and induce relaxation [24].
Researchers have observed extensive variation in individual responses to Snoezelen, and have recommended assessing individual needs and preferences when determining appropriate exposure to the multisensory environment [2, 3, 25, 22, 10, 14, 8, 21, 26]. Moreover, as some researchers have noted [27, 23], it is not yet clear whether specific elements of the Snoezelen room are linked with the observed benefits, highlighting the need to clarify which aspects of multisensory therapy work best and for whom.
Patient self-expression and empowerment are at the core of Snoezelen therapy [8]. This is a particularly salient issue for children with varying disabilities and medical conditions who are regularly exposed to this intervention. It is their perspectives and preferences that should inform clinical choices for therapeutic interventions. By attempting to examine the use of Snoezelen for children with complex medical conditions from their perspective, we are supporting children’s right to participate in decisions regarding their health care.
This pilot study was conducted to address the lack of research about Snoezelen therapy for children and to profile a population that, to our knowledge, has not yet been the focus of research in this area: children who require complex continuing care in a hospital setting. The available literature about Snoezelen suggests that the multisensory environment should be tailored to the specific needs of each individual, which makes ascertaining those needs an essential step in the therapeutic process [2, 3, 8, 22]. Because children in complex continuing care often have limited verbal and physical abilities, one important aspect of the present study was attempting to ascertain responses from a group who do not communicate through traditional channels.
Snoezelen enables patients to actively regulate their engagement by choosing from a myriad of sensory experiences that can be manipulated, intensified, or reduced according to the individual’s needs and preferences [28]. Snoezelen is an important feature of psychosocial care for children with complex medical conditions because it is an exercise in self-determination and decision-making in a context of otherwise limited control [9]. Research has revealed that empowering children and adolescents in their own health care is beneficial, especially when information is presented in a way appropriate to their abilities and developmental level [29, 30, 31, 32]. To date, relatively few studies have acknowledged the importance of considering the perspectives of children and adolescents about their health care experiences [33, 34]. The right of children to participate in decision-making is increasingly informing clinical approaches, so it is vital that researchers and practitioners seek the views of all children, including children who have difficulty articulating their opinions.
Guided by this philosophy of patient-centred and patient-directed care, the present study was conducted to determine: 1) the effects of Snoezelen, as manifested in physiological and behavioural changes, on children and adolescents in complex continuing care; and 2) whether these effects are unique to the Snoezelen experience rather than common to other audiovisual stimuli (e.g. watching a favourite TV show).
Study design
Setting and participants
This study was conducted at a large pediatric rehabilitation hospital in a major Canadian city. The hospital is a treatment, research, and education facility serving children with a variety of disabilities, including acquired brain injury, amputation, arthritis, cerebral palsy, cleft lip and palate, epilepsy, muscular dystrophy, spina bifida, autism and other developmental disabilities. The hospital also provides services to a small number of children with complex chronic diseases who reside in the Complex Continuing Care unit, which provides 24-hour medical attention.
Patients were selected for the study according to the following inclusion
criteria: between the ages of 5 and 18 years; awake or minimally sedated based on
standardized scales (Glasgow Coma Scale
Participants comprised five children and adolescents (aged 6–17 years) receiving complex continuing care at the hospital. Their diagnoses included traumatic brain injuries, chromosomal disorders, and refractory status epilepticus. Participants had been hospitalized for extensive periods, ranging from eight months to five years. They all required around the clock medical attention and could not perform self-care tasks independently. Four of the five participants had a tracheostomy and required constant care and suctioning. None of the participants were mobile and they spent most of their time in bed or sitting in a chair. Previous research has stressed the need to allow participants to become acclimatized to multisensory therapy before assessing its effects [3]; all of the participants in this study had previously been exposed to Snoezelen. For reasons of care, all of the participants received multisensory therapy at the bedside.
Design
Due to the limited accessibility of this target population and the criteria for participant inclusion, the study followed a single-subject design, so that each partici- pant acted as his/her own control. The order of interventions was counterbalanced for each participant (see Table 1). Participants were exposed to the two protocols (AB and BA) on separate days within the span of two weeks. The decision to use a single-subject design was based on similar research with this patient population [35], and due to the variability among our participants. Children in complex continuing care constitute a diverse population with widely divergent needs [36], which makes it difficult to compare groups.
