
Abstract
Background:
The phase III TALAPRO-2 trial established that combining talazoparib (TALA) with enzalutamide significantly extends progression-free survival (PFS) and overall survival in metastatic castration-resistant prostate cancer (mCRPC) patients. Given the substantial cost implications of novel targeted therapies, economic evaluation is essential to determine whether the clinical benefits of this regimen justify its expense in the first-line mCRPC setting.
Objectives:
To evaluate the cost-effectiveness of talazoparib plus enzalutamide versus enzalutamide monotherapy as first-line treatment for mCRPC, informing clinical decision-making and healthcare resource allocation.
Design:
A Markov model-based cost-effectiveness analysis.
Methods:
Based on data from the TALAPRO-2 trial, a dynamic Markov model was constructed to simulate disease progression in mCRPC patients. From the perspectives of U.S. and Chinese payers, total costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratios (ICER) were considered as the primary outputs in the model. One-way sensitivity analysis and probabilistic sensitivity analysis were used to validate the robustness of the model. Price reduction analysis provided an evidence-based basis for drug pricing and health insurance negotiations by quantifying the impact of price adjustments on economics.
Results:
In the base-case analysis, the ICERs for talazoparib plus enzalutamide were $646,743.72/QALY and $57,635.76/QALY from the U.S. and China perspectives, respectively, which were above the willingness-to-pay thresholds ($150,000 in the U.S. and $40,334 in China). Sensitivity analyses showed that the utility of PFS and drug prices impacted the results most. Price adjustment scenarios showed that China needed a 34.5% price reduction to achieve affordability, whereas the U.S. remained unaffordable even with an 80% price reduction.
Conclusion:
At current pricing, talazoparib plus enzalutamide as first-line treatment of patients with mCRPC is not cost-effective in either the U.S. or China. The study supports differentiated pricing strategies to balance clinical benefits with the rational allocation of healthcare resources.
Keywords
Introduction
Accounting for nearly one-tenth of cancer mortality in American men, prostate cancer represents the second leading cause of male cancer incidence nationwide. 1 This mortality burden is primarily attributed to its high propensity for bone metastasis and the eventual failure of hormonal therapies. The proliferation of early-stage prostate cancer critically depends on androgen receptor (AR) signaling and its ligand testosterone, which has prompted the development of therapeutic strategies targeting both androgen biosynthesis and AR-mediated oncogenic pathways. Androgen deprivation therapy (ADT), encompassing surgical castration and pharmacologic approaches, aims to suppress systemic androgen synthesis. However, all patients exhibit disease progression post-ADT through AR overexpression that sustains tumor growth in low-testosterone environments,2,3 leading to metastatic castration-resistant prostate cancer (mCRPC). To address this, second-generation AR competitive inhibitors, including enzalutamide, apalutamide, 4 and darolutamide 5 and androgen precursor synthesis inhibitors such as abiraterone acetate have been employed in mCRPC management, demonstrating significant clinical benefits in multiple phase III trials.6,7
Nearly a quarter of individuals diagnosed with prostate cancer present with genetic alterations in DNA damage repair (DDR) pathways, predominantly involving homologous recombination repair (HRR)-associated genes. 8 The HRR pathway encompasses multiple members, including ATM, CHEK2, and BRCA1/2. An observational study demonstrated that patients with HRR mutations (HRRm) exhibited shorter overall survival (OS) and differential therapeutic responses to identical treatment modalities compared to non-HRRm counterparts. 9 Consequently, ctDNA genomic profiling to delineate molecular characteristics enables optimized therapeutic decision-making and prognostic evaluation. 10 Poly(ADP-ribose) polymerase (PARP), a critical enzyme in DDR, demonstrates enhanced activity mediated by AR inhibition during ADT, concomitant with downregulation of HRR gene expression. Given the high prevalence of HRR deficiency in metastatic mCRPC, PARP inhibitors (PARPi) exert synthetic lethality by impairing DNA repair mechanisms, particularly when combined with ADT, thereby conferring survival benefits in advanced mCRPC. However, clinical responses to PARPi are heterogeneous and strongly influenced by the specific HRR gene affected. While BRCA1/2 mutations predict robust sensitivity and significant survival benefits, mutations in genes such as ATM are associated with diminished efficacy, 11 and CDK12 mutations exhibit a spectrum of responses to PARPi, dependent on the mutational burden and residual functional impact. 12 Consequently, optimal patient selection requires consideration of the specific genetic lesion beyond a broad “HRR-deficient” classification. Recent phase III trials, including PROfound and PROpel, established that olaparib combined with abiraterone significantly prolongs progression-free survival (PFS) and OS across all study populations, with enhanced clinical benefits observed in HRRm and BRCA1/2-mutated cohorts. This regimen has been endorsed as a Category 1A recommendation for mCRPC treatment in the 2024 American Society of Clinical Oncology (ASCO) guidelines. Subgroup analyses revealed striking efficacy differences: HRRm subgroups achieved rPFS hazard ratio (HR) = 0.66 versus HR = 0.89 in non-HRRm groups, with BRCA1/2-mutated cohorts demonstrating HR = 0.29. These findings were corroborated in the PROfound cohort.13,14 Olaparib and rucaparib have received U.S. and European approval as first-line therapies for mCRPC patients with BRAC1/2 mutations.13,15 A majority of experts’ consensus strongly supports PARPi combination therapy with AR pathway inhibitors in BRCA1/2-altered patients, while demonstrating overwhelming opposition to PARPi use in DDR-intact mCRPC cases. Current treatment algorithms recommend referencing metastatic hormone-sensitive prostate cancer (mHSPC) therapeutic paradigms for DDR-wildtype mCRPC management. 16
In 2018, talazoparib (TALA) received FDA approval for prostate cancer treatment and was subsequently designated as a first-line therapeutic agent for mCRPC by the Chinese Society of Clinical Oncology (CSCO) guidelines in 2020. The phase III TALAPRO-2 trial demonstrated that talazoparib plus enzalutamide significantly improved PFS and OS across the entire study population, achieving a 37% reduction in risk of disease progression or death (HR = 0.62; 95% confidence interval: 0.475–0.814). Subgroup analyses stratified by HRR gene mutation status revealed substantial therapeutic heterogeneity: the talazoparib plus enzalutamide cohort with HRRm exhibited median OS not reached after 52.5 months of follow-up, compared to 42.4 months in non-HRRm patients receiving the same combination. This underscores the critical impact of HRR mutational status on clinical outcomes with talazoparib-based therapy. Notably, this study provides pivotal evidence that HRRm profiling constitutes a more robust predictor of therapeutic responsiveness to PARPi-ADT combination regimens than BRCA1/2 mutation status alone (ASCO GU; February 13–15, 2025).
