
Abstract
Background:
The relationship between systemic inflammatory processes to total knee arthroplasty (TKA) outcomes remains unclear. This study investigates the relationship between serum high-sensitivity C-reactive protein (hs-CRP) and functional outcomes post-TKA.
Methods:
A total of 31 patients with osteoarthritis (OA) who underwent TKA were enrolled in the study; 15 with hs-CRP ≤1.0 mg/l (low hs-CRP group) and 16 subjects with hs-CRP ≥4.0 mg/l (high hs-CRP group). During surgery, synovium and bone sections were sequestered, formalin-fixed, and paraffin embedded for slide preparation. Tissue sections were stained with hematoxylin and eosin and analyzed using a light microscope. A total of 12 cytokines were measured in synovial fluid samples from the knee joint at time of surgery and analyzed using the Luminex Multi-Analyte Profiling System. Relationships between cytokines and hs-CRP were assessed using Spearman correlation coefficients. Student’s t-tests were used to compare Short Form health outcomes survey (SF-12) health outcomes between high and low hs-CRP, and presurgical and postsurgical visits.
Results:
Mean ± standard deviation (SD) baseline and 1-year hs-CRP values for the low hs-CRP group were 0.55 ± 0.23 mg/l and 1.22 ± 1.32 mg/l, respectively (n = 15; p = 0.051) and for the high hs-CRP group were 7.86 ± 5.98 mg/l and 14.11 ± 38.9 mg/l, respectively (n = 13; p = 0.54). Lymphocytes were present in 10 synovium and one bone sample (all but one from high hs-CRP group). Interleukin (IL)-5 and IL-10 were significantly correlated with hs-CRP (p = 0.0137 and p = 0.0029, respectively). The low hs-CRP group exhibited significant improvement in the physical component of SF-12 at 6 and 12 months compared with baseline, whereas the high hs-CRP group exhibited significant improvement only at 6 months. Body mass index (BMI) had a significant positive correlation with presurgical hs-CRP.
Conclusions:
The results of this study provide support for inflammatory mechanisms contributing to the OA progression, with hs-CRP being a possible predictive variable, combined with BMI and other comorbidities, of post-TKA function.
Introduction
Osteoarthritis (OA) is the most common type of arthritis, affecting nearly 27 million Americans [Lawrence et al. 2008], or 12% of adults in the United States. By the year 2030, this number is expected to reach 72 million or about 20% of the adult US population [Bitton, 2009; Elders, 2000]. The combined annual cost of medical care and lost wages due to OA is expected to approach US$100 billion by the year 2020 [Bitton, 2009; Elders, 2000; Leigh et al. 2001]. This growing financial burden combined with the negative impact OA has on quality of life has resulted in heightened interest in developing more objective measures for identifying OA early in the disease process, as well as improved treatment modalities and rehabilitation protocols.
OA is characterized by joint space deterioration, pain, and loss of motion resulting in restricted activity and loss of independence during activities of daily living [Crepaldi and Punzi, 2003; Punzi and Oliviero, 2005]. The typical treatment modalities for OA include drug therapy, exercise, weight control, and in more severe cases, surgical intervention including total knee arthroplasty (TKA). While the goals of TKA are relief of pain and improvement in function, the factors that influence long-term surgical treatment outcomes of OA have not been clearly delineated [National Institutes of Health, 2003].
Bone quality has been implicated in the success rate of primary surgical outcomes as well as revisions, and has been the focus of recent research to identify the clinical relevance of biomarkers of inflammation including high-sensitivity C-reactive protein (hs-CRP) [Conrozier et al. 1998] and cytokine levels [Perovic-Rackov and Pejnovic, 2006] in relation to disease activity and bone quality.
