
Abstract
Purpose
To review all paediatric ankle syndesmotic injuries occurring at our institution and identify risk factors associated with operative intervention.
Methods
Among 22 873 evaluations for ankle trauma, we found 220 children suffering from syndesmotic injuries (incidence: 0.96%). We recorded demographic data, details of the injury, features on examination and treatment variables. Univariable and multivariable logistic regression modelling was performed to identify risk factors associated with operative intervention.
Results
The mean age at injury was 15.8 years (8.9 to 19.0) with a median follow-up of 13 weeks (IQR 5 to 30 weeks). A sports-related injury was most common (168/220, 76%). A total of 82 of 220 (37%) patients underwent operative fixation, of which 76 (93%) had an associated fibular fracture. Patients undergoing surgery had a higher incidence of swelling and inability to weight bear (p < 0.001). Statistically significant differences were recorded in tibiofibular (TF) clear space, TF overlap and medial clear space (MCS) between the operative and non-operative cohorts (6.0 vs 4.6 mm (p = 0.002), 5.4 vs 6.9 mm (p = 0.004) and 6.4 vs 3.5 mm (p < 0.001)). Multivariable analysis revealed patients with a fracture of the ankle had 44 times the odds of surgical intervention, patients with a closed physis had over five times the odds of surgical intervention and patients with a medial clear space greater than 5 mm had nearly eight times the odds of requiring surgical intervention.
Conclusions
Operative ankle syndesmotic injuries in the paediatric population are often associated with a closed distal tibial physis and concomitant fibular fracture.
Introduction
Injuries to the ankle syndesmosis, termed ‘high ankle sprains’, can affect high-level and recreational athletes and have been related to delayed return to play and persistent pain, and adult injuries have been associated with longterm disability. 1 The most common mechanism involves external rotation and dorsiflexion of the foot, with injury to the anterior inferior talofibular ligament (AITFL), posterior inferior talofibular ligament (PITFL) or the interosseous ligament (IOL).1,2 Children most at risk for syndesmotic injuries participate in sports that involve cutting and pivoting (football, soccer) or sports with rigid immobilisation of the ankle (skiing, hockey).1,3 The reported incidence of syndesmotic ankle sprains as a percentage of all ankle injuries is between 1% and 11% in adults but there is no reported incidence of syndesmotic injuries within the paediatric population.4,5
The purpose of this report is to review our experience with syndesmotic ankle injuries in the paediatric and adolescent population focusing on patient, injury and treatment factors associated with the ability to return to sports (as reported by the patient) and risk factors associated with operative intervention. We hypothesise that higher-grade injuries will be associated with increased time to return to sports and that operative intervention for syndesmotic injuries occurs more commonly in skeletally mature than in skeletally immature patients.
Patients and Methods
We performed an IRB approved (protocol no. IRB-P00008624), retrospective, single tertiary referral centre study of 220 consecutive children who were aged 18 years or younger, treated for a syndesmotic ankle injury between January 2003 and January 2013 in our multiple paediatric orthopaedic surgeon group. Patients were identified through an electronic search using ICD-9 (845.03) and appropriate CPT codes (27829), including a clinic note word search for terms such as syndesmosis sprain, open treatment of syndesmotic disruption, high ankle sprain, AITFL, PITFL and IOL injury/tear/sprain. The demographic variables, injury event details and clinical examination features were recorded for each patient (Table 1). Charts were reviewed to verify accuracy of diagnosis, which we defined as patients with (Fig. 1):
Abnormal radiographic widening of the ankle syndesmosis on static radiographs (Table 2) with associated fibular/tibial fracture or without associated fracture. Standard adult criteria were used to define radiographic widening based on historical precedent;1,6–11
Normal radiographs (stress radiographs were not used in this study) with MRI of the ankle demonstrating injury to at least one of AITFL, PIFTL or IOL; or
Normal radiographs, MRI not obtained or MRI obtained and syndesmotic ligaments intact, but injury mechanism and physical examination (tender over syndesmosis, positive ‘squeeze’ test, pain with foot external rotation) strongly consistent with syndesmotic ligament injury.
Characteristics of the cohort.
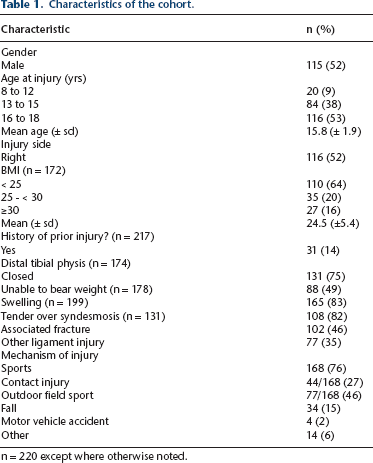
n = 220 except where otherwise noted.
