
Abstract
Background:
The objective of this study was to assess healthcare utilization and complications associated with acute kidney injury (AKI) in patients undergoing primary total knee arthroplasty (TKA).
Methods:
We used the 1998–2014 US National Inpatient Sample to assess whether AKI is associated with healthcare utilization or in-hospital postoperative complications post-TKA using multivariable-adjusted logistic regression analyses. We calculated odds ratios (ORs) and a 95% confidence intervals (CIs). Sensitivity analyses additionally adjusted for hospital characteristics (location/teaching status, bed size, and region).
Results:
Of the 8,127,282 people who underwent primary TKA from 1998 to 2014, 104,366 (1.3%) had a diagnosis of AKI. People with AKI had longer unadjusted mean hospital stay, 6.1 versus 3.5 days, higher mean hospital charges, US$71,385 versus US$42,067, and higher rates of all in-hospital postoperative complications, including mortality. Adjusted for age, sex, race, underlying diagnosis, medical comorbidity, income, and insurance payer, AKI was associated with a significantly higher OR (95% CI) of total hospital charges above the median, 2.76 (2.68, 2.85); length of hospital stay > 3 days, 2.21 (2.14, 2.28); and discharge to a rehabilitation facility, 4.68 (4.54, 4.83). AKI was associated with significantly higher OR (95% CI) of in-hospital complications, including infection, 2.60 (1.97, 3.43); transfusion, 2.94 (2.85, 3.03); revision, 2.13 (1.72, 2.64); and mortality, 19.75 (17.39, 22.42). Sensitivity analyses replicated the main study findings, without any attenuation of ORs.
Conclusions:
AKI is associated with a significantly higher risk of increased healthcare utilization, complications, and mortality after primary TKA. Future studies should assess significant factors associated and interventions that can prevent AKI.
Introduction
Acute kidney injury (AKI) is a feared complication of total joint arthroplasty, an elective surgery performed to improve pain and function. More than one third of all AKI cases occur in surgical settings.1,2 AKI is common, affecting 22% of adults and 34% of children, associated with a mortality of 24% in adults and 14% in children, 3 a problem that is worse in developing countries. 4 AKI is associated with a higher risk of long-term chronic kidney disease (CKD) and end-stage renal disease (ESRD), 5 making it a major public health problem.
In a single-center study, 15% of all patients undergoing total joint arthroplasty developed AKI. 6 Increased body mass index (BMI), older age, lower preoperative glomerular filtration rate and use of angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers were each associated with a higher risk of AKI. 6 The use of antibiotics in the perioperative period is also associated with the risk of AKI. 7 In a recent review of AKI after arthroplasty, higher BMI, metabolic syndrome, antihypertensive medications, perioperative antibiotics, antibiotic-impregnated cement, cerebral or peripheral vascular disease, use of general anesthesia, and perioperative blood transfusions were independently associated with risk for AKI. 8 Major limitations included most studies being single centered with small sample size, and most examined a limited number of variables in the analyses of TKA complications related to AKI.
Very few studies have examined healthcare utilization outcomes after TKA. In a Scottish study of 413 consecutive patients who underwent TKA/total hip arthroplasty (THA), 8% developed AKI, associated with 50% longer hospital stay. 9 AKI was associated with increased hospital length of stay and cost across several health conditions. 10 Most studies combined both knee and hip arthroplasty patients,9,11 while these surgeries and their outcomes differ from each other. 12 Our objective was to assess whether AKI was associated with higher healthcare utilization and in-hospital complications after primary TKA, using a representative national sample.
Methods
Data source and study cohort
We used the nationwide inpatient sample (NIS) from 1998–2014 to perform this study. The NIS is a 20% stratified sample of all discharge records from all participating community hospitals from all participating states in the United States. 13 Unweighted, the NIS has data from more than 7 million US hospitalizations each year, which estimates more than 35 million hospitalizations nationally (weighted). The University of Alabama at Birmingham’s Institutional Review Board approved this study (X120207004) and waived the need for informed consent for this database study since these national data are de-identified. All investigations were conducted in conformity with ethical principles of research.
