
Abstract
Background:
Lateral dislocation of the patella is a common injury in children. It can occur in previously healthy and anatomically normal knees, but there are several abnormalities that predispose to patellar instability. Magnetic resonance imaging is an essential part of assessing for associated injuries and risk of further instability. Treatment aims to prevent redislocation, residual instability, osteoarthritis, and allow return to previous activities. The purpose of this review was to assess evidence for management of first-time patella dislocation in children and adolescents.
Methods:
Literature review was performed, accompanied by the current best practice by the authors.
Results:
Non-operative treatment is preferred, except where there are associated injuries such as osteochondral fractures that would benefit from surgery. The exact method of ideal non-operative management is not clearly defined but should focus on restoration of range of movement and strength with bracing as indicated. There seems to be a trend toward operative intervention that may well be inappropriate.
Conclusion:
Further prospective studies are required with focus on the younger patient to fully understand if there is an at-risk group that would benefit from early surgery.
Level of evidence:
level III.
Introduction
Lateral dislocation of the patella is a common injury, with an annual incidence of 29–43 per 100,000. 1 It usually occurs in the second decade, most commonly among female patients. Often as a result of sports injury, one in five occurs in usual activities of daily living. 2 Soccer, gymnastics, and dancing are typical injuries, where outward rotational forces and valgus stress when flexing a knee may drive the patella out of the sulcus. In rare cases, dislocation may be due to a direct blow to the medial aspect of the patella. The rate of re-dislocation after first patella dislocation is approximately 30%, but the reported rates generally vary between 10% and 50%. 3 Rates may be even higher in the skeletally immature.1,4
Dislocation can occur in previously healthy and anatomically normal knees, but there are several abnormalities that predispose to patellar instability. Both bone and soft-tissue abnormalities may associate to increased risk of recurrent instability. Furthermore, there are chronic diseases that associate with patella instability, such as disorders that increase general ligamentous laxity (e.g. Ehlers-Danlos or Marfan syndrome) and genetic conditions such as trisomy-21.
Treatment aims to prevent re-dislocation, residual instability, osteoarthritis and allows return to activities.5,6 First-time patella dislocation has traditionally been managed non-operatively, although surgical management may be becoming more common in the pediatric cohort. 7 This is in part due to a lower rate of re-dislocation after surgery (22%), compared to non-operative care (31%). 8 However, given that the majority of non-operatively treated patients (50%–70%) still manage without further dislocations, no agreement regarding surgery after first-time dislocation has been reached. Furthermore, despite the risk of recurrence, patients treated non-operatively still show good clinical and subjective results.3,5,9 Operative care has also been associated with increased risk of later patellofemoral osteoarthritis. 10 This may be due to selection bias or the wrong choice of surgical procedure.
The purpose of this review was to assess evidence for management of first-time patella dislocation in children and adolescents, accompanied by the current best practice by the authors.
Methods
Published articles concerning first-time dislocation was reviewed, focusing on contemporary literature from 2010 onwards. Systematic reviews and consensus statements were appreciated as the primary source. The production of this work follows from presentation by the authors and subsequent discussion at the European Pediatric Orthopedic Society (EPOS) Annual Meeting in 2022, in the scientific session of the EPOS Sports Group, with the authors including their treatment preferences.
Assessment and investigation
A detailed history of the injury should be performed inquiring after previous instability in the injured and contralateral knee. A family history of instability is also important. Habitual dislocation, meaning a patella that dislocates on each attempt to move the knee to flexion, in contrast to first-time or recurrent patellar dislocation, should be excluded. Habitual dislocation is associated with several potential predisposing factors such as contracture of the lateral patellar soft tissue, lateral femoral condyle hypoplasia and general ligamentous laxity, and can be due to various syndromes. Clinical examination should look at alignment in the coronal and sagittal plane as well as assessing for generalized laxity. The location of the patella in the midline or laterally will be observed. Tenderness at the medial aspect of patella and distal femur are invariably present with first-time dislocation. The presence of an hemarthrosis should prompt assessment for a chondral or other intra-articular injury. Often bone fragments seen on plain radiographs are avulsions of the patella attachment of the medial patellofemoral ligament (MPFL), although surprisingly most of these tend to be from the distal patella and represent avulsion of the medial patellotibial ligament (MPTL). These should not be confused with osteochondral fractures caused by dislocation, and do not require surgery.
