
Abstract
Abstract
Objective
To evaluate the clinical and functional results of surgical treatment of patellar dislocation in children.
Material and methods
A prospective study was undertaken from January 1995 to December 2004. Patients who suffered from patellar dislocation after receiving intramuscular antibiotic injections to quadriceps were recruited. A complete history of each patient was recorded, and both a clinical and a roentgenographic examination were performed preoperatively. Patellar dislocation was classified according to Bensahel's criteria. The iliotibial tract and lateral retinacula was released to restore the tension of the medial retinaculum. Quadricepsplasty was used in all patients for full flexion of knee.
Results
There were nine males and 65 females in this study. All 74 patients (76 knees) developed dislocation of the patella after repeated intramuscular injections of antibiotic(s) into the quadriceps muscle. Fifty-six knees (73.7%) were type 1, and 20 knees (26.3%) were type 2 (Bensahel's classification). In all, we attained excellent results in 56 knees (73.7%), good results in 17 knees (22.4%), and fair results in three knees (3.9%). There have been no poor results or recurrences so far.
Conclusion
Use of the iliotibial tract, adequate lateral retinacular release, restoration of the tension of the medial retinaculum and associated quadricepsplasty achieved a high success rate. The technique is simple, safe and effective in skeletally immature children.
Keywords
Introduction
Dislocation of the patella is one of the most common problems seen in orthopedic practice and it has been well documented that dislocation causes chronic knee pain and instability in the pediatric and adolescent population. Baum and Bensahel [1] in 1973 and Bensahel et al. [2] in 2000 presented deformities in dislocation of the patella and emphasized the concept of developmental dysplasia of the patella (DDP).
There are many proposed mechanisms for this disorder, such as patellofemoral mechanism, dysplasia of distal femur, imbalance between lateral and medial retinacula (such as fibrous quadriceps caused by intramuscular antibiotic injection). A great number of surgical procedures have been described for realignment of the patellofemoral mechanism. Proximal realignment procedures alter the medial and lateral position of the patella by balancing the soft tissues proximal to its inferior pole. Lateral retinacular release, medial retinacular or capsular plication, vastus medialis oblique advancement, and medial patellofemoral ligament repair or reconstruction are included in this category. However, there is no single procedure that is appropriate for all cases because of variations among patients [3–5]. Soft tissue operations are advisable during growth to avoid secondary deformities such as recurvatum, which can occur when the tibial tubercle is disturbed in childhood [6]. Since 1995, we have used the iliotibial tract to treat dislocation of patella in children. The reasons for using the iliotibia tract are simplicity and its effectiveness in holding the patella in the patellar groove. The purpose of this study was to evaluate the long-term results of this technique.
Materials and methods
From January 1995 to December 2004, 74 patients [76 knees (two patients with bilateral dislocation)] formed the basis of this study. There were nine males (12.2%) and 65 females (87.8%) in the study. The patient was operated on by only one surgeon: the author. All pertinent clinical and operative records were prospectively reviewed.
Clinical and roentgenographic examinations
A complete preoperative history of dislocation was recorded. The affected knees were evaluated preoperatively and postoperatively on the basis of the symptoms, signs, and roentgenographic findings. The examination was performed in the standing, sitting, and supine positions. The examiner looked for evidence of lateralization of the extensor mechanism and tilt. The patellar compression test should be performed with flexion and extension of the knee to evaluate articular click or pain. The Q angle is the angle measured between a line connecting the anterior superior iliac spine and the midpatella and a line connecting the midpatella to the tibial tubercle [7–11]. The apprehension sign was elicited by the examiner while attempting to dislocate the patella laterally with the quadriceps muscle relaxed and the knee in 30° of flexion. The sign was positive when the patient became apprehensive and uncomfortable as the patella reached the point of maximum passive displacement or when any further displacement was resisted by the patient when attempting to straighten the knee in order to pull the patella into the normal position. We calculated this angle in all of our patients.
Genu valgum was determined by goniometer with the patient standing. The range of motion was estimated using the opposite knee as a control unless both knees were involved. A range of 0–150° was used as the norm.
