
Abstract
Objectives:
The aim of this study was to investigate changes over time in osteoarthritis risk factors most closely associated with the occurrence of total knee arthroplasty (TKA). We hypothesize that the robustness of a longitudinal case–control study will provide new information on the association between changes in various clinical and structural parameters in different time frames before TKA.
Methods:
Cases (195; TKA after cohort entry) and controls (468) matched for age, gender, income, WOMAC pain, Kellgren–Lawrence grade and follow-up duration were from the Osteoarthritis Initiative cohort. Associations between changes in sociodemographic, clinical, imaging and osteoarthritis therapies with the occurrence of TKA were performed using conditional logistic regression analyses.
Results:
Worsening of WOMAC scores (cOR 1.02–1.20, p ⩽ 0.012), KOOS (1.02–1.04, p ⩽ 0.014), knee injuries sustained in the previous 30–40 years (women 2.70, p = 0.034) and valgus alignment (1.10, p = 0.052) were associated with the occurrence of TKA. Also associated with TKA was cartilage volume loss in the lateral (overall 1.76, p = 0.025; women 1.93, p = 0.047) and medial compartments (⩾10%, overall 1.54, p = 0.027; men 2.34, p = 0.008), occurrence of medial meniscal extrusion (overall 1.77, p = 0.046; men 2.86, p = 0.028), and increase in bone marrow lesions (BMLs) for women (1.09, p = 0.048). The association of risk factors with TKA was reinforced when both an increase in WOMAC pain and cartilage volume loss (1.85, p = 0.001) were combined. Pain medication usage, mainly narcotics and intra-articular steroid injections (IASI), was also associated with TKA, with no impact on changes in cartilage loss or structure.
Conclusion:
This study provides new information about gender differences in risk factors associated with the occurrence of TKA. Worsening of valgus alignment, cartilage volume loss in the lateral compartment, BMLs and older injuries are important risk factors in women, while medial compartment cartilage loss and meniscal extrusion are in men. The use of pain medication and IASI although associated was found not causal with TKA.
Keywords
Introduction
Knee osteoarthritis (OA) is an incapacitating condition and an increasing health burden,1,2 which leads to the need for total knee arthroplasty (TKA) in a number of patients. 3
TKA, a clinically relevant and cost-effective treatment for end-stage OA, is a widely accepted outcome endpoint of OA progression.4–8 The decision to undergo TKA is multifactorial.9–11 Among the most dominant decision-driving factors are a significant worsening in pain, a decrease in function and quality of life (QoL), and radiographic OA progression years prior to the TKA procedure. 12 However, structural changes could also be assessed by magnetic resonance imaging (MRI) and although both radiography and MRI methods have shown to be predictive for TKA,4–8,13,14 the latter have been demonstrated most useful to study long-term disease outcomes.4,6–8,14
In the search for TKA predictors, most studies have been of cross-sectional design or shorter follow-up duration and focused on disease symptoms and demographic factors.11,12,15 Yet, very little information is available on gender differences in predictors or the association between the role of the changes in concomitant symptoms, varus/valgus malalignment, structural lesions and trauma with TKA on the same study population over an extended period. Varus/valgus malalignment alone, or in association with an increase in body mass index (BMI), is known to represent an increased risk for knee OA development or progression.4,16–18 A comprehensive recent meta-analysis established an urgent need for high-quality longitudinal studies looking at the causal relationship between specific biomechanical factors and the development of knee OA. 19
The main hypothesis of this study was to investigate if the robustness of using a longitudinal case–control study would provide new information on the role of various clinical and structural changes in different time frames before TKA. More specifically, we explored the association between the occurrence of TKA with the changes over time in sociodemographic, clinical and imaging (X-ray, MRI) characteristics, and OA treatment. These associations were analysed using individuals with TKA (cases) matched with controls (without TKA).
Methods
The reporting of this study conforms to the Strengthening the Reporting of Observation Studies in Epidemiology (STROBE) statement for reports of observational studies. 20
Study design
This study used a nested case–control design to evaluate the association between changes over time in sociodemographic, clinical and imaging characteristics of OA participants with the occurrence of TKA.
Study setting
Participants were from the Osteoarthritis Initiative (OAI) cohort (https://nda.nih.gov/oai/). The OAI established and maintained, through yearly visits over 108 months (9 years), a natural history database for knee OA that included clinical evaluation data, and radiological and MR images of 4796 (including the controls) men and women aged 45–79 years at the time of enrolment (cohort entry) between February 2004 and May 2006. Selected participants were from both the Progression (n = 1389) and Incidence (n = 3285) OAI subcohorts. The participants from Progression subcohort have symptomatic tibiofemoral knee OA at baseline, and the Incidence participants did not have symptomatic knee OA but had characteristics that placed them at increased risk of developing symptomatic knee OA. Written informed consent was obtained from all participants. The OAI study was approved by the Institutional Review Boards at the University of California, San Francisco (OAI Coordinating Centre; Approval No. 10-00532). Each of the four clinical sites also approved the study.