Our study cohort consisted of all people who underwent primary TKA in the US from 1998 to 2014, identified by the presence of International Classification of Diseases, ninth revision, common modification (ICD-9-CM) code of 81.54, as the primary procedure code for hospitalization, a validated approach with a high positive-predictive value of 95%. 14 The underlying diagnosis for TKA was listed as the primary diagnosis code for index TKA hospitalization.
We identified the occurrence of AKI by the presence of ICD-9-CM code of 584.5, 584.6, 584.7, 584.8, or 584.9, listed as a secondary diagnosis for index TKA hospitalization. The use of these diagnostic codes for AKI is a validated approach used previously by other researchers. 15 The positive-predictive value of using ICD-9-code-based approach was 98% in the National Hospital Discharge Survey (a dataset similar to the NIS) compared with serum-creatinine-based laboratory criteria. 16
Study outcome, and covariates
We assessed healthcare utilization outcomes and common in-hospital post-TKA surgical complications and mortality. Healthcare utilization outcomes for the index primary TKA hospitalization included total hospital charges, length of hospital stay, and discharge to home versus a rehabilitation facility, that is, intermediate care facility, a certified nursing facility, rehabilitation facility, or a skilled nursing facility.
We assessed several postoperative in-hospital complications, including infection, transfusion, TKA revision, and mortality during the index admission for primary TKA, as surgical complications and possible contributors to, or a result of, AKI, based on the presence of the following ICD-9-CM codes listed as a secondary diagnosis for index TKA hospitalization: (a) infection, 711.xx, 730.xx, 996.66 or 996.67; (b) transfusion, 99.0x; (3) revision, 81.55. 00.80, 00.81, 00.82, 00.83, 00.84, 84.56, 84.57 or 80.06; and (4) mortality.
We examined several covariates including patient socio-demographics, the underlying diagnosis for primary TKA, medical comorbidity, insurance payer type, and hospital characteristics. Socio-demographics included age (<50, 50–<65, 65–<80 and ⩾80 years), sex, race/ethnicity (White, Black, Hispanic versus other), and annual household income categorized as quartiles, based on residential zip code. The underlying diagnosis for primary TKA was the primary diagnosis for index hospitalization. It was categorized as osteoarthritis, rheumatoid arthritis (RA), fracture, avascular necrosis of the bone (AVN) or other. Medical comorbidity was assessed using the Deyo-Charlson Index, a validated measure of medical comorbidity consisting of 17 comorbidities, based on the presence of ICD-9-CM codes, 17 categorized as none, one or at least two comorbidities. Health insurance payer was categorized as Medicare, Medicaid, private insurance, self-pay, or other.
Hospital location/teaching status was categorized as rural, urban nonteaching or urban teaching. Hospital bed size was classified as small, medium, or large, using the NIS cut-offs that vary by the year. Hospital region was categorized as Northeast, Midwest, South, and West.
Statistical analyses
We implemented survey analysis procedures that accounted for the weights, clusters, and strata, as defined in NIS, including the modified weights with the change in sampling in 2012. 13 We compared the characteristics of people with versus without AKI using the t test for continuous and chi-squared test for categorical variables. We assessed each healthcare utilization outcome and in-hospital postoperative complication with a separate multivariable logistic regression, including exposure of interest (AKI) and all covariates (sociodemographics, comorbidity, insurance, income, underlying diagnosis) listed above. Healthcare utilization outcomes for the index primary TKA hospitalization were analyzed as follows: total hospital charges above the median, length of hospital stay > 3 days (median), and discharge to a nonhome setting such as rehabilitation/inpatient facility, which included a skilled nursing facility, intermediate care facility, certified nursing facility, or rehabilitation facility.
We calculated the odds ratios (ORs) and 95% confidence intervals (CIs). We performed sensitivity analyses that additionally adjusted each main analysis for hospital variables (location/teaching status, bed size, and region), and a sensitivity analyses for revision surgery outcome that excluded two codes unlikely to have occurred during the same admission as the index surgery, 84.56 and 84.57 (insertion and removal of cement spacers).
