
Abstract
Background:
Androgen receptor signaling inhibitors (ARSis) abiraterone acetate (AA) plus prednisone and enzalutamide (Enza), are currently the most administered first-line treatments for metastatic castration-resistant prostate cancer (mCRPC). AA and Enza have shown similar overall survival (OS) benefits and there is no consensus upon the best option for mCRPC first-line treatment. Volume of disease may represent a useful biomarker to predict response to therapy in such patients.
Objectives:
In this study, we seek to evaluate the impact of volume of disease on patients treated with first-line AA versus Enza for mCRPC.
Design and methods:
We retrospectively evaluated a cohort of consecutive patients with mCRPC categorized by volume of disease [high volume (HV) or low volume (LV) per E3805 criteria] at ARSi onset and treatment type (AA or Enza), assessing OS and radiographic progression-free survival (rPFS), from therapy start, as co-primary endpoints.
Results:
Of the 420 patients selected, 170 (40.5%) had LV and received AA (LV/AA), 76 (18.1%) LV and had Enza (LV/Enza), 124 (29.5%) HV and were given AA (HV/AA), and 50 (11.9%) HV and received Enza (HV/Enza). Among patients with LV, OS was significantly longer when treated with Enza [57.2 months; 95% confidence interval (CI): 52.1–62.2 months] versus AA (51.6 months; 95% CI, 42.6–60.6 months; p = 0.003). Consistently, those with LV receiving Enza showed increased rPFS (40.3 months; 95 CI, 25.0–55.7 months) than those having AA (22.0 months; 95% CI, 18.1–26.0 months; p = 0.004). No significant difference in OS or rPFS was observed in those with HV treated with AA versus Enza (p = 0.51 and p = 0.73, respectively). In multivariate analysis of patients with LV, treatment with Enza was independently associated with better prognosis than AA.
Conclusion:
Within the intrinsic limitations of a retrospective design and small population, our report suggests that volume of disease could be a useful predictive biomarker for patients starting first-line ARSi for mCRPC.
Keywords
Introduction
Prostate cancer is the second most frequent cancer and fifth cause of cancer-related death in men worldwide. 1 Metastatic castration-resistant prostate cancer (mCRPC) is an aggressive state of disease with a median overall survival (OS) of approximately 30 months.2,3
Clinical data on the optimal management of men with mCRPC and low volume (LV) or high volume (HV) of disease are currently scarce in the literature. 4 Although there is yet no consensus over the definition of LV, mCRPC patients with bone and/or lymph node metastases showed a more favorable prognosis than those with visceral extension. 5
In current clinical practice, the androgen receptor signaling inhibitors (ARSis) abiraterone acetate (AA) plus prednisone and enzalutamide (Enza) are the first and second, respectively, most administered first-line therapies for mCRPC. 6 In this setting, AA and Enza have shown similar efficacy as life-prolonging agents and to date there is no validated outlier indicating the better option as first-line treatment for mCRPC. 6 In the CHARTEED trial (E3805), patients’ stratification by disease volume highlighted the clinical benefit of chemohormonal therapy compared to ADT alone on the OS of patients affected by HV metastatic castration-sensitive prostate cancer (mCSPC). 7 Determining whether patients with different volume of disease at ARSi start benefit more from one ARSi than the alternative is of medical interest and could improve treatment decision-making. Therefore, this study retrospectively investigated the clinical impact of volume of disease on patients receiving AA versus Enza as first-line therapy for mCRPC.
Methods
This cohort study followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines. Nine institutions in the United States, Italy, Switzerland, France, and Brazil participated in this retrospective study. An institutional review board approval was achieved in each center prior to commencing data collection and a waiver of informed consent was granted owing to all data being deidentified.
A cohort of consecutive patients who started AA or Enza as first-line treatment for histologically confirmed and radiologically evident mCRPC between 1 January 2015 and 1 April 2019 was identified from the clinical and electronic registries of the nine participating centers. Those treated with other life-prolonging therapies prior to AA or Enza, apart from ADT, ADT plus docetaxel, or ADT plus radiotherapy, were excluded from the study. CRPC diagnosis was based on Prostate Cancer Working Group (PCWG) 2 or 3 (depending on whether the case was prior to 2016 or not) definition.8,9 Clinicopathologic data, including age, race, Gleason score, type of metastatic disease presentation (whether after prior local therapy or newly diagnosed), treatment for mCSPC, volume of disease at time of metastatic disease presentation, type of metastases at ARSi start, Eastern Cooperative Oncology Group (ECOG) performance status (PS) at ARSi start were collected from medical and electronic charts of each participating center. Data cutoff date was 1 April 2022. Patients were categorized into four cohorts by type of ARSi received (AA or Enza) and volume of disease (LV or HV per E3805 definition; HV defined as the presence of visceral metastases and/or ⩾4 bone metastases of which ⩾1 out of the spine/pelvis 7 ) at ARSi start. Co-primary endpoints were OS, defined as time from AA or Enza initiation to death from any cause or censored at the last follow-up visit, whichever occurred first, and radiographic progression-free survival (rPFS), defined as the interval within AA or Enza onset and radiological progression by conventional imaging (CT scan, MRI, and bone scan) according to the Response Evaluation Criteria in Solid Tumors criteria, version 1.1, 10 or death from any cause or censored at last clinical visit, whichever occurred first. Time to prostate-specific antigen (PSA) progression was defined as the record time between first-line ARSi start and PSA progression per PCWG 2 definition. 8 Kaplan–Meier method was used to estimate endpoints distributions, including median time-to-event and its 95% confidence interval (CI), while log-rank test was used to compare time-to-event distributions among the cohorts. The Cox model was applied to assess the time-to-event endpoints in univariate and multivariate models.