The roentgenographic examination included an anteroposterior view with the knee in extension, a lateral view with the knee flexed at 30°, a tunnel view made with the knee flexed, and infrapatellar or skyline views made with an X-ray beam tangential to the patella and the knee in various degrees of flexion to demonstrate the patella without overlapping of the femur or tibia.
Lateral tilt of the patella was diagnosed when the space between the medial patellar facet and the medial femoral condyle, as seen on the infrapatellar view, was increased compared to that between the lateral patellar facet and the lateral femoral condyle.
Patella alta was diagnosed using the Insall and Salvati method [12]. The ratio between the length of the patella and the length of the patellar tendon is normally 1.02 ± 20%.
Classification of patellar dislocation
Our patients were classified according to Bensahel's criteria [2]: (1) type 1, dislocation of the patella without major radiographic abnormality; (2) type 2, dislocation of the patella with major femoropatellar dysplasia, namely a patella alta and a flat or convex trochlea.
Conservative treatment
The patient was positioned supine, and flexion and extension of the knee were performed with the patella held in the intercondylar groove of the knee. The patella was mobilized in superior–inferior and medial–lateral movement. One hour of practice a day was carried out over six weeks. After each physical therapeutic practice, the knee was placed in a plastic splint with the knee maximally flexed but without patellar dislocation. The knee flexion was gradually increased. If after conservative treatment the patient had recurrent patellar dislocation when the knee was flexed, a surgery was performed.
For patients with habitual patellar dislocation or with more than two dislocations, operation was performed immediately without conservative treatment.
Surgical procedure
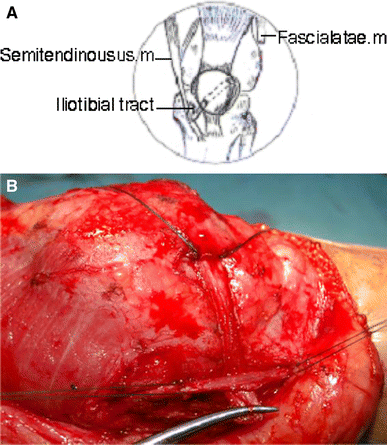
The patient was positioned supine on a standard operating table, under general anesthesia, and the anterolateral part of the thigh was exposed. We used the anterolateral approach, which extended from the mid-third of the thigh to the tibial tuberosity. The incision was slightly curved to follow the lateral border of patella. The subcutaneous tissues were undermined sufficiently to create a skin flap that would expose the quadriceps muscle, the medial and lateral retinaculum of the patella, the iliotibial tract, the semitendinosus insertion, and the patellar tendon. This incision avoided penetration into the capsule and the infrapatellar nerve. The operation was performed in three stages.
The first stage involved releasing the lateral retinacular patella and restoring the tension of the medial retinaculum using No. 3 Ethibond sutures while holding the patella in the normal position and allowing 25% lateral translation with the knee flexed 45–60° (Fig. 1B, C).
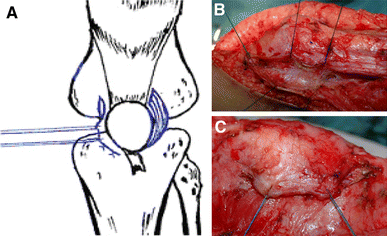
These images belong to left knees during operation.
The second stage involved releasing the iliotibial tract 3″ above the superolateral border of the patella (Fig. 2B), suturing the remaining proximal end to the fascial thigh, and creating a tunnel between the front face of the patella and the patellar aponeurosis from the superolateral border to the inferomedial border (Fig. 3B). The iliotibial tract was passed through the tunnel (Fig. 4B), while the patella was translated medially and distally. The iliotibial tract was sutured to the patella, and the free end of the iliotibial tract was sutured to the insertion of the semitendinosus muscle with the knee flexed 45–60° using No. 3 Ethibond sutures (Figs. 4, 5B).
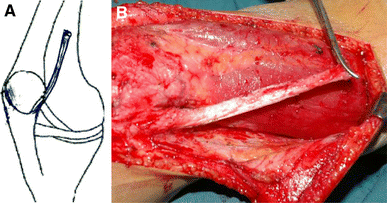
These images belong to left knees during operation.