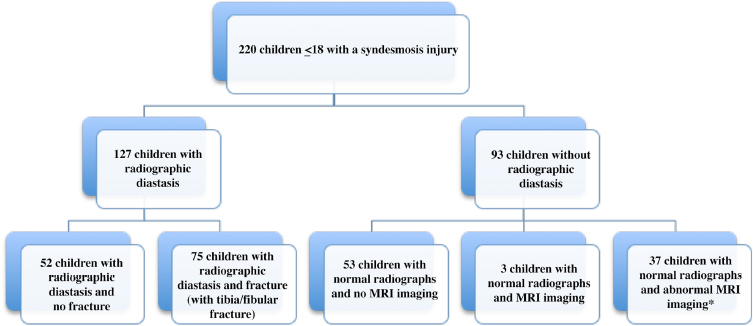
Flow chart showing the study population.
To calculate the incidence of syndesmotic injuries, we identified all patients seen during the study period with any ankle derangement as per ICD-9 codes.
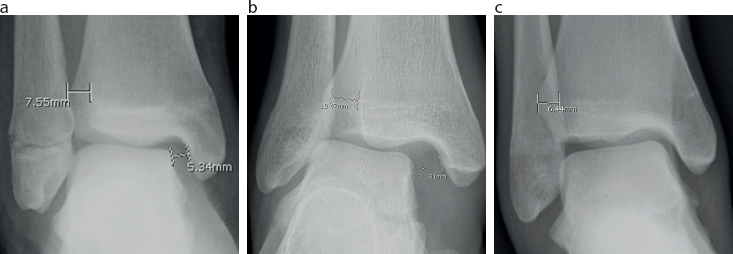
Anteroposterior (AP) and mortise ankle radiographs were reviewed to assess for signs of syndesmotic widening. Specifically, the tibiofibular (TF) overlap (on AP and mortise radiographs), TF clear space (on AP and mortise) and medial clear space (MCS) (on mortise only) were measured by study authors and classified using previously described technique and parameters (Table 2 and Fig. 2).1,6–11
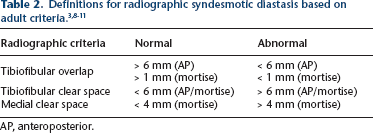
AP, anteroposterior.
(
Outcome variables studied for the cohort included time to return to weight-bearing, time to return to sport (when indicated by patient and recorded in clinical notes), pain at follow-up, treatment (surgical vs non-surgical), complications and re-injury.
Radiographic variables of TF overlap, TF clear space and MCS were recorded as mean and standard deviation. Further analysis was performed to determine if cutoff values existed for indication of surgical intervention. Receiver operating characteristic (ROC) analysis was used to assess the discriminatory ability of each radiographic measure with respect to surgical intervention. The optimal cutoff value for each radiographic measure was identified using Youden's Index. 12
Patient and injury characteristics were compared across patient subgroups using Student's t-test, chi-squared tests or Fisher's exact tests, as appropriate. Outcomes, including time immobilised, time to return to sports and pain at follow-up, were analysed across subgroups using general linear modelling, the Cochran-Armitage test for trend and binary logistic regression. The log transformation of time immobilised and time to return to sports were used in order to meet the assumptions of the general linear model. All tests were two-sided and p < 0.05 was considered significant.
Univariable and multivariable logistic regression modelling were performed to identify risk factors associated with operative intervention. Backward model selection procedures were used based on Akaike's information criteria (AIC). 13 Final model fit was assessed using the likelihood ratio test. Comparisons were conducted between a model using the current radiographic cutoff values based on abnormal definitions for the adult population1,8–11,14 and with a model using discriminant cutoffs based on ROC analysis. Models were compared using AIC and McFadden's pseudo R2 values. In general, smaller AIC and higher pseudo R2 indicate better model fit. The final logistic regression model was tested and validated using a 75% holdout dataset for model fitting and validation was conducted on the remaining 25% with random data splitting run 100 times. The model exhibited excellent stability, significance, discrimination and calibration across all iterations, indicating its ability to be used for predictive purposes. Using this model, an algorithm was developed to indicate the probability that an injury underwent surgical intervention based on significant clinical and imaging factors.
