
Abstract
PURPOSE:
Youth with physical disabilities have lower psychosocial health and attention compared to their typically developing peers. Recent research has shown positive associations between sports participation and these outcomes. The purpose of the current study was to explore whether a school-based sports program affects psychosocial health and attention in youth with physical disabilities.
METHODS:
Seventy children and adolescents (mean age (SD) 13.8 (2.9) years, aged 8–19 years, 54% boys) with physical disabilities were included in this quasi-experimental study from schools for special education. The sports group (
RESULTS:
Linear regression analyses revealed no differences between the sports and control group for self-perception, quality of life, and attention.
CONCLUSION:
A school-based sports program seems to have no effect on psychosocial health and attention in youth with physical disabilities. Research into the important factors influencing these variables is needed before further resources can be given to improve sports participation for increasing psychosocial health and attention.
Introduction
Typically developing youth who participate in sports (i.e., physical activity engaged in for pleasure) have higher self-perception and health-related quality of life compared to their non-sporting peers [1]. This positive association between sports participation and improved psychosocial health is stronger for team sports than individual sports, probably because of the social nature and interaction of peers and adults [1]. Another factor positively associated with sports participation is attentional control [2]. Studies in typically developing youth have shown that enhanced physical activity is associated with improved attention [3, 4]. This relationship is supposed to be dose-responsive, meaning that greater amounts of physical activity induce larger attentional gains [2]. Moreover, the content of exercise seems to be important as well, integrating more coordinative and cognitive demands (i.e., sports) [3, 5].
For youth with physical disabilities, it seems more difficult to participate in sports; only 26% of Dutch children and adolescents with a physical disability at schools for special education participate at least once a week in sports [6]. In addition, they tend to have lower psychosocial health and attention compared to their typically developing peers [6, 7, 8, 9]. Regarding psychosocial health, involvement in sports can provoke successful motor experiences and focus on children’s abilities rather than on their inabilities [1]. For attention, physical activity can affect the brain’s physiology by increasing the cerebral blood flow and density of neural networks [2]. Recent research in youth with physical disabilities has shown a positive association between participation in sports and quality of life and self-perception, such as self-perceived physical appearance and global self-worth [10, 11, 12, 13]. Studies regarding attention are still very limited in this population.
While results regarding the role of sports in psychosocial health and attention are positive, the evidence for youth with physical disabilities is weak and limited by cross-sectional design. Since sports are a type of physical activity integrating both social interaction and including cognitive demands, the aim of this quasi-experimental study was to explore whether a school-based sports program affects psychosocial health and attention in youth with physical disabilities.
Methods
This quasi-experimental study was part of the Sport-2-Stay-Fit study, which was conducted between September 2014 and July 2016 in the Netherlands. The Sport-2-Stay-Fit study started with an eight week interval training for all participants which was performed twice a week for 30 minutes, containing 8–12 series of 30 seconds of all-out exercises [14]. Following the interval training, the sports group began a school-based sports program once a week for six months, while the control group performed assessments only. Anaerobic performance was the primary outcome measure of the study. The design of the study has been described extensively elsewhere [14]. The results of the school-based sports program were published in two separate papers, whereas this paper focused on the effect on psychosocial health and attention. A previously published paper showed that the sports program improved anaerobic performance and fat mass after six months, while no effects were found for anaerobic performance, peak oxygen uptake (VO
Participants
Recruiting was conducted through four schools for special education dedicated to youth with physical disabilities. Compared to regular schools, these non-integrated schools for youth with disabilities have similar learning objectives. However, additional attention, support and rehabilitation medicine are provided within school hours. In the Netherlands, 1.9% (26,500) of youth following primary or secondary education follow special education programs [16, 17]. Participants, both ambulatory and non-ambulatory, were screened for eligibility by a physical therapist, physical educator, or physician. Criteria for inclusion were: (1) a chronic disease or physical disability (neuromuscular, musculoskeletal, metabolic, or cardiovascular disorder), (2) age between 6 and 19 years, (3) participation in sports less than twice a week during leisure time in the preceding three months or advised to participate in sports by their physical therapist or physician, and (4) ability to follow simple instructions. Exclusion criteria were: (1) a progressive disease, (2) use of a powered wheelchair, and (3) participation in other research that could possibly influence current results. Additionally, prior to study initiation all parents and participants over 12 years of age provided informed consent.