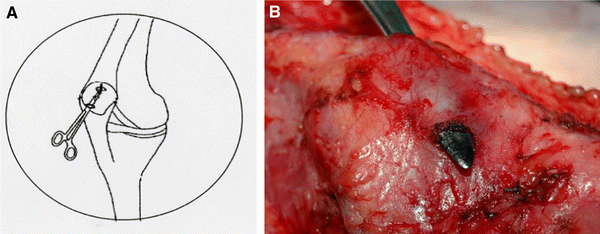
These images belong to left knees during operation.
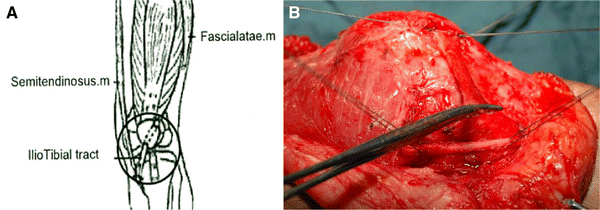
These images belong to left knees during operation.
These images belong to left knees during operation.
During the third stage, the contracted components of the quadriceps muscle were identified by forcibly flexing the knee, and they were reconstructed by a quadricepsplasty procedure of the distal part with the tendon lengthened by V–Y plasty to achieve passive full flexion of the knee.
Upon completion of the release, complete hemostasis was achieved by the coagulation of all sources of bleeding, especially the lateral superior geniculate artery at the superolateral border of the patella. The skin was closed without leaving drainage; the lower extremity was placed in a cast with the knee flexed at 60°.
Intraoperative biopsy
Biopsy specimens of the muscular vastus lateralis, medialis, intermedialis, rectus fermoris, fasciae latae, lateralis, and medial retinacular patella were done to find tissue abnormalities.
Postoperative rehabilitation
Postoperatively the knee was placed in a double capsule cast with the knee flexed 45–60° (cf. Fig. 6). The double capsule cast was a long cast placed from above the knee to the toe, and the cast was divided into two parts, an anterior part and a posterior part. The double capsule cast could easily be removed before practice. After each practice session both parts were put back in place using rolling bands. Patellar mobilization in the superior–inferior and medial–lateral directions was started three days after the operation to prevent parapatellar contractures. During the first two weeks a passive range of motion up to 60° was performed with a physiotherapist. After two weeks the range of motion was increased up to 90°. After three weeks the range of motion was increased to normal. The cast was removed after about six weeks, but without weight-bearing. Patients were allowed to bear 25% of their body weight for the first two weeks, and 50% of their body weight the following two weeks. Full weight-bearing was allowed between the fourth and sixth week after cast removal.

These images belong to left knees during operation. Postoperatively, the knee is placed in a double capsule cast with the knee flexed 45–60°
Follow-up
Patients were re-examined at three and six weeks, three and six months, one year, and afterwards every year.
We classified the results of the operations according to Kumar [13], with an objective evaluation undertaken using the Fulkerson [9] and Kujala [14] functional knee-scoring systems. The scores were graded as follows:
Excellent: 90–100 points Good: 80–89 points Fair: 70–79 points Poor: <70 points
Results
From January 1995 to December 2004, 74 patients (76 knees) were operated. The mean age of the patients at the time of surgery was ten years and three months (range, seven years and six months to seventeen years and four months). Twenty-nine right knees and 43 left knees were affected; two patients [2.7% (one male and one female)] had bilateral problems. Seventy-four (74) patients (76 knees) developed dislocation of the patella after repeated antibiotic intramuscular injections into the quadriceps muscle. Most of those injections were performed within the first 24 months of life. The medical agents that had been injected were all antibiotics: penicillin, gentamycine and others like lincomycin, streptomycin, and cloxacilin. In the patients there was no history of trauma or family history of patellar dislocation, genu valgum or other congenital diseases. Two knees (2.6%) had habitual patellar dislocation (the patella rested laterally at all times) and the remaining 74 knees (97.4%) had recurrent patellar dislocation. Due to post-injected quadriceps fibrosis and contracture, if the patella was held in the intercondylar groove, the knee could not flex beyond 30°.