Participants
Case
Cases were composed of participants who had the first occurrence of TKA between February 2004 and October 2015 (last month of reported TKA data in the OAI database), as previously described. 11 These data represented the latest available information on TKA from the OAI database. The date on which the TKA occurred [OAI variable: V99E (L or R) KDATE] was defined as the index date. The target knee was defined as the first knee with an occurrence of TKA, notwithstanding if the patient had both knees with symptomatic OA. Cases that had missing information concerning variables used for the match with controls were excluded.
Control
Each case was matched up to four control participants (without a history of TKA before index date), as recommended 21 and previously described. 11 Matching parameters included age, gender, income level, Western Ontario and McMaster Universities Arthritis Index (WOMAC) pain, Kellgren–Lawrence (KL) grade and duration of the follow-up. Only controls who had complete information available on TKA and matching variable characteristics were selected.
Variables
Sociodemographic and clinical characteristics
Sociodemographic and clinical data were from the OAI subcohorts (Progression and Incidence) and included knee status, age, gender, race, income level, education level, BMI, WOMAC scores (pain, function, stiffness, total), 22 KOOS scores (pain, symptoms, QoL), 23 KL grade, medial JSW (mJSW), frontal plane goniometric knee alignment, cartilage volume, meniscal extrusion, bone marrow lesion (BML) and time to first reported knee injury.
Risk factors
Risk factors were defined as changes over time of sociodemographic, clinical and imaging characteristics and their association with the occurrence of TKA was evaluated. Changes over time measured the difference between the value at index date (or the last available visit before) and the one at baseline. Changes were evaluated for the following characteristics: BMI, WOMAC scores (stiffness, function, total), KOOS scores (pain, symptoms, QoL), frontal plane goniometric knee alignment, mJSW, cartilage volume, BML, meniscal extrusion, OA therapies [acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), COX-2 inhibitors, narcotics, glucosamine/chondroitin sulphate, and intra-articular steroid injections (IASI)]. Information on the usage of OA therapies was obtained from the medical history of participants (forms available at http://oai.epi-ucsf.org). The change of each OA therapy was separated into three categories: (1) unchanged, (2) started and (3) stopped.
The overtime variation in knee alignment (i.e. the evolution of the goniometric frontal plane measurements from neutral to either varus or valgus, or the change in varus/valgus angulation) was calculated as the difference in angulation between index date and baseline.
Change in cartilage volume was categorized into four overlapping threshold levels of loss: (1) >0%, (2) ⩾7%, (3) ⩾10% and (4) ⩾20%. These thresholds were selected based on the previous studies in which the extent of cartilage volume loss and TKA was found to be associated.4,8,24 Change in meniscal extrusion was defined into two categories: unchanged (extrusion or no extrusion over the follow-up period) and changed (extrusion occurred over the follow-up period). Moreover, mJSW and cartilage volume change were also assessed annually for 5 years preceding the index date, and results were stratified according to the use (yes/no) of IASI over the follow-up.
Data sources/measurement
BMI, WOMAC scores (stiffness, function, total), KOOS scores (pain, symptoms, QoL) and frontal plane goniometric knee alignment were obtained from the OAI AllClinicalxx data sets. Coronal plane alignment was obtained from goniometric measurements in the OAI database at baseline and from each clinical visit [OAI variable: Vxx (L or R) KALNMT]. In brief, this was done manually with the goniometer axis of rotation positioned over the centre of the knee joint line, one arm along the axis of the femur and the other arm along the length of the tibia, directed towards the centre of the ankle. In this analysis, varus was considered clinically significant at values greater than 2° and valgus at values less than −2°. Knees were considered neutral when angulation was −2° to 2°. 18
Injury to the target knee prior to baseline was documented from the OAI question: Have you ever injured your (right/left) knees so badly that it was difficult for you to walk for at least 2 days? The answer (yes/no) and the age at injury were recorded allowing for the calculation of the duration between the injury (age at index date minus age at injury) and the index date. The occurrence of a first knee injury, at any time prior to the index date, was categorized as follows: no injury, first injury in 10, 10–20, 20–30, 30–40 or more than 40 years preceding the index date.
MR images were obtained from the OAI database and were acquired with a 3.0 T apparatus (MAGNETOM Trio, Siemens) at the four OAI clinical centres using a double-echo steady-state imaging protocol. The KL grades and mJSW measurements were derived from the OAI central reading https://nda.nih.gov/oai/. Baseline and follow-up KL grades (0–4) (files: kXR_SQ_BUxx) were centrally scored. Baseline and follow-up medial JSW (files: kxr_qjsw_duryeaxx) were blindly measured from bilateral, weight-bearing, fixed-flexion posterior–anterior knee.25,26
Fully automated and validated quantitative MRI technologies were used to assess the cartilage volume and the BMLs, and a validated scoring method was used for the meniscal extrusion, as previously described.27–29
Cartilage volume was measured, as previously described, 28 and analysed for the global tibiofemoral (femur and plateau) knee and their respective medial and lateral compartments. The change in cartilage volume was obtained by subtracting the follow-up volume from the initial (baseline) volume divided by the initial (baseline) volume and reported as a percentage (%) of loss.
