
Abstract
A 72-year-old female patient with a fixed valgus knee deformity due to a Schatzker type V tibial plateau fracture treated with bilateral locking plates 8 years ago was admitted to our clinic with complaints of chronic pain and knee instability when walking. Radiographs revealed Kellgren–Lawrence Classification grade 4 knee osteoarthritis and 20.5° of valgus knee deformity. She was treated with three-dimensional templating and proximal lateral tibial fitting patient-specific instrumentation-assisted mechanically aligned posterior sacrificing total knee arthroplasty with minimal removal of the retained hardware for the internal fixation of the tibial plateau fracture via a lateral approach, resulting in a favorable clinical outcome. The use of proximal lateral tibial fitting patient-specific instrumentation in fixed valgus complex primary total knee arthroplasty for patients with retaining hardware for internal fixation to treat tibial plateau fractures is considered a treatment option to decrease surgical invasion.
Keywords
Introduction
Tibial plateau fracture is one of the most challenging fractures for knee and trauma surgeons because of the high incidence of posttraumatic knee osteoarthritis (KOA). 1 Total knee arthroplasty (TKA) is a widely used surgical procedure to alleviate pain and improve daily activities in patients with end-stage KOA. TKA following a tibial plateau fracture is not that common. However, this treatment may complicate tibial component placement during TKA because of the implant position for internal fixation to treat a tibial plateau fracture. 2 Furthermore, hardware removal would impose a physical and financial burden on the patient. 3 Agreement on whether a staged or concurrent approach is preferable for hardware removal during TKA is currently unavailable. 4 TKA without hardware removal would reduce surgical invasion in patients with KOA following a tibial plateau fracture. Herein, we present the case of a 72-year-old female patient with a fixed valgus knee deformity due to a Schatzker type V tibial plateau fracture treated with bilateral locking plates 8 years ago and was treated with proximal lateral tibial fitting three-dimensional templating and patient-specific instrumentation (PSI)-assisted mechanically aligned (MA)-posterior sacrificing (PS) TKA with minimal removal of the retained hardware for the internal fixation of the tibial plateau fracture via the single standard longitudinal skin incision, resulting in a favorable clinical outcome.
Case presentation
A 72-year-old female admitted to our hospital’s Knee Sports Traumatology departmental clinic complained of chronic pain and knee instability while walking. Radiographs demonstrated Kellgren–Lawrence Classification 2 grade 4 KOA and 20.5° of valgus knee deformity. The range of motion (ROM) was 0° of extension and 120° of flexion, and her Forgotten Joint Score (FJS; 0–100 as worst to best) 3 was 25. She had undergone internal fixation using locking compression plate (LCP)-MPTP and LCP-PTP (DepuySynthes, Solothurn, Switzerland) to treat Schatzker type V tibial plateau fracture due to a fall from height 8 years before admission (Figure 1). The preoperative planning of Prophecy Evolution medial pivot patient-specific instrumented knee replacement systems (MicroPort Orthopedics, Inc., Arlington, TN, USA) 4 revealed that at least eight proximal locking screws inserted into medial and lateral LCP required removal during tibial bone resection using a cutting guide following the application of the proximal lateral tibial fitting PSI for the lateral approach (Figure 2). Therefore, PSI-assisted MA-PS TKA, followed by partial screws and LCP removal 5 was planned.

Preoperative images of the right knee. (a, b) Anteroposterior (AP) radiograph of Schatzker type V tibial plateau fracture. (c, d) AP radiograph of valgus knee osteoarthritis 8 years following osteosynthesis. (e) Standing whole-leg plain radiographs. Blue line indicates mechanical axis of right lower limb.