Eleven patients had stiffness in one knee and stiffness in the contralateral knee with dislocation of the patella. The recovery of thigh atrophy was highly significant:P = 0.0000 (see Table 1). Preoperatively, limited medial translation of the patella proved slackness or contracture of the lateral patellar retinacula. After the intervention the patella could be moved normally in superior–inferior and mediallateral directions at 30° of knee flexion. The average preoperative Q angle was 15.5° [range, 12°–22° (there were two knees with a Q angle of more than 20°)]; postoperatively, the average Q angle was 8.8° (range, 5–14°).
Clinical signs before and after the operation

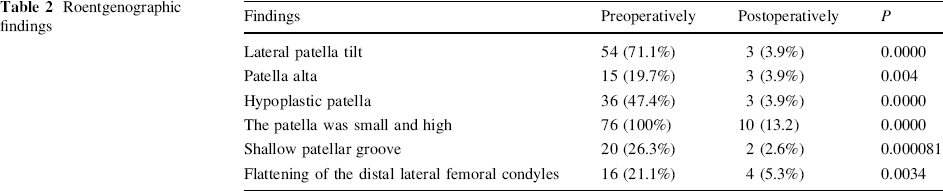
Preoperatively there were shallow patellar grooves in 20 knees, 16 of which had a flattening of the distal lateral femoral condyle, while postoperatively only four knees showed a shallow patellar groove (see Table 2).
Roentgenographic findings
Classification of patellar dislocation
Type 1: 56 knees (73.7%), and type 2: 20 knees (26.3%).
We performed muscular biopsy intraoperatively. The results of the biopsy showed marked fibrous muscular lateral vastus, intermedius vastus, and lateral retinacular patella. Degeneration of the medial vastus and the rectus femoris was also noted. All of these signs were also seen with fibrosis of the quadriceps, the triceps, the gluteal, and the deltoid muscle after antibiotic intramuscular injections. The quadriceps muscle was usually shortened due to severe degrees of fibrosis.
The vastus lateralis muscle was markedly fibrosed, contracted and shortened. The iliotibial tract was attached to the distal vastus lateralis muscle. The lateral retinacular patella was thick and fibrous.
The insertion of the muscular vastus lateralis into the upper pole of the patella was seen clearly and fibrous tissue developed around its lateral aspect, distinct from the rest of the fascia lata. The iliotibial tract was attached to the muscular vastus lateralis about 2.5–5 cm above the superolateral patella by fibrous tissues. For that reason the tendon of the vastus lateralis, the connecting band, and the iliotibial tract had to be divided in turn before the patella would remain in the intercondylar groove and knee without dislocation of the patella during full passive flexion of the knee.
The average length of follow-up was five years and one month, ranging from three years and four months to nine years and three months. Long-term follow-up showed excellent results in 56 knees (73.7%), good results in 17 knees (22.4%), fair results in three knees (3.9%), and poor results in no knees. There was no redislocation or subluxation in any of the knees. The mean Kujala score was 58.3 points (range, 33–86) preoperatively and 97.4 points (range, 76–100) at final follow-up.
Discussion
The etiology of patellar instability requires a thorough physical and radiographic examination. The causes may include genu valgum, genu recurvatum, patella alta, patellar dysplasias, femoral anteversion, external tibial torsion, ligamentous laxity, trauma, congenital abnormalities, arthrogryposis multiplex congenital and syndromes such as nail patella and Down Syndrome [15–18]. Lateral patellar dislocation also may occur after repeated antibiotic intramuscular Injections which cause stiffness of the knee.
Williams reported 26 patients with stiffness of the knee and 13 of them with dislocation of the patella [19], Alvarez [20], Dennis [21], Mukherjee [22], and Sharrard [23] reported stiffness of the knee with dislocation of the patella. Those patients developed dislocation of the patella after repeated antibiotic intramuscular injections into the quadriceps muscle. Our study found a history of repeated antibiotic intramuscular injections into the quadriceps muscle in all patients, which caused thigh atrophy. The patella was held in the intercondylar groove so that the knee could not flex beyond 30°. All parts of the quadriceps except the vastus medialis were involved, and there was also an abnormal attachment of the iliotibial tract. The quadriceps muscle was usually shortened and fibrous. In the majority of the cases fibrosis developed into the deep part of the vastus lateralis and onto the fascia lata on the lateral side of the thigh and the lateral and superior aspects of the patella to create an imbalance between the medial and lateral muscle forces on the patella, thereby causing lateral patellar dislocation. Furthermore, this fibrosis also diffused into the lateral retinacular patella, which was shown by the patellar medial glide test to be <5 mm at 30° of knee flexion. Fibrous tissue of the lateral vastus, intermedius vastus, and lateral retinaculum were shown even more clearly in muscular biopsy. All of these fibroses were identical to those of the triceps, gluteal, and deltoid after repeated antibiotic intramuscular injections. In all patients there was no history of trauma, family history of patellar dislocation or other congenital diseases. That is why we thought that lateral dislocation of the patella may be caused by a postinjected fibrous quadriceps muscle.
