
Abstract
Background:
The incidence of meniscal tears in children has been increasing. Early sport specialization, more intense training activity, and increasing participation in competitive sports may have affected to that increasing trend. Diagnosing acute menisci tear in children is based on suggestive clinical and magnetic resonance imaging findings. There are special particulars in immature menisci, due to relatively good vascular supply. Furthermore, growing skeleton makes differences in injury pattern, and a clinician needs to recognize not only meniscus but also potential injuries in growth plates and ligaments, which are usual in connection with pediatric meniscus leasion. Clinical and imaging investigation prior to treatment is crucial, because non-operative care is considerable, to achieve spontaneous healing, especially in peripherial tears of younger children. Second, repair is preferred always as possible, in spite of resection due to high rate of long-term sequelae after partial meniscectomy. High standard preoperative imaging aid in preparing to the meniscus sparing arthroscopic intervention.
Methods:
In this current concept article, the clinical considerations of imaging the injured pediatric knee with a suspected meniscus tear and the treatment options by the imaging findings are reviewed.
Level of evidence:
level III.
Introduction
One of the most common injuries in a skeletally immature knee is a traumatic meniscal tear. 1 Meniscal injuries usually exist with concurrent ligamentous injuries, particularly anterior cruciate ligament (ACL) injury. 2 The incidence of meniscal tears in children is significantly lower compared to adults; however, it has been increasing.3,4 Early sport specialization, more intense training activity, and increasing participation in competitive sports may have affected to that increasing trend.
Diagnosing acute menisci tear is based on suggestive clinical findings and magnetic resonance imaging (MRI) findings. 5 There are several pitfalls in diagnosing tear of immature menisci. Due to relatively good vascular supply to the immature menisci in younger children, treatment philosophy is different in children. 6 Spontaneous healing is considerable, in particular in peripherial tears and not all tears should be operated upon. 7 However, surgery is required for most pediatric patients with menisci tear. Repair is a preferred method, as compared to partial meniscectomy. 6 Arthroscopy with all-inside technique is primarily attempted for all patients. Outside-in and inside-out techniques are alternatives.
Given that surgical treatment of pediatric menisci tear is always a challenging intervention with a potential to iatrogenic surgery-based chondral lesions in particular in younger patients with small anatomic dimensions of the knee, proper clinical and imaging examinations, and their interpretation are essential to decision-making. In this article, anatomical considerations and MRI findings of acute pediatric meniscal tears are reviewed, accompanied by the MRI-based treatment options.
Methods
This current concept article is based on the subsequent topics at the European Pediatric Orthopedic Society (EPOS) Annual Meeting in 2022, in the scientific session of the EPOS Sports Group, contributed by the authors, accompanied by the treatment practices by the authors. Published articles of acute pediatric menisci tear, clinical characteristics, and imaging were reviewed (not systematically), focusing on contemporary literature from 2010 onwards.
Anatomical consideration of pediatric menisci
Menisci is the intra-articular skeletal structure of a knee, with function of absorbing shock, distributing axial load, assisting in joint lubrication, and facilitating nutrient distribution in a knee. Menisci are divided into anterior horn, body, posterior horn, and roots. In 2% of the population, an anomalous insertion of the medial menisci (MM) parallels the ACL and can be mistaken for a tear. The MM anterior root can occasionally insert along the anterior margin of the tibia and mimic pathologic subluxation.
Meniscal formation happens during gestation weeks 8–14. In fetal developing period, a meniscus is entirely vascularized. In newborns, the peripheral 50% of the meniscus is vascularized (the “red zone”) by the surrounding, perimeniscal capillary plexus. The degree of vascular penetration to the meniscus tissue declines with increasing age, to being about 10%–30% in a mature skeleton. In adults, menisci get nutrition directly from synovial fluid, without proper blood supply.
Mechanically, circumferentially (longitudinally) oriented type I collagen bundles provide the meniscus with hoop strength and are critical to resisting axial load and preventing meniscal extrusion. Thinner radial fibers are interposed perpendicular to these bundles and act to tie the bundles together, forming a lattice and providing structural support for the menisci.8,9 The MM is less mobile because of its peripheral attachments to the deep fibers of the medial collateral ligament. In addition, considering the macroscopic anatomy of the menisci, the MM has a more open C-shaped configuration, with higher width from anterior to posterior direction.9,10
Anatomic variants and diagnostic pitfalls
There are several common anatomic structures that can mimic a tear of pediatric menisci. Transverse meniscal (geniculate) ligament is a thin fibrous band that is present in 90% of dissection specimens and 83% of the patients in MRI studies.9,11 It connects and stabilizes the anterior horns of the menisci to the central part of the knee. On sagittal projection of the images, this ligament can simulate an anterior root tear.