BMLs, expressed as a percentage (%) of the lesion in the bone volume region, as previously described, 29 were assessed in the same MRI sequences used for the cartilage, quantified in each of the regions: tibiofemoral, medial and lateral compartments of the knee, but due to insufficient statistical power for the compartments, data are presented only for the global knee. Meniscal extrusions were scored as absence (0) or presence (1) of partial/complete meniscal extrusion at any segments of the medial or lateral compartments as reported. 27
Study size
As previously reported, 393 participants had TKA during the follow-up period. 11 From this number, 198 participants were excluded as they had missing information for the measurement of characteristic changes over time. A total of 195 cases were matched to 468 controls.
Statistical analyses
Descriptive analyses at the index date were conducted for case and control participants. Proportions were calculated for categorical variables and median and interquartile range (IQR) for continuous variables. We used a case–control design that allowed the comparison of the changes in characteristics over time. In this design, as there was no time measurement to the event, the association between the occurrence of TKA and change in sociodemographic, clinical and imaging data was measured using conditional logistic regression. Crude odds ratios (cOR) and 95% confidence interval (CI) were calculated. cOR for BMI were reported per increase in 1 kg/m2 over time, WOMAC total and subscales per increase in one unit of a score, while KOOS subscales were reported as a decrease in one unit of each subscore over time. The cOR for varus and valgus were reported per increase in one degree (unit) over time, mJSW loss per decrease in 1 mm (unit), BMLs per increase in 1% over time and meniscal extrusion as the occurrence of a new extrusion over time. Analyses were performed using all case and control participants followed by discriminating women and men. A two-tailed p value < 0.050 was considered significant. No corrections for multiple testing were made. All statistical analyses were performed using SAS software, V.9.4 (SAS Institute, Cary, NC, USA).
Results
Participant characteristics at the index date
Data show that the sociodemographic characteristics of participants at the index date were balanced between cases and controls (Table 1). Of note, the median time from cohort entry to having a TKA was 4.4 years. The clinical characteristics were also balanced, but cases presented slightly higher WOMAC scores (except stiffness), lower KOOS scores and smaller mJSW than controls (Table 2). In regard to gender (data not shown), for both cases and controls, there was a greater incidence of women than men with valgus alignment (cases, 40.2% versus 25.6%, respectively; controls, 41.0% versus 16.2%) and a greater incidence of men than women with varus alignment (cases, 47.4% versus 19.7%; controls, 45.6% versus 17.0%).
Participant sociodemographic characteristics at index date.*

IQR, interquartile range; OAI, Osteoarthritis Initiative; n, number of participants; TKA, total knee arthroplasty.
Index date, the date on which the total knee arthroplasty (TKA) occurred.
Clinical characteristics at index date.*

BMI, body mass index; BML, bone marrow lesion; IQR, interquartile range; mJSW, medial joint space width; KOOS, knee injury and osteoarthritis outcome score; n, number of participants; QoL, quality of life; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Index date, the date on which the TKA occurred.
WOMAC 22 and KOOS 23 questionnaires were self-administered: higher WOMAC scores and lower KOOS scores indicate more symptoms and greater functional impairment.
Meniscal extrusion: presence of partial or complete extrusion in any of the three segments of the medial and lateral compartments of the meniscus.
Association between changes in sociodemographic, clinical and imaging characteristics and the occurrence of TKA
Significant associations with the occurrence of TKA were found with the global worsening of WOMAC scores, and a decrease in KOOS scores (Table 3). For both WOMAC and KOOS, the level of association was about similar for all scores regardless of gender, except for WOMAC stiffness in men.