Results
Of the 8,127,282 people who underwent primary TKA from 1998 to 2014, 104,366 (1.3%) had AKI (Table 1). Compared with people without AKI, patients undergoing primary TKA who had AKI were older, more likely to be male, Black, have more comorbidities, Medicare or Medicaid insurance type, lower income, or have residence in southern US (Table 1).
Demographic and other cohort characteristics of entire cohort and people with versus without AKI in those undergoing primary TKA.
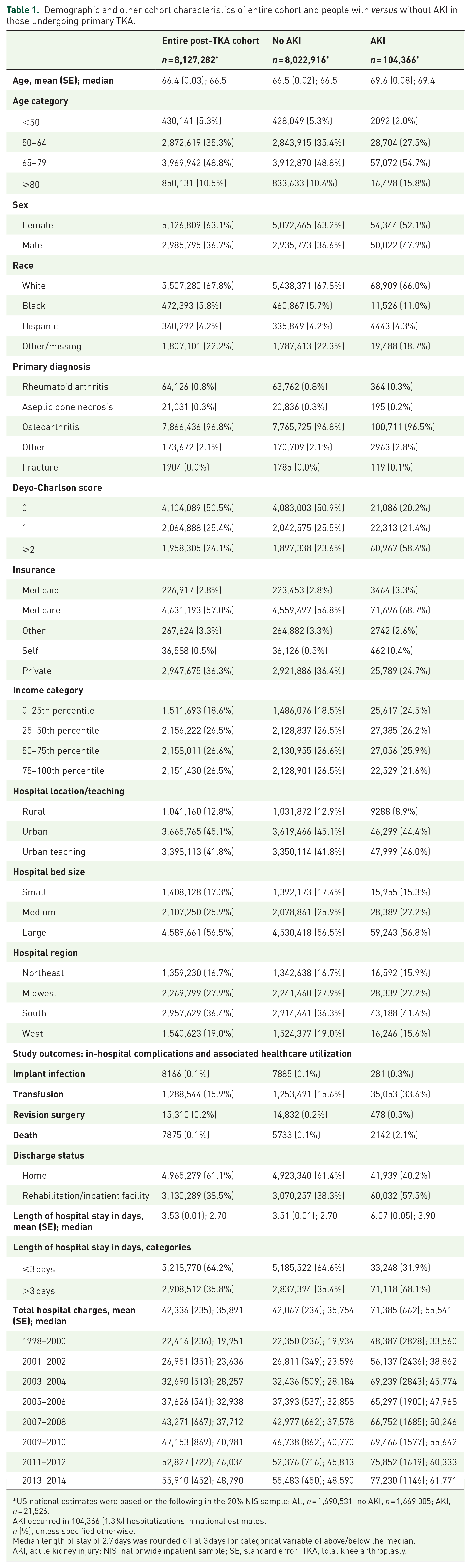
US national estimates were based on the following in the 20% NIS sample: All, n = 1,690,531; no AKI, n = 1,669,005; AKI, n = 21,526.
AKI occurred in 104,366 (1.3%) hospitalizations in national estimates.
n (%), unless specified otherwise.
Median length of stay of 2.7 days was rounded off at 3 days for categorical variable of above/below the median.
AKI, acute kidney injury; NIS, nationwide inpatient sample; SE, standard error; TKA, total knee arthroplasty.
Healthcare utilization and in-hospital complications post-TKA in patients with versus without AKI
Unadjusted
People with AKI during primary TKA hospitalization had a greater mean hospital stay of 6.1 versus 3.5 days and a higher mean (median) hospital charge of US$71,385 (median, US$55,541) versus US$42,067 (median, US$35,754) (Table 1). Compared with people without AKI for primary TKA hospitalization, mean (median) hospital stay and charges in people with AKI and primary TKA hospitalization were higher by 2.5 days (median difference, 1.2 days) and US$29,318 (median difference, US$19,787). All in-hospital postprimary TKA complication rates (including mortality) were higher in people with AKI compared with people without AKI (Table 1).