CRP, in particular, is produced in response to inflammation, infection, and injury, and has been correlated with complications related to conditions such as hypertension, cardiovascular disease, and diabetes [Ablij and Meinders, 2002; Dalton et al. 2003; DiNapoli and Papa, 2003; Gabay and Kusher, 1999]. In relation to OA, elevated levels of CRP have been correlated with synovial fluid interleukin (IL)-6 and degree of synovial fluid infiltration [Pearle et al. 2007], as well as symptoms of pain and stiffness, radiographic gradings [Sturmer et al. 2004; Takahashi et al. 2004], and disease progression [Conrozier et al. 1998, 2000; Sharif et al. 2000]. However, the relation between hs-CRP and localized cytokine levels, as well as surgical outcomes is still unclear.
The purpose of this study was to investigate the relationship between serum hs-CRP and postoperative functional outcomes in patients with OA who elected to undergo TKA. It was expected that hs-CRP would correlate with indices of inflammation found in bone and synovium biopsies, as well as with postsurgical functional improvement, in patients undergoing TKA.
Methods
The study was approved by an Institutional Review Board and all patients consented prior to enrollment in the study. Serum hs-CRP and synovial fluid cytokine measurements were obtained in 31 subjects, between 2007 and 2009, who underwent either unilateral or bilateral TKA, all of which were performed by the same orthopedic surgeon (Park City, UT). Subjects were enrolled based on the diagnosis of OA, which was confirmed preoperatively with radiographs and careful review of past medical conditions. Additional examination of the patients’ extremities was performed to exclude patients who had any typical signs/deformities of rheumatologic disease. None of the patients in the study had a previous history of rheumatoid arthritis (RA) or exhibited signs/symptoms of RA. Patients were enrolled based on their hs-CRP: 15 were enrolled with an hs-CRP level less than or equal to 1.0 mg/l (low hs-CRP group) and 16 with an hs-CRP level greater than or equal to 4.0 mg/l (high CRP group). Owing to the lack of hs-CRP risk stratification levels for OA patients, subjects were stratified into hs-CRP levels based on levels associated with low and high risk of developing stroke, myocardial infarction, and severe peripheral vascular disease [Myers et al. 2009].
Serum hs-CRP was measured prior to surgery and at 1-year postsurgery using the ARCHITECT c8000 (Abbott Diagnostics, Abbott Park, IL), which is an open-reagent system that utilizes spectrophotometry to analyze samples. Subjects included males or females between 45 and 76 years of age who were not using medication that may artificially alter hs-CRP including lipid-lowering therapies such as HMG-CoA (3-hydroxy-3-methylglutaryl-coenzyme A) reductase inhibitors, fibric acid derivatives, niacin, or bile acid sequestrants within 6 weeks of study enrollment. Other exclusion criteria included: (a) current use of oral hormone replacement therapy (HRT); (b) current treatment with cyclosporin, tacrolimus, azathioprine, or other immunosuppressants including chronic use of oral glucocorticoids; (c) current use of insulin and/or an oral hypoglycemic agent; (d) history of malignancy within the past 5 years, with the exception of basal cell or squamous cell carcinoma of the skin; (e) use of thyroid replacement therapy that was initiated or modified within the last 3 months; (f) presence of a known chronic inflammatory condition not related to bone health such as, but not limited to, severe lupus or inflammatory bowel disease; (g) history of alcohol or drug abuse within the past 1 year; and (g) participation in another investigational drug study <30 days before enrollment in the current study.
Gross bone appearance (bone health) was evaluated during surgery using a five-point qualitative scale. The bone health score was based on the surgeon’s qualitative assessment of bone color, density, and visual presence of cysts and/or necrosis where a score of ‘1’ represented poor bone health and ‘5’ represented good bone health, with the following scale (1 = presence of cystic/necrotic disease; 2 = average density, grayish/pale color, and precystic/oxidative disease; 3 = moderate density and minimal oxidative changes; 4 = moderate to optimal density and golden color, and slight to no signs of inflammation; and 5 = optimal density, golden color, and no inflammation). Evaluations were performed independent of knowledge of hs-CRP levels and were confirmed by the physician’s assistant also participating in the surgery.
During surgery, synovium and bone sections removed from the femoral condyle to perform the TKA were sequestered, formalin-fixed, and paraffin embedded for slide preparation. Tissue sections were stained with hematoxylin and eosin (H&E) and analyzed using a light microscope by a trained pathologist (ARUP Laboratories, Salt Lake City, UT). Results were compared to identify correlations between presence or absence of inflammatory cells and hs-CRP values.