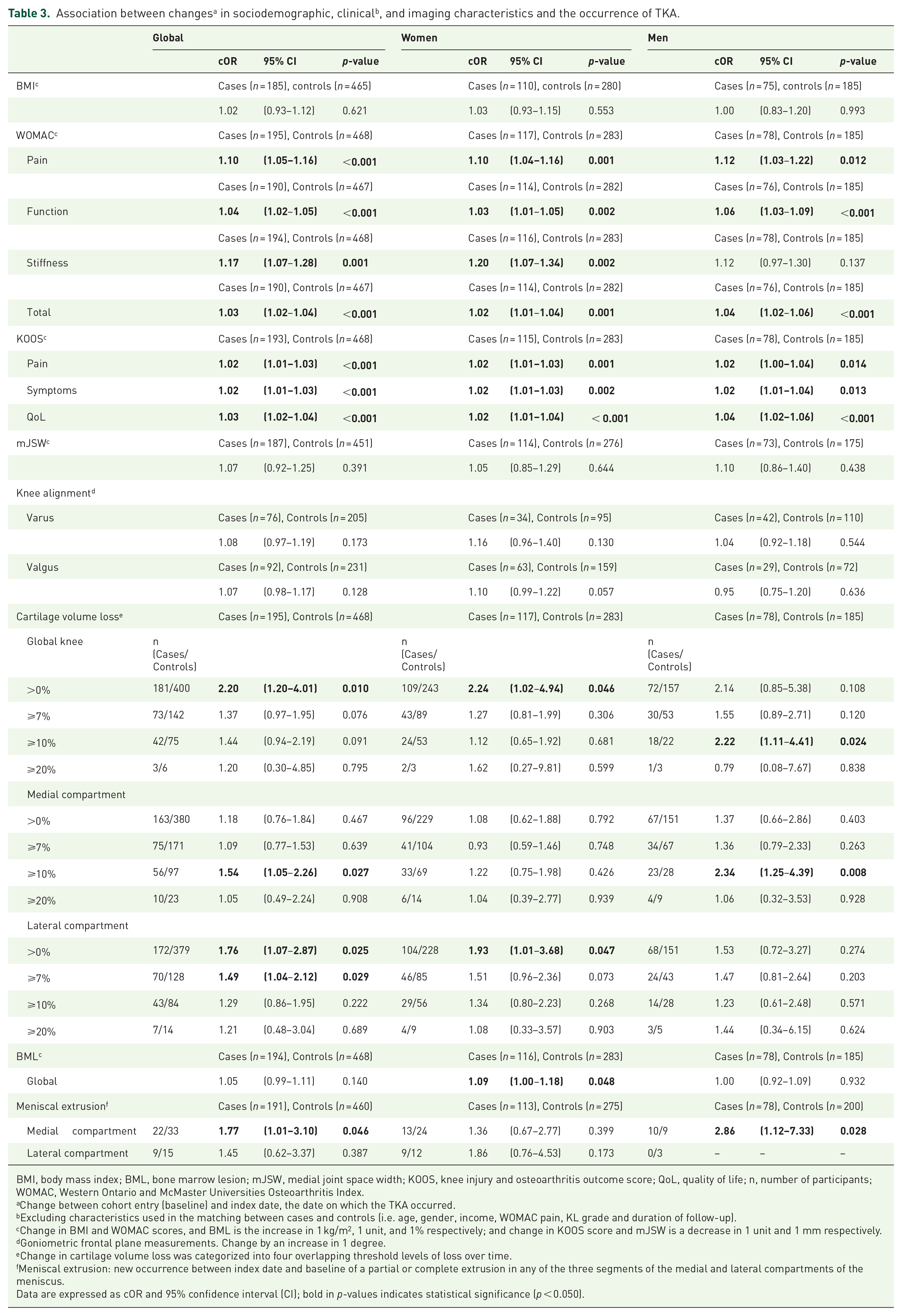
BMI, body mass index; BML, bone marrow lesion; mJSW, medial joint space width; KOOS, knee injury and osteoarthritis outcome score; QoL, quality of life; n, number of participants; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Change between cohort entry (baseline) and index date, the date on which the TKA occurred.
Excluding characteristics used in the matching between cases and controls (i.e. age, gender, income, WOMAC pain, KL grade and duration of follow-up).
Change in BMI and WOMAC scores, and BML is the increase in 1 kg/m2, 1 unit, and 1% respectively; and change in KOOS score and mJSW is a decrease in 1 unit and 1 mm respectively.
Goniometric frontal plane measurements. Change by an increase in 1 degree.
Change in cartilage volume loss was categorized into four overlapping threshold levels of loss over time.
Meniscal extrusion: new occurrence between index date and baseline of a partial or complete extrusion in any of the three segments of the medial and lateral compartments of the meniscus.
Data are expressed as cOR and 95% confidence interval (CI); bold in p-values indicates statistical significance (p < 0.050).
For the knee alignment in women, the increase in valgus angulation showed a numerical trend towards an association with TKA (p = 0.057).
Loss of cartilage volume >0% in the global knee was significantly associated with TKA for both men and women together (global). According to gender, this association was found in women having a cartilage loss >0% and in men ⩾10%. In the medial compartment, there was an overall association for a cartilage loss ⩾10%, (cOR 1.54, p = 0.027), with a stronger association in men (cOR 2.34, p = 0.008). In the lateral compartment, there was also a global association with cartilage loss >0% and ⩾7%, more particularly in women having a loss >0%.
The increase in BML size demonstrated an association with TKA in women. The occurrence of medial meniscal extrusion was also found to be significantly associated with TKA globally, while most prominent in men.