Meniscofemoral ligaments (MFLs) originates from the posterior horn of the lateral menisci (LM) and insert onto the lateral aspect of the medial femoral condyle. At least one MFL is identified in 93% of the population in MR imaging studies.9,12–14 The MFLs assist the posterior cruciate ligament (PCL) and help control the mobility of the posterior horn of the LM during knee flexion and extension, to avoid anterior–posterior movement and entrapment. The commonly recognized MFL ligaments also in children are the Humphry and Wrisberg ligaments, which lay anterior and posterior to the PCL. Popliteomeniscal fascicles are synovial-lined fibrous bands that attach to the LM’s posterior horn and aid in forming the popliteal hiatus. These fascicles can mimic a peripheral posterior horn flap tear in MRI. There are other anatomic variants that can mimic a menisci tear and needs to be recognized when interpreting the MRI findings (Table 1; Figure 1).
Anatomic variants of a pediatric menisci that can mimic a menisci tear.
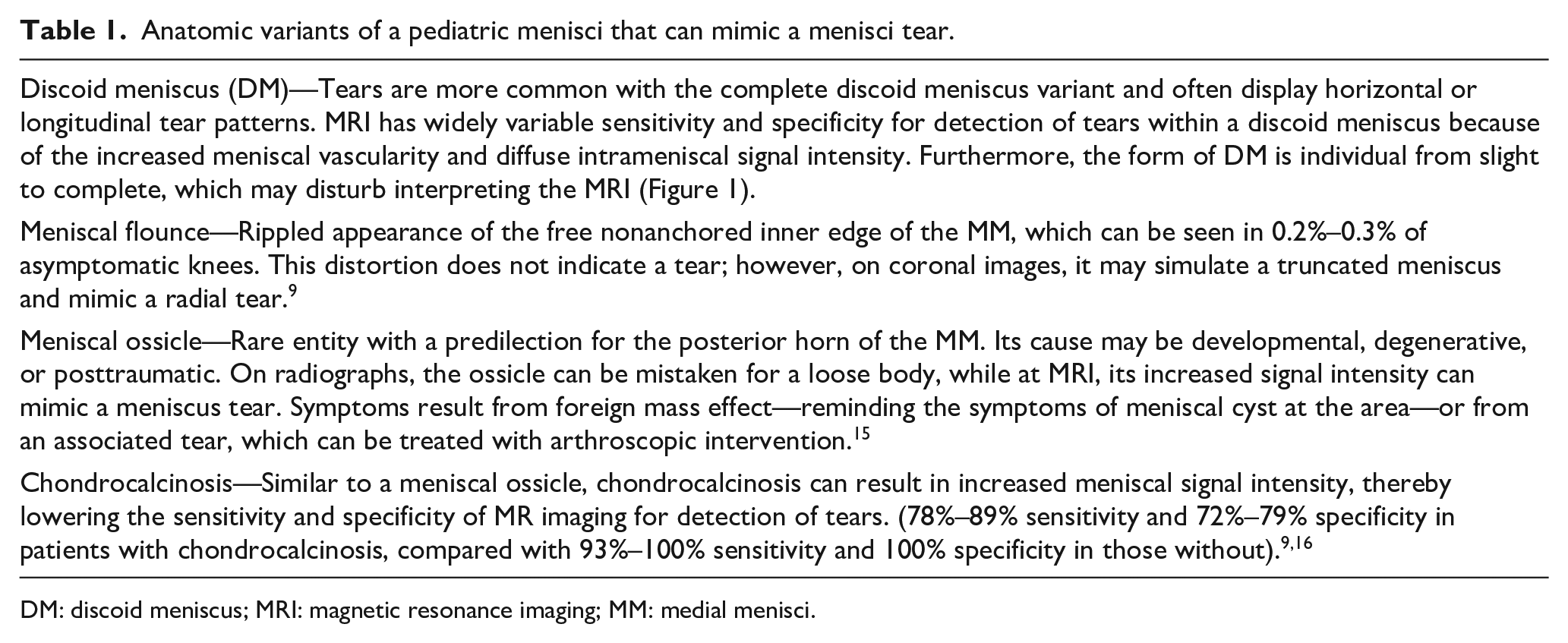
DM: discoid meniscus; MRI: magnetic resonance imaging; MM: medial menisci.