Although the combination therapy of talazoparib and enzalutamide has demonstrated clinical efficacy in the TALAPRO-2 trial, its high cost compared to other PARPi 17 raises uncertainties regarding the cost-effectiveness of global implementation, particularly in middle-income countries where its potential to improve quality of life for mCRPC patients remains unverified. To optimize healthcare resource allocation, identify high-benefit patient subgroups, enhance scientific decision-making in treatment strategies and drug pricing, and balance multi-stakeholder interests, this study evaluated the cost-effectiveness of talazoparib plus enzalutamide versus enzalutamide monotherapy from the perspectives of U.S. and Chinese healthcare payers.
Materials and methods
Population and intervention
This research strictly adhered to the updated Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS 2022). Detailed compliance with each checklist item is provided in Table S1. Based on the TALAPRO-2 clinical trial, the model simulated mCRPC patients aged 70 years (the median age of the clinical trial population) who had received continuous castration therapy (testosterone ⩽50 ng/dL) with ongoing ADT, presented radiologically confirmed bone or soft tissue metastases, and exhibited asymptomatic or mildly symptomatic disease. The target patient population was randomly assigned 1:1 to either the TALA arm or the placebo (PBO) group. The TALA arm received two 0.25 mg talazoparib capsules administered orally once daily plus four 40 mg enzalutamide capsules daily, while the PBO arm received two matching placebo capsules daily alongside four 40 mg enzalutamide capsules. Upon radiographically confirmed disease progression, second-line therapeutic regimens from the TALAPRO-2 were initiated, with remaining progressive cases receiving best supportive care (BSC). Monitoring protocols followed the TALAPRO-2 study design during the initial 56 weeks of follow-up, transitioning thereafter to surveillance strategies recommended by the CSCO guidelines. Patients continued treatment until death, adverse event (AE)-induced discontinuation, or study endpoint attainment.
Model construction
This study employed a dynamic Markov model constructed using TreeAge Pro 2022 software (TreeAge, Williamstown, MA, USA) to evaluate the cost-effectiveness of talazoparib plus enzalutamide in treating mCRPC. Within the modeling framework, patients could transition between three mutually exclusive states: PFS, progressive disease (PD), and the absorbing state of death. As per model specifications, the initial health state for the entire cohort was defined as PFS and could transition between these states during disease progression (Figure 1). A 28-day cycle length was implemented to align with TALAPRO-2 treatment intervals, with a 30-year time horizon to ensure that more than 99% of patients enter the death state.

The structure of the decision tree (a) and the Markov state transition model (b).
The economic evaluation focused on three primary outcomes: total costs, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratio (ICER). All cost and utility estimates underwent 3% and 5% annual discounting in the U.S. and China, with half-cycle correction. Following the 2020 China Guidelines for Pharmacoeconomic Evaluations, 18 willingness-to-pay (WTP) thresholds were set at $40,334/QALY (3× China’s 2024 per capita GDP) for China and $150,000/QALY for the U.S. 19
Clinical data
Given the unavailability of original individual patient data (IPD), OS and PFS estimates for the mCRPC cohort were derived from Kaplan-Meier curves published in the TALAPRO-2 trial. For quantitative analysis of published survival data, the GetData Graph Digitizer software (Version 2.26, S. Fedorov, Moscow, Russia) was employed to extract data points from both OS and PFS curves, and R software (Version 4.3.2, R Foundation for Statistical Computing, Vienna, Austria) was used to reconstruct IPD. Based on Guyot et al.’s
20
algorithm, Exponential, Weibull, Log-logistic, Log-normal, and Gompertz standard parametric survival functions were subsequently employed to fit and extrapolate survival curves. The final model selection was determined through a comprehensive evaluation incorporating Akaike Information Criterion, Bayesian Information Criterion statistical criteria, and visual inspection for clinical plausibility (Table S2 and Figure S1). The optimal distributions for OS and PFS survival curves were Log-logistic
Transition probability
The disease progression dynamics in mCRPC patients were simulated using transition probability modeling, which incorporated the method of Latime
21
to calculate time-dependent transition probabilities between distinct health states within a Markov model. The transition probability from PFS to death was assumed to be the natural mortality. Based on OS and PFS survival functions, the specific-cycle transition probability between states was calculated using the following formula:
Cost and utility
This study adopted the perspectives of third-party payers in China and the U.S., considering only direct medical costs, which included drug costs, examination costs, follow-up costs, hospice care costs, BSC, and the treatment costs of the top 5 severe AEs (grade ⩾3; Table 1). The price adjustments were made using the consumer price index to reflect inflation, and all costs were adjusted to the 2025 U.S. dollars according to the formula from https://www.inflationtool.com. Since second-line treatments such as cabazitaxel and docetaxel require dosing based on patient body surface area, we assumed the average weight of U.S. and Chinese patients to be 70 and 65 kg, respectively, to calculate dosing and costs, which were then incorporated into the sensitivity analysis. As Lutetium was not yet available in China, its cost in China was estimated by multiplying the U.S. cost by the ratio of talazoparib costs in China and the U.S. Other costs were obtained from local tertiary hospital fee standards, published literature, and relevant websites, and all second-line treatment costs were weighted before being input into the model (Table 2).
Clinical outcomes for each cohort.