Multivariable adjusted
Adjusted for age, sex, race, underlying diagnosis, medical comorbidity, income and insurance payer, AKI during primary TKA hospitalization was associated with significantly increased OR (95% CI) of total hospital charges above the median, 2.76 (2.68, 2.85), discharge to a rehabilitation facility, 2.21 (2.14, 2.28), and the length of hospital stay above the median, 4.68 (4.54, 4.83; Table 2). AKI was also independently associated with higher odds of in-hospital infection, 2.60 (1.97, 3.43); transfusion, 2.94 (2.85, 3.03); revision, 2.13 (1.72, 2.64); and mortality, 19.75 (17.39, 22.42) post-TKA (Table 2).
Multivariable-adjusted association of AKI with in-hospital complications and healthcare utilization outcomes after primary TKA.
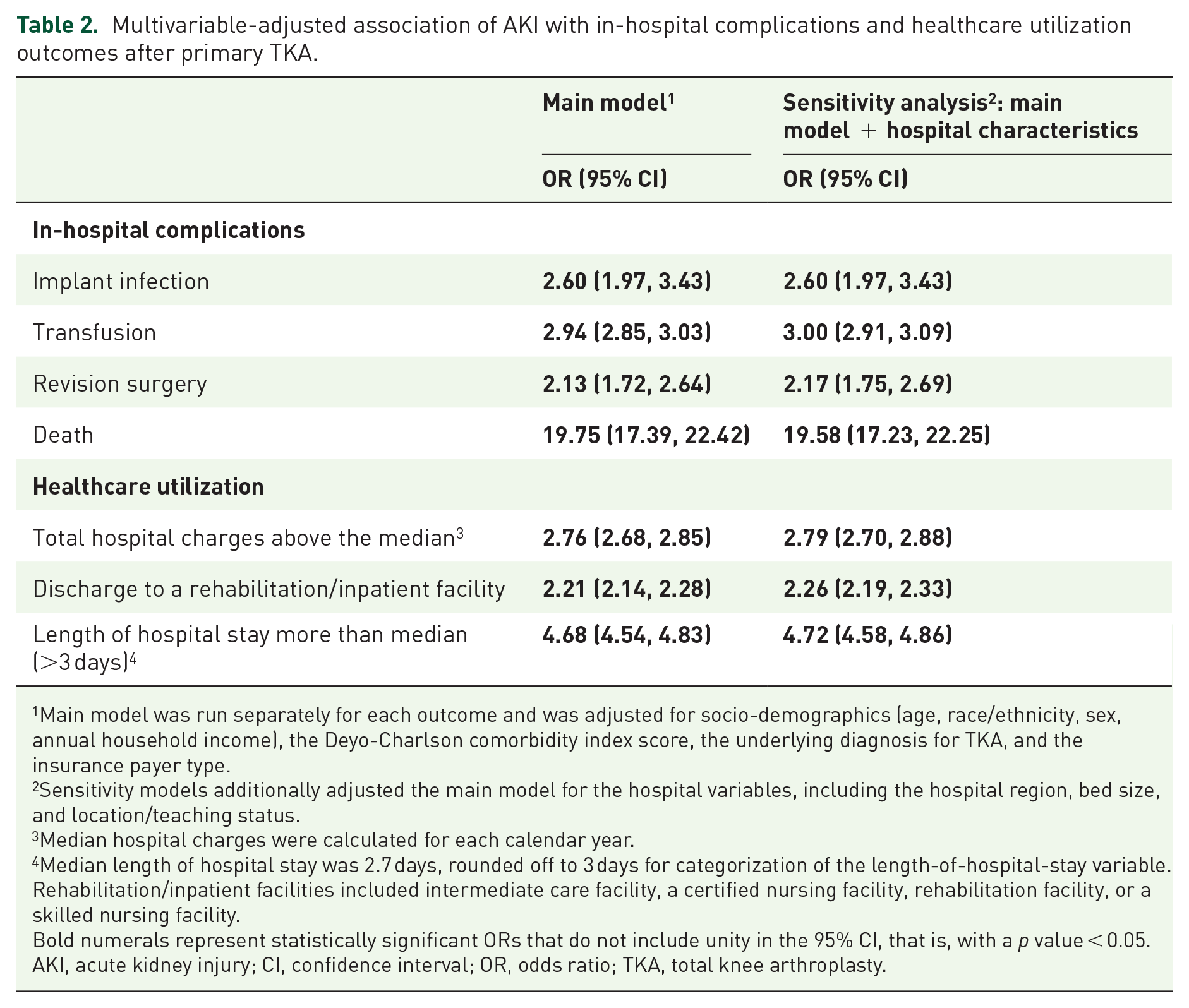
Main model was run separately for each outcome and was adjusted for socio-demographics (age, race/ethnicity, sex, annual household income), the Deyo-Charlson comorbidity index score, the underlying diagnosis for TKA, and the insurance payer type.