Procedure
Schools for special education (
Flowchart from initial inclusion to intervention. T0, measurement at baseline; T1, measurement at two months after completion of the interval training; T2, measurement at eight months after completion of six months of school-based sports or control; HIT, high-intensity interval training. 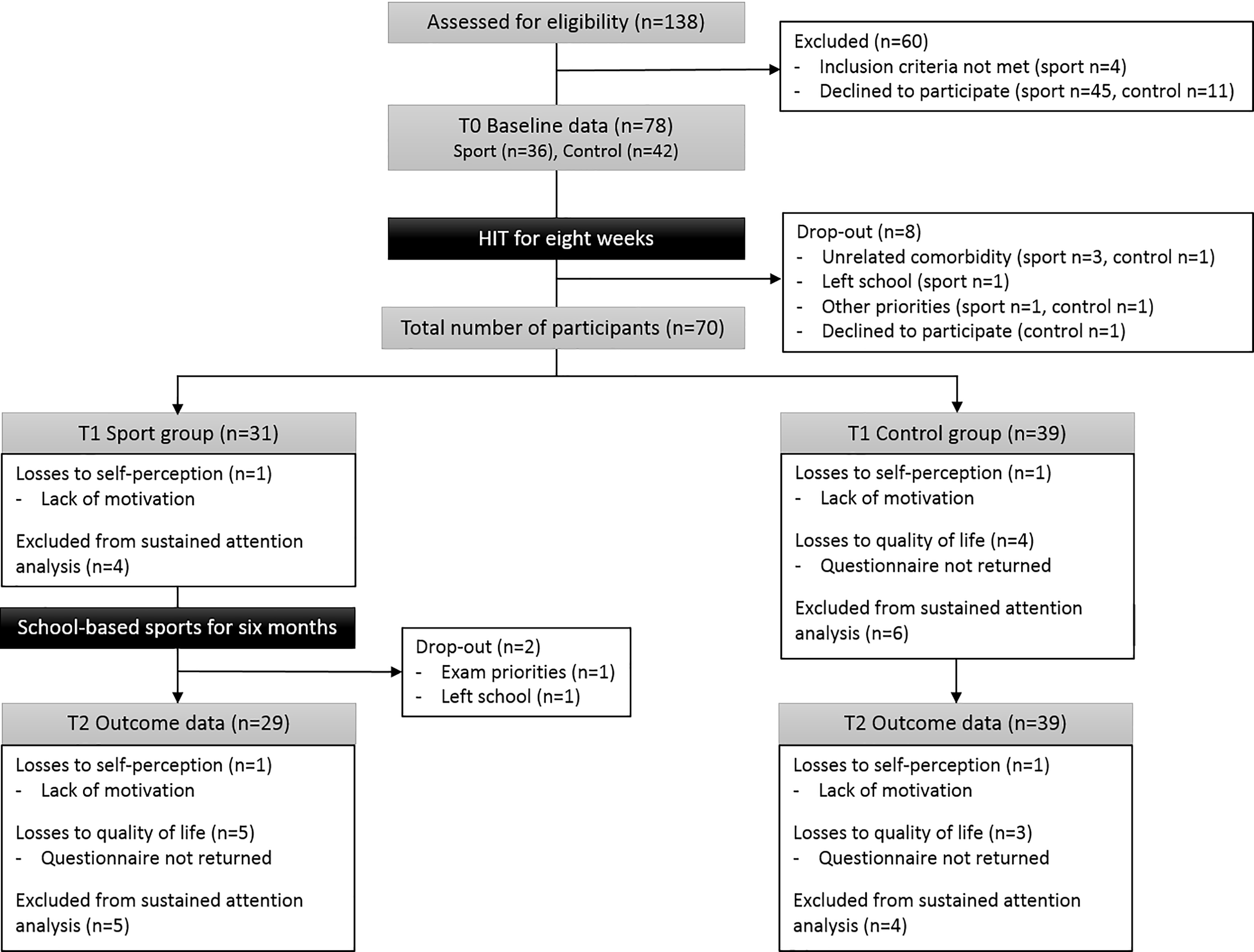
In addition to the regular schedule, the school-based sports program was provided once a week for 45 minutes by an experienced physical educator. Providing a school-based sports program once a week is relatively easy to implement and possibly increases children’s level of sports participation. Compared to physical education where body skills, teamwork, and cooperation are taught [18], sports is about having fun and exercising at higher intensities. Physical educators were instructed to encourage youth to play the game, be physically active, and have fun. No specific instructions were given on the activity type or exercise intensity. The physical educator adapted the content of the program based upon the skills and cognitive level of the children and adolescents. The school-based sports program could include soccer, (wheelchair-) basketball, (wheelchair-) hockey, and/or easy to practice games like playing tag, but was not restricted to these sports. Participants’ presence was documented every session.
