
Abstract
Objective:
We aimed to compare the efficacies of rehabilitation with the hybrid assistive limb and conventional rehabilitation after total knee arthroplasty.
Materials and methods:
A total of 37 consecutive patients who underwent primary total knee arthroplasty for knee osteoarthritis were enrolled. Seven patients withdrew from the study after randomization, and 30 patients (hybrid assistive limb group: n = 16; conventional group: n = 14) completed the randomized controlled trial. Patients in the hybrid assistive limb group underwent ten 20-min rehabilitation sessions with the hybrid assistive limb as well as 20-min conventional sessions over the course of 2 weeks, whereas patients in the conventional group received ten 40-min conventional sessions during the same period. The primary outcome measure was walking speed, whereas the secondary outcome measures included quadriceps strength and knee pain assessed using a numerical rating scale. The outcome measures were evaluated prior to surgery and on postoperative weeks 1, 2, and 3.
Results:
In the early postoperative period, rehabilitation after total knee arthroplasty with the hybrid assistive limb resulted in a significantly greater improvement in walking speed (weeks 1 and 2: p = 0.045), quadriceps strength (weeks 1 and 2; weeks 1 and 3: p < 0.0001), and numerical rating scale scores (week 1: p = 0.03) than conventional rehabilitation.
Conclusion:
Rehabilitation with the hybrid assistive limb after total knee arthroplasty led to greater improvements in walking speed, quadriceps strength, and pain scores than conventional rehabilitation.
Keywords
Introduction
Total knee arthroplasty (TKA) is the most widely used surgical treatment for end-stage osteoarthritis (OA) of the knee and is reportedly effective in alleviating pain, enabling functional recovery, and improving the quality of life (QOL).1,2 It is also considered to be a safe surgical procedure. 3
In Japan, the mean duration of hospitalization for TKA is 35.1 ± 15.9 days, whereas that for initial TKA only is 35.0 days. 4 It is important to minimize the hospitalization period as this reduces associated healthcare costs. Since the time of discharge usually depends on walking ability, patients who start walking sooner can be discharged more quickly.
The hybrid assistive limb (HAL) is an exoskeletal robot suit developed in 1992 to provide the wearer with physical support during daily activities and heavy labor. 5 The HAL for the lower limbs was developed as a gait assistance system for individuals with difficulty in standing up, sitting down, and climbing stairs. 6 The HAL has two modes: a voluntary control mode and an automatic control mode. In the voluntary control mode, the suit provides support for physical activities based on weak bioelectric signals generated when the wearer makes a voluntary movement. 7 These bioelectric potentials are detected by electrodes attached to the surface of the skin. In most cases, the electrodes are attached to the quadriceps femoris and gluteus maximus muscles in the area around the hip joint and the vastus lateralis and biceps femoris in the area around the knee. The assistive force generated by the HAL power unit is calculated based on the bioelectric potentials generated by the muscles. This approach is used to support and control movements. 8 In the voluntary control mode, the HAL provides functional support for multiple joints of both legs simultaneously, which makes it suitable for use by individuals with leg disabilities as well as healthy individuals. 9 Accordingly, HAL training, which utilizes the wearer’s own muscle activity, could enhance the feedback for inducing appropriate movements better than standard robotic training. 10
One study (a randomized controlled trial) assessed the use of the HAL in rehabilitation for improving locomotion in the recovery phase after cerebral stroke, 10 and several reports have documented its use in rehabilitation of patients with cerebral stroke and spinal cord injury to promote gait improvements. 11 However, to our knowledge, there have been few reports on the use of HAL in rehabilitation after TKA only, both in terms of pilot studies 12 and case reports. 13
We hypothesized that, in addition to the effects demonstrated in previous studies, the HAL may also be useful for facilitating the recovery of leg function and gait function in patients after TKA. To test this hypothesis, we decided to assess the rate of change in walking speed rather than walking speed alone since the latter varies widely depending on the baseline values. In the present randomized controlled trial, we aimed to verify whether the HAL can be used in rehabilitation after TKA to promote functional recovery.
Materials and methods
Participants
All patients underwent primary TKA for knee OA at JR Tokyo General Hospital between September 2014 and August 2015. Patients were enrolled according to the following inclusion criteria: scheduled to undergo primary TKA due to OA and age of 65–80 years. The exclusion criteria were as follows: inability to receive concurrent physical therapy; presence of rheumatoid arthritis, stroke, malignant tumor, Parkinson’s disease, dementia, active infection, pulmonary embolism, or deep vein thrombosis; body dimensions inappropriate for the use of the HAL; presence of skin disease precluding electrode placement; and presence of an implanted pacemaker.