Results
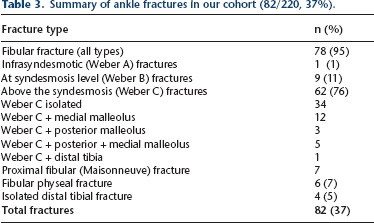
The demographic characteristics and injury specific information are shown in Table 1. During the ten-year study period a total of 22 873 patients were seen in our clinic for ankle complaints, resulting in an overall incidence of syndesmotic injury of 0.96% (220/22 873). A sports-related injury was most common (168/220, 76%), with basketball and football being most associated with syndesmotic injury. Patients presented to clinic at a median of three days after injury (IQR 1 to 7 days) and 97% of patients presented within one month of injury. There were 82 fractures within our cohort and the majority were fibular fractures above the syndesmosis (Weber C) as shown in Table 3.
Summary of ankle fractures in our cohort (82/220, 37%).
Radiographs were available for review in 190/220 (86%) cases; however, in 29 of the 190 cases, portions of the radiographs were excluded from review (most commonly due to inadequate mortise view or difficulty with measurements due to significant fracture). In total, 64 patients (64/220, 29%) underwent MRI to further characterise their injury. The decision to obtain an MRI was made by the treating physician at the time of injury to further evaluate the syndesmosis. An abnormality of at least one of the three syndesmotic ligaments was noted in 58/64 (90%) patients. The AITFL was the most commonly injured ligament (57%, among those that had an MRI) with 18/64 (28%) complete tears and 25/64 (39%) sprain/partial tears. The IOL was completely torn in 3/64 (5%) patients and 27/64 (42%) had sprain/partial tears. A total of 13/64 (20%) patients had a PIFTL sprain/partial tear.
Non-operative treatment was successful in 138 patients. Of these patients, 13 were casted for a median of 3.2 weeks while 88 were placed into an air cast boot for a median of 3.9 weeks. Total immobilisation time was 4.1 weeks. Two patients suffered a minor ankle re-injury during the follow-up period.
A total of 82 patients (37%) underwent surgical fixation of their syndesmosis injury. The most common indication for syndesmotic fixation was abnormal radiographic diastasis (53 cases) followed by documented intra-operative instability of the syndesmosis in the setting of fracture fixation (23 cases). In the remaining six patients (none of whom had fractures), borderline radiographs combined with severe syndesmotic injury on MRI prompted examination under anaesthesia in the operating room to check for instability followed by syndesmotic stabilisation.
Time from injury to surgery was 6.2 ± 4.8 days (0 to 21). Surgical fixation of the syndesmosis commonly occurred in the presence of associated ankle fractures (75/82, 91%). Combined fracture and syndesmosis fixation was used in 59 patients. The remaining 23 patients who underwent isolated syndesmotic fixation (without simultaneous fracture fixation), included 16 patients with fractures and seven patients with syndesmotic injuries in the absence of fracture.
The seven patients with isolated syndesmotic fixation in the absence of a fracture were closely reviewed. In six patients, radiographs showed borderline diastasis and five underwent subsequent MRI which revealed severe syndesmotic ligament injury patterns including four complete AITFL tears with IOL injuries and one complete IOL tear. All six had a stress examination under anaesthesia, which subsequently revealed syndesmotic diastasis which led to syndesmotic fixation. The indication for surgery in the last case was clear diastasis on radiographs.
Risk factors for surgical intervention were assessed (Table 4). Surgical intervention was significantly associated with older age (p = 0.03), inability to weight-bear on presentation (p < 0.001), presence of an associated fracture (p < 0.001), a closed distal tibial physis (p = 0.02) and abnormalities in all five radiographic measurements. Time to return to weight-bearing was 7.6 weeks in the operative group compared with three weeks in the non-operative group (p < 0.001). Return to sport was three times longer in the operative group compared with the non-operative group (21.7 weeks vs 7.8 weeks, p < 0.001).
Analysis of risk factors for surgical intervention.
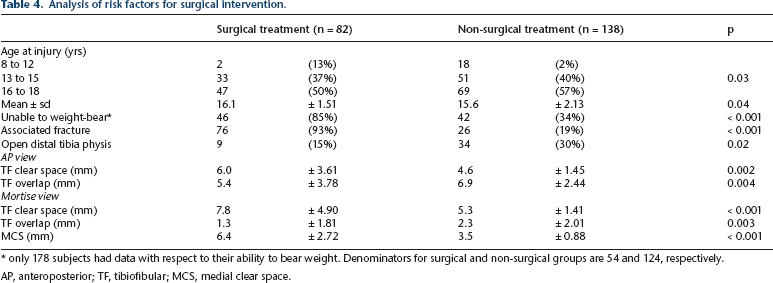
only 178 subjects had data with respect to their ability to bear weight. Denominators for surgical and non-surgical groups are 54 and 124, respectively.