AEs, adverse events; BSC, best supportive care.
Cost-related parameters in the U.S. and China.

Since Lutetium is not approved in China, its cost in the Chinese context was estimated based on the U.S. market price, with the cost conversion ratio referenced to the price differential of talazoparib between China and the United States.
AE, adverse event; BSC, best supportive care; CT, computed tomography; PSA, prostate-specific antigen; SA, sensitivity analysis.
Utility values, ranging between 0 and 1, measured quality of life of patients and indirectly reflect the benefits of medical interventions. Since utility values for PFS and PD states were not reported in the TALAPRO-2 trial, the PFS utility value adopted in this study was drawn from a meta-analysis of prostate cancer utilities, 32 while the PD utility values were sourced from a cost-effectiveness study. 33 The utility decrements due to AEs include only the disutility values of the top 5 AEs with grade ⩾3 severity (Table 3).
Utility in model.

SA, sensitivity analysis.
Sensitivity analysis
We used one-way sensitivity analysis (OWSA) and probabilistic sensitivity analysis (PSA) to explore the impact of each variable input into the model on the ICER. In the OWSA, the low and high values of each variable were determined by ±20% of the baseline value, with the high value of the discount rate set at 0.8 and the low value at 0. The results of the OWSA were presented using a tornado diagram. In addition, we conducted 10,000 Monte Carlo simulations for the PSA, assuming that the costs in the model followed a Gamma distribution, while utility and probability parameters followed a Beta distribution. The results of the PSA were presented in the form of incremental cost-effectiveness scatter plots and cost-effectiveness acceptability curves.
Scenario analysis
To further explore the cost-effectiveness of talazoparib plus enzalutamide in the treatment of mCRPC, we conducted a price reduction simulation for talazoparib, assuming price reductions of 20%, 40%, 60%, and 80%, respectively. The analysis compared changes in the ICER and the probability of cost-effectiveness acceptability.
Results
Base-case analysis