A small sample of synovial fluid was removed from around the knee joint during surgery and analyzed by ARUP Laboratories (Salt Lake City, UT) for cytokine concentrations. For subjects with bilateral knee replacements, one sample was obtained from each knee. A total of 12 cytokines were measured using the Luminex Multi-Analyte Profiling System, developed at ARUP Laboratories (Salt Lake City, UT); IL-1b, IL-2r, IL-4, IL-5, IL-6, IL-8, IL-10, IL-12, IL-13, tumor necrosis factor (TNF)-α, CD401, and interferon (IFN)-γ. The multiplexed cytokine assay was developed and validated in the ARUP Institute for Clinical and Experimental Pathology using a standard sandwich capture format and has been described previously [Martins et al. 2002, 2004].
Radiograph reviews were performed to identify correlations in rehabilitation and progression of healing between the low and high hs-CRP groups. Evaluations were performed using the Knee Society Roentgenographic Scoring System (KRSS) [Ewald, 1989], a standardized scoring system that allows comparisons across implant types and institutions. Based on the KRSS, a seven zone femoral implant component, seven zone tibial implant component, and five zone patellar implant component were used for the purposes of scoring. The scoring system for each of the three components is determined by measuring the width of the radiolucent lines for each of the zones (in millimeters). The total widths are added together for each zone and each of the three components. For each subject, lucency was measured at all implant component zones on the 6 week (Study Visit 3), 6 month (Study Visit 4), and 1 year (Study Visit 5) radiographs. A total score of 4 or less in any zone was considered insignificant, 5–9 indicated that the patient should be closely followed for progression, and 10 or greater signified possible or impending failure regardless of symptoms. In the event that migration or shifting of the prosthesis was present on the radiograph, this was considered as a possible or impending failure regardless of the total score [Ewald, 1989].
Health outcomes were assessed using the SF-12v2 Health Survey which was completed at baseline (preop), 6 months postop, and at 12 months postop using categorical, norm-based scoring for physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), vitality (VT), social functioning (SF), role emotional (RE), and mental health (MH). Physical component summary (PCS) and mental component summary (MCS) values were also computed. Raw scores were converted to norm-based scoring using methods described in the SF-12v2 User’s Manual. PCS and MCS scores were also converted to z-scores and then transformed using coefficients presented in the SF-12 User’s Manual [Ware et al. 2002].
Statistical analyses
Subject demographics were summarized using descriptive statistics. Tests for equal variance were performed and appropriate two-tailed Student’s t-tests were used to compare bone scores, body mass index (BMI), and age between low and high hs-CRP groups. Two-tailed t-tests were also used to compare SF-12 results between high and low hs-CRP, and two-tailed t-tests for paired data were used to compare results between presurgical and postsurgical visits. Missing data were excluded analysis by analysis, allowing for different sample sizes across tests.
Qualitative relationships were evaluated between presurgical serum hs-CRP and bone and synovium histological assessments. Histological assessments were performed by a trained pathologist at ARUP laboratories.
For subjects who had more than one synovial fluid sample (i.e. five subjects who had bilateral TKA and five subjects who had unilateral TKA, but had more than one tissue sample sequestered from the same knee), the variability within samples was compared with the variability between subjects. The correlation within subjects for all samples was greater than between subjects and, therefore, the samples within subjects were averaged and this value was used for comparison between subjects.
Multiple variable logistic regression analyses were performed to identify correlations between low and high hs-CRP and synovial fluid cytokines. Cytokine results were determined to have a nonnormal distribution and, therefore, spearman correlation coefficients were used and receiver operating characteristic (ROC) curves were developed to evaluate sensitivity versus specificity of hs-CRP compared with cytokines, and area under the curve (AUC) for each variable compared with hs-CRP.