Baum and Bensahel [1] in 1973 and Bensahel et al. [2] in 2000 presented deformities in dislocation of the patella and emphasized the concept of DDP. DDP includes bone, muscle, and ligament pathologic lesions. DDP refers to the abnormal growth and development of the anterior portion of the knee and related structures. The pathologic change in each of these tissue elements must be appreciated to restore normal alignment and function of the extensor mechanism. The distal end of the femur may have a complete absence of the trochlear groove in cases of congenital dislocation. In lesser degrees of dysplasia, lack of development of the trochlear groove was characterized by a low lateral femoral condyle. The lateral femoral condyle usually was the highest part of the distal femur viewed in cross-section to resist lateral displacement of the patella [24]. When the lateral femoral condyle was hypoplastic, there was less bony resistance to lateral displacement of the patella. However, development of the trochlea seems to be in response to a normal functioning quadriceps mechanism. When the patella is realigned in a young child, development of the trochlear groove occurs during continued growth and development. In cases of bone dysplasia such as spondyloepiphyseal dysplasia or Ellis–van Creveld syndrome, the degree of genu valgum that develops because of abnormal bone growth may create such a strong lateral vector that dislocation of the patella occurs either full-time or intermittently [11]. The major component of correction in these cases is osteotomy, which realigns the vectors of action of the quadriceps muscle and is the most important element in establishing normal patellofemoral joint function. Muscular dysplasia and the associated quadriceps mechanism cause the lateral abnormal deviation of the patella. The most consistent pathologic finding in patellofemoral joint dysplasia was the lateral soft tissue contracture, which caused deviation and malalignment of the mechanism of the quadriceps muscle, the patella, and the quadriceps tendon.
This contracture was most severe in persistent lateral dislocation of the patella. This malalignment generated a lateral vector that had to be considered and often surgically corrected in cases of patellofemoral dysplasia. The quadriceps muscle was weak and often was shortened. The medial muscles were underdeveloped or weak, in need of operation to support centering of the patella in the trochlear groove and to realign the vectors of action of the quadriceps muscle. The hamstring muscles were in some cases shortened and the posterior capsule knee was contracted [25]. Ligament dysplasia: in cases of severe dysplasia such as those seen in congenital dislocation of the patella, the pathologic features of the capsule were similar to those of arthrogryposis in that the joint capsule was contracted and constricted, causing the volume of the joint to decrease. Anatomists consider the patellar ligament to be an extension of the quadriceps tendon that is continued distal to the patella to insert into the tibial tubercle. The lateral placement of the tibial tubercle is associated with an abnormal lateral insertion of the patellar ligament.
In this study, bone dysplasia, the small and hypoplastic patella, was seen in all cases. Furthermore, roentgenographic examination showed a marked shallow patellar groove in 20 knees (26.3%) and a flattening of the distal lateral femoral condyles in 16 knees (21.1%). In all knees lateral retinacular patella was thick and fibrous, and medial retinacular patella was thin and wide. Patella alta was observed in 15 knees (19.7%). Nevertheless, our surgical technique only restored muscular and ligament components as bony interventions were not recommended in children. In 1964 Brattstrom [26] originally defined the Q angle as the supplement angle to the valgus angle of the extensor mechanism formed by the quadriceps’ resultant + the patella + the ligamentum patellae. The Q angle varied depending on the amount of knee flexion and foot position; it increased with foot pronation and external tibial rotation [11], and if the patella was subluxed laterally, then the central reference point of measurement was altered. When the iliotibial tract was passed through the tunnel, the patella was translated medially and distally for realignment of the patellofemoral mechanism, and as a result the Q angle was improved. In this study, the average preoperative Q angle was 15.5° (range, 12°–22°; there were two knees with a Q angle of more than 20°). Postoperatively the average Q angle was 8.8° (range, 5–14°).