Measures
Demographic information was collected from all participants; this included age, gender, diagnosis, developmental considerations, duration of hospital stay, previous Snoezelen exposure, and sedation scores prior to intervention (see Table 2).
Participants’ demographic information
Participants’ demographic information
Because participants were not able to communicate verbally, we chose to record physiological and behavioural indicators as representations of patients’ responses to the stimuli presented as opposed to simply making inferences regarding their preferences. The T7500M ProComp Infiniti System with BioGraph software recorded physiological data through sensors attached to the fingers and one band placed around the chest. Four autonomic nervous system (ANS) responses were measured: blood volume pulse, electrodermal activity, skin temperature, and respiration. Emerging evidence suggests that these components of the ANS are reliable indicators of affective state in healthy populations [35, 37]. Because the reliability of this method has not yet been established for participants with disabilities or medical conditions, we complemented these physiological data with observational data.
For the observational component of the study, one of the first two authors documented each participant’s consciousness, behaviour, facial expression, and activity level. These data were collected using an instrument adapted from two scales specifically designed for research involving multisensory therapy [38, 39]. In order to ensure a level of content validity between the two scales, the adapted version was shared with two individuals with extensive experience administering and coordinating the use of Snoezelen within the facility. Following other research in this area [40, 41], we relied on cues such as vocalizations, physical gestures, and visual fixation to gauge the preferences of participants. Observations were recorded within 20-second windows during each intervention phase of the study, for a total of 30 observations per intervention period.
The two lead authors and a research assistant (RA) conducted the data collection. The first and second authors alternated in collecting observational data and monitoring the recording of physiological data, while the RA managed the biofeedback equipment. The resident Child Life Specialist (CLS), who was familiar to all participants and regularly provided them with Snoezelen therapy, administered the interventions.
The RA began each session by affixing the four physiological sensors to the participant’s hand. The CLS instructed the participant to remain as still and relaxed as possible for the five-minute pre-intervention window. At this point, the RA would start the ProComp Infiniti System to begin recording physiological signals and initiate the appropriate protocol.
Three pieces of Snoezelen equipment used in this study. Fibre-optic light sprayset
(left), massage tube (middle), and interactive bubble tube (right).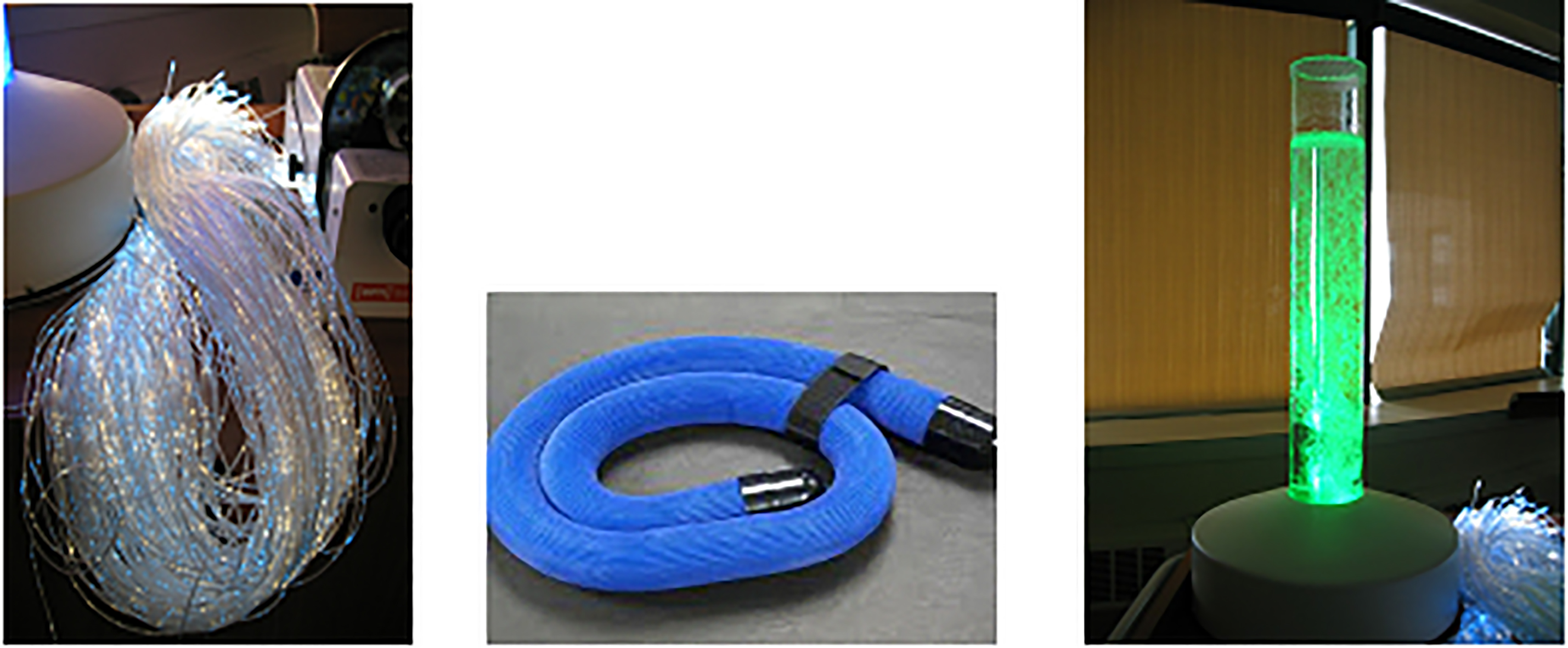
Difference between sessions AB and BA
Black
For the TV sessions, the CLS presented the child with a preferred TV program (informed by a knowledgeable caregiver). They watched the TV program together for 10 minutes without interacting. For the Snoezelen sessions, the CLS brought the Snoezelen cart to the participant’s bedside and introduced five commonly used Snoezelen items in the following order: stereo/CD player, solar effect wheel and projector, interactive bubble tube, fibre-optic set, and massage tube (see Fig. 1). Items were presented one at a time and then left on, so that by the end of the intervention window, the patient was exposed to all five pieces of equipment simultaneously. The participant had the opportunity to interact with the items for 10 minutes, after which the CLS removed the equipment. Some participants