The results of the cost-effectiveness analysis showed that from the Chinese perspective, the total cost of treatment with talazoparib in combination with enzalutamide for mCRPC patients was $97,286, which amounted to an incremental cost of $53,537 compared to the total cost of $43,748 for treatment with enzalutamide. Compared to the enzalutamide-treated group that averaged or gained 2.25 QALYs, the talazoparib in combination with enzalutamide group could gain an additional 0.93 QALYs with an ICER of $57,635.76/QALY, which was greater than the Chinese payer WTP, suggesting that talazoparib in combination with enzalutamide was not cost-effective in China. From a U.S. perspective, the talazoparib plus enzalutamide combination yielded an incremental cost of $708,234 with an incremental effectiveness of 1.10 QALYs, resulting in an ICER of $646,743.72/QALY gained. This ICER exceeded the U.S. WTP threshold of $150,000/QALY and was therefore not considered cost-effective in the U.S. setting (Table 4).
Result of base-case analysis.

ENZA, enzalutamide; IC, incremental cost; ICER, incremental cost-effectiveness ratio; IE, incremental effectiveness; PBO, placebo; QALYs, quality-adjusted life years; TALA, talazoparib.
Sensitivity analysis
OWSA showed that the most influential parameter on ICER in both the U.S. and Chinese perspectives was the utility of PFS. Of the remaining parameters entered into the model, those that had a remarkable impact on the ICER values were the unit price of talazoparib, the unit price of enzalutamide, and the utility of PD. Changes in other variables had less impact on the stability of the model, showing that the model is stable and the conclusions of this study are reliable; all parameters within the range of changes cannot make the ICER value lower than the WTP (Figure 2). The scatter plots demonstrated that all scatters fall above the WTP line (Figures 3 and 4) that is, none of the treatment of talazoparib in combination with enzalutamide is economical compared with enzalutamide alone, the probability of cost-effectiveness was 1.33% at a WTP threshold of $40,334/QALY in China, in contrast to 0% at a WTP threshold of $150,000/QALY in the U.S.
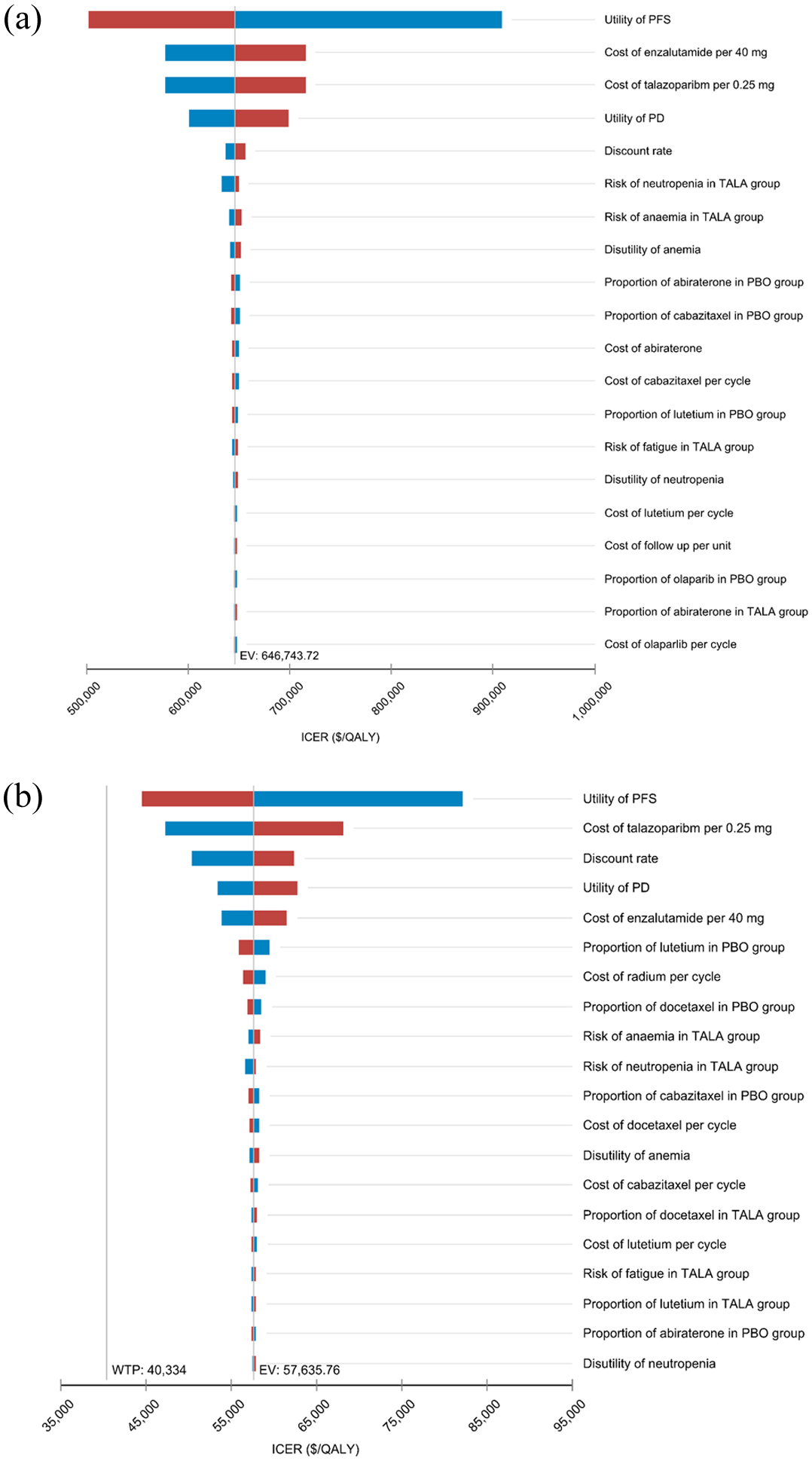
Tornado diagram of one-way sensitivity analysis of the talazoparib plus enzalutamide compared to placebo plus enzalutamide in the U.S. (a) and China (b).
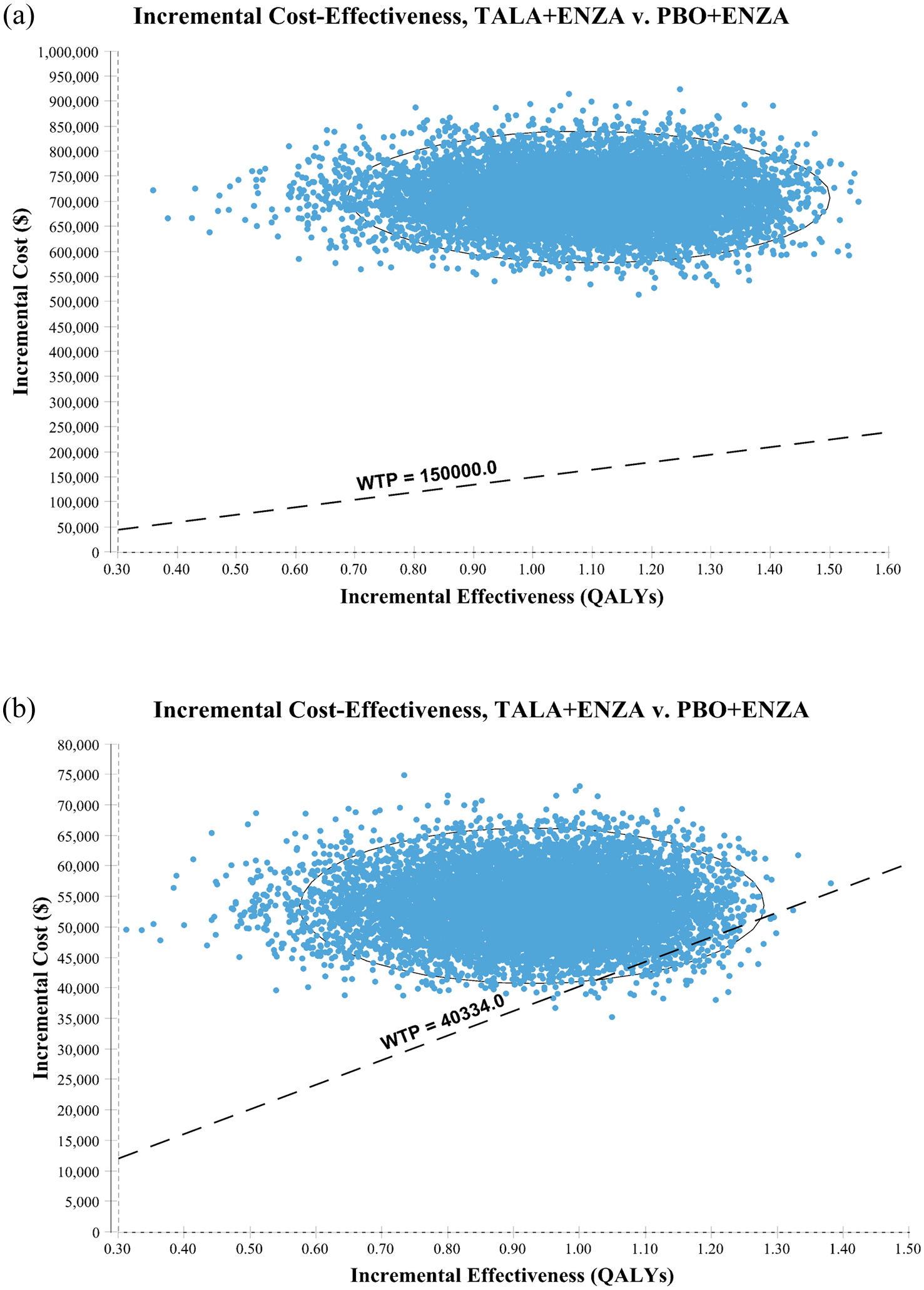
Incremental cost-effectiveness scatter plot of the talazoparib plus enzalutamide compared to placebo plus enzalutamide in the U.S. (a) and China (b).