AP, anteroposterior; TF, tibiofibular; MCS, medial clear space.
ROC analysis determined that all five radiographic measurements reviewed showed discriminant ability for surgical intervention with AUCs in the range of 0.62 to 0.87 (Table 5). MCS and TF clear space (mortise) had the highest discriminant abilities where an 87% probability of surgical intervention existed if the MCS was > 5 mm and a 76% probability if the TF clear space (mortise) was > 7 mm.
ROC analysis with sensitivity and sensitivity for each radiographic measurement and cutoff.

AUC, area under curve; M, mortise view; TF, tibiofibular; AP, anteroposterior view.
Multivariable logistic regression analysis determined that the presence of a fracture, a closed physis, increased MCS (mortise), and increased TF clear spaces (mortise) were the best predictors of surgical intervention. A comparison was conducted between the model using the available adult abnormal radiographic cutoff values with the model using the newly identified discriminant cutoffs in the adolescent population. The model using the newly identified discriminant cutoffs had the lowest AIC value compared with other models considered and was nearly eight units lower when compared with the model using the adult cutoffs (AIC = 80.5 and 88.4, respectively). The pseudo R2 value for the new adolescent cutoff model was higher than the adult cutoffs (76% and 73%, respectively) confirming better model fit.
The final logistic regression model (Table 6) was tested and validated and a prediction algorithm was developed to indicate the probability that an injury underwent surgical intervention based on the presence of a fracture, status of the distal tibial physis, MCS > 5 mm (mortise) and TF clear space > 7 mm (mortise) (Table 7).
Comparison of risk factors for surgical intervention.
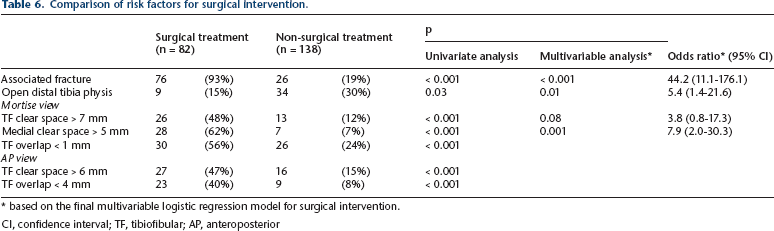
based on the final multivariable logistic regression model for surgical intervention.
CI, confidence interval; TF, tibiofibular; AP, anteroposterior
Probability algorithm for surgical intervention.
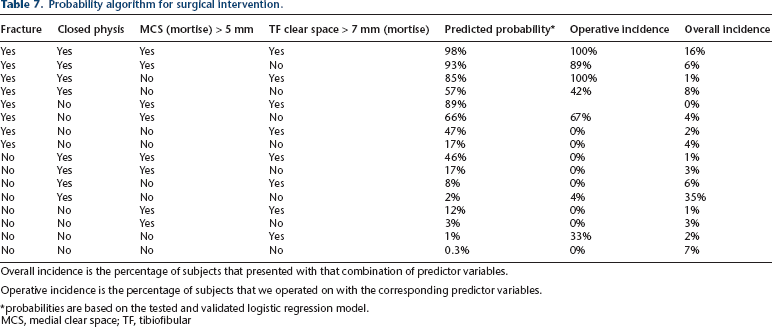
Overall incidence is the percentage of subjects that presented with that combination of predictor variables.
Operative incidence is the percentage of subjects that we operated on with the corresponding predictor variables.
probabilities are based on the tested and validated logistic regression model.
MCS, medial clear space; TF, tibiofibular
Discussion
The purpose of this study was to report our experience in treating a large sample of adolescent patients with syndesmotic injuries and identify the indications associated with operative intervention. Our primary findings were that syndesmotic injuries were rare (incidence 0.96%) and that older age, closed distal tibial physis, presence of an associated fracture, MCS (mortise) > 5 mm and TF clear space (mortise) > 7 mm were all significantly associated with operative intervention which was associated with a longer time to weight-bearing and to return to sports.
In our cohort, a total of 43 patients had syndesmotic injuries in the presence of an open physis and only nine of these patients required surgical fixation. When looking at these nine patients, only one presented with a purely ligamentous injury with widening of the syndesmosis; the remaining eight suffered fractures around the ankle requiring operative fixation. This finding illustrates the concept that an open physis is protective against purely ligamentous injuries to the syndesmosis requiring surgical fixation. Of note, this study focused on functional injury to the syndesmosis and did not include bony syndesmotic equivalent injuries, such as the isolated juvenile Tillaux fracture.