Randomization
Patients meeting the inclusion criteria were randomly assigned in a 1:1 ratio to the HAL group or to the conventional training group. Randomization was performed according to age and sex. To ensure that all doctors, institutional investigators, assessors, and patients involved in the trial remained blinded to treatment assignment, the randomization was performed by an independent organization, the 22nd Century Medical & Research Center of the University of Tokyo.
Study protocol
We used a computer-generated sequence, with odd-numbered patients participating in rehabilitation using the HAL and even-numbered patients participating in conventional training. Patients in the HAL group performed gait rehabilitation with the HAL five times a week for a total of 10 HAL training sessions (over the course of 2 weeks). Patients in the conventional group performed conventional gait rehabilitation five times a week for a total of 10 conventional training sessions (over the course of 2 weeks). Patient demographics and baseline values of outcome measures were assessed prior to randomization into treatment groups. The study was approved by the Ethics Committee of the JR Tokyo General Hospital. All patients provided written informed consent prior to participation.
Rehabilitation using the HAL
The HAL for the lower limbs was used in all the patients (Figure 1). One 40-min session was completed once a day. While wearing the HAL, patients performed quadriceps muscle strength exercises in a sitting position and practiced standing up from a seated position for 20 min. They also undertook a single 20-min rehabilitation session consisting of range of motion exercises and walking. HAL instructors were skilled and experienced physical therapists licensed to use the HAL. The cybernic voluntary control mode was used.

Training in standing up from a seated position with the HAL.
Conventional rehabilitation
Conventional training was performed for 40 min once a day. Patients performed the same 20-min program of quadriceps muscle strength exercises and standing up from a seated position as in the HAL group but without wearing the HAL. They also completed a single 20-min rehabilitation session of range of motion exercises and walking. Conventional training instructors were skilled and experienced physical therapists.
Assessment
All measurements were conducted by physical therapists trained to perform standardized assessment procedures. The outcome measures were evaluated prior to surgery and on postoperative weeks 1, 2, and 3. The primary outcome measure was walking speed. For the assessment of walking speed, patients walked 10 m on the ground at a comfortable speed. The secondary outcome measures included quadriceps strength and knee pain assessed using a numerical rating scale (NRS). Isometric contraction quadriceps strength of knee extension was measured used a hand-held dynamometer (µtas F-1). A pressure sensor was fixed to the belt worn around the ankle to record the maximum power. The maximum value from three trials was used in the analysis.
Statistical analysis
To ensure balanced randomization, we tested the differences between the HAL and conventional groups at baseline using the Fisher exact test for sex and unpaired t-tests for age, height, weight, body mass index (BMI), walking speed, and quadriceps strength. The primary outcome was the difference in the change of walking speed between the two groups between week 1 and week 2 or 3, which was assessed by a paired t-test. The change ratio was calculated using the following formula: ([follow-up] − [week 1])/[week 1]) × 100. All statistical tests were performed at a significance level of 0.05 (two-sided) without adjusting for multiple testing.
The sample size was calculated in a preliminary study to detect a difference between the groups in change ratio of walking speed of 10%. A sample size of 15 patients per group (30 patients in total) resulted in a power of 80%.
Data analyses were performed using SAS, version 9.1.3 (SAS Institute Inc., Cary, NC).
Results
Figure 2 shows the flow chart of patient enrollment and participation. A total of 37 patients underwent primary TKA and were assessed for eligibility. Among the 16 subjects allocated to the HAL group, 1 withdrew consent, 1 could not continue rehabilitation because of delirium, and 1 could not use the HAL because of obesity and contralateral lower-extremity deformity. Among the 14 subjects allocated to the conventional training group, post-intervention outcomes could not be assessed for 1 subject. Thus, a total of 26 subjects completed the study. No differences were observed in the demographics and baseline clinical data between the two groups (Table 1).

Flow chart of patient enrollment and participation.
Demographics and preoperative descriptive parameters in the HAL and conventional groups.