Variations among patients with patellar instability suggest that one specific procedure may not be an appropriate procedure for all patients with patellar dislocation [24]. The number of different techniques for patellar realignment and stabilization reported in the literature is astonishing. In 1959 Cotta [27] counted 137 surgical methods directed at solving the problems of an unstable patella. These procedures can be classified into soft-tissue balancing procedures and bony transfer procedures. In a skeletal immature patient with open growth plates, transfer of the tibial tubercle must be avoided if possible to prevent premature physeal closure and subsequent development of genu recurvatum. In children, soft-tissue balancing procedures are widely accepted methods of treatment, such as the surgical procedure which involves a lateral retinacular release with mobilization of the vastus medialis muscle to a more distal and lateral position on the extensor mechanism. The quadriceps muscle was weak and often shortened. As a result, realigning the vectors of action of the quadriceps muscle was the most important element in establishing normal patellofemoral joint function. However, when only the quadriceps mechanism was corrected the recurrence rate was high. Many studies have published data relating to recurrent dislocation rates of between 4 and 44% [21, 28–42]. Poor results have been reported, especially when lateral release is used as a solo procedure [8, 9, 40, 43–47]. Galeazzi, Baker [6, 48] used semitendinosus tenodesis passed through the patella for repair of recurrent dislocation of the patella in children. However, this technique has some complications, such as fracture or degeneration and hypermobility of the patella, and patella alta is not fully corrected [49]. Hauser [36], while summarizing various types of operations, divided them into six groups, namely: (1) those procedures which are directed against the relaxed median capsule; (2) those in which the fascia is transplanted; (3) those in which secondary muscles are used to hold the patella medially; (4) those in which free fascial transplants are used to hold the patella medially; (5) those in which the lower end of the femur is attached; and (6) those in which the patellar ligament is transplanted.
The iliotibial tract is normally inserted into a facet on the lateral condyle of the tibia. Through this insertion the gluteus maximus and the tensor fasciae latae stabilize the slightly flexed knee during weight-bearing. However, the iliotibial tract is merely a thickened strip of the fascia lata. This fascia gives origin to the intermuscular septa of the quadriceps group of muscles, and on either side of the patella is reinforced by fibers which blend with the aponeuroses of the vastus lateralis and the vastus medialis. These fibers are stronger on the lateral side, where they arise from the iliotibial tract. The iliotibial tract lies in front of the axis of rotation of the knee joint, and passes behind that axis as the knee bends. It follows that if the patella is tethered to the tract in any way, it must be pulled laterally during flexion of the knee. The iliotibial tract is attached to the distal vastus lateralis muscle. If the vastus lateralis muscle is shortened the lateral dislocation of the patella is created when the knee flexes. The tendon of the vastus lateralis and the iliotibial tract have to be divided so that the patella can remain in the intercondylar groove when the knee is fully flexed. However, no one ever thought of using a divided iliotibial tract to keep the patella in place.
Based on all of these premises, we used the iliotibial tract for dislocation of the patella. We passed the iliotibial tract through a tunnel which was created between the front face of the patella and the patellar aponeurosis, without drilling the patella, so there was no fracture of the patella. The iliotibia tract created a force to stabilize the patella, medially aligning the quadriceps patellar tibial mechanism, and providing a balancing medial vector and distal realignment of the extensor mechanism. Our surgical technique meets all of the demands of Hinton [50] and Stanitski [51]: (1) releasing an abnormal tethering vector, (2) balancing the medial vector, and (3) aligning the quadriceps patellar–tibial mechanism. Clinical realities showed an excellent rate of 73.7%, with no poor results or redislocations, proving the preeminence of this technique.
Conclusion
Dislocation of the patella in children may be caused by repeated antibiotic intramuscular injections into the thigh. Using the iliotibial tract with adequate lateral release and associated quadricepsplasty is a safe and effective technique for dislocation of patella in skeletally immature children.