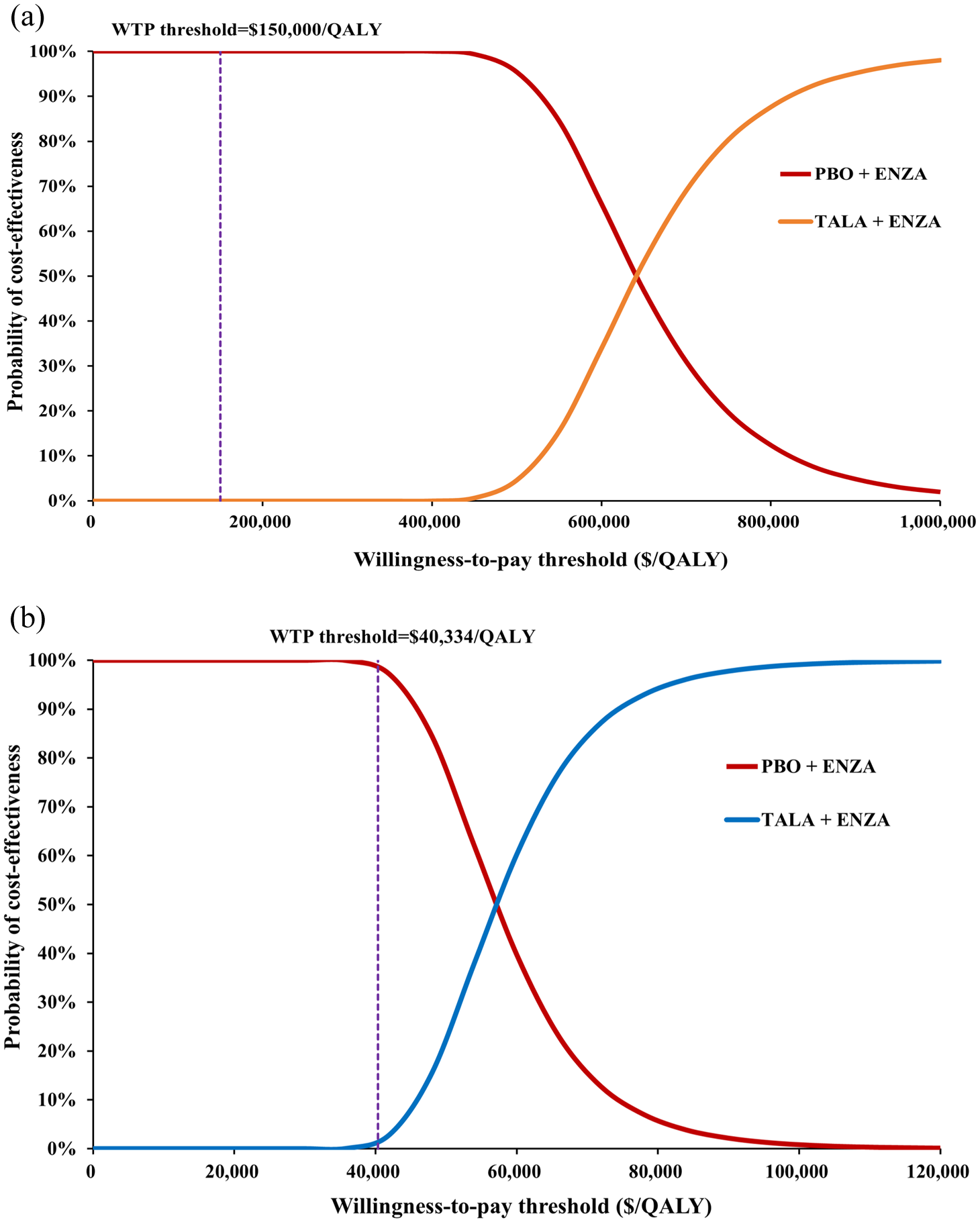
Cost-effectiveness acceptability curves of the talazoparib plus enzalutamide compared to placebo plus enzalutamide in the U.S. (a) and China (b).
Scenario analysis
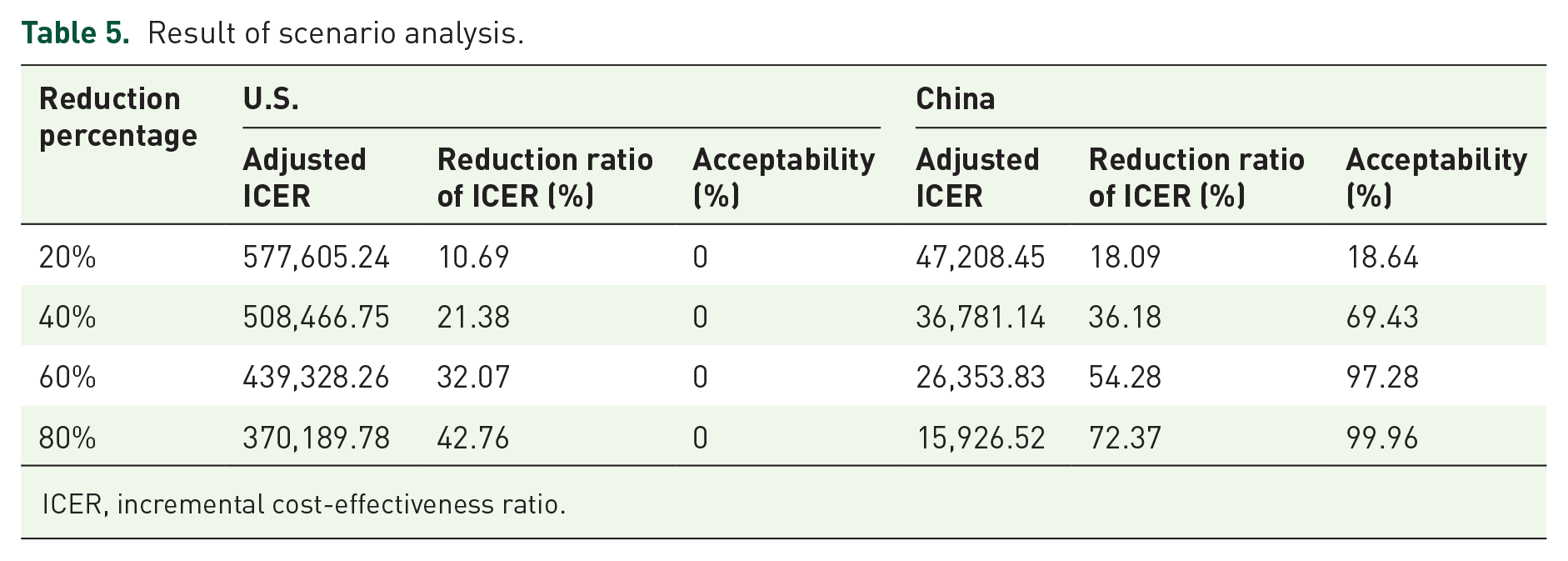
After doing 20%, 40%, 60%, and 80% price reductions for talazoparib 0.25 mg unit price, it was found that the talazoparib plus enzalutamide group demonstrated economy with an acceptable probability of 64.87% for the Chinese payer perspective, with a price reduction ratio of 40%. For the U.S. payer perspective, on the other hand, even with a price reduction percentage of 80%, talazoparib remained not cost-effective. Further study found that in the Chinese payer perspective, the talazoparib plus enzalutamide group had a greater than 50% likelihood of being cost-effective, showed higher economic benefits than the placebo group when the price reduction percentage reached 34.5% (Table 5 and Figure 5).