Results
A total of 31 subjects were enrolled in the study with one subject in the high hs-CRP group discontinuing after Study Visit 2 due to noncompliance with Study Visits 3–5. This subject underwent TKA, and synovium and bone samples were sequestered during surgery and, therefore, these data were included in the cytokine and histological analyses, but not in the SF-12 analyses. Two additional subjects in the high hs-CRP group did not complete the 1-year hs-CRP measurement.
Five subjects underwent bilateral TKA; three in the low hs-CRP group and two in the high hs-CRP group. A total of 28 subjects were implanted with a Duracon press fit implant (Stryker Orthopaedics, Mahwah, NJ), and three subjects were implanted with the Triathlon press fit implant (Stryker Orthopaedics, Mahwah, NJ). Patient demographics are summarized in Table 1.
Subject demographics and hs-CRP at baseline.
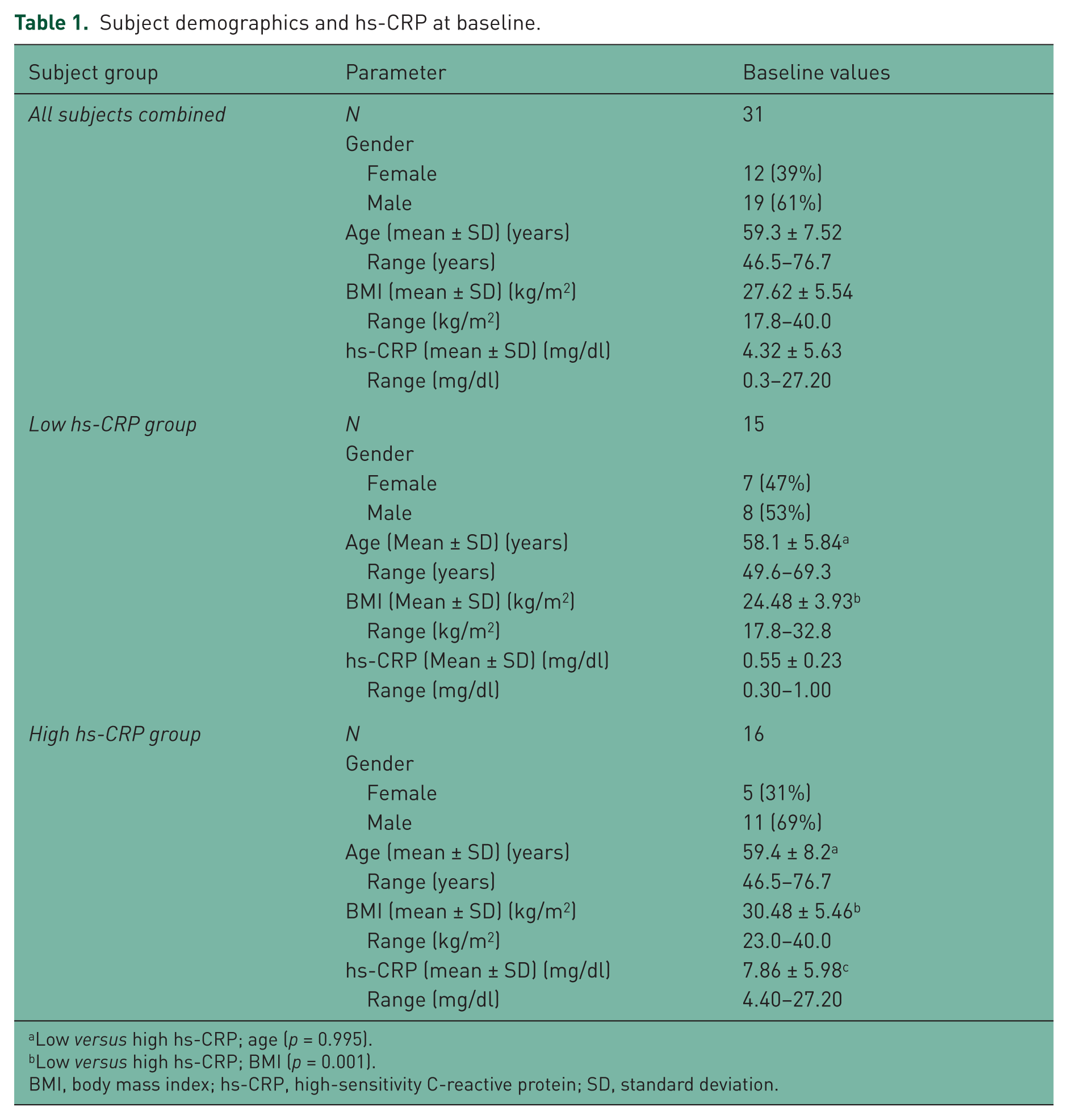
Low versus high hs-CRP; age (p = 0.995).