appeared to prefer some pieces of equipment, as suggested by their holding on to an item as other items were introduced, or by their active manipulation of the equipment. The CLS guided each participant through the transition between sessions by asking him or her to relax for five minutes during the post-intervention window and then for another five minutes prior to beginning the second intervention. Once the post-intervention data had been collected, the RA removed all sensors from the participant. Observations were conducted away from the bedside, and the researchers interacted as little as possible with the participant while the protocol was being carried out.
Physiological data
The approach used to analyze physiological data followed the same method used in a similar study conducted on the same population in Kingsnorth et al. [36]. First, the raw autonomic physiological signal analysis took part in two stages: splicing, and pattern comparison. During the splicing stage, all four physiological signals (blood volume pulse (BVP), electrodermal activity (EDA), skin temperature and respiration) were visually inspected for artifacts. Every second of recorded data were used for each physiological category.
As the analysis requires valid recordings from all physiological sensors, sections where signals from any one sensor were contaminated were removed. Subsequently, data were spliced into 6 different segments:
Pre-intervention 1: time preceding the first intervention
( Intervention 1: time during the first intervention
( Post-intervention 1: time following the first intervention
( Pre-intervention 2: time preceding the second intervention
( Intervention 2: time during the second intervention
( Post-intervention 2: time following the second intervention
(
During the pattern comparison stage, a model of the participant’s resting physiological state was generated from the pre-intervention data and this was designated as the baseline model. Subsequently, each second of data generated during intervention and post-intervention were compared against the baseline model. If the second (e.g. 1 s) of data fell within model, the participant was considered to be in a resting physiological state. If the second of data fell outside of the model, this datapoint was considered an outlier or a salient feature and was characterized using two variables: magnitude and direction. Magnitude measured the distance of the outlier from the model – the greater the magnitude, the greater the difference in physiological pattern from the baseline state. Direction measured which physiological signals were most responsible for the outliers – specifically, the average contribution of each physiological signal to each outlier were calculated. For example, the average direction of change in heart rate would be considered a salient feature [36]. Finally, the total number of outliers was calculated. Comparisons were always made with respect to the baseline model immediately prior to the intervention (e.g. intervention 2 was compared against pre-intervention 2, intervention 1 was compared against pre-intervention 1).
Following the completion of the splicing and pattern comparison, a within-case design was used for statistical analyses of the physiological data for each participant. GraphPad InStat 3 software was applied to assess whether significant differences appeared in any of the four physiological measures during TV and Snoezelen interventions relative to baseline relaxation levels. The alpha level was set at 0.05. Paired t-tests were used to determine whether the mean of a variable differed between TV and Snoezelen conditions for each participant. Analyses explored the number of outliers (scores that fell outside the baseline average), blood volume pulse (BVP), electrodermal activity (EDA), skin temperature (Temp), and respiration (Resp).