Result of scenario analysis.
ICER, incremental cost-effectiveness ratio.
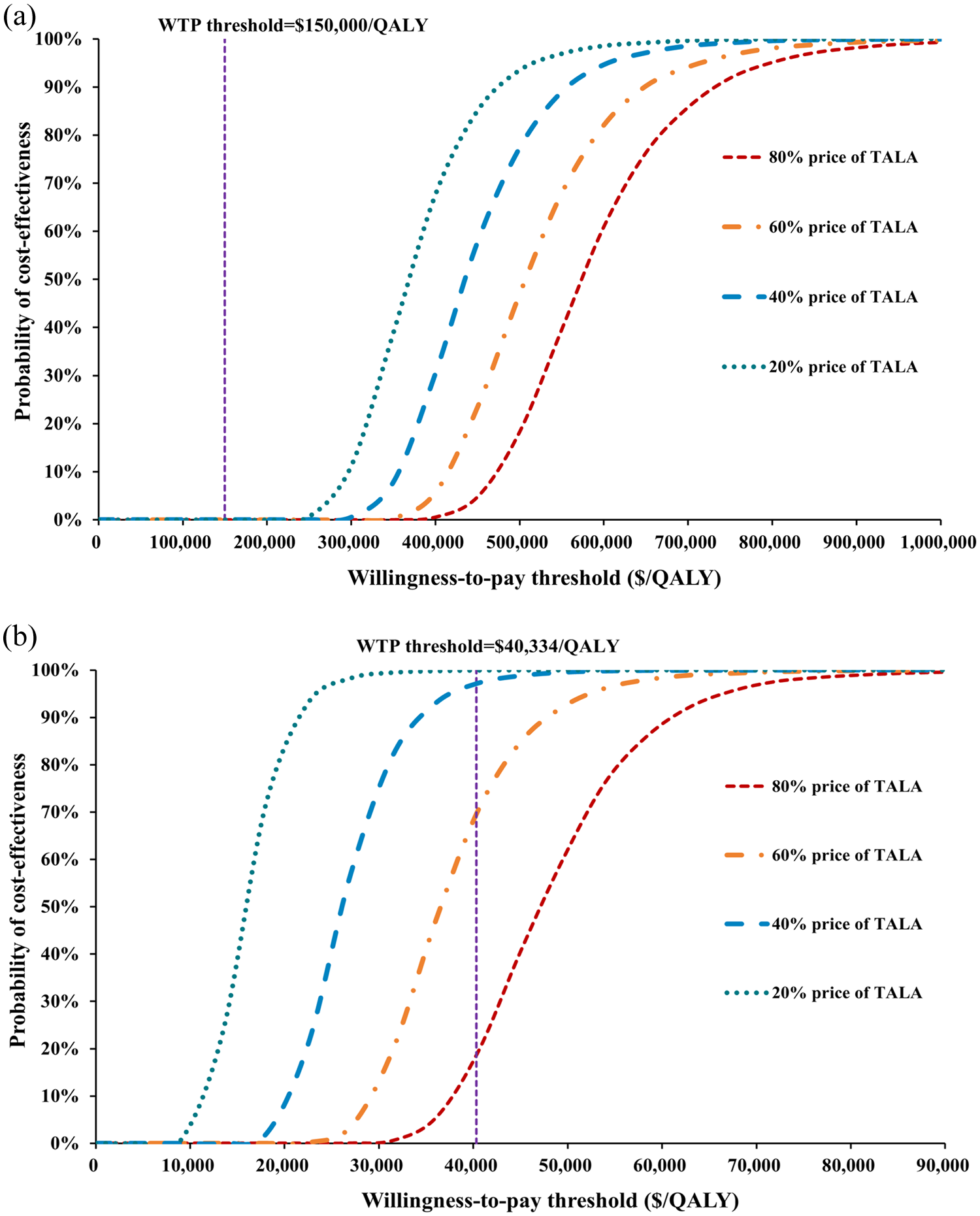
Cost-effectiveness acceptability curves for talazoparib under progressive price reductions in the U.S. (a) and China (b).