Low versus high hs-CRP; BMI (p = 0.001).
BMI, body mass index; hs-CRP, high-sensitivity C-reactive protein; SD, standard deviation.
hs-CRP
Baseline hs-CRP values ranged from 0.3 to 1.0 mg/l (mean ± SD: 0.55 ± 0.23 mg/l; n = 15) for the low hs-CRP group and from 4.4 to 27.2 mg/l (mean ± SD: 7.86 ± 5.98 mg/l; n = 16) for the high hs-CRP group. The mean ± SD, 1-year follow-up hs-CRP for the low and high CRP groups were 1.22 ± 1.32 mg/l (n = 15) and 14.11 ± 38.9 mg/l (n = 13), respectively. There was no 1-year hs-CRP measurement available for three subjects in the high hs-CRP group; one subject was discontinued after Study Visit 2 and two subjects did not complete the 1-year follow-up hs-CRP measurement. The hs-CRP values were not significantly different between baseline and 1 year for the high hs-CRP group (p = 0.55), but were nearly significantly higher at 1 year for the low hs-CRP group (p = 0.051).
Cytokines
Cytokine analyses were performed on all but two subjects. One subject’s synovial fluid sample could not be quantitated and one sample was not sequestered during surgery. All cytokines except IL-2 were detectable in synovial fluid samples and, therefore, IL-2 was omitted from the analysis. The mean value for all cytokines measured, with the exception of CD-40 ligand, were higher in the high hs-CRP group than the low hs-CRP group (Table 2).
Mean cytokine values measured in synovial fluid.

The number of subjects included in the hs-CRP analysis for cytokines does not include the two subjects for which cytokines were not analyzed; one subject’s sample could not be quantitated and one subject’s sample was not obtained.
Cytokine results were averaged for all subjects who had more than one sample; this includes subjects for which more than one sample was taken from the same knee and subjects who had one sample taken from each knee (i.e. in the case of bilateral TKAs).
Two-sided t-test comparing low and high hs-CRP groups, p = 0.029.
IFN, interferon; IL, interleukin; hs-CRP, high-sensitivity C-reactive protein; SD, standard deviation; TKA, total knee arthroplasty; TNF, tumor necrosis factor.
Data were determined to be non-normally distributed and, therefore, nonparametric analyses were performed. Spearman correlation coefficients for all subjects combined ranged from −0.31 (p = 0.0977) for IL-6 versus CD40L, to 0.75 for IL-4 versus IL-13 (p < 0.001). When data from all subjects were combined, statistically significant correlations occurred for 24 different cytokine comparisons (Table 3). IL-10 and IL-5 were significantly correlated with hs-CRP (p = 0.0029 and p = 0.0137, respectively) and IL-10 showed the most significant trend toward being a positive predictor for high hs-CRP (i.e. hs-CRP ≥4.0 mg/l; p = 0.055) with an AUC of 0.76.
Spearman correlation coefficients and corresponding p-values for synovial fluid cytokines and hs-CRP (all subjects combined).

IFN, interferon; IL, interleukin; hs-CRP, high-sensitivity C-reactive protein; SD, standard deviation; TKA, total knee arthroplasty; TNF, tumor necrosis factor.
There was a significant difference between the low and high hs-CRP groups for IL-10 (2.81 pg/ml versus 6.10 pg/ml, respectively; p = 0.029) and a trend toward significance for IL-6 (33.79 pg/ml versus 176.28 pg/ml, respectively; p = 0.079). Otherwise, there were no significant differences between the low and high hs-CRP groups for any of the cytokines measured (Table 2).