Apprehension test (Fairbanks sign) is positive when fast-protective quadriceps muscle activation is found as a consequence of pushing the patella laterally. 6 Clinical examination of the knee, including cruciate ligaments and menisci may be challenging in the acute phase.
Rotational profile of the lower extremities should be evaluated and measured clinically, if tolerated. The presence of rotational malalignment is valuable when estimating the risk of recurrent injuries and the potential of later surgery. Valgus alignment of the mechanical axis should be evaluated clinically during initial presentation if full extension with full weight-bearing can be achieved.
Plain radiographs are the routine investigation for all patients. Anterior–posterior and lateral projections as well as a merchant view can be taken to exclude associated fractures. Patella alta can be determined by initial lateral radiographs, although a 30° flexed view is required for assessment. Magnetic resonance imaging (MRI) is the investigation of choice, especially in the presence of an hemarthrosis that may suggest an osteochondral fracture. MRI is also useful to comprehensively assess the patella-stabilizing soft-tissues, particularly the MPFL and the MPFL complex, as well as other associated injuries. Furthermore, MRI is worthwhile in excluding the anatomical abnormalities that may be the risk factors of instability; trochlear dysplasia, patella alta, and assessment of the tibial tubercle-trochlea groove distance (TT-TG). Patella alta can be assessed by measurement of the patella-trochlear index or Caton–Deshamps Index, although with lateralization of the patella this can sometimes be difficult 11 (Figure 1). The advantage of MRI is the method by which the images are taken is more standardized and less prone to positioning effects seen with plain radiographs.
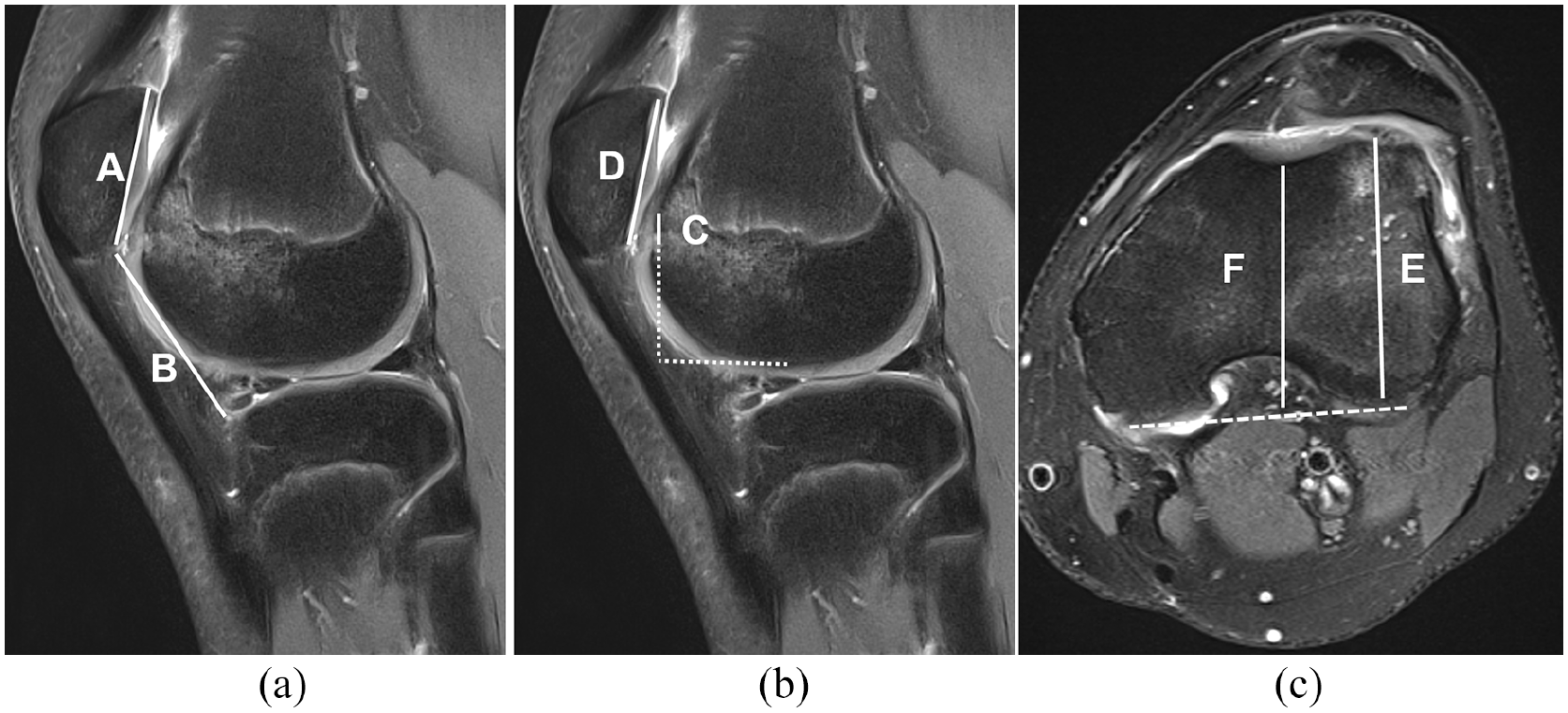