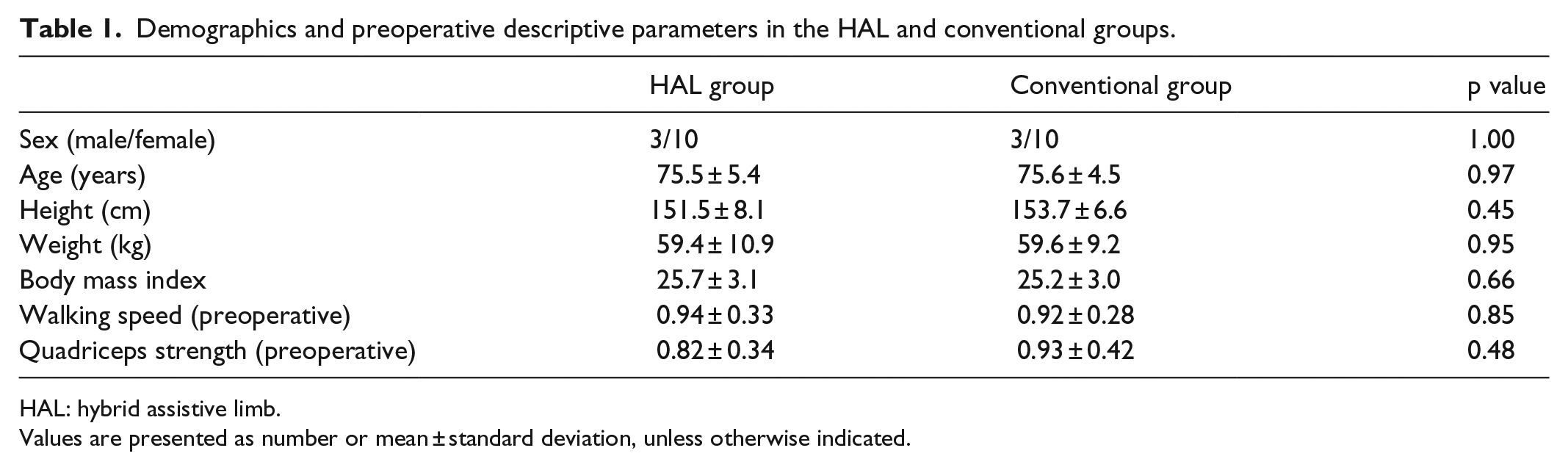
HAL: hybrid assistive limb.
Values are presented as number or mean ± standard deviation, unless otherwise indicated.
A comparison of the rates of change in walking speed between week 1 and week 2 after TKA revealed significantly better values for patients who underwent rehabilitation with the HAL. In contrast, a comparison of the rates of change in walking speed between week 1 and week 3 after TKA did not show a significant difference (Table 2).
Rates of change in walking speed and quadriceps strength in the two groups.

HAL: hybrid assistive limb.
Values are presented as number or mean ± standard deviation, unless otherwise indicated.
A comparison of the rates of change in quadriceps strength between postoperative weeks 1 and 2, as well as postoperative week 1 and 3, showed significant differences between the two groups (Table 2). Moreover, a significantly greater number of patients who did not use the HAL had a high pain score (≥6) at 1 week postoperatively. However, there was no difference in the NRS scores between the two groups at 2 weeks or 3 weeks postoperatively, and the scores improved over time in both groups (Table 3).
Numbers of participants with high NRS scores (≥6).

HAL: hybrid assistive limb; NRS: numerical rating scale.
Discussion
To our knowledge, this is the first randomized controlled trial of the use of the HAL for rehabilitation after TKA. We found that, compared to conventional rehabilitation, the use of the HAL during early rehabilitation after TKA efficiently improved locomotion and quadriceps femoris strength, while reducing pain.
In this study, walking speed was used as a measure of postoperative recovery. Walking speed has a low failure rate (<5%) in the elderly 14 and is a highly reliable indicator, with an intra-session correlation coefficient of 0.90–0.98 and an inter-session correlation coefficient of 0.78–0.94 among patients with knee OA. 15 Changes in comfortable walking speed reflect the ability to respond to conditions that occur during environmental changes and when crossing intersections and avoiding obstacles. 16 Moreover, walking speed has been found to be correlated with other indicators such as the Berg Balance Scale score 17 and timed up and go (TUG) test results, 18 both of which reflect the balance function. In a study by Cress et al. 19 conducted in 200 elderly residents of a nursing home, walking speed was an independent factor reflecting physical function.