Bone health
Gross bone appearance (bone health) was evaluated during surgery using a five-point qualitative scale described above. The overall bone health score was based on the surgeon’s qualitative assessment, without prior knowledge of hs-CRP level, of bone color, density, and visual presence of cysts and/or necrosis. Of the subjects who had lymphocytes present in their synovium sample, five had a bone score of 1; two had a score of 2; and three had a score of 3. The low hs-CRP group had a significantly higher average bone score than the high hs-CRP group (2.9 versus 2.0; p = 0.014) indicating better overall bone health.
Figure 1(a) is a representative image, taken during surgery, of bone from a high hs-CRP subject with a bone score of 1 (i.e. poor bone health). In contrast, Figure 1(b) shows a subject with a bone score of 4 who was in the low hs-CRP group.

(a) Photograph of representative patient with high hs-CRP. Patient has hypertrophic bone spurs on patella and darkened areas in bone indicative of poor bone quality. (b) Photograph of representative low hs-CRP subject’s bone with a bone score of 4. Note the consistency of the color and lack of gross cystic or inflammatory changes.
Histological examination revealed signs of synovitis including lymphocytes in 10 synovium samples and one bone sample, and neutrophils in one bone sample. Nine of the synovium samples that contained lymphocytes were from the high CRP group (one bilateral TKA subject had lymphocytes present in both synovium samples). The subject with lymphocytes present in bone was also in the high hs-CRP group, as was the subject with neutrophils present.
Radiographic evaluation
Radiograph reviews were performed at 6 weeks, 6 months, and 1 year post-op using the KRSS [Ewald, 1989]. Overall, there were 28 subjects that had 1-year radiographs available for review; 23 subjects with unilateral and 5 subjects with bilateral (10 total), for a total of 33 radiographs. At the 1-year postop visit, there was no lucency in any subject radiographs, and no revisions were required for any subject during the first year of follow up.
Health and functional outcomes: SF-12 Health Survey
SF-12 results were evaluated at baseline (preop), and at 6 months and 1 year postop using categorical scoring for PF, RP, BP, GH, VT, SF, RE, and MH. PCS and MCS values were also computed. Norm-based scoring was used for all SF-12 parameters as well as for PCS and MCS comparisons. The results showed that SF-12 parameters assessed in this study were higher than published norms for subjects with OA in the general population, with the exception of bodily pain, which was lower in the present study population.
There was a statistically significant difference between low and high hs-CRP groups at the baseline evaluations for MCS (p = 0.0206), GH (p = 0.0250), SF (p = 0.0174), and RE (p = 0.0302). Otherwise, there were no significant differences between low and high CRP groups at any other visits for any of the SF-12 parameters.
Both the low and high hs-CRP groups showed improvements in PCS following surgery, with the low CRP group showing a greater improvement at 1 year than the high hs-CRP group (Figure 2). MCS worsened postsurgery for the low CRP group, but improved postsurgery for the high CRP group (Figure 3).

Physical Component Summary (PCS) results by low and high C-reactive protein (CRP) groups (baseline, 6 months postop, and 1 year postop). **p < 0.05 compared with baseline (presurgery).

Mental Component Summary (MCS) results by low and high C-reactive protein (CRP) groups (baseline, 6 months postop, and 1 year postop). **p < 0.05 compared with baseline (presurgery).
Discussion
Inflammation has been implicated in the pathogenesis of OA, yet the specific correlations between biomarkers of inflammation are still being elucidated. The primary goal of the present study was to evaluate potential correlations between hs-CRP and postoperative functional outcomes.