Sensitivity models additionally adjusted the main model for the hospital variables, including the hospital region, bed size, and location/teaching status.
Median hospital charges were calculated for each calendar year.
Median length of hospital stay was 2.7 days, rounded off to 3 days for categorization of the length-of-hospital-stay variable.
Rehabilitation/inpatient facilities included intermediate care facility, a certified nursing facility, rehabilitation facility, or a skilled nursing facility.
Bold numerals represent statistically significant ORs that do not include unity in the 95% CI, that is, with a p value < 0.05.
AKI, acute kidney injury; CI, confidence interval; OR, odds ratio; TKA, total knee arthroplasty.
Sensitivity analyses
Sensitivity analyses that additionally adjusted for hospital characteristics, including hospital location/teaching status, region, and bed size replicated the findings from the main analyses, without any attenuation of ORs (Table 2). We performed sensitivity analyses excluding two codes for revision 84.56 and 84.57 (insertion and removal of cement spacers) that were unlikely to occur during index hospitalization for primary TKA, and found that the odds ratio for revision surgery changed minimally to 2.41 (1.82, 3.19) and 2.38 (1.80, 3.16) for the main and the sensitivity model with hospital-level variables, that is, our findings from Table 2 were replicated.
Discussion
In this study, we used US NIS data from 1998 to 2014, which represents a 20% stratified sample of all US discharges. 13 We found that a diagnosis of AKI in patients who underwent primary TKA was associated with a significant increase in healthcare utilization, and in-hospital complications and mortality. Several findings in our study merit further discussion.
We found that postprimary TKA patients with AKI had significantly higher healthcare utilization, that is, a two- to threefold increase in total hospital charges above the median and total hospital stay >3 days, and a twofold higher risk of discharge of patients to a rehabilitation facility rather than home, compared with those without AKI. In a Turkish study of hip fracture surgery in the elderly, the mean hospital stay was 3 days (2–6 days) longer and the hospital charge was US$2500 higher for the patients with AKI. 18 In a Scottish study of 413 TKA/THA patients, AKI was associated with a 50% longer hospital stay 9 ; another study reported higher cost and a longer hospital stay in a combined cohort of patients with THA or TKA. 11
Our study extends these earlier findings to a primary TKA cohort. We found a 2.5-day longer hospital stay and US$29,318 higher mean total hospital charges in primary TKA hospitalizations with AKI (unadjusted estimates). We also found that multivariable-adjusted ORs for hospital charges and hospital stay above the median were increased by 2.4 and 4.7 times, respectively. Both the absolute and the relative differences noted with AKI were not only statistically significant but also clinically meaningful. This adds to the existing knowledge. We speculate that AKI may have interfered with the usual discharge planning post-TKA, due to the need for a longer observation period required for the reversal of AKI with fluid and medication management. AKI can also negatively impact the optimal early rehabilitation needed before discharge from the hospital.19,20
Discharge to a rehabilitation facility after primary TKA was 2.2-fold higher in patients with AKI. This is consistent with an odds ratio of 2.0 associated with AKI from an earlier study that used the National Hospital Discharge Survey to examine AKI-associated resource utilization in all hospitalized patients in the US. 16 AKI may lead to suboptimal post-TKA recovery and patients may need a longer inpatient physical rehabilitation. Optimization of treatment of medical comorbidities (hypertension, heart disease, diabetes) in the presence of AKI usually requires close monitoring of renal and cardiac function in an inpatient setting.