Differences between TV and Snoezelen interventions relative to baseline
Differences between TV and Snoezelen interventions relative to baseline
Black
Differences following TV and Snoezelen sessions
Black
Difference between sessions AB and BA. To determine
whether the order of interventions was associated with physiological changes, each
participant’s responses during Session AB were compared with his or her responses during
Session BA (see Table 3). No significant
differences were found for Participant 1. Significant differences
(
Difference between TV and Snoezelen interventions relative to
baseline. For each participant, the two sessions of TV (AB
Difference following TV and Snoezelen interventions. To
explore what kind of physiological state was induced in participants following exposure to
the interventions, we compared post-intervention rest periods for two sessions of TV (AB
In an attempt to collate behavioural responses, observational data were categorized as positive (smiling, alert, engaged) or negative (crying, upset, withdrawn). Descriptive statistics were used to aggregate data across participants and paired t-tests were conducted to reveal behavioural differences between exposure to TV and Snoezelen. Table 6 provides a descriptive overview of all the coded behaviors and associated number corresponding to the intervention (TV versus Snoezelen).
Number of responses per behavior where one intervention showed greater
incidence
Number of responses per behavior where one intervention showed greater incidence
Positive behaviours observed during TV and Snoezelen.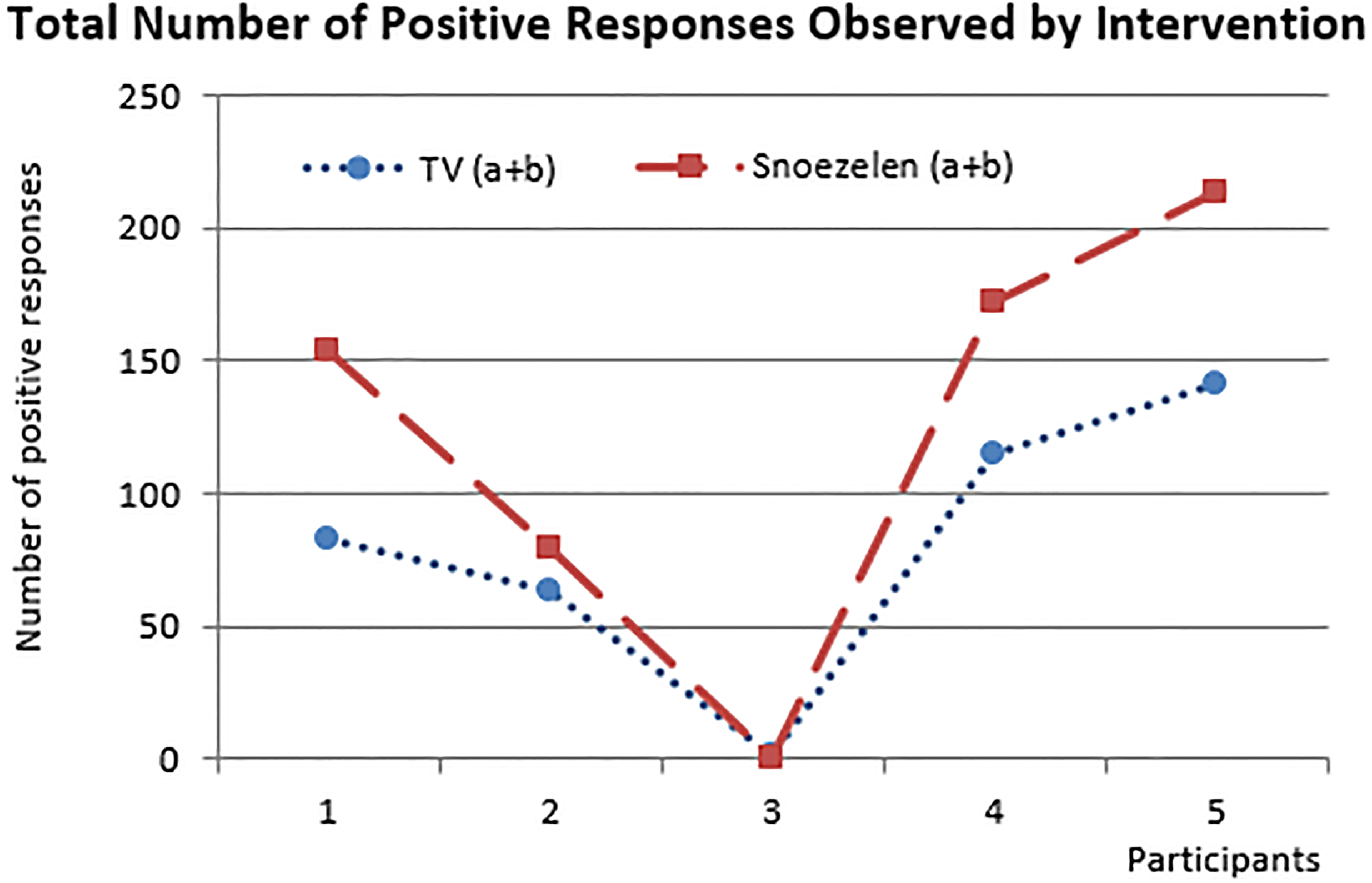
Negative bahaviours observed during TV and Snoezelen.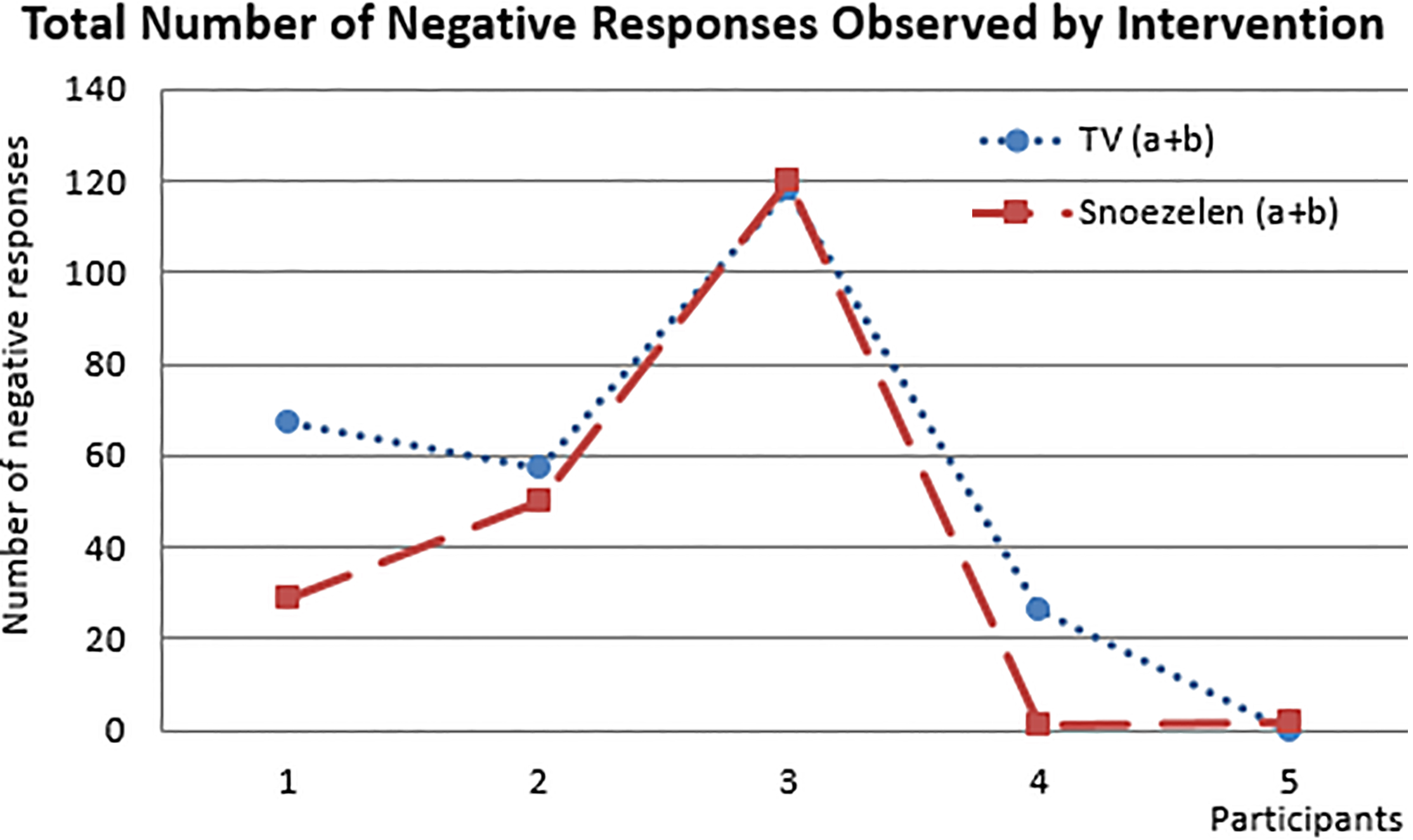
Total number of positive responses observed intervention.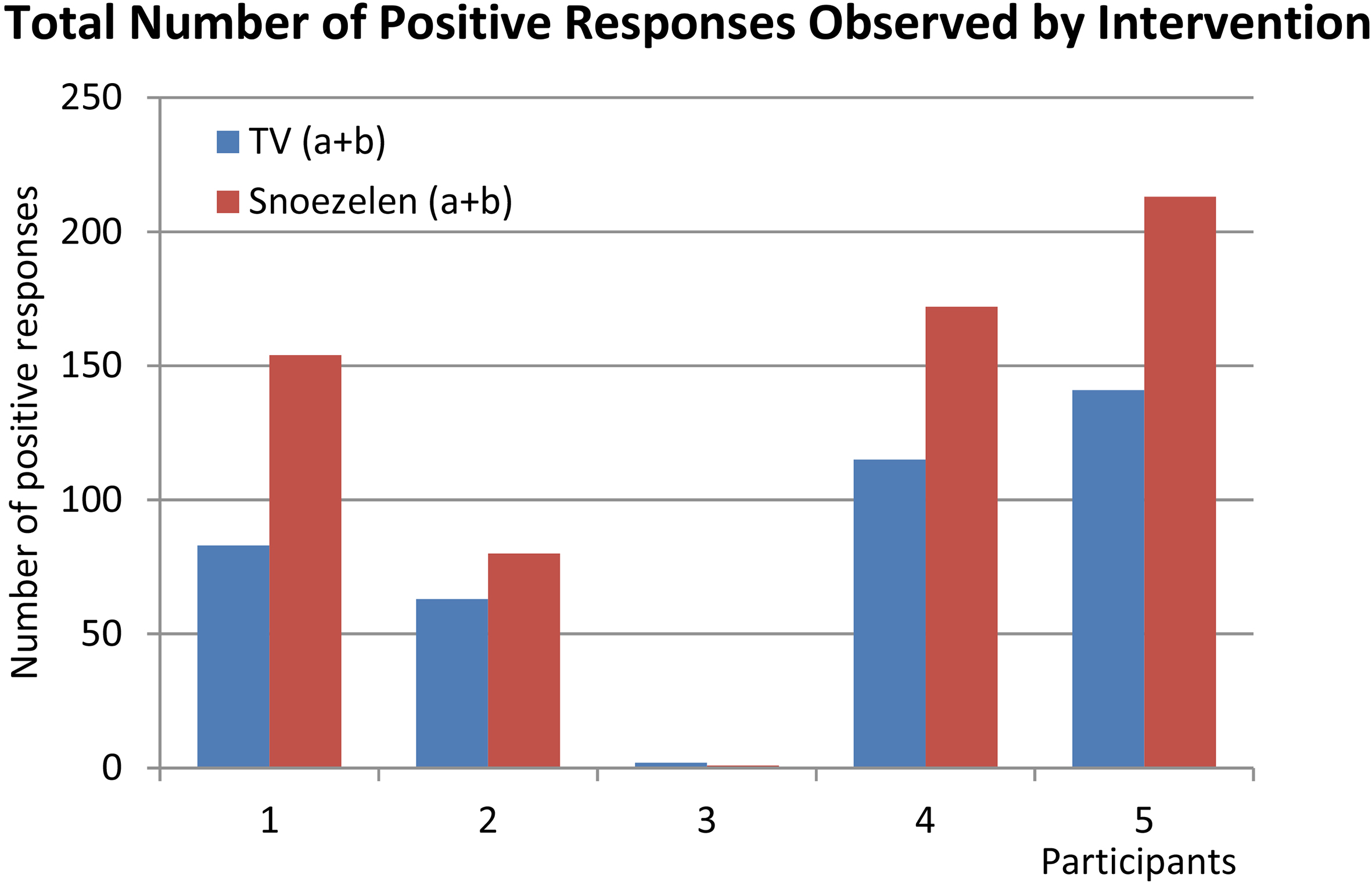
Using an alpha level of 0.05, the paired t-test results revealed a
significant difference in positive behaviours between participants watching TV (M
Based on the raw scores, Participants 1, 2, and 4 displayed more negative
behaviours during TV than during Snoezelen. The reverse was true for Participants 3 and 5:
slightly fewer negative behaviours were recorded during TV than Snoezelen (see Fig. 3). However, using an alpha level of
0.05, the paired t-test results revealed no significant differences in negative behaviours
between participants watching TV (M
This pilot study examined the physiological and behavioural responses to Snoezelen and TV of five children and adolescents receiving complex continuing care in a Canadian rehabilitation hospital. It was evident that no two participants exhibited the same patterns or combinations of physiological signals and observed behaviours. A wide range of responses is consistent with the findings of other multisensory therapy research involving children. For example, Shapiro et al. [21] found that, compared with time spent in a regular playroom, Snoezelen sessions produced greater changes in participants’ heart rates, which increased in some participants and decreased in others.