Association between change in OA therapies over time and the occurrence of TKA
A significant association with TKA was found in men who started using acetaminophen over time (Table 4). Similarly, the initiation of treatment with narcotics for the global population was associated with TKA, more particularly in women, but with a numerical trend towards an association in men (p = 0.057). A strong association with treatment initiation was also observed with IASI in all groups (global, women and men, all p < 0.001).
Association between change a in OA therapies over time and the occurrence of TKA.

CI, confidence interval; COX-2 inhibitors, cyclooxygenase-2 inhibitors; GLU/CS, glucosamine/chondroitin sulphate; IASI, intra-articular steroid injections; NSAIDs, non-steroidal anti-inflammatory drugs; n, number of participants.
Change between cohort entry (baseline) and index date, the date on which the TKA occurred.
Reference group for statistical purposes.
Data are expressed as cOR and 95% confidence interval (CI); bold in p-values indicates statistical significance (p < 0.050).
Change in mJSW and cartilage volume loss in the years prior to the index date in relation to the use of IASI
The yearly change in mJSW and cartilage volume loss between no IASI and with IASI in both cases and controls were relatively similar although highly variable at any time up to 5 years before the index date (Table 5, Figures S1 and S2). Of note, the number of cases and controls was insufficient to go back more than 5 years prior to the index date.
Yearly change in medial joint space width and cartilage loss with the use of IASI.
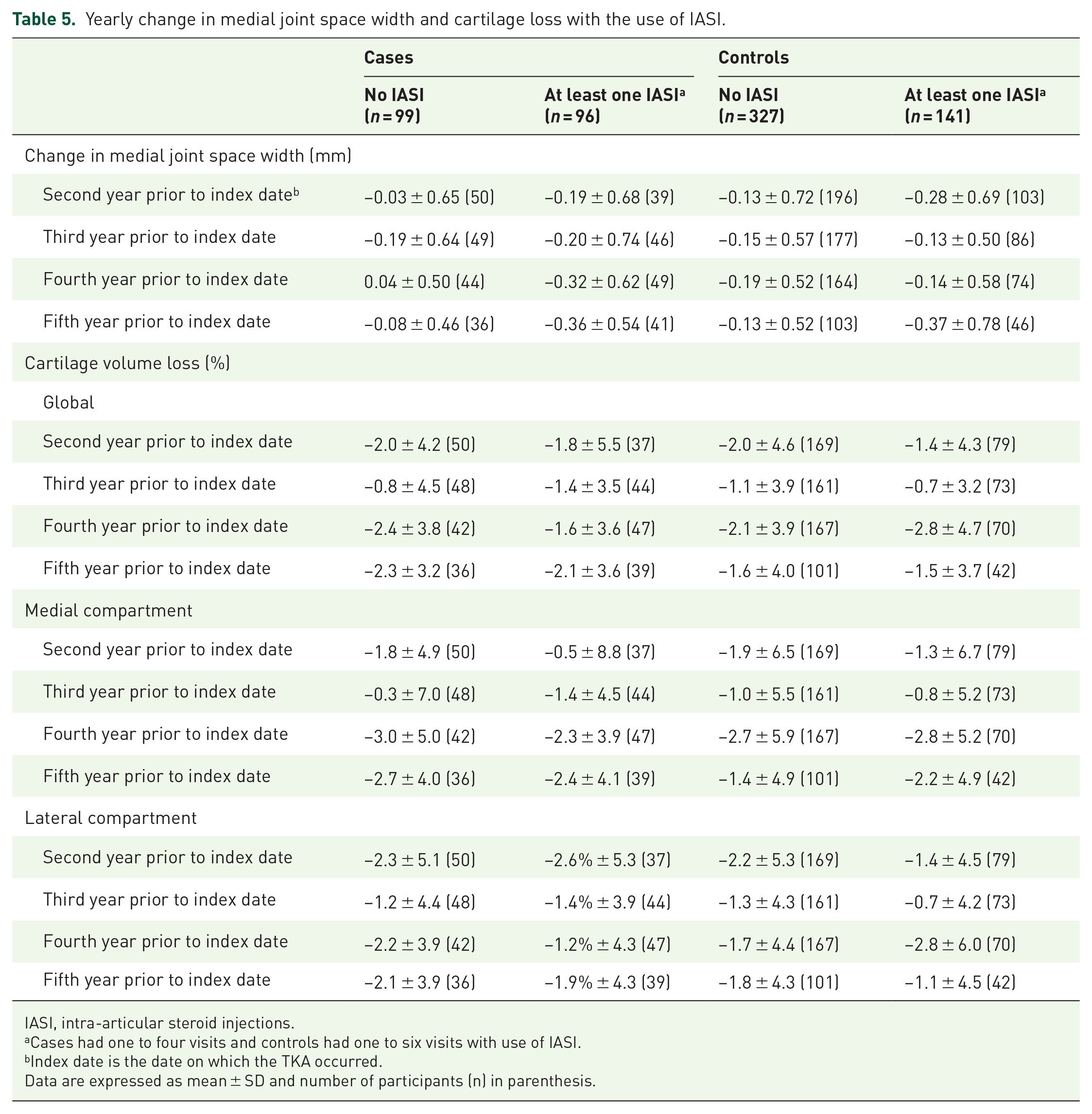
IASI, intra-articular steroid injections.