In the current study, there was a correlation between patients with elevated serum hs-CRP (≥4.0 mg/dl) and the presence of inflammatory changes in synovium samples taken from the knee joint in patients with OA. Upon histological examination, lymphocytes were present in 10 synovium samples and one bone sample, all but one from the high hs-CRP group. This finding is consistent with other studies suggesting that the presence of inflammatory synovitis in individuals with OA, which includes the infiltration of macrophages and lymphocytes, is indicative of more severe pain and joint dysfunction, and may be more predictive of faster rates of cartilage loss [Sellam and Berenbaum, 2010; Scanzello and Goldring, 2012]. In addition, there was a correlation between bone health (based on gross visual appearance), serum hs-CRP, and synovial fluid cytokines. While these secondary findings lend support for greater localized inflammation in individuals with higher hs-CRP, it is not clear how localized inflammation may have affected functional outcomes postoperatively.
The bone health score used in this study was based on several years of observation by the principal investigator of this study. It became obvious after performing hundreds of TKA surgeries and measuring hs-CRP in subjects undergoing TKA surgery, that there are gross visual differences in bone and tissue quality between subjects with low and high hs-CRP. These observations were further refined based on visual observations including color, presence of cysts or other oxidative changes, and bone density, which is easily discerned via the bone cuts required to install a knee implant. Although the scoring system has not been thoroughly validated, the results of this study provide evidence supporting the potential merit of the scale and the possibility of evaluating bone health through simple observation and clinical experience. Consistent with prior studies, BMI was significantly higher in the high hs-CRP group than the low hs-CRP group. Although this correlation is not an unfamiliar finding [Timpson et al. 2010], the results support the growing body of evidence that BMI and obesity are correlated with inflammation, as well as the progression of OA [Conrozier et al. 1998, 2000; Sharif et al. 2000]. This finding is also an important consideration in the present study, as a higher BMI in the high hs-CRP group may provide an alternative explanation for the poorer functional outcomes postoperatively in the high hs-CRP group. Support for this explanation are found in a study by Jones and colleagues, where severe obesity was shown to be a significant risk factor for worse pain and functional recovery at 6 months post-TKA [Jones et al. 2012], as well as a study by Gandhi and colleagues that showed a correlation between obesity and poorer outcomes post TKA [Gandhi et al. 2010]. The authors of the latter study concluded that patient function following joint replacement surgery is negatively affected by metabolic abnormalities which is possibly related to a systemic proinflammatory state. In contrast to these findings, a study by Stevens-Lapsley and colleagues showed no correlation between BMI and functional outcomes at 1, 3, and 6 months post-TKA [Stevens-Lapsley et al. 2010]. A potential explanation for the equivocal results is differences in methodology of how functional outcomes were measured, as well as the presence of comorbidities and associated inflammation. These findings highlight the need for additional research to delineate the impact of BMI, metabolic abnormalities, as well as inflammation on relevant functional outcomes, and how postop rehabilitation may be designed to best address these deficits.
Research has also shed light on the association between synovitis and cytokines in the pathogenesis of OA and suggests that cytokines play an important role in the progression of OA [Luyten et al. 2006]. To further understand how cytokines may influence the progression and presentation of OA and their potential relationship with hs-CRP, we evaluated 12 cytokines measured in synovial fluid samples in patients with OA undergoing TKA. Results showed a significant difference in IL-10 between the low and high hs-CRP groups, and IL-6 trended toward a significant difference between the two CRP groups. IL-10, in particular, has been shown to have a significantly greater presence in osteoarthritic chondrocytes compared with healthy controls [Iannnone et al. 2001] and has been suggested as a potential therapeutic target for OA due to its anti-inflammatory effects and inhibition of IL-1 and TNF-α synthesis [Fernandes et al. 2002]. Results from the present study lend further support to the potential role of IL-10 and other cytokines in the pathogenesis of OA.
Radiographic results showed no visible lucency at 1 year in any subject, indicating that the appropriateness of the prostheses used was not significantly affected by the subjects’ initial bone health or inflammatory status. Although a higher BMI, and associated hs-CRP, would be expected to be associated with a higher implant failure rate, the highly variable and multifaceted nature of implant failures would dictate a much larger patient population to identify how the parameters investigated in this study may affect the rate of implant failure. Additional research is indeed necessary to delineate how inflammatory processes or expectation of postsurgical functional ability may influence the choice of implant.