Outcome measures
Outcome measures were psychosocial functioning as operationalized by self-perception and health-related quality of life. Cognitive functioning was measured by experimental tasks of attention, because this domain of cognition was shown to be associated with exercise [3].
Psychosocial health
The Dutch version of the self-perception profile for children (SPPC), a valid and reliable tool for youth with cerebral palsy [19], was used to address a total of six domains: five specific domains of self-perception (i.e., scholastic competence, social acceptance, athletic competence, physical appearance, behavioral conduct), and global self-worth [20]. The questionnaire was filled out at school with one of the research assistants. All items were scored on a four item Likert-scale and sum scores were calculated for each of the six domains ranging from 6–24 points with higher scores indicating a higher self-perception.
Regarding health-related quality of life, the Dutch version of the DISABKIDS for children with chronic health conditions (DCGM-37) was filled out [19]. This was done online by either the participant alone (
Attention
All tests for attention were performed on a tablet PC (Asus Eee Slate Tablet, Asus Europe BV, Nieuwegein, the Netherlands) to minimize coordination problems and guaranteeing detection of subtle improvements in performance. To assess search efficiency, a valid object cancellation task was used [21]. In a cancellation task, a participant is required to search for and cross out targets, which are embedded among distractor stimuli. Given the layout of this particular cancellation task, the most efficient way is to start searching at an extremity, for example the upper left corner, and proceed orthogonally, either downward and upward or rightward and leftward. Search efficiency is a useful way to measure executive control. This cancellation task was digitized and analyzed with the CancellationTools software [22]. The presented screen contained 56 targets presented as apples. The distractors consisted of 52 pears, 12 single letters, and 10 strings of letters (Fig. 2a). Children and adolescents had to tap on all apples, both red and green, until they completed all targets. No time limit was given. Search efficiency was measured using best R, which was defined as the highest absolute value of the Pearson correlation between the cancellation order and either horizontal or vertical cancellation position [23]. The best R increases with search efficiency and was calculated in the CancellationTools software as described previously [22].
Descriptive statistics
Descriptive statistics
A sample of the attention tasks performed on a tablet a, Object cancellation task to assess search efficiency; b, Extensive dot cancellation task to assess sustained attention; c, capture task to assess distractibility 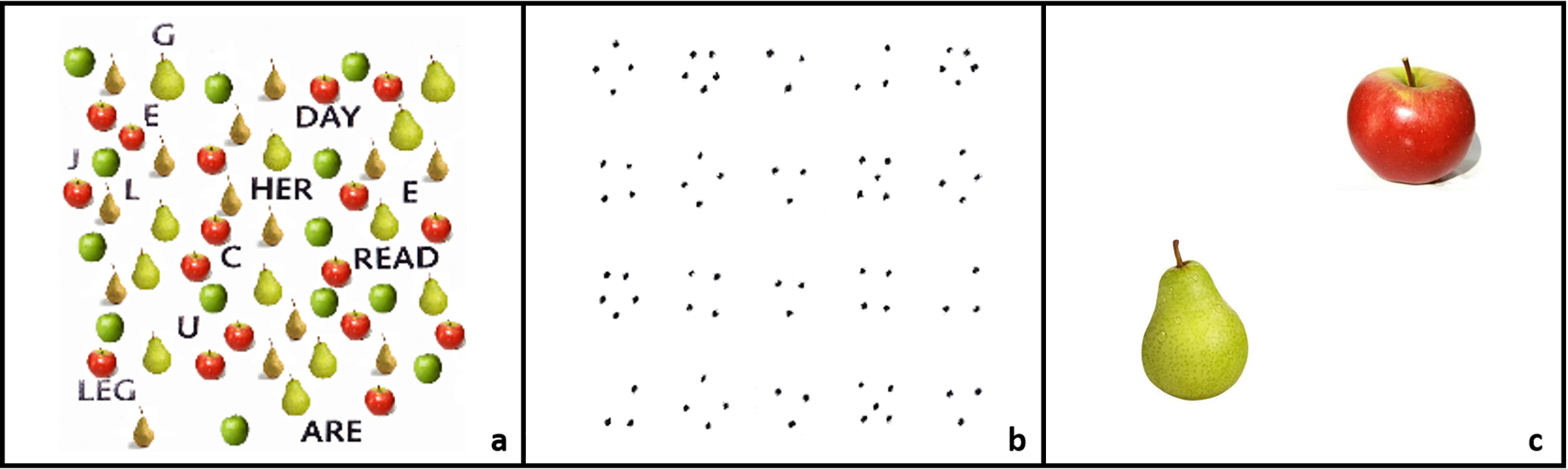
The extensive dot cancellation task consisted of 35 rows with 24 clusters of either three, four of five dots (Fig. 2b). The original frequently used pen and paper task is a valid and reliable test to measure sustained attention [24]. Children were instructed to work line by line and mark all clusters of four dots (i.e., target) by tapping the tablet as fast and accurately as possible. Every line contained eight targets and 16 distractors. After a short practice session, the actual cancellation test was started. When a participant did not finish the test within 10 minutes, the test was stopped. Outcome variables were average speed per row (in seconds) and average accuracy of marked targets per row, calculated as a ratio score between 0 and 1. Data was excluded if test instructions were not followed properly (i.e., working line by line).