Cases had one to four visits and controls had one to six visits with use of IASI.
Index date is the date on which the TKA occurred.
Data are expressed as mean ± SD and number of participants (n) in parenthesis.
For the IASI, 89.6% of cases and 87.6% of controls received one or two injections. The remaining participants received three to four injections for the cases and three to six for the controls.
Association between time of first injury, combination of major risk factors and the occurrence of TKA
Data first showed (Table 6) that there was a gradual increase in the likelihood of TKA over time after the first injury, with the greatest and significant cOR at 30–40 years for women.
Association between time from first injury a and the occurrence of TKA.

CI, confidence interval; n, number of participants.
Interval of time between the date of the first injury reported by the participants prior to entry (baseline) or at one of the subsequent clinical visits to the index date, the date on which the TKA occurred.
Reference group for statistical purposes.
Data are expressed as cOR and 95% CI; bold in p-values indicates statistical significance (p < 0.050).
The combination of changes (increases) in WOMAC pain score with simultaneous cartilage volume loss >0% in the global knee was the major factors responsible for the occurrence of TKA (Table 7). Hence, the combination of the changes of the two abovementioned factors, in addition to the first injury sustained 30–40 years prior to entry, was also linked to the greatest cOR for TKA with a numerical trend towards significant difference (p = 0.067).
Association of changes in major risk factors a and the occurrence of TKA.

CI, confidence interval; n, numbers of participants; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Major risk factor prior to index date, the date on which the TKA occurred.
Interval of time between the date of the first injury reported by the participants prior to entry (baseline) to the index date.
Data are expressed as cOR and 95% CI; bold in p-values indicates statistical significance (p < 0.050).
Discussion
This longitudinal study provides new information on the gender differences in risk factors associated with the occurrence of TKA. Worsening of valgus alignment, cartilage volume loss in the lateral compartment, BMLs and older injuries are the important risk factors in women, while medial compartment cartilage loss and meniscal extrusion are in men. Previous use of pain medication and IASI, although associated with TKA, was found not causal. The combination of the worsening of pain and cartilage volume loss, and a history of old trauma provided the greatest cOR for TKA.
Over the years, there have been numerous studies looking for risk factors associated with the occurrence of TKA.4–14 Most of them have used cross-sectional analyses and very few studies employed, such as the present one, a longitudinal approach. The present case–control study investigates the association of factors with the occurrence of TKA in OA. This was done by assessing simultaneously demographics, and baseline and changes of disease symptoms or structural characteristics over time. A significant advantage of such a design is that it allows the patient profiles who had a TKA to be evaluated at the very date of TKA surgery. We believe this is more clinically relevant compared to performing a cohort study design in which the risk factors are assessed at entry (baseline) into the cohort. 30 In this study, with case and control groups being well balanced with regard to sociodemographic, clinical and imaging characteristics, and the majority of participants having moderate-to-severe disease as shown by X-rays (mJSW and KL grades) at the time of TKA (index date), it enables us to propose strong and valid new information on the risk factors and those gender-based associated with TKA in OA patients.
Here, data support key association of TKA with the worsening of knee symptoms, found for both WOMAC and KOOS scores. These findings highlight not only the importance of the worsening in disease symptoms and loss of function but also of the QoL, which in turn may influence the patient’s decision to seek a TKA.6,12 This is also supported by other studies,9,31,32 indicating that these factors are among the strongest predictors of TKA in OA. Of particular interest, in our study, was the association in the increase in WOMAC stiffness score with the occurrence of TKA in women. Although the exact reason for this difference remains to be determined, one could speculate on the possibility of a relation to the greater incidence of synovitis in women with knee OA, which is often associated with more severe symptoms and disease progression, known as risk factors linked to TKA.31,33,34
This study also provides new information on the association, in women, of TKA with ancient trauma. This association may be linked to ligament damage, encountered at the time of injury, 35 which may have led to a greater risk of valgus alignment. As malalignment is a well-known factor associated with cartilage loss, it could provide a possible explanation for the higher incidence of TKA.7,16,17,36,37
The extent and location (knee compartment) of cartilage loss, meniscal extrusions and BMLs were also found associated with TKA, and findings differed greatly between genders. The data showing that BMLs are linked to the prediction of TKA was not surprising as their relationship to the progression of knee OA, 38 cartilage loss 39 and the severity of knee OA symptoms40–42 have all been demonstrated. However, the finding of an association in the increase in BML size with TKA only in women is a new finding that needs further exploration. In established knee OA, data from cross-sectional studies have shown that knee malalignment can predict the progression of the tibiofemoral disease and the extent of cartilage loss, more particularly in overweight and obese individuals.16,17,35,43 The data of our longitudinal study showing that the worsening of the valgus alignment, an alteration more common in women than men, 44 is associated (numerical trend) with TKA in women, is also a most interesting new finding of our study. It contrasts with a recent study also exploring the OAI cohort, which reported no association between joint laxity and risk of TKA. 45 The study design and the fact that the imaging data were restricted to X-rays may have been important limiting factors of this report. The observation of the association of TKA with the progression of valgus malalignment and cartilage loss in the global knee and lateral compartment in women extends the existing knowledge from previous studies36,37 and could be an explanation for the association between BML and TKA being found only in women.