In the present study, four of the five participants exhibited significant changes between sessions on one or two physiological measures. This finding suggests that the order of the interventions, rather than the particular intervention, may influence how individual patients respond, or that responses may change over time. It is possible that participants’ alertness and activity levels varied depending on the time of day or the day of the week.
Two of the five participants displayed significant physiological changes during Snoezelen relative to baseline levels, while no participants displayed significant changes during TV relative to baseline levels. The changes recorded during Snoezelen consisted of a change in blood pressure for Participant 2 and a change in skin temperature for Participant 4. In healthy populations, lower blood pressure signals a reduction or lack of stress, while cooler body temperature is associated with increased stress [42]. At the same time, lower blood pressure has been linked to lower levels of enjoyment, while cooler body temperature has been associated with higher levels of enjoyment in healthy populations [43]. While it is difficult to determine which affective states these physiological signals represent in the case of our participants, these findings underscore the variability of responses to Snoezelen.
Participant 2 also exhibited a drop in skin temperature following Snoezelen and was the only participant to display a significant change in autonomic arousal following either intervention. It is worth noting that Participant 2 experienced a drop in blood pressure during Snoezelen and a drop in temperature following Snoezelen; based on the psychophysiological model of stress outlined above, it is possible that while the intervention itself was not necessarily stressful, its termination may have been.
In summary, the behavioural responses to Snoezelen were significantly more positive than watching TV for four out of five participants. No significant differences appeared in the number of negative responses observed for each intervention. Finally, a comparison of the physiological and behavioural results revealed that one set of data do not necessarily predict or correspond to the other. For example, Participant 1 exhibited no significant physiological changes between sessions, between interventions, or following interventions, but displayed more positive and fewer negative behaviours during Snoezelen than during TV. This finding illustrates the importance of employing multiple methods of data collection to ensure a more comprehensive assessment of intervention-related outcomes.
Study context and limitations
The small sample size of the present study is suitable for an exploratory investigation of this kind [44, 45], but it also reflects the unique considerations of having children with complex health care needs involved in research. While measuring physiological responses, the researchers needed to navigate and bypass intravenous, feeding, and ventilating tubes, as well as monitor their own equipment. The spastic movements of some participants made it difficult to obtain comprehensive readings when sensors from the biofeedback equipment were displaced and had to be restored and secured. Finally, frequent interruptions from nurses and physicians further impeded the data collection process.
Additional challenges with conducting this research involved the scheduling of administering protocols on different days – usually within the same two weeks. Competing demands between the researchers, parents and the health care providers made it difficult to find mutually convenient times. There were also instances when the child participant was tired, medicated, sleeping or not feeling well, and this required re-scheduling of the visit. Although we would have preferred more opportunities to administer the protocols to patients over longer periods of time, ethics approval for more sessions would have been difficult to achieve.
The physiological changes that occurred during Snoezelen can be interpreted in several ways. For example, if arousal decreased with exposure, this could indicate that patients were adjusting to the experience and becoming more comfortable and relaxed in the environment; alternatively, it could indicate that Snoezelen was not providing sufficient or appropriate stimulation to keep them engaged. We tried to minimize this ambiguity by recording baseline levels of arousal and observing the behaviour of participants.
