
Abstract
Objective:
Our aim was to provide practical recommendations on the management of patients with metastatic castration-resistant prostate cancer (mCRPC) who have progressed after docetaxel plus androgen-deprivation therapy (ADT) or abiraterone plus ADT.
Methods:
Systematic literature review (SLR), nominal group meeting, and Delphi process. A panel of 12 experts was established who defined the scope, users, and sections of the document. We performed an SLR in order to assess the efficacy and safety of available drugs in patients with mCRPC. Abstracts from the American Society of Oncology and European Society for Medical Oncology meetings were also examined. The results were discussed during an expert meeting in which 14 recommendations were generated. The level of agreement with the recommendations was also tested by 13 additional experts following the Delphi process. Recommendations were voted by means of scores ranging from 0 (total disagreement) to 10 (total agreement). We defined agreement when at least 70% of the experts voted ⩾7. Next, we assigned a level of evidence and grade to the recommendation using the Oxford Centre for Evidence-based Medicine Levels of Evidence, following which the final document was drafted.
Results:
The literature search did not find any articles meeting the inclusion criteria. Finally, 13 out of 14 recommendations were accepted after two Delphi rounds (two were modified after the first round). They pertain to general and individual case-based treatment recommendations.
Conclusions:
In mCRPC patients who have progressed after docetaxel or abiraterone plus ADT in the metastatic hormone-sensitive prostate cancer setting, these recommendations may support treatment decision-making, due to the lack of evidence or other globally accepted sequencing algorithms.
Keywords
Introduction
Prostate cancer is still a leading cause of death worldwide largely due to metastatic disease. 1 For patients with an initial diagnosis of metastatic hormone-sensitive prostate cancer (mHSPC), continuous androgen-deprivation therapy (ADT) represented the standard of care until 2015, when trials such as the Androgen Ablation Therapy with or without Chemotherapy in Treating Patients with Metastatic Prostate Cancer (CHAARTED) 2 showed that ADT combined with six courses of docetaxel (DOC) significantly prolonged/extended the overall survival (OS) of patients with high-volume disease. Similarly, in 2017, the LATITUDE trial demonstrated that adding abiraterone acetate (ABI) and prednisone to ADT significantly increased OS and radiographic progression-free survival in mHSPC men with high-risk features. 3 These trials contributed to modifying the initial treatment approach of mHSPC.
In the previous years, several agents were approved for the management of men with mCRPC, including ABI, 4 enzalutamide (ENZ), 5 radium-223, 6 cabazitaxel (CAB), 7 and sipuleucel-T. 8 Nonetheless, little is known about optimal sequencing and combination strategies, or how cross-resistance is likely to affect subsequent treatments in the continuum of patient care.
On the other hand, patients following CHAARTED and LATITUDE strategies will likely progress later on to metastatic castration-resistant prostate cancer (mCRPC). Therefore, in the near future, many patients presently on these new schemes will progress and be seen in daily practice, while the available evidence to define the best next step proves to be scarce.
In 2018, there was no robust evidence to define the best next step for patients progressing to the castration-resistant state after ADT plus DOC (CHAARTED) or ABI (LATITUTE). Therefore, the aim of this document is to provide practical recommendations for the management of patients in this setting. These recommendations are based on the available evidence and experience of a panel of prostate cancer experts, covering common clinical scenarios and the characteristics of patients attended in daily practice. We are confident that these recommendations are likely to support health professionals involved in the treatment of these patients in the decision-making process.
Methods
The nominal group and Delphi techniques were employed to elaborate the consensus. The document was created following the distribution of tasks and comments to the participants with the help of a systematic literature review (SLR) and other comprehensive literature searches across international oncology congresses. All processes were supervised by a methodologist. The expert panel comprised 12 oncologists with recognized experience in the management of prostate cancer. Two were also coordinators of the project.
SLR
A SLR was performed to address the experts’ questions regarding the management of patients with mCRPC who have progressed after on ADT plus DOC or ADT plus ABI. For this purpose, a protocol was defined with the coordinators and the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement was followed. 9
Search strategy
Studies were identified by sensitive search strategies in the main bibliographic databases (supplemental data). An expert librarian collaborated with the expert panel and checked the search strategies. The following bibliographic databases were screened: Medline and Embase from 1961 to 11 January 2018, and Cochrane Central register of Controlled Trials (CENTRAL) up to 11 January 2018. We used specific Medical Subject Headings (MeSH) and additional keywords to identify studies. The strategy combined disease and treatment terms as listed above, with a controlled vocabulary to describe any of them. All the retrieved references were managed using Endnote X5 (Thomson Reuters).
The abstracts of the scientific meetings of the American Society of Oncology (ASCO/ASCOGU; 2017, 2018) and European Society for Medical Oncology (ESMO; 2016, 2017) were similarly examined through simple keywords in the organizations’ websites.
Study selection
The studies retrieved by the search strategies were incorporated if they met the following pre-established inclusion criteria: (a) involving mCRPC patients who have progressed after on ADT plus DOC or ADT plus ABI; (b) focusing on those who start a new available antineoplastic treatment, such as DOC, CAB, ABI, ENZ, or radium-223; (c) analyzing outcomes that are usually evaluated in mCRPC trials, such as OS, PFS, prostate-specific antigen (PSA) response or progression, radiographic response or progression, quality of life, and safety; (d) meta-analyses, systematic reviews, randomized clinical trials (RCT) were solely selected, as were English and Spanish articles. We excluded articles on animals, basic science, as well as publications analyzing sipuleucel-T, as this product has been withdrawn from use in the European Union.