Static syndesmotic diastasis has been defined in adults with radiographic parameters such as MCS (mortise) > 4 mm, TF overlap (AP) < 6 mm or TF clear space (mortise) > 6 mm.1,8,11 Similar parameters have not yet been established in children and adolescents. Bozic et al 14 found that the criteria to evaluate the integrity of the syndesmosis in adults do not apply to children. In our younger population, we found that MCS (mortise) > 5 mm, TF overlap (AP) < 4 mm and TF clear space (mortise) > 7 mm were more appropriate cutoffs than the adult standards to indicate surgical intervention. To our knowledge, this is the first study to outline these radiographic guidelines in children and adolescents with suspected syndesmotic injuries.
The use of MRI is increasing for syndesmosis injuries; and in adults has been shown to be 93% to 100% sensitive and specific for both AITFL and PITFL tears. 15 Interestingly, in our cohort MRI was more often used in the non-operative group (57 patients) even though syndesmotic ligament injury was commonly identified (90%) indicating that MRI results often confirmed the syndesmosis was not widened. Six patients with MRI findings consistent with multiple syndesmotic ligament disruption ultimately underwent stabilisation following documented instability under anaesthesia. The seven patients who required syndesmotic fixation in the absence of fracture serve as a reminder to the treating physician to be suspicious of syndesmosis injury in the clinically appropriate setting even with normal radiographs.
As a group, we do not rely on MRI findings to guide surgical intervention. In the vast majority of cases, syndesmotic fixation was performed in the setting of obvious radiographic diastasis (53 cases) or documented intraoperative instability of the syndesmosis in the setting of fracture fixation (23 cases) or without fracture (six cases). Documented instability was determined intra-operatively through a fluoroscopic examination under anaesthesia using either an external rotation stress or the Cotton test 16 to assess for diastasis at the syndesmosis using radiographic parameters. Techniques for reduction and fixation of the syndesmosis varied but most commonly involved indirect reduction using a reduction clamp between the distal fibula and tibia. Fluoroscopic comparison to the contralateral ankle was used to assess reduction in skeletally immature patients. The most common fixation technique involved one or two metal screws to position and hold but not compress the syndesmosis. Bioabsorbable screws (two cases) or suture button fixation (six cases) were less commonly used.
There is limited guidance for the operative management of paediatric syndesmotic ligament injuries. To aid with treatment, we created a probability algorithm based on the four multivariable predictors for surgery (presence of a fracture, closed physis, MCS (mortise) > 5 mm and TF clear space (mortise) > 7 mm) (Table 7). Presence of a fracture and any two of the other three predictors resulted in at least an 85% likelihood of surgical intervention. While all patients with radiographic diastasis require intervention, this algorithm serves to guide physicians in caring for paediatric syndesmotic injuries when the diagnosis or decision for surgical intervention may not be as clinically straightforward.
The strength of this paper is that it describes a large series of patients (n = 220 operative; > 22 000 visits overall) and examines a topic that has rarely been reported in the literature. Additionally, MRI characteristics of syndesmotic injuries in this younger population are described in a large number (64/220, 29%) of patients. Based on this study, children/adolescents with suspected syndesmotic injury may need greater radiographic displacement compared with adults to be considered for surgical intervention.
There are several notable limitations to this study. The retrospective design suffers from inherent selection and recall bias. Follow-up was short given that most patients made a full recovery. No prospective or functional data were collected. Our inclusion criteria relied on physician diagnosis; therefore, the calculated incidence likely underestimates the true incidence as cases may have been missed. Outcome measures such as time to weight-bearing and to return to sports are likely to be influenced by a combination of injury severity and the treating physician's preference. Finally, we used the decision to operate as a major outcome measure. Our surgical indications were defined above; however, this definition can be subjective and vary among treating physicians in borderline cases, especially for dynamic intraoperative syndesmotic instability.
Despite these limitations, this is the largest study to date reviewing syndesmotic injuries in the paediatric population. Operative ankle syndesmotic injuries in this age group are most often associated with a closed distal tibial physis and concomitant fibular fracture. Closed distal tibial physis may simply be associated with patient age and not an independent risk factor for syndesmosis injury although this is unclear. This study will serve as a foundation for future prospective multi-centre studies investigating indications for surgery and long-term outcomes within this population.
Footnotes
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Institutional IRB approval was obtained for this study (protocol no. IRB-P00008624). This article does not contain any studies with human participants or animals performed by any of the authors.
Y-M Yen declares he is a consultant to Orthopediatrics and Smith-Nephew.