The ability to make accurate assessments of the child’s experience is further confounded by the inability to verbally ask the child how he or she is experiencing the stimulation. In a population with poor motor control, changes in behaviour are also open to interpretation. For instance, it can be difficult to distinguish between a smile and a grimace or between a spasm and a reaching gesture. This challenge can be addressed through the presence of a family member or health practitioner who knows the patient’s habitual repertoire of behaviours and can identify any deviations from this pattern. In the present study, the child life specialist (CLS) was able to assess the reactions of the participants because she routinely engaged with the patients when providing psychosocial care. For example, it is difficult to assess why several of the patients preferred the use of fibre-optic cables during their Snoezelen sessions.
Although the CLS ensured the safety and comfort of participants during data collection, her presence was also a potential confounding variable. Some researchers have suggested that the reported benefits of Snoezelen may be related to the increased interaction with staff members within this setting, as opposed to the Snoezelen equipment itself [4, 27, 46, 26]. The participants in this pilot study visibly responded to the arrival of the CLS even before she started administering the interventions. The CLS engages patients in leisure activities and provides attention, comfort, and support; these positive associations could have influenced the responses of participants during the sessions. One recent study, designed to separate sensory from social stimulation in the Snoezelen setting, reported that two autistic youth exhibited fewer stereotyped behaviours in a Snoezelen room than in a living room, regardless of the level of attention from staff [47]. More research in this area is necessary to disentangle the effects of interpersonal contact from contact with multisensory equipment.
Implications for practice
Given that children in complex medical care are often limited in terms of mobilization and choices for play-based and therapeutic activities, Snoezelen offers a viable option for sensory stimulation in the home or in hospital. This form of stimulation, however, is not generally used in the home because of equipment size, costs and limitations associated with having a skilled therapist such as a child life specialist available to administer. Moreover, Snoezelen has been used in a variety of pediatric specialty areas including critical care where opportunities to engage in play-based activities are also restricted.
Replicating this study with pediatric patients in other long-term care settings would help expand on our results. A between-subjects study, comparing children with complex care needs across multiple sites, would be beneficial. While our goal here was to examine the within-session impact of Snoezelen, the carry-over effects of the intervention for this population also merit examination.
Reviews of the Snoezelen literature suggest that the degree of exposure to the multisensory environment affects study results: sessions that are few in number and short in duration limit the conclusions that can be drawn from the data [7, 13]. However, Lindsay et al. [49] reported that certain clients may benefit from brief, infrequent exposure, while others may benefit from longer, more numerous sessions. Future studies could explore how individual patients respond to different degrees of exposure.
Finally, researchers have called for additional qualitative research to provide a more complete understanding of how clients experience Snoezelen [13]. Interviewing hospitalized children with more developed verbal abilities would enable researchers to question them directly about their experiences with the multisensory environment. It would also be helpful to obtain supplementary information from family members or health care professionals, who have an understanding of patients’ needs and preferences.
Conclusions
Based on the range of responses from the participants in this study, our results are inconclusive. These preliminary results underscore the need to critically evaluate Snoezelen as an effective intervention for all patients in rehabilitative care. While the findings of this study are helpful in establishing the general utility of multisensory therapy for broader application in medical settings, they also demonstrate the need to consider the physiological and behavioural responses of individual patients. By continuing to test a variety of research methods in pediatric rehabilitation, greater child participation in research can be developed to inform evidence-based practice. The challenge of identifying the preferences of children with complex medical conditions does not lessen our obligation to provide care that accommodates and reflects those preferences.
Footnotes
Acknowledgments
We wish to thank Holland Bloorview Kids Rehabilitation Hospital for their collaborative support in completing this study. The contributions of Virginia Wright, Senior Scientist, Breanne Mathers, Child Life Specialist, and Lorraine Thomas, Snoezelen Coordinator from Holland Bloorview and the research assistance of Michelle Pegler, Basmel Al Saad, and Amonrat Saekang are gratefully acknowledged. We also wish to thank the children and families who took part. The methods for this study were adapted from: Kingsnorth, S., Blain, S. & McKeever, P. (2011). Physiological and emotional responses of disabled children to therapeutic clowns: A pilot study. eCAM, 1–10. Funding was provided by the Faculty of Community Services, the School of Early Childhood Studies and the EDGE Lab at Ryerson University.
Conflict of interest
The authors have no conflict of interest to report.