Finally, a hand search was conducted by reviewing the references of the included studies, along with all the publications or other information related to the SLR provided by the experts.
Screening of studies, data collection, quality evaluation, and data analysis
These processes were performed by two reviewers. Both reviewers independently screened the titles and abstracts of the retrieved articles for selection criteria. When the reviewers encountered any discrepancy, a consensus was reached by including a third reviewer (LC). After the articles originating from the selection process had been read in detail following the same principles, a list of studies to be included was established. Afterwards, the reviewers collected the articles data independently. As in previous phases, in the event of discrepancies, a consensus was reached by looking at the original article or by including a third reviewer (LC).
To grade the quality, we used the Jadad score 10 for RCT and a modification of The Oxford Centre for Evidence-based Medicine Levels of Evidence in its updated version of May 201111 for the remaining study designs. Evidence tables were produced. Meta-analysis was only scheduled when enough homogeneity existed among the included studies.
Nominal group meeting
The expert panel held a nominal group meeting in which objectives, scope, and users were defined. Then, the results of the SLR and of the ASCO/ASCOGU and ESMO meetings were presented and discussed. Taking into account the lack of robust evidence, the experts considered their experience, patients/disease/health system characteristics, indirect data from other RCTs, and preliminary published data (observational studies). Through a guided discussion, different clinical scenarios were addressed and recommendations for optimal treatment proposed. These recommendations were rephrased several times during the meeting in order to achieve the best wording and the maximum level of agreement. For each clinical scenario, specific patient profiles and treatments were similarly considered, in addition alternative treatment possibilities.
Delphi and final document
After several expert reviews, definitive recommendations were generated and subsequently submitted to on-line Delphi voting. Delphi was extended to a group of 24 oncologists with experience in the management of patients with prostate cancer. The participants voted each recommendation using a scale ranging from 0–10 (0 = totally disagree; 10 = totally agree). Agreement was obtained when at least 70% of the participants voted ⩾7. The recommendations with a lower level of agreement (LA) were reassessed and, if appropriate, re-edited and voted in a second Delphi round.
Subsequently, the final document was written. For each recommendation, the level of evidence (LE) and grade of recommendations (GR) were applied according to the Oxford Centre for Evidence Based Medicine Guidelines, 11 along with the LA according to the Delphi process, as previously presented. The document was then distributed to the experts for final assessment and comments.
Results
SLR and Delphi results
The SLR retrieved more than 5000 articles. We additionally analyzed 633 abstracts from ASCO/ASCO-GU and ESMO meetings, yet none met the inclusion criteria (see supplemental data). As described in the methods section, due to a lack of robust evidence the experts based their recommendations on other aspects like their experience, patients/disease/health system characteristics, indirect data from other RCTs, and preliminary published data. Finally, we show the preliminary data (from observational studies or phase I–II RCTs) captured from the project.
The expert panel generated 14 recommendations that were voted. The Delphi response rate was 70%. All but one recommendation achieved the pre-established LA in the first round. During this round, however, the Spanish Medicine Agency issued a press release recommending a restriction in the use of radium-223 (Xofigo©) to only patients who have undergone two previous treatments for mCRPC or were not eligible for any other systemic treatment (see recommendations 12 and 13). As two of the recommendations were related to the use of radium-223 (one did not obtain agreement), they were re-formulated and evaluated in a second Delphi round, with only one eventually accepted.
General considerations and other evidence
Despite the lack of robust evidence, there are some observational data concerning patients with mCRPC who have progressed after undergoing DOC plus ADT or ABI plus ADT that we would like to briefly describe.
A recent retrospective study has shown that rechallenging with DOC at castration-resistance was only active in a limited number of patients (14%) treated upfront with ADT plus DOC for metastatic castration-naive prostate cancer. 12 Though based on a small number of patients, anticancer activity was observed with ABI or ENZ in this article. 12 In line with this finding, another small-sized retrospective observational study seemed to support these data. 13
We would like to point out that the decision-making process for these patients must take into account several aspects, especially the time-to-progression, patient’s performance status and fitness for a specific treatment, 14 and previous and potential drugs toxicities or cross-resistance between treatments. Yet, there are also patients with other characteristics (high volume, visceral disease, aggressive variants, etc.) for whom an individual case-based strategy appears to be most appropriate, as we will further explain later on.
In addition, the panel considers that treatment decisions should be individualized according to the physicians’ experience and patients’ characteristics and preferences. Therefore, patient information and discussions prove to be crucial.
Of note is that there is evidence supporting drug-sequencing in mCRPC patients who were only treated following progression after ADT, and these data may likewise contribute to the decision making.15,16
General recommendations are presented below and in Table 1, with a treatment algorithm depicted in Figure 1.
Recommendations and results of the Delphi process.

ABI, abiraterone; ADT, androgen-deprivation therapy; CAB, cabazitaxel; DOC, docetaxel; ECOG, Eastern Cooperative Oncology Group; EMA, European Medicines Agency; GR, grade of recommendation; LE, level of evidence; Max, maximum; mCRPC, metastatic castration-resistant prostate cancer; Min, minimum; p25, percentile 25; p75, percentile 75; SD, standard deviation; SIOG, International Society of Geriatric Oncology.