The original capture task used in Van der Stigchel and Nijboer [25] was adapted to measure distractibility. Each trial started with the presentation of a central fixation cross. When the cross disappeared, the target (i.e., an apple), appeared in one of the four quadrants. In 50% of the trials, a distractor (i.e., a pear) appeared as well (Fig. 2c). Participants were instructed to react as fast and accurately as possible to the appearance of the apple. Distractibility was represented as the difference in reaction time (ms) between both conditions.
Sample size calculation showed that at least 32 participants per subgroup were needed for the primary anaerobic performance outcome of the Sport-2-Stay-Fit study [14]. Descriptive statistics were performed for group characteristics. Differences between groups in sports participation were checked nonparametrically using a Mann-Whitney U test. Statistical analyses were performed using SPSS for Windows (version 25.0, SPSS Inc, Chicago, IL, USA) with a statistical significance level of
For all outcome measures, assumptions for normal distribution and homoscedasticity were graphically checked using normal P-P plots and scatterplots for residuals, respectively. All residuals were within acceptable ranges for normal distribution. To investigate whether the sports group and control group changed over time, a paired sample t-test was used for all outcome measures. To investigate the groups by time interaction following the intervention, a linear regression was performed according to the intention to treat principle. A single model was fit for every outcome measure, with an outcome measure at T2 as the dependent variable, and both the paired outcome measure at T1 and group allocation as independent variables. The paired outcome measures at T1 were included in the analyses to correct for potential baseline differences between groups, because group allocation was not assigned randomly. Since the dataset contains incomplete data, we used multiple imputation to create and perform linear regression analyses on 10 imputed datasets using SPSS for Windows. The analysis on 10 imputed datasets resulted in one estimate. Linear regression analyses were performed on both the original data and multiple imputation data. Because both linear regression analyses resulted in similar conclusions, only the results from the imputed data are shown here. Results are reported as means and standard deviation (SD), regression coefficients (
Results
A total of 70 children and adolescents participated in the current study (Table 1). Sports participation at T0 did not differ between the sports (median 1 (range 0–3) times a week) and control group (median 1 (range 0–3) times a week) (
The number of analyzed cases are illustrated in Fig. 1. During the school-based sports program none of the participants of the control group dropped out, whereas two of the sports group quit because of exam priorities and due to leaving school. Presence at the school-based sports program was 86%, with children and adolescents attending 14.4 (4.1) sports sessions on average.
Between T1 and T2, no time effects were found for any of the outcomes in either the sports or the control group according to the paired sample t-test, except for physical limitation, which improved in the sports group (
Discussion
This study explored the effects of a school-based sports program on psychosocial health and attention in youth with physical disabilities. No differences were observed between the sports and control group after six months in any of the subscales of self-perception and health-related quality of life. In addition, attention showed no effects in favor of the sports group following the school-based once a week sports program.