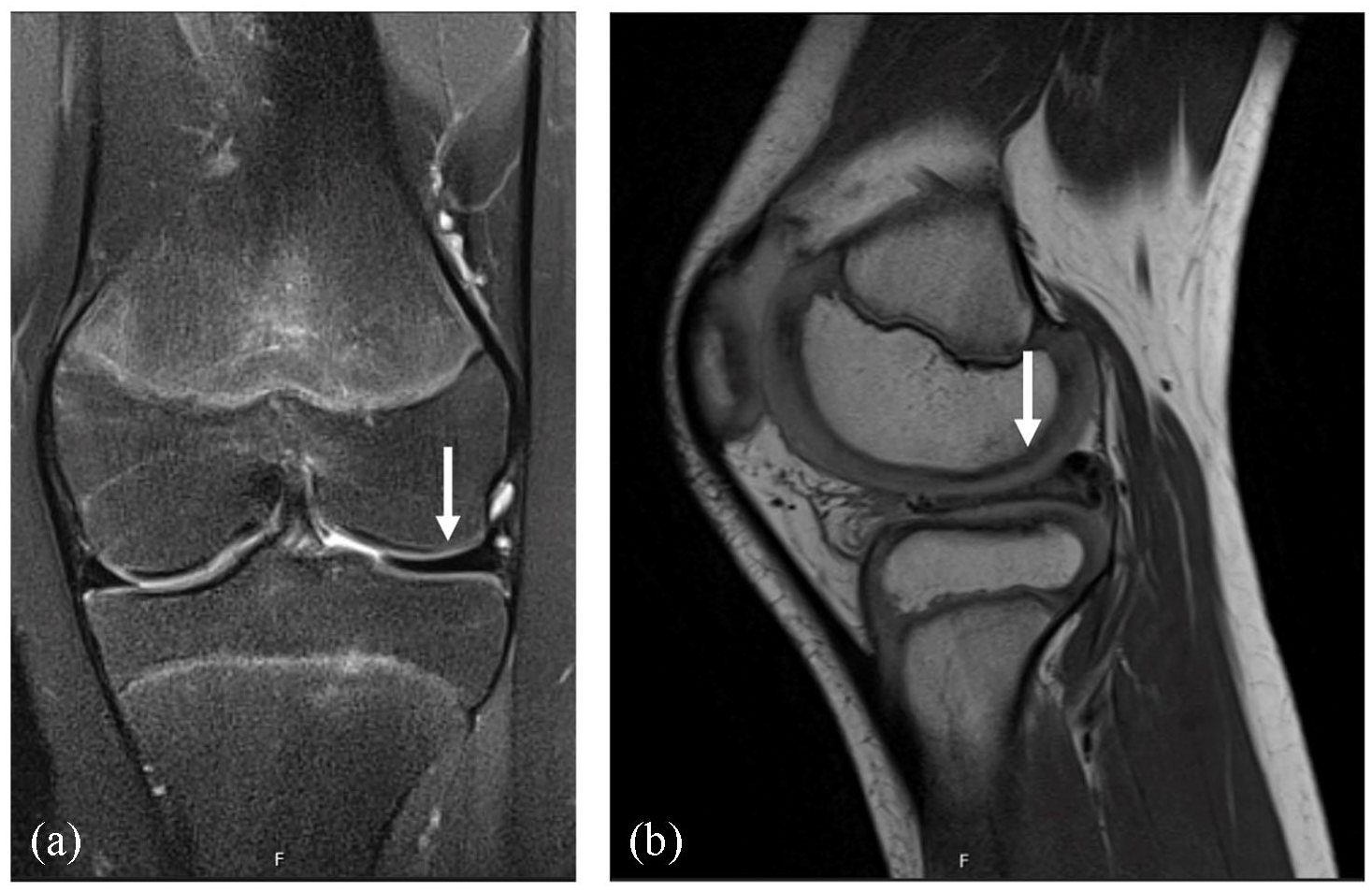
(a) Coronal normal MR imaging appearance of the medial meniscus and the typical bow-tie configuration of the lateral discoid meniscus and (b) sagittal view of the same lateral discoid meniscus as seen in Figure 1(a).