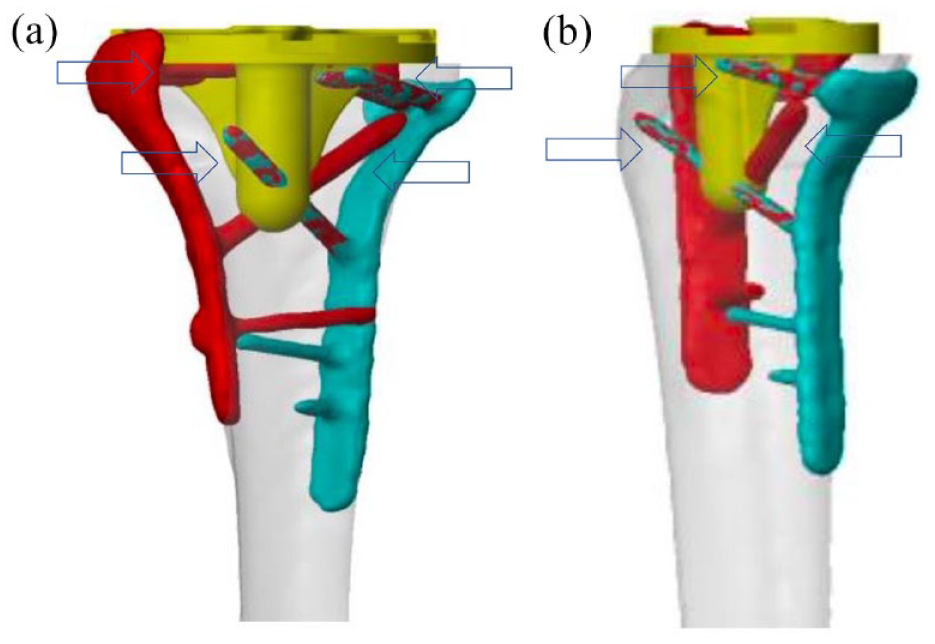
Three-dimensional templating showing that at least eight proximal locking screws required removal during tibial bone resection. (a) Anteroposterior and (b) Lateral view.
The surgical procedure using PSI-assisted MA-PS TKA
Surgery was performed under general anesthesia in the supine position with a pneumatic tourniquet placed on the proximal femur. Varus stress could not reduce valgus knee even under general anesthesia. Therefore, a PS cemented-bearing implant (Evolution, MicroPort Orthopedics, Inc., Arlington, TN, USA) with lateral release via a lateral parapatellar approach was used for the proximal lateral tibial fitting PSI for lateral approach-assisted TKA. First, single standard longitudinal skin incision was made, and the distal iliotibial ligament and lateral bursa were completely released. 6 Patella resurfacing was not performed. Subsequently, eight proximal locking screws inserted into the LCP were removed via the same incision. Then, the distal femoral and proximal tibial cut lines were defined following PSI pin locations to obtain a rectangular extension gap. LCP-PTP placed on the proximal-anterolateral tibia should be removed so that lateral tibial PSI could be placed on the proximal lateral tibia. The femur’s transepicondylar axis (TEA) was 2.8° external to the posterior condyles. First, the osteotomy line of posterior condyles was set parallel to TEA following the size suggestion of the femoral component from PSI to obtain an adequate flexion gap. Then, the thinnest 10-mm PS-fixed bearing was inserted. Fat flapping was performed to cover the capsule defect due to lateral release before incision closure (Figures 3 and 4). The postoperative ROM under anesthesia after incision closure was measured as 0° of extension and 120° of flexion.
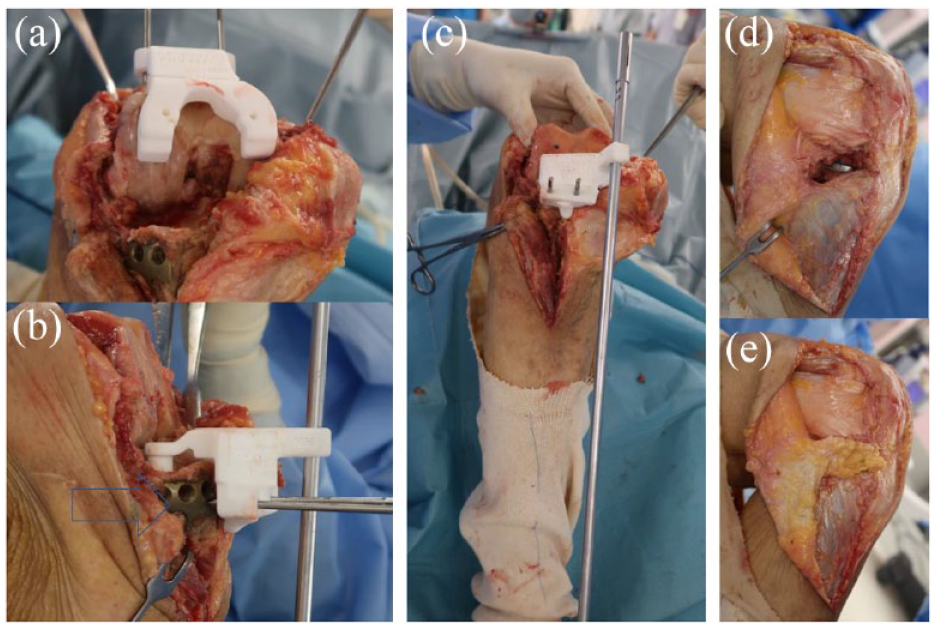
Distal femoral and proximal tibial osteotomies with patient-specific instrumentation. (a) Femoral osteotomy via lateral parapatellar approach. (b and c) The locking plate placed on the proximal-anterolateral tibia had to be removed so that the lateral tibial PSI could be placed on the proximal lateral tibia. The blue arrows indicate that the locking plate was interfering with the pin insertion. (d and e) Fat flapping was performed to cover the capsule defect due to lateral release before incision closure.