The change in walking speed after TKA is also considered an indicator of the effectiveness of rehabilitation. 20 A study of post-discharge walking speed in 57 patients with knee OA who underwent initial TKA found that the mean post-discharge 10-m walking speed was 0.7 ± 0.2 m/s. 21 In general, the walking speed 21 and TUG test results 22 decrease temporarily after discharge following TKA, followed by recovery over several months and improvement beyond the preoperative levels.
In this study, the rate of change in walking speed between weeks 1 and 2 after TKA was significantly better in patients who underwent rehabilitation with the HAL. However, there was no significant difference between the two groups in the rate of change in walking speed between postoperative weeks 1 and 3. These results suggest that the use of the HAL in rehabilitation after TKA is particularly valuable during the early part of the postoperative recovery phase, with the difference between HAL and conventional rehabilitation diminishing over time.
It was found that 44.4% of patients experience persistent severe pain 1 month after TKA. 23 Pain affects functional recovery after TKA as it restricts walking and reduces walking speed. We used the NRS as a pain measure. A significantly greater number of patients who did not use the HAL had a high pain NRS score (≥6) at 1 week postoperatively. However, there was no difference in the NRS scores between the two groups at 2 weeks and 3 weeks postoperatively, and the scores exhibited improvement over time in both groups. This suggests that the use of the HAL during the early postoperative period reduced pain during rehabilitation. This might have a beneficial effect on the recovery of walking speed.
The mechanism through which the use of the HAL improves gait function after TKA remains unclear. Quadriceps arthrogenic muscle inhibition (QAMI) may be one reason for the effectiveness of rehabilitation after TKA. QAMI is the phenomenon of inhibition of the quadriceps femoris muscle after surgery. 24 It is believed to result from pain or swelling of the knee or damage to pressure receptors 24 and may also occur because of swelling of the knee alone. 25 At present, the suggested mechanisms for QAMI include possible inhibition of α motor neurons via the spinal reflex 26 and involvement of pathways engaging upper motor neurons. 24
Concentrated repetition of specific tasks is also known to induce neural plasticity and promote functional recovery from paralysis following stroke or spinal cord damage.27–31 In this study, the rates of change in quadriceps strength between postoperative weeks 1 and 2 and between postoperative weeks 1 and 3 were significantly different between the two groups. These results suggest that the knee could be affected by the QAMI phenomenon after TKA, and the effectiveness of repeating specific tasks in combination with the feedback provided by the use of the HAL might promote neural plasticity, thus improving quadriceps function and enabling the recovery of gait function during the early recovery phase.
Limitations
This study has certain limitations. First, fitting the HAL requires considerable time and effort, and adjustments are needed in the sites of attachment of the electrodes and settings such as the assistance level. Therefore, the level of familiarity of the physiotherapists with the HAL may have affected the results.
The second limitation concerns the device itself. The HAL used in this study was designed as an assistive device for both legs. To adapt the system for functional recovery after TKA, a model wore the HAL on only one leg, which reduced the weight of the device and allowed freedom of movement of the unaffected leg, thus increasing its efficiency.
The third limitation originates from the unique medical insurance system, in which medical procedures from surgery to discharge are fully covered. This study showed only that using the HAL facilitated functional recovery of patients after TKA. There is a possibility that early functional recovery after TKA promoted by the use of the HAL reduced the hospitalization time. The latter effect would be limited to Japan, where hospital stay is longer than in Western countries.
Furthermore, it was reported by Husted that fast-track knee arthroplasty has low morbidity and mortality, as well as high patient satisfaction. 32 Considering the short hospitalization period for fast-track knee arthroplasty in Western countries, using the HAL will not shorten the length of hospital stay. In Japan, the discharge conditions are much stricter than those in Western countries (i.e. more than 1 m/s on 10-min walk test, visual analog scale <3). Thus, using the HAL can be feasible in Japanese patients given the longer hospital stay.
Clinical messages
This is the first randomized controlled trial of the use of the HAL for rehabilitation after TKA.
The use of the HAL during early rehabilitation after TKA efficiently improved locomotion and reduced pain compared to conventional rehabilitation.
It is necessary to improve the device by adapting it for use after TKA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of the JR Tokyo General Hospital (No. H26-06).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All patients provided written informed consent prior to participation.
Trial registration information
Trial registration number: UMIN000014974; date of registration: 8 September 2014; date of enrollment of the first participant in the trial: 20 November 2014.