Discussion
Prostate cancer is a malignancy with a persistently high incidence in males. In the natural history of advanced HSPC, virtually all patients treated with ADT will eventually develop CRPC, indicating that the tumor acquires the ability to continue progressing despite castrate levels of serum testosterone (<50 ng/dL). The HRR gene-deficient cells experience a functional impairment in their DNA double-strand break repair mechanisms. 35 Since the proposal of the concept that PARPi induce synthetic lethality in HRR-deficient tumor cells by blocking the backup DNA repair pathway 36 first-generation PARPi such as olaparib and talazoparib have been developed and entered clinical trials. The TALAPRO-2 trial investigated the clinical significance of talazoparib plus enzalutamide in mCRPC populations. Results showed that talazoparib extended patient OS by 14 months and PFS by 18.4 months. In January 2024, the European Commission granted regulatory approval for the talazoparib-enzalutamide combination therapy in the management of mCRPC without clinical indications for chemotherapy, marking the first PARPi regimen certified by the European Commission. A network meta-analysis indicated that, compared with other PARPi combined with AR signaling inhibitor therapies, talazoparib plus enzalutamide holds the greatest potential to prolong PFS, thereby reducing the need for second-line treatments. 37 It is noteworthy that the exclusion of genetic testing costs in our model stems from fundamental differences between the TALAPRO-2 and PROpel trials. Whereas PROpel exclusively enrolled HRR-altered patients, making testing costs inherent to its intervention, 14 TALAPRO-2 demonstrated efficacy in an unselected population without biomarker pre-screening. 38 Consequently, our analysis reflects the drug’s label-agnostic implementation context, where testing remains discretionary. This approach aligns with health economic evaluation standards for interventions approved in overall populations.
However, the high cost of talazoparib limits its economic viability and clinical application. This investigation represents, to our knowledge, the inaugural economic evaluation of talazoparib-enzalutamide combination therapy as a first-line treatment for mCRPC, incorporating both Chinese and U.S. healthcare perspectives. From the Chinese and U.S. perspectives, the cost of talazoparib plus enzalutamide significantly exceeded that of enzalutamide monotherapy, with incremental costs per additional QALYs gained reaching $57,635.76 and $646,743.72, respectively, both surpassing our predefined WTP thresholds. Consequently, the combination therapy lacks economic feasibility in both countries.
OWSA revealed that key drivers of ICER in both contexts were utility values of PFS, drug prices of talazoparib and enzalutamide. Given the pronounced influence of PFS utility values on ICER, wherein increased PFS drives significant ICER reduction, this suggests that selecting patients with HRR gene mutations for talazoparib plus enzalutamide therapy could extend PFS duration, thereby increasing QALYs and reducing ICER. This supports the necessity of HRR gene testing at diagnosis.
Price reduction simulations for talazoparib demonstrated that a 20% price cut in China reduced ICER to $47,208.45/QALY, increasing cost-effectiveness acceptability probability from <1% to 15%, indicating that moderate price adjustments could substantially improve economic viability—a finding particularly relevant given talazoparib’s high pricing in China. At a 40% price reduction, the combination therapy demonstrated superior cost-effectiveness versus enzalutamide monotherapy. Further analysis showed that a 34.5% price reduction achieved a 50% cost-effectiveness probability. In China, drug pricing is closely tied to national medical insurance inclusion, and future centralized procurement/price negotiations could reasonably bring ICER within acceptable ranges. From the U.S. perspective, we found that even with an 80% price reduction for talazoparib, the benefit of gaining one additional QALY when the WTP is $150,000/QALY still does not cover the incremental cost of $370,189.78. And for every 20% price reduction of talazoparib, the ICER value was only reduced by 10.69%, suggesting that the high cost of other adverse effect management and second-line treatment is also one of the reasons why talazoparib in combination with enzalutamide does not show economic value. On the one hand, the U.S. has a high degree of drug marketization, and the price of PARPi drugs such as talazoparib fluctuates with patent expiration and extensive development of PARPi; on the other hand, PARPi have shown clinical benefits in malignant tumors such as breast cancer 39 the expansion of market capacity may lead to increased competition in the market, further driving the price of talazoparib back down. Currently, the higher price of talazoparib is not reflective of its true value to U.S. payers, and we expect that talazoparib will achieve efficacy-based pricing to reduce payer risk. The sensitivity of the model to talazoparib demonstrates that there are price distortions in the current price of talazoparib, likely due to patent protection and market monopoly, and that reasonable price reductions and differentiated pricing based on regional levels of development could correct the price distortions and improve the economics of talazoparib in combination with enzalutamide.
Data from the TALAPRO-2 trial showed that the combination therapy reduced the risk of progression of the disease by 37% but the price would need to be commensurate with the health benefit to maximize its health-promoting effect. Fortunately, Pfizer runs a patient assistance program that makes lower-cost treatment with talazoparib available to some low- and middle-income populations. The PROpel trial, conducted concurrently with TALAPRO-2, explored the clinical efficacy of olaparib in combination with abiraterone in patients with mCRPC. Olaparib, as approved by the FDA as a treatment for mCRPC patients with BRCA mutations, 40 shows very different results in the study of Xu et al. 22 They found that olaparib in combination with abiraterone was also not economical in China, which is consistent with our opinion, whereas in the U.S. perspective, the cost of the olaparib plus abiraterone treatment group was instead decreased by $69,675.20 compared to the control group and higher utility values were obtained (incremental effectiveness = 0.23 QALY), which is undoubtedly economical in the U.S. perspective. There are several reasons for this difference. (1) Olaparib costs $17,313.88 for a treatment cycle in the U.S. market after discounting to 2025 dollars, which is only 60% of the cost of talazoparib over a treatment cycle, making it more economical; (2) Xu et al.’s data were derived from the PROfound cohort, 13 which exclusively enrolled mCRPC patients with BRCA1/2 or ATM defects. In contrast, the TALAPRO-2 cohort included an all-comer population regardless of HRR gene mutation status. Our study simulated the cost-effectiveness of talazoparib plus enzalutamide in this unselected population, where the incremental benefits were understandably lower than in populations with PARPi-targetable genetic alterations. This indirectly