Results
A total of 420 patients [median age, 75 years; 376 Caucasian men (90.4%)] was selected for this analysis. Of these, 170 (40.5%) had LV and received AA (LV/AA), 76 (18.1%) had LV and were given Enza (LV/Enza), 124 (29.5%) had HV and received AA (HV/AA), and 50 (11.9%) had HV and were treated with Enza (HV/Enza). Median follow-up was 32.4 months (95% CI, 30.6–34.2 months) (Table 1).
Patient characteristics.
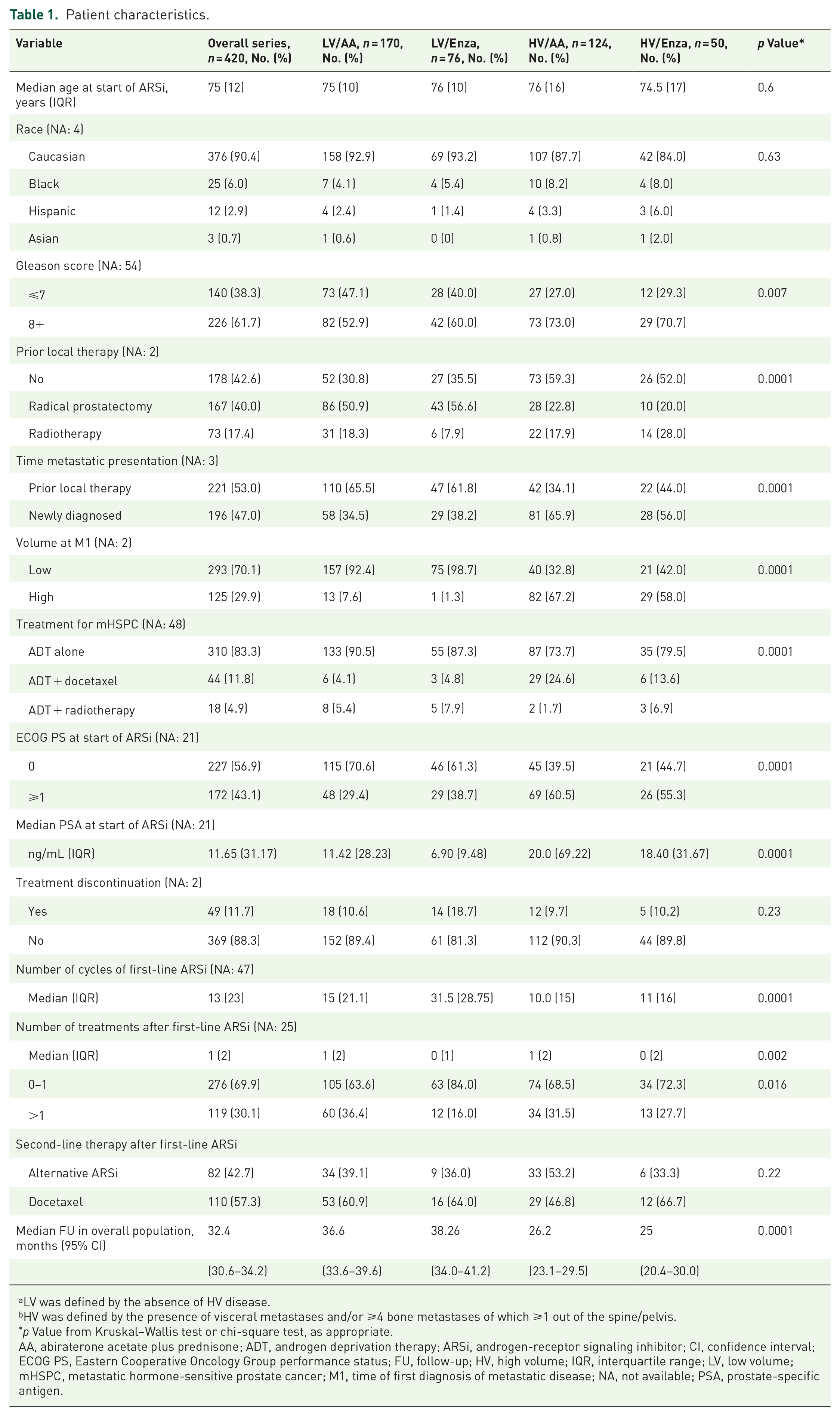
LV was defined by the absence of HV disease.