Imaging of meniscal tear
Knee radiographs including anterior–posterior, lateral, and sunrise views are taken primarily to exclude alternative injuries, such as fracture or osteochondrosis dissecans. Proximal tibiae metaphysis is an area prone to compressive torus fracture in anterior cortex, which is a typical trauma in younger children, in particular. 17 MRI is an imaging method-of-choice in investigating suspected meniscus lesion. With arthroscopy considered the standard of reference on detection of meniscal tears, MRI demonstrates high sensitivity—93% for the MM and 79% for the LM—and specificity—88% for the MM and 96% for the LM. 18 However, in younger children with higher vascularity of the menisci, interpretation of MRI of acute menisci tear is challenging, because of greater intrameniscal tissue signal intensity and vascular intraparenchymal structures (capillary vessels) in children.8,19
In addition to a evidente tear, there are indirect, secondary signs of meniscal injury. Parameniscal cysts are distinguished from bursae and ganglion cysts by their intimate association with the meniscus, either through direct contact or via a fluid track. They represent the peripheral escape of joint fluid through a meniscal tear, which typically contains a horizontal component. Subchondral bone marrow oedema is adjacent to the meniscal attachment site, parallels the articular surface, and is less than 5 mm deep. A meniscus tear needs to be suspected with this findings. 20
Clinical decision-making of meniscos tear by MRI-based injury type
In general, MRI-confirmed non-discoid meniscal tears in children can be treated with non-operative therapy, surgical repair, or partial meniscectomy. However, an accurate and precise diagnosis of a menisci injury is important in planning the treatment and preventing unnecessary surgical exploration or repeated interventions in children. 21 Furthermore, surgery often requires general anaesthesy in younger children.
Treatment decision should be based on injury patterns and associated injuries, as well as patient’s age. MRI is justified prior to operation, nevertheless, that may require a general anesthesia, too. Due to satisfactory vascular supply to the particular areas, the spontaneous healing potential of peripheral tears is considerable in children.8,19 Thus, MRI finding with a small peripheral (<10 mm) longitudinal tear can be first treated nonoperatively, taken that there is no major displacement. 7 However, most of MRI-confirmed meniscal tears in children need some surgery. Because of better vascular supply, menisci sparing repair is preferred in children and should be primarily attempted for middle and peripheral third tears, instead of partial meniscectomy.21,22 Partial meniscectomy, when required, should be performed gently, because of the risk of later osteoarthritis. 23
After making a primary diagnosis of meniscal tear, arthroscopy is recommended surgical approach for both repair and debridement. 24 Meniscal repair can be made through all-inside, inside-out, or outside-in techniques. All-inside approach is preferred by the authors, as appropriate, but particularly anterior horn tear may be best repaired using outside-in approach. 25 Inside-out approach is practical in younger children, if arthroscopy is inappropriate due to small dimensions. 26 Prior to fixation, damaged menisci tissue is prepared with abrasion, to enhance healing. Vertical madrass sutures are preferred, to avoid obstruction of vessels and spare vascular supply.
Currently, there is no standard tear classification system for pediatric menisci tear. Instead, descriptive definition of a tear is used: horizontal, longitudinal, radial, root, complex, displaced, and bucket-handle tears are the most common types of tears. Simple tear will heal better, compared to bucket-handle or complex tears. More central tears show poorer healing prognosis, as compared with more peripherial tears, due to vascular diferences, particular in younger children. It is not clear if healing potency is differente between medial and lateral meniscus. The types of pediatric tears and their treatment options are presented in Table 2 (Figures 2–6).
Types of menisci tear and their treatment options in children.