indicates that while olaparib demonstrates better economic viability in the U.S., its target population is narrower than talazoparib’s. The cost-effectiveness of olaparib in genetically unselected broad populations remains uncertain. (3) The PROfound trial reported substantially fewer AEs than the TALAPRO-2 trial. In the olaparib-abiraterone treatment arm, the incidence of grade ⩾3 overall AEs and grade ⩾3 anemia was 51% and 21%, respectively, compared to 75% and 46% in the talazoparib plus enzalutamide arm. Combined with the 19-fold higher cost of AEs management per treatment cycle in the U.S. versus China, these factors led to lower total costs for olaparib plus abiraterone therapy. Consequently, its ICER against the comparator was more favorable, thereby demonstrating economic viability. Teppala et al. 41 conducted a cost-effectiveness analysis of olaparib combined with abiraterone for BRCA1/2-mutated mCRPC patients from an Australian perspective. The results showed an incremental cost of $4,884.141 for an additional 0.06 QALYs, yielding an ICER of $91,138/QALY. At Australia’s defined WTP threshold of $62,289.772, this regimen was not cost-effective. Price reduction analysis revealed that a 30% reduction in olaparib’s monotherapy price was required to achieve >50% probability of cost-effectiveness acceptability for the olaparib plus enzalutamide. In conclusion, both talazoparib plus enzalutamide and olaparib plus abiraterone are FDA-approved for mCRPC treatment. While olaparib plus abiraterone demonstrates superior economic viability in the U.S., this advantage comes at the expense of biomarker dependency and reduced generalizability to unselected patient cohorts. Conversely, although talazoparib plus enzalutamide lacks initial cost-effectiveness in both Chinese and U.S. healthcare systems prior to price adjustments, it exhibits robust clinical benefits across broad, unselected populations. With rational price reductions, the combination achieves cost-effectiveness within acceptable thresholds, positioning it as a promising first-line therapy for mCRPC. It is worth noting that our findings should consider current treatment trends. As most mHSPC patients now receive ARPIs as first-line therapy, fewer patients progress to mCRPC without prior ARPI exposure. This shrinking eligible population poses real-world challenges for talazoparib plus enzalutamide implementation, despite its efficacy in ARPI-naïve settings. Future trials should test this combination in ARPI-pretreated patients or earlier disease stages.
Limitation
This study has some limitations in evaluating the cost-effectiveness of talazoparib plus enzalutamide from U.S. and Chinese perspectives. First, the utility values lack localization for China. The Chinese model referenced utility values derived from the QQL questionnaire administered to the U.S. population, 33 which introduces potential cultural bias due to differences in health preference weights between American and Chinese societies. Although we conducted OWSA on utility values, these addressed random variations rather than systematic cultural differences. We were unable to perform scenario analyses quantifying cultural preference heterogeneity due to the absence of Chinese-specific utility benchmarks. To address potential cultural bias, future studies should incorporate locally validated instruments such as EQ-5D-5L in Chinese cohorts or conduct sensitivity analyses reflecting cultural preference heterogeneity. Second, subgroup analyses have not been performed as survival curves from the TALAPRO-2 trial have not been fully published; however, published cost-effectiveness analyses of PARPi 42 and survival data from TALAPRO-2 suggest a greater likelihood of economic benefit of TALA for the HRRm+ population, and therefore, further analysis is required to validate this when data are refined. However, patient access to genetic testing faces practical barriers worldwide, with only 37% of mCRPC patients undergoing testing due to tissue availability constraints and limited clinical utility until recently. On the other hand, the high cost of genetic testing may also make talazoparib plus enzalutamide less economical. Apart from this, indirect treatment comparisons and network meta-analyses between talazoparib plus enzalutamide, olaparib plus abiraterone/prednisolone, and other PARPi were precluded due to disconnected evidence networks, unresolved population heterogeneity in BRCA-positive subgroups, and critical gaps in published baseline characteristics and outcome data. 37 Lastly, while China’s WTP threshold was set at three times the national per capita GDP, regional economic disparities were not considered. In high-income cities such as Shanghai, Beijing, and Shenzhen, elevated local payment capacities might render the talazoparib plus enzalutamide regimen cost-effective at subnational thresholds. Despite these limitations, we believe that this study can evaluate clinical treatment options for patients with mCRPC.
Conclusion
In conclusion, due to the high cost of talazoparib, the regimen of talazoparib plus enzalutamide did not show economic value for the treatment of mCRPC from the perspectives of healthcare payers in the United States or China at the WTP threshold. To improve its economy, it is recommended to achieve a price reduction for talazoparib. For mCRPC patients not harboring HRRm, ARPI monotherapy (e.g., abiraterone plus prednisone) remains the standard first-line regimen, but there are many combinations of further systemic therapies in development. Although specific clinical applications require validation, some studies suggest that combinations with other systemic agents may provide additional benefit,43–46 and numerous novel therapeutic strategies are currently under active investigation.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251367329 – Supplemental material for Cost-effectiveness of talazoparib plus enzalutamide as first-line therapy in metastatic castration-resistant prostate cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359251367329 for Cost-effectiveness of talazoparib plus enzalutamide as first-line therapy in metastatic castration-resistant prostate cancer by Jiaming Zhu, Zhengxiong Li, Ye Ding and Qiaoping Xu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-png-2-tam-10.1177_17588359251367329 – Supplemental material for Cost-effectiveness of talazoparib plus enzalutamide as first-line therapy in metastatic castration-resistant prostate cancer
Supplemental material, sj-png-2-tam-10.1177_17588359251367329 for Cost-effectiveness of talazoparib plus enzalutamide as first-line therapy in metastatic castration-resistant prostate cancer by Jiaming Zhu, Zhengxiong Li, Ye Ding and Qiaoping Xu in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-png-3-tam-10.1177_17588359251367329 – Supplemental material for Cost-effectiveness of talazoparib plus enzalutamide as first-line therapy in metastatic castration-resistant prostate cancer
Supplemental material, sj-png-3-tam-10.1177_17588359251367329 for Cost-effectiveness of talazoparib plus enzalutamide as first-line therapy in metastatic castration-resistant prostate cancer by Jiaming Zhu, Zhengxiong Li, Ye Ding and Qiaoping Xu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.