HV was defined by the presence of visceral metastases and/or ⩾4 bone metastases of which ⩾1 out of the spine/pelvis.
p Value from Kruskal–Wallis test or chi-square test, as appropriate.
AA, abiraterone acetate plus prednisone; ADT, androgen deprivation therapy; ARSi, androgen-receptor signaling inhibitor; CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group performance status; FU, follow-up; HV, high volume; IQR, interquartile range; LV, low volume; mHSPC, metastatic hormone-sensitive prostate cancer; M1, time of first diagnosis of metastatic disease; NA, not available; PSA, prostate-specific antigen.
Among patients with LV, the administration of Enza was associated with improved median OS (57.2 months; 95% CI, 52.1–62.2 months; p = 0.003) compared to AA (51.6 months; 95% CI, 42.6–60.6 months) and the risk of death was more than halved in the LV/Enza cohort compared to the LV/AA cohort [hazard ratio (HR) = 0.46; 95% CI, 0.27–0.78). No statistically significant difference in the median OS of those with HV receiving AA versus Enza was observed (p = 0.0.51) (Table 2). The Kaplan–Meier curves highlight the protective effect of Enza for those with LV (Figure 1(a)) and similar efficacy of AA or Enza for those with HV (Figure 1(b)). Similarly, median rPFS was significantly extended in the LV population receiving Enza versus AA (40.3 months; 95% CI, 25.0–55.7 versus 22.0 months; 95% CI, 18.1–26.0; p = 0.004) and the risk of progression or death was decreased by 40% (HR = 0.60; 95% CI, 0.42–0.85), whereas no differential rPFS effect was observed in the HV population according to the type of ARSi administered (p = 0.73) (Table 2). The Kaplan–Meier curves remark the greater rPFS benefit of Enza versus AA for the population with LV splitting early (Figure 2(a)) while the curves clearly overlap in the population with HV suggesting that Enza and AA fare similarly (Figure 2(b)). Consistently with the co-primary endpoints outcomes, median time to PSA progression in those with LV having Enza was twofold compared to those having AA (21.4 months; 95% CI, 15.9–24.1 versus 10.7 months; 95% CI, 8.6–11.8; p = 0.003) and the risk of biochemical progression was more than halved (HR = 0.46; 95% CI, 0.31–0.68), whereas no significant difference was observed between the two treatment cohorts in those with HV (p = 0.57) (Table 3).
OS and rPFS outcomes in overall population by volume of disease and type of ARSi.

LV was defined by the absence of high volume disease.
HV was defined by the presence of visceral metastases and/or ⩾4 bone metastases of which ⩾1 out of the spine/pelvis.
p Value from univariate Cox regression analysis.
AA, abiraterone acetate plus prednisone; ARSi, androgen-receptor signaling inhibitor; CI, confidence interval; Enza, enzalutamide; HR, hazard ratio; HV, high volume; LV, low volume; mo, months; OS, overall survival; rPFS, radiographic progression-free survival.

Kaplan–Meier curves of OS in patients with LV (a) and patients with HV (b), by type of ARSi administered.

Kaplan–Meier curves of rPFS in patients with LV (a) and patients with HV (b), by type of ARSi administered.
Time to PSA progression in overall population by volume of disease and type of ARSi.

LV was defined by the absence of high volume disease.
HV was defined by the presence of visceral metastases and/or ⩾4 bone metastases of which ⩾1 out of the spine/pelvis.
p Value from univariate Cox regression analysis.
AA, abiraterone acetate plus prednisone; ARSi, androgen-receptor signaling inhibitor; CI, confidence interval; Enza, enzalutamide; HR, hazard ratio; HV, high volume; LV, low volume; mo, months; OS, overall survival; PSA, prostate-specific antigen; rPFS, radiographic progression-free survival.
Consistently with the univariate model, in the multivariable analysis of patients with LV, adjusting for clinicopathological variables resulted significant in the univariate model, the use of Enza was independently associated with increased survival compared to AA (HR = 0.49; 95% CI, 0.25–0.95; p = 0.034) (Table 4).
Multivariable analysis of OS in patients with LV by type of ARSi.

AA, abiraterone acetate plus prednisone; ADT, androgen deprivation therapy; CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group performance status; HR, hazard ratio; LV, low volume; mCSPC, metastatic castration-sensitive prostate cancer; OS, overall survival; PSA, prostate-specific antigen.