Our data also showed an association between the occurrence of a new medial meniscal extrusion and TKA in men. Such a finding, to our knowledge, is novel and extends over data from previous reports6,46 and, in addition, to providing further support to the important dynamic role played by this risk factor. Hence, it showed that not only existing meniscal extrusions but also the appearance of new ones are important risk factors for TKA. Moreover, in knee OA patients, meniscal extrusion has been found to be associated with neuropathic pain and severe OA symptoms, 34 which may have indirectly contributed to the occurrence of TKA. Finally, the association in men between TKA and cartilage volume loss (loss ⩾ 10%) in the medial compartment could be related, at least in part, to the occurrence of meniscal extrusion and the higher incidence of varus alignment, as both could lead to a greater loss of cartilage in that compartment.27,35,46
The lack of association between mJSW loss and KL grade worsening with the occurrence of TKA contrasts to other reports.5–7,12,31,32,47,48 A possible explanation could be that the mean observation time in the other reports was much longer6,31,47 than the one in our study (4.4 years). In addition, the assessment of mJSW loss in this study was done only on the medial compartment as a greater number of the participants (cases) were women in whom valgus malalignment is more commonly found, which could have favoured cartilage loss preferentially in the lateral compartment. Data on JSW loss in that compartment would have been interesting information in the context of this study.35,36,43,44
Regarding the use of OA medication, the start of the narcotics and IASI found in the participants in this study was expected. Indeed, data concur with the present OA participants having a strong association with the disease symptoms, in addition to being in line with the latest recommendations of associations for OA treatment49,50 and common practice by physicians. Of note, the number of visits reporting the use of IASI was relatively small but reflects the real-life scenario in knee OA management. Although the start of these medications was associated with TKA, this was not found for the other OA treatments, such as NSAIDs, COX-2 inhibitors and glucosamine/chondroitin sulphate. While this finding concurs with a recent publication, 11 there is an absence of consensus on the effects of such treatments on knee OA progression.6,11,51–56 Finally, data showing that IASI in the period prior to TKA did not demonstrate at any time (at least 5 years prior) a detrimental effect on cartilage loss, as assessed by change in both mJSW and cartilage volume loss, is in strong support that this treatment was not causal of knee surgery.
This study provides several interesting new findings that have potential clinical implications for the prevention and treatment of patients with knee OA. There is an obvious difference in risk factors associated with TKA between genders. The role played by the progression of valgus alignment in the need for TKA in women is important information and supports the implementation of preventive measures to reduce its progression. The reduction of BMI in obese patients is among one of the preventive measures and is supported by several previous studies.57–60 Similarly, a reduction in joint trauma may also help to decrease the risk of soft tissue damage leading to joint malalignment. 19 In men, the appearance of new meniscal extrusions seems to be the primary risk factor for TKA. The role of trauma, including occupational trauma for this gender, cannot be excluded. Therefore, safety measures at work and home, to reduce the likelihood of trauma, could be most helpful to counteract the progression of varus alignment and appearance of meniscal extrusions. These latter measures can be broad, starting from non-invasive medical management to surgical intervention.19,61,62 Our study also provides reassurance about the safety of IASI, in a real-life scenario, for the symptomatic treatment of knee OA. In the future, when disease-modifying treatments for OA (DMOADs) will become available as treatment, the identification of patients with a high risk of disease development/progression using the abovementioned risk factors will be very helpful in selecting those that could benefit the most from such treatment.