(a) Patella alta (Figure 1a) can be measured with MRI, using the Caton–Deschamps Index. The length of the patellar articular surface and its shortest distance from the tibia are compared with the normal value (B/A) < 1.3. (b) Patellotrochlea index is another reliable index to measure and evaluate patella alta: The length of the trochlear cartilage overlapping the patellar cartilage (C) is compared to maximal length of the patella (D). The mean patellotrochlear index is 32%. (c) There are several variables describing dysplasia of trochlear sulcus; however, the trochlear depth is among the most important. Measurement is performed 3 cm above the joint line by comparing the highest bone distance (E) and lowest bone distance at the sulcus (F). Sulcus depth >3 mm is taken as normal.
The TT-TG measurement assesses lateralization of the extensor mechanism or medialization of the trochlea groove relative to the tibial tuberosity. This measurement changes with age, and values utilized for adults are not suitable for children. 12 This can be measured with less accuracy with plain radiographs. 13 The importance of MRI is in stratifying the risk of recurrent instability and the need for surgical management for first-time dislocation. Currently, due to improved availability of MRI, it is the recommended modality of imaging by the authors for all children presenting with first-time patella dislocation.
Principles of management with acute dislocation
Although the dislocation is normally reduced before attendance, reduction of the patella should be performed and clinically confirmed, prior to any other care. In the rare case of an irreducible patella, general anesthesia may be needed in younger children to reach reduction by extending the knee and slightly lateral pressure on the patella. Although medial dislocation is rare, this should be considered. Patients may well describe feeling something prominent medially, but this is often the prominence of the medial femoral condyle seen with lateral patella dislocation and should not be confused with medial dislocation. Basic principles of treating acute musculoskeletal injury are valid; cryotherapy, pain relief, compression, and elevation are advised. Full weight-bearing is allowed as tolerated. Crutches may be needed primarily.