All in-hospital post-TKA complications, including infection, transfusion, and revision, were more frequent in patients with AKI versus no AKI. A two- to threefold higher risk of each complication separated these two groups, clinically and statistically significantly. A 19-fold higher risk of mortality in people with AKI highlighted the importance of preventing AKI in patients undergoing primary TKA. Optimal perioperative fluid and medication management, including antihypertensives, and avoiding nephrotoxic antibiotics and nonsteroidal anti-inflammatory drugs (NSAIDs), might help reduce AKI risk post-TKA. Implementation of an AKI care pathway triggered by an abnormal serum-creatinine value is an example of an intervention that may reduce AKI-associated morbidity and improve outcomes by early diagnosis and treatment. 21
Our study findings must be interpreted considering limitations. NIS counts discharges, not people, that is, data are not at patient level. Thus, NIS does not allow longitudinal data analysis of longer-term outcomes on a patient level, such as 30- and 90-day complications with or without readmission. These outcomes are of great interest and should be examined with other datasets that provide such data. NIS cannot account for bilateral procedures and would count them as a single procedure. Bilateral TKA procedures may be associated with more complications 22 that possibly contribute to post-TKA complications; we are unable to examine this in the NIS data. However, since a small proportion of TKA involves simultaneous bilateral procedures (<3%), 22 this introduces a minor error in our estimates and minimal confounding in our regression analyses. NIS excludes military and Veterans Affairs hospitals. Therefore, our findings cannot be generalized to people receiving healthcare at these facilities. We examined hospital charges, not actual hospital costs or what they were reimbursed, which are usually lower. Since AKI and complications both occurred during the same index hospitalization, it is possible that in some cases, complications may have occurred at the same time as the AKI or before AKI, that is, their temporal sequence cannot be determined. Our findings only show associations of AKI with TKA outcomes; these associations do not imply any causality. Finally, misclassification bias due to the use of diagnostic codes for AKI15,23 and complications is possible, but this approach of using AKI codes has a high positive-predictive value of 88%. 16 AKI was a secondary diagnosis for these index primary TKA hospitalizations, for which the primary diagnosis was the underlying arthritis. It is possible that misclassification bias is higher for AKI diagnosis, compared with the primary diagnosis for the hospitalization. Misclassification would likely bias the results toward the null, that is, it potentially makes our estimates more conservative.
Conclusion
In conclusion, we found higher healthcare utilization, in-hospital complications, and mortality in people with AKI during primary TKA hospitalization. These findings indicate that we need quality initiatives and studies of interventions to prevent AKI in patients undergoing primary TKA, so that postoperative AKI and associated morbidity can be reduced after primary TKA, an elective surgery.
Footnotes
Acknowledgements
The study was approved by the Institutional Review Board at the University of Alabama at Birmingham (UAB).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JAS is supported by the resources and the use of facilities at the VA Medical Center at Birmingham, Alabama, USA. No grant funding was obtained for this study.
Conflict of interest statement
JAS has received consultant fees from Crealta/Horizon, Medisys, Fidia, UBM LLC, Trio health, Medscape, WebMD, Clinical Care Options, ClearView Healthcare Partners, Putnam Associates, Spherix, Practice Point Communications, the National Institutes of Health, and the American College of Rheumatology. JAS owns stock options in Amarin pharmaceuticals and Viking Therapeutics. JAS is on the speaker’s bureau of Simply Speaking. JAS is a member of the executive of OMERACT, an organization that develops outcome measures in rheumatology and receives arms-length funding from 12 companies. JAS serves on the US Food and Drug Administration Arthritis Advisory Committee. JAS is a member of the Veterans Affairs Rheumatology Field Advisory Committee. JAS is the editor and the director of the UAB Cochrane Musculoskeletal Group Satellite Center on Network Meta-analysis. JAS previously served as a member of the following committees: member, the American College of Rheumatology’s (ACR) Annual Meeting Planning Committee (AMPC) and Quality of Care Committees, the Chair of the ACR Meet the Professor, Workshop and Study Group Subcommittee and the co-chair of the ACR Criteria and Response Criteria subcommittee. JDC has no conflicts.