Postoperative images of the right knee. (a) Anteroposterior and (b) lateral plain radiographs.
The patient was allowed immediate weight bearing as much as tolerated. There were any complications including dropfoot, superficial and deep infections observed during the 6-month follow-up, and her visual analog scale (0–10 as best to worst) 7 during walking on even ground had improved from 10 to 0, and her FJS 3 had improved from 25 to 5 during the latest follow-up. Postoperative ROM 6 month after surgery remained same as 0° of extension and 120° of flexion.
Additionally, no radiological symptoms of suspected component loosening were observed. Besides, the patient can walk without any crutches.
Discussion
The goal of surgical treatment of tibial plateau displacement fractures is to stabilize the injured knee and restore optimal function, minimizing the risk of posttraumatic arthritis and the eventual need for TKA. However, older patients and patients with severe fractures, such as the present case, are also more likely to require TKA after surgical treatment of tibial plateau fractures; Wasserstein et al. 8 reported that 7.3% of patients 10 years after tibial plateau fracture surgery underwent TKA. This corresponds to a 5.3-fold increase in likelihood compared to the matched cohort. 8 Realignment for severe valgus deformities due to KOA is also challenging. The implant and soft tissue balance selection is a prerequisite for achieving proper alignment and medial and lateral ligament balance. Techniques to release lateral structures, such as the iliotibial band, lateral collateral ligament, popliteus tendon, and posterior cruciate ligament, are necessary. The stiffness of the medial collateral ligament should be noted, and minimal medial release should be allowed only when necessary. 9 In case with retained implants often require hardware removal resulting in medial instability due to medial soft tissue release. The use of a constrained prosthesis may be required in patients with loose medial structures and persistent instability due to extensive soft tissue release. Therefore, we used a proximal lateral tibial fitting PSI for the lateral approach to provide appropriate lateral release with minimal invasion of the medial aspect of the knee. The lateral parapatellar approach is less commonly performed but is an effective approach to address the fixed valgus knee. This technique has been reported to achieve excellent functional and radiological results without increased prosthetic constraints or additional soft tissue release, and it is safe and reliable for fixed valgus deformities while maintaining soft tissue stability. 10 An additional skin incision during internal fixation and a longer operative time are required for retained hardware removal during primary TKA for patients with end-stage KOA. A precedent for staged or concurrent hardware removal is currently unavailable, and a case-by-case approach should be considered. 11 Despite the fact that there are currently no studies comparing the clinical outcomes of KOA patients with hardware retained for tibial plateau rupture with and without PSI, Thienpont et al. 12 described that the use of PSI to perform TKA in patients without access to the intramedullary canal due to fixation devices resulted in improved function and restored limb alignment within acceptable hemostatic times averaging up to 75 min (range, 62–83 min). This surgical technique enabled PSI-assisted MA-TKA with minimal removal of the retained hardware for the internal fixation of the tibial plateau fracture via the single standard longitudinal skin incision without addition of another two-stab wound.
Conclusion
The use of preoperative 3D templating is useful to determine the screws that may interfere with the implant for patients with retaining hardware for internal fixation to treat tibial plateau fracture. In addition, proximal lateral tibial fitting PSI in fixed valgus complex primary TKA may be a useful treatment option to decrease surgical invasion.
Footnotes
Acknowledgements
The corresponding author would like to thank Yuka Kato, and Kenichi Tada of Microport Orthopedics.
Author contributions
Y.M., T.T., M.I., A.S., and K.T. designed and wrote the article. H.S., M.H., and T.M. participated in the surgery. All the authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: One of the authors received a grant for another clinical research as a principal investigator from MicroPort Orthopedics, Inc., Arlington, TN, USA.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.