Nonetheless, there were differences in the SF-12 health survey results presurgery and postsurgery between the two CRP groups, suggesting that the presence of increased inflammatory processes may affect long-term rehabilitation and physical function. More specifically, quality of life evaluations were performed using the SF-12v2 scoring system, the results of which were consistent with other studies of subjects undergoing TKA. Specifically, Hartley and colleagues showed improvements in the SF-12 physical scores in both primary and revision TKA subjects that were highly statistically significant at 6 months [Hartley et al. 2002]. Similarly, in the present study, when all subjects were combined, there was a statistically significant improvement in PCS postsurgery at both 6 and 12 months. In addition, there was greater improvement in physical function for the low hs-CRP group postsurgery, compared with the high hs-CRP group, even though they had similar presurgery PCS scores. The low hs-CRP group achieved a PCS similar to that of the general population postsurgery, whereas the PCS score for the high hs-CRP group remained below the mean values. This is an important finding considering the general, long-term deficits in physical function in TKA patients, and points to the need for modified or improved rehabilitation protocols for patients with elevated CRP.
Overall, these findings may indicate a potentially better long-term prognosis for the low hs-CRP group with regard to physical function, but it is unclear how the mental component of SF-12 factors in. The MCS score declined in the low hs-CRP group at the postsurgical evaluations, but improved, nonsignificantly, in the high hs-CRP group. This may point to improved, presurgical, mental well-being in the low hs-CRP group that was affected negatively by the rehabilitation process postsurgery. At the 1-year visit, the low hs-CRP group’s MCS score increased somewhat compared with the 6-month visit, but was still below the initial level.
The limitations of the study include the small sample size, lack of a healthy control group, lack of validation of the bone scoring system, and follow up of only 1 year postop. Because a healthy control group was not included in this study, it was not possible to determine whether the inflammation observed in this study was a cause or symptom of OA, or a contributing factor to joint degradation. It is suspected that the answer is multifaceted with many inflammatory pathways contributing to and acting in concert to both cause and mitigate inflammatory processes systemically.
It is recognized that the bone score used in this study has not been thoroughly validated and additional research is required to fully understand how gross bone appearance may correlate with overall bone health, and how this information may be used to guide surgical decisions. While the bone scoring method used in this study was validated by two individuals participating in the surgery (the surgeon and physician’s assistant, who is also an author on this manuscript), it requires validation by additional, independent surgeons to ensure validity and reliability of the measurement. Future research should evaluate correlations between cytokines in synovial fluid to results in serum. The latter is clearly a more appropriate clinical test that could be distributed to a large number of patients.
This study also discerned a possible link between hs-CRP level and joint pathogenesis and potentially reduced physical function postsurgery. There were clear differences between cytokine levels in the two CRP groups, but the small sample size may have affected the ability to identify additional significant correlations.
Conclusions
The results of this study showed that patients with OA who also had elevated hs-CRP have increased cytokine levels and inflammatory changes indicative of synovitis compared with subjects with OA and lower hs-CRP. The clinical implications of this finding suggest that hs- CRP may be useful, in combination with other indicators of poor outcomes such as BMI and other comorbidities, as a possible predictive variable of severity of OA, rate of progression, and long-term level of postoperative improvement.
While the findings of this study are considered preliminary, markers of inflammation and gross bone health may eventually assist in determining the most appropriate knee replacement implant and rehabilitation protocol for individual patients to ensure optimal recovery and activity post-surgery. The findings point to possible rehabilitation targets postsurgery that extend beyond muscle strength and function, to address overall lifestyle changes to lower hs-CRP and other lifestyle-related indices. Further research is needed to identify long-term implications of inflammation in patients undergoing TKA.
Footnotes
Funding
Financial support for the study was provided by Stryker Orthopedics (Mahwah, NJ).
Conflict of interest statement
Stryker Orthopedics provided funding for activities directly related to this research project, from which Jessica Smith was paid for her activities directly related to this project. Dr Rosenberg also previously received consultancy fees from Stryker Orthopedics for various activities, which are not currently ongoing. There are no other potential conflicts of interest.