At present, the primary treatment of first-time patella dislocation in children and adolescents is non-operative.14–17 There is a lack of evidence concerning immobilization and the use of patella stabilizing splints or orthoses after first-time dislocation. 2 Similarly, there is no general consensus about the accepted degrees of knee flexion after first dislocation. However, immobilizing by using a cast or rigid orthosis is not recommended by the authors. It prevents motion recovery and early strengthening of the muscles, which are essential. An elastic patella-specific brace may be useful, as it encourages weight-bearing and recovery and reduces anxiety which may be helpful especially in younger children. Furthermore, it aids in patellar realignment. 18 In practice, a dynamic brace with lateral patella stabilizing support is advocated by the authors after first-time acute traumatic patella dislocation, but it should not be used more than several weeks (Figure 2). Taping may also aid help with symptoms, but it does not prevent maltracking. 2
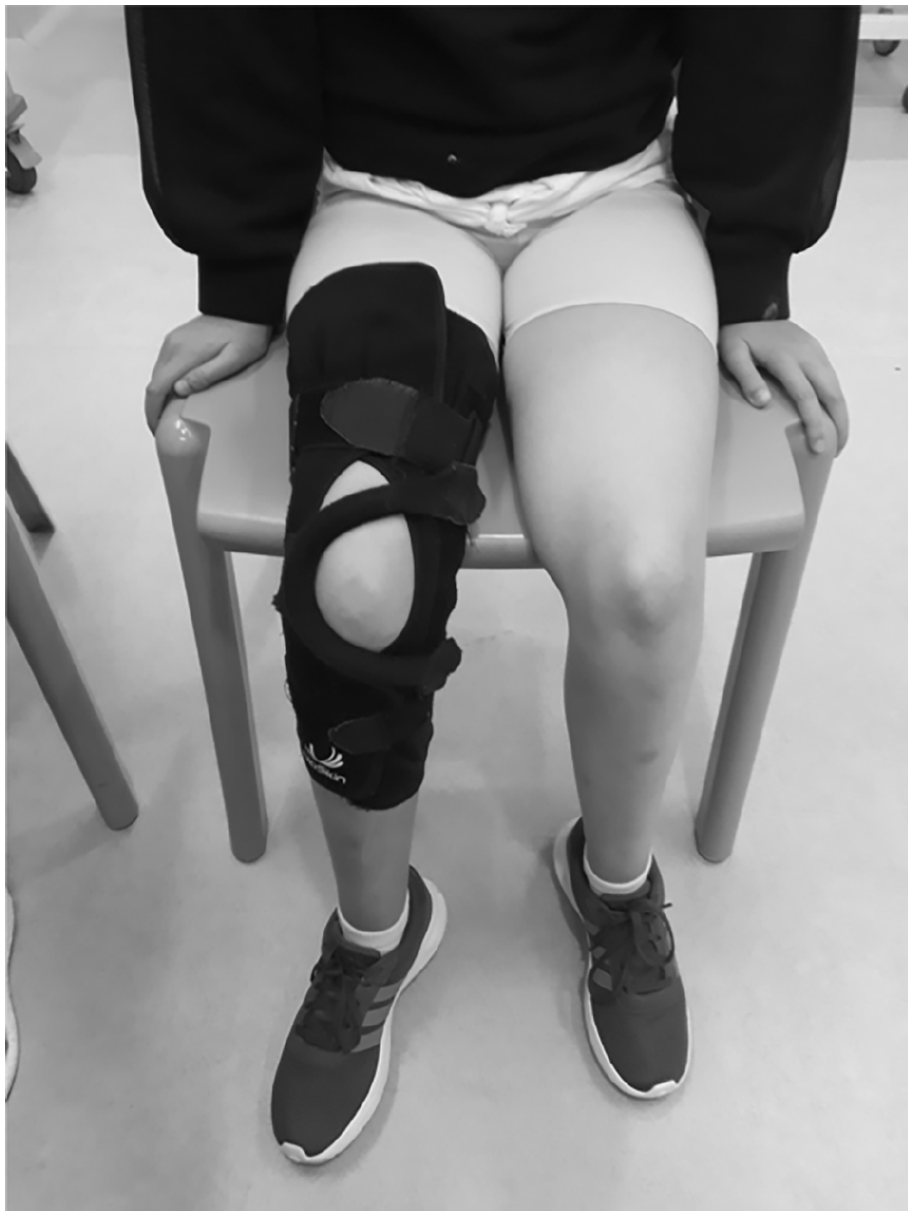
Example of a patella stabilizing brace that can be used for recovery following a first-time dislocation.
Physical therapy is commenced early, with the main purpose to gain full movements, increase quadriceps strength and function and improve coordination and core and hip stability. The physical therapy progress step-by-step, thorough five different stages: pain and swelling resolution, joint mobilization, muscle strength, proprioception, coordination, and return to play. 19 Developing good movement patterns is important in injury prevention.
The best available method of non-operative management is still not known in either adults or children and should be an area of focus for future research. 20 Not all patients do well after first-time dislocation, and recurrent symptoms may result in the need for corrective surgery. Therefore, appreciated practice by the authors is to perform ongoing clinical follow-up.
The role of surgery
Recurrent instability runs the risk of further cartilage damage, which is known to be the main factor in patellofemoral instability that predisposes to osteoarthritis. 21 Identifying patients that should have a stabilizing procedure for a first-time dislocation is controversial due to the fact that around half will have no further episodes of instability. What has altered is the role of risk stratification to allow the clinician to select those patients who are at a higher risk of further instability. Factors that predispose to recurrent instability after a first episode include patella alta, trochlea dysplasia, an abnormal TT-TG, open physes, and younger age. 22 The presence of an osteochondral fracture is according to the authors the only current indication for acute surgery. There is disagreement about what procedure is indicated after the index injury.23,24 Surgery needs to be considered individually for every patient. However, given that 50% to 70% of the children with first acute patellar dislocation will resolve without a second dislocation, routine corrective operation will not be justified for all patients.
Surgical treatment of patellar dislocation should be primarily focused for the patients who evidently have predisposing anatomical risk factors as they present higher rate of recurrent morbidity. In these patients, definitive surgery should be performed to restore anatomy and stability—and in many cases, this will involve reconstruction of the MPFL. This is torn in up to 4 out of 5 of the patients with first-time dislocation. 25 Isolated MPFL reconstruction is an option after first-time dislocation of a growing child, but it is rarely justified. Trochleoplasty and tibial tuberosity transfer are not recommended for a patient with an immature skeleton, and they should be postponed until skeletal maturity. There are methods to correct an abnormal TT-TG and patella alta in the skeletally immature. Often isolated MPFL reconstruction will correct some patella height, and additional procedures may not be necessary. 26 One positive factor in those with growth remaining is the ability to use guided growth with temporary epiphysiodesis in order to improve patellar tracking.27,28 Recently, it has been challenged if all or any of the predisposing factors should be corrected, when performing MPFL reconstruction, and further studies are warranted.29,30 There are many surgical techniques for performing reconstruction of the MPFL, this topic in itself is beyond the scope of a review of first-time patella dislocation.
Return to play and follow-up
The return to pre-injury sport is depending on the individual recovery rather than time from the injury. Symmetric thigh strength and neuromuscular control should have been achieved. 31 An arthrometer may be used for evaluation but several variations of hop tests may work as well. Approximately 80%–90% of strength, as compared to the uninjured side is required prior to return to play. Functional recovery, including dynamic stability and agility, are assessed clinically. Usually, return to knee intensive sports is allowed not earlier than 10–12 weeks from the injury but may be much later. It is important to note that with non-operative management, return to prior sporting activities is reported to be under 30%. 32 Further investigations are required to define safe return-to-sports (RTS) criteria for first-time patella dislocation in skeletally immature patients.
Evidence for surgical management and future developments
High-level clinical trials in both adults and children assessing benefits of surgery for first-time dislocation are sparse and often have variable outcomes, meaning at present, there is still no clear answer as to what the role of surgery is.33,34 Functional outcomes need to be more adequately assessed along with re-dislocation rates, which is only one facet of assessment of failure of treatment. Clinical trials specific to children are limited and often involve historical procedures as opposed to contemporary MPFL reconstruction. 35 There are current trials randomizing to operative versus non-operative management, although none are specifically targeted at the very young under-16 cohort (Pediatric and Adolescent Patellar Instability (PAPI)). 36
Conclusion
At present, management of first-time dislocation in the pediatric age group should be non-operative, except where there are associated injuries such as osteochondral fractures that would benefit from surgery. MRI forms an essential part of assessing for associated injuries and calculating risk of further instability. The exact method of ideal non-operative management is not clearly defined but should focus on restoration of range of movement with bracing as indicated. There does appear to be a trend moving toward operative intervention that may well be inappropriate, certainly further prospective studies are required with focus on the younger patient to fully understand if there is an at-risk group that would benefit from early surgery.
Footnotes
Author contributions
J.S. contributed to the study design, manuscript writing and final editing, and manuscript approval. N.N. contributed to the study design, manuscript writing and editing, and manuscript approval.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.S. is a member of the International Editorial Board of Journal of Children’s Orthopedics. Otherwise, there are no conflicting interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.