This study is not without potential limitations. First, our main outcome specifically focused on OA knees in need of surgery, which has known issues concerning procedure indication and access, such as socioeconomics, comorbidities and patient preferences to name a few. In addition, we did not investigate other associations, for example, the chronic use of therapeutic interventions and subclinical structural damage. Second, the data on drug usage and IASI were obtained by a self-administered questionnaire and not by precise information as in clinical trials, which could have underestimated the true prolonged and cumulative usage of these interventions. Third, information on OA disease duration is not available at baseline for the OAI cohort. It was, therefore, impossible to predict time to TKA occurrence from knee OA symptom onset or to identify confounding factors that may influence the speed of TKA occurrence. This is one of the reasons we chose to use a case–control design starting from the TKA and go ‘backwards’ to find predictors instead of the classic longitudinal, prospective analysis. Fourth, another potential limitation is the assessment of the time of injury as probed per the subject’s questionnaire. The longer the duration from time to injury to study inception would certainly impact its association with symptoms. However, we felt that no skewness was to be expected, which in turn could influence the occurrence of symptomatic knee OA as all patients that had a surgical procedure associated with such trauma (if any) were excluded from the study. We must, however, acknowledge that the data of such a relationship between trauma history and TKA occurrence do not have a strong linear association. It may well be that a recall bias is in play since remembering the precise time of a trauma that happened beyond 10 years may be indeed difficult. Further studies refining this relationship are needed. As for the knee side being traumatized, which knee was affected (study knee or not) was specifically addressed on the questionnaire. Fifth, the relatively small sample size of TKA occurrences (n = 195) over the years despite the overall large patient numbers in the OAI cohort (4674 subjects) decreased the study’s statistical power. Such a number is, however, in line with previous studies using the same cohort,8,9,11,46 but does not prevent being cautious when interpreting the data in the study. The number of TKA also prevented us from performing extensive multivariate analyses with a model that would include confounding variables to evaluate if the associations found in our study would still hold. However, the matching of cases and controls was excellent and addressed this issue, but the impact of unknown confounding variables, which may have skewed our results, is unpredictable. Sixth, as no statistical corrections for multiple testing were made, type 1 errors in data interpretation were not excluded. Another limitation relates to the population-specific characteristics of the OAI cohort, which includes the fact that it is an American cohort and has, for example, higher BMI 2 or better access to TKA 63 contrasting to other regions of the world. Cross-validation studies should be done with separate data sets from other countries to support the generalizability of our results. Finally, it is important to note that, per the study design, the matching of cases (TKA) and controls were at the time of the surgery occurrence. This was a retrospective analysis of data and, as such, survival curves from study inception to TKA occurrence entry or finding predictors from baseline (study entry) information were not among our research questions.
In conclusion, this study provides new information on several risk factors associated with knee OA development/progression. The risk profile for TKA of changes over time in structural lesions and gender is different for medial and lateral tibiofemoral compartments. These results can find clinical applications in helping healthcare providers to identify patients at high risk of severe knee OA and implement risk prevention/reduction strategies to improve the QoL and, hopefully, the disease outcome of those patients.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X221091359 – Supplemental material for Risk factors associated with the occurrence of total knee arthroplasty in patients with knee osteoarthritis: a nested case–control study
Supplemental material, sj-docx-1-tab-10.1177_1759720X221091359 for Risk factors associated with the occurrence of total knee arthroplasty in patients with knee osteoarthritis: a nested case–control study by Jean-Pierre Pelletier, Marc Dorais, Patrice Paiement, Jean-Pierre Raynauld and Johanne Martel-Pelletier in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X221091359 – Supplemental material for Risk factors associated with the occurrence of total knee arthroplasty in patients with knee osteoarthritis: a nested case–control study
Supplemental material, sj-docx-2-tab-10.1177_1759720X221091359 for Risk factors associated with the occurrence of total knee arthroplasty in patients with knee osteoarthritis: a nested case–control study by Jean-Pierre Pelletier, Marc Dorais, Patrice Paiement, Jean-Pierre Raynauld and Johanne Martel-Pelletier in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Acknowledgements
The authors would like to thank the OAI participants and Coordinating Center. This work was prepared using an OAI public data set and does not necessarily reflect the opinions or views of the OAI investigators, the NIH, or the private funding partners
The authors also wish to thank Santa Fiori for her assistance with the preparation of the article
Author contribution(s)
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J-P.P. and J.M-P. are shareholders in ArthroLab Inc. J-P.R. and M.D. are consultants for ArthroLab Inc. P.P. is an employee of ArthroLab Inc. None of the authors are part of the Osteoarthritis Initiative (OAI) investigative team.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded in part by grants from Osteoarthritis Research Unit of the University of Montreal Hospital Research Centre and the Chair in Osteoarthritis of the University of Montreal.
Ethics
Data analysed in this study are from the Osteoarthritis Initiative (OAI), and ethics approval was obtained by each OAI clinical site (University of Maryland Baltimore – Institutional Review Board, Ohio State University Biomedical Sciences Institutional Review Board, University of Pittsburgh Institutional Review Board and Memorial Hospital of Rhode Island Institutional Review Board) and the OAI coordinating centre [Committee on Human Research at University of California, San Francisco, CA, USA (#10-20053)]. All patients provided written informed consent for participation in the OAI.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.