Baseline scores for health-related quality of life were comparable to children and adolescents with cerebral palsy [19]. For self-perception, all scores on the subscales were comparable to those of typically developing children and adolescents [20]. A possible explanation might be peer perception; the children and adolescents included in this study attend schools for special education and are therefore surrounded by comparable peers having physical disabilities [26]. A non-integrated or non-inclusive school system is a unique system compared to those in other countries worldwide. The fact that this study was performed in a country with a non-integrated school system makes it difficult to translate the results to countries with inclusive school systems.
Meaningful sports participation is a complex phenomenon, with the interaction of environmental and personal factors [27]. In the current intervention, the school-based sports program was focused on playing sports or games, experiencing success, and having fun in a familiar and disability adapted environment (i.e., school). Important environmental barriers, like transportation, supportive trainers, and social acceptance and integration, were deliberately eliminated by performing sports at school. Consequently, the environmental involvement from family and society is underrepresented in the current intervention. To illustrate,
Mean (SD) at (T1) and after six months school-based sports (T2), and results from linear regression analysis with T2 as dependent variable and both T1 and group allocation as independent variables
the most important feature for a child’s perception of meaningful sports participation (i.e., social in- or exclusion) is having authentic friendships [28]. Since children and adolescents in the current study already knew each other from school, it is unknown whether the intervention contributed to strengthening their feelings of acceptance by others. Furthermore, our study was performed in a non-integrated disability specific setting without multiple opportunities for social comparisons. However, an integrated sports setting seems to have an impact on quality of life and perceived social competence compared to non-integrated sports settings [29]. Another environmental factor that was not actively integrated in the current sports program was family support, which can play a central role in children’s motivation [28]. It is possible that these factors, related to social integration and the environment, are important to induce positive effects of sports participation on psychosocial health regardless of the type, frequency, or intensity of sports.
Furthermore, when children or adolescents are joining an adapted sports club, they consciously choose a certain type of sport, and often also participate in a competition. These personal factors provide a sense of belonging to the community, expressing themselves through the specific sport, developing an identity by being part of a team, and providing the opportunity for making new friends [28]. It is unknown from the literature if these personal factors are necessary for gaining psychosocial health, since there might be a self-selection bias in youth joining sports clubs. To date, adolescents with better psychosocial function (i.e., social skills) are more likely to join sports clubs and maintain that connection [30]. This self-selection bias may partly account for the positive association found between sports participation and psychosocial health in cross-sectional studies [1]. In addition, a recent longitudinal study showed no additional effect of providing positive, specific, and progressive feedback to enhance self-perception in children with a developmental coordination disorder following physical therapy [31]. Therefore, it is still unknown which factors are important to induce positive effects of sports participation on psychosocial health.
It is important to take into account that the sports program was designed to improve physical fitness and not attention. However, the program did include a progressive increase in task complexity, ensuring and challenging cognitive efforts, but attention did not change compared to the control group over a six-month period. This is in contrast to results presented by Hillman et al. [32] where typically developing children showed improved attention following a school-based intervention of nine months. Their program consisted of 70 minutes of physical activity each day after school. Taking into account the dose response relation between physical activity and cognitive functioning [2], the frequency and duration of the program could be an explanation why our intervention showed no improvements. Our dose of 45 min/week might be too low to induce effects on attention. On the other hand, by increasing physical activity levels alone, it is still unknown which specific factors (i.e., active ingredients) related to the environment and social integration contribute to inducing attention and should be integrated in future interventions.
Besides the limitation discussed before, other limitations have to be recognized. Firstly, participants were not randomly assigned to either the sports or control group. Moreover, the assessors were not blinded for group allocation. Secondly, the current sample comprised a large age range and a variety of diagnoses, which makes it implausible to discover anything other than the most major effect. However, this heterogeneity does reflect the real-life situation at schools for special education as children and adolescents participate in sports together. In addition, a recent cross-sectional study in children and adolescents with physical disabilities found that beneficial scores on psychosocial health in youth who participate in sports at least twice a week were independent of age, sex, school type (i.e., special or regular education) and diagnosis [13].
In conclusion, a school-based sports program did not increase psychosocial health and attention in youth with physical disabilities. There is a need for more research to identify the potential factors which account for the positive association between sports participation and both psychosocial health and attention.
Footnotes
Acknowledgments
The authors gratefully acknowledge all children and adolescents and their parents for participation. We would like to thank the physical therapists, physical educators and students at four schools for special education in the Netherlands for their time and effort: Ariane de Ranitz