Discussion
To our knowledge, this international multicenter cohort study is the first to assess the clinical impact of volume of disease on the efficacy of AA or Enza used as first-line therapy for mCRPC patients. This report showed that those with LV experienced significantly longer OS, rPFS, and time to PSA progression with Enza compared to AA. Interestingly, the cohort LV/Enza had numerically higher rates of Gleason Score ⩾ 8 (60% versus 52.9%), de-novo disease (38.2% versus 34.5%), and ECOG PS ⩾1 (38.7% versus 29.4%) compared to the cohort LV/AA (Table 1). Furthermore, the proportion of patients receiving at least two lines of treatment after first-line ARSi progression was higher for LV/AA (84.0%) compared to LV/Enza (63.6%) (Table 1). In aggregate, these data seem to highlight the greater benefit of Enza versus AA on those with LV since this effect was observed despite LV/Enza cohort showing worse prognostic factors and receiving lesser life-prolonging treatments for mCRPC.
In contrast, those with HV fared similarly in terms of survival and radiographic or biochemical progression, regardless of the ARSi used. However, it should be noted that the HV/AA cohort had numerically higher proportions of men with de-novo disease (65.9% versus 56%), ADT plus docetaxel for mCSPC (24.6% versus 13.6%), and alternative ARSi as second-line therapy (53.2% versus 33.3%) than the HV/Enza (Table 1) and this may have biased the results in the HV population. In this regard, the retrospective design and the restricted sample size are chief limitations to this study. Also, the lack of randomization and subsequent numerical imbalances among the cohorts inevitably introduced confounding factors into the analysis. Finally, the missing record of some clinically meaningful variables such as the presence and intensity of pain, blood test data, or use of prior first-generation antiandrogens further limits the generalizability of the results. However, while discrepancies in patient characteristics and therapy patterns across sites are expected given the retrospective multicenter design of this study, they also allow for this analysis to provide useful real-world data which reflect clinical practice among centers located in different countries and continents, in the western world. Furthermore, in univariate analysis of OS stratified by study center, the protective effect of Enza versus AA on those with LV disease as well as the lack of differential survival impact of the treatment cohorts on those with HV disease were confirmed (Supplemental eTable 1).
Moreover, except for the different safety profile, there is little data in the literature guiding the choice between AA or Enza as first-line therapy for mCRPC patients. A personalized selection between these two agents is even more important considering their potential cross-resistance, which negatively impacts the efficacy of their sequential use. A clinical variable, intuitive and easily attainable in clinical practice, such as the disease burden assessed at start of ARSi, could be a potential outlier of great value to aid treatment decision-making.
Conclusion
Although large prospective clinical trials are warranted to validate these data, our findings suggest that volume of disease could be a predictive biomarker for patients starting AA or Enza as first-line for mCRPC and an accurate classification by volume of disease at ARSi start of such patients could aid optimizing the sequential treatment for mCRPC. Finally, such a potential clinical outlier could help inform large-scale clinical trials resulting in a more precise selection of the population and more balanced randomization process.
Supplemental Material
sj-doc-1-tam-10.1177_17588359231156147 – Supplemental material for Clinical outcomes of volume of disease on patients receiving enzalutamide versus abiraterone acetate plus prednisone as first-line therapy for metastatic castration-resistant prostate cancer
Supplemental material, sj-doc-1-tam-10.1177_17588359231156147 for Clinical outcomes of volume of disease on patients receiving enzalutamide versus abiraterone acetate plus prednisone as first-line therapy for metastatic castration-resistant prostate cancer by Pier Vitale Nuzzo, Francesco Ravera, Calogero Saieva, Elisa Zanardi, Giuseppe Fotia, Andrea Malgeri, Sabrina Rossetti, Loana Bueno Valença, Thiago Martins Oliveira, Charles Vauchier, Ricardo Pereira Mestre, Mikol Modesti, Anna Patrikidou, Sandro Pignata, Giuseppe Procopio, Giuseppe Fornarini, Ugo De Giorgi, Antonio Russo and Edoardo Francini in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We would like to thank and acknowledge the SPARTACUSS Investigators, including: Gianpaolo Spinelli, José Mauricio Mota, Praful K. Ravi, Richard Lee-Yang, Daniel Herchernhorn, Orazio Caffo, Daniele Santini, Carlotta Ottanelli, Karim Fizazi, Christopher Sweeney, Daniel Heng, Silke Gillessen, Stefania Cusenza, Vincenzo Gennusa, Talal El Zarif, Heather McClure, Matthew Davidsohn, and Livia Maria Andrade.
Correction (June 2023):
Authors “Talal El Zarif”, “Matthew P. Davidsohn”, “Heather McClure”, and “Praful Ravi” have been added to the author list
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.