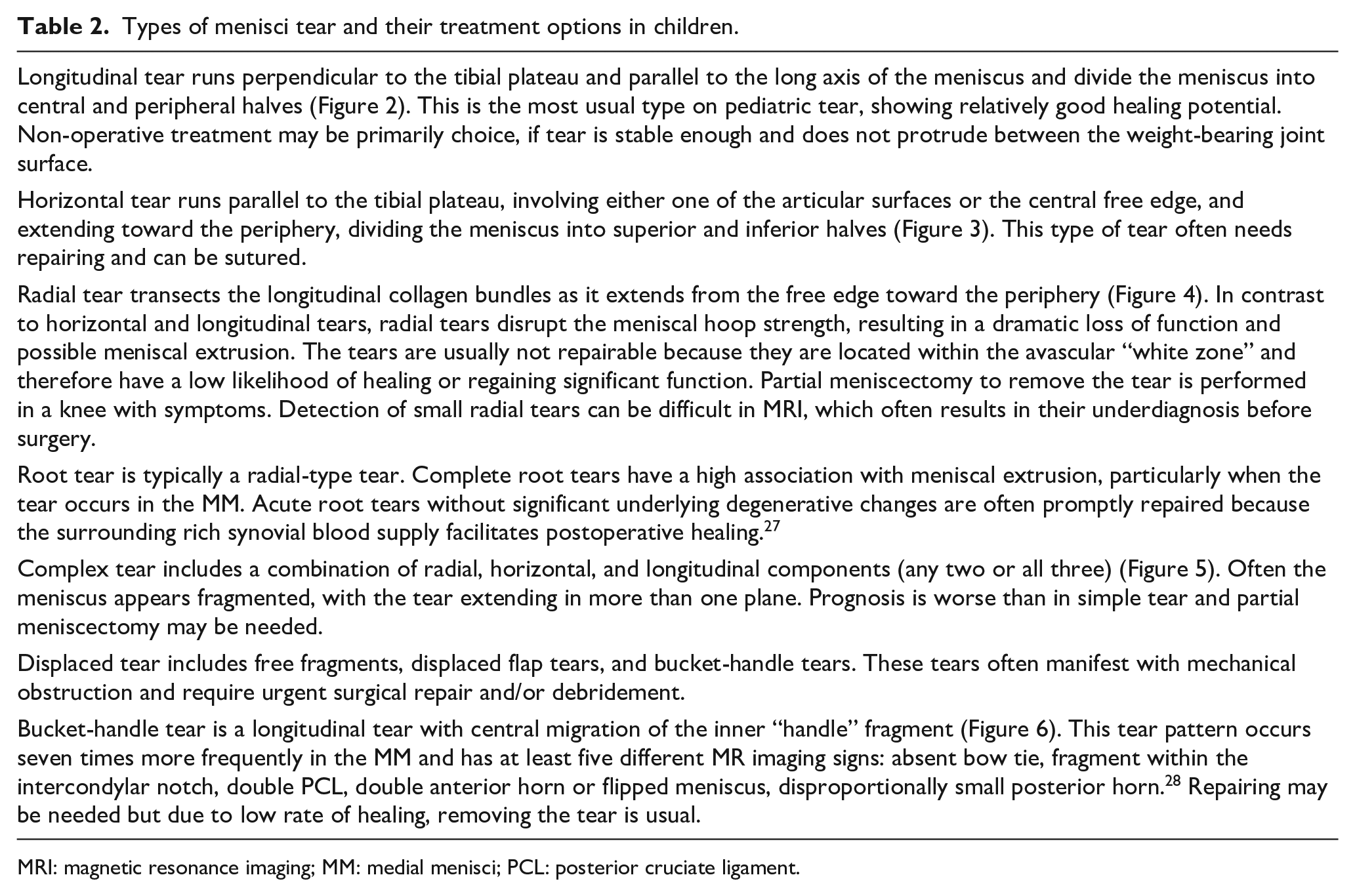
MRI: magnetic resonance imaging; MM: medial menisci; PCL: posterior cruciate ligament.
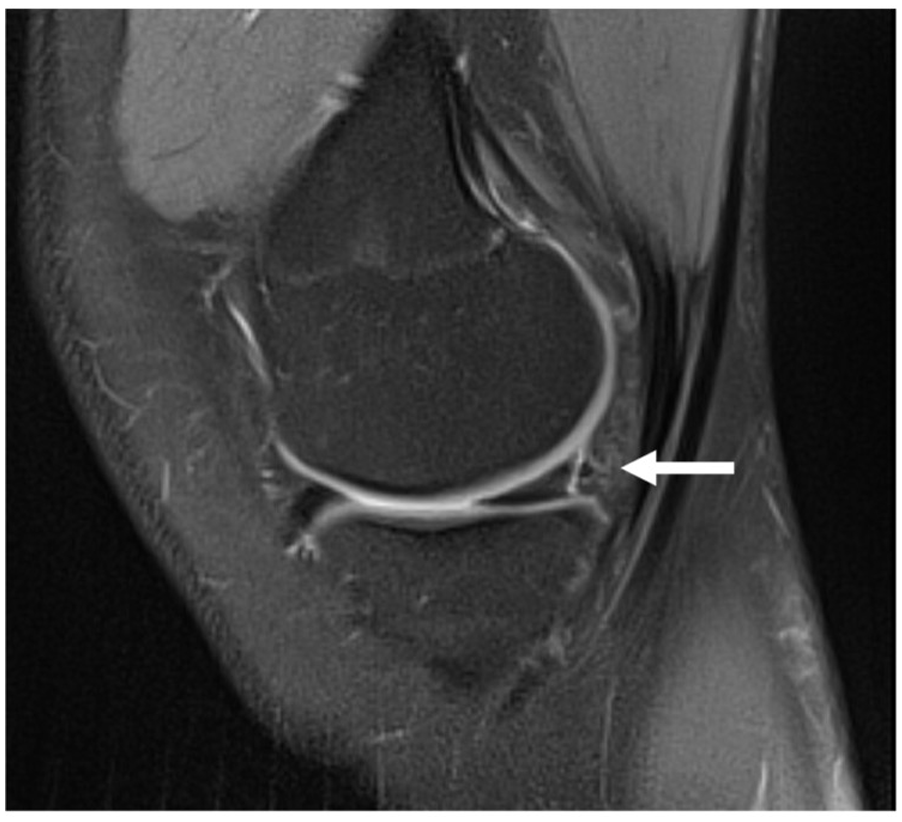
Longitudinal tear, internal meniscus, and sagittal view.

Horizontal tear, internal meniscus, and sagittal view.

Radial tear, lateral meniscus, and sagittal view.

Complex tear, internal meniscus, and sagittal view.

Bucket-handle tear, internal meniscus, and coronal view.
Comprehensive rehabilitation should be addressed in close collaboration with a physical therapist, depending on the MRI findings of non-operatively treated menisci tear. Post-operatively, when repairing procedure has been performed, comprehensive rehabilitation should also be addressed in close collaboration with a physical therapist, familiarized in pediatric knee. The authors suggest partial weight-bearing and full knee range of movements, to decrease compression at the operation area. Physical therapy is usually initiated immediately postoperatively, and it aims in improving strength, motion, and joint control. Gradual return to the pre-injury sport is the final goal of the treatment, but recovery may take 4–6 months; full motion, close to symmetrical tight forces, lack of symptoms and no pain are required prior to return. Cutting and twisting movements are prohibited until full control of the painless knee.
Conclusion
The incidence of meniscus tears in children has increased. 29 The injury is isolated or combined with other lesions, most usually ACL rupture. 30 MRI has a high accuracy for preoperative detection of meniscal tears, but it is not certain, in particular in nondisplaced tear or in younger children with prominent meniscal vessels. MRI allows accurate characterization of various tear patterns, which can be instrumental for patient counseling and surgical planning. Familiarity with the normal anatomy of a growing patient, common anatomic variants, and indirect secondary signs of meniscal tears as well as usual differential diagnostic choices in children, particularly bone bruise, proximal tibiae fracture, ligamentous lesion and juvenile osteochondrosis, can help in reducing interpretation errors.31,32 Nondisplaced small tears in younger patients may heal spontaneously and a high threshold for surgery is recommended. In case surgery is needed, repair is preferred over partial resection in children and adolescents, due to better vascularization.33,34 Post-operative rehabilitation after repairing is important, while progressive strengthening and gaining the movements will be reached under physical therapist’s guidance.
Footnotes
Author contributions
J.C. contributed to study design, manuscript writing and final editing, and manuscript approval. J.S. contributed to study design, manuscript writing and editing, and manuscript approval.
Data availability
Data availability is not an applicable issue in this systematic review without any patient series.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.S. is the member of International Editorial Board of Journal of Children’s Orthopedics. Otherwise, there are no conflicting interests.
Ethical statement
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. According to official instructions by the local ethical boards of the study institution, this study was not evaluated by a review board, due to study design (current concepts review), while no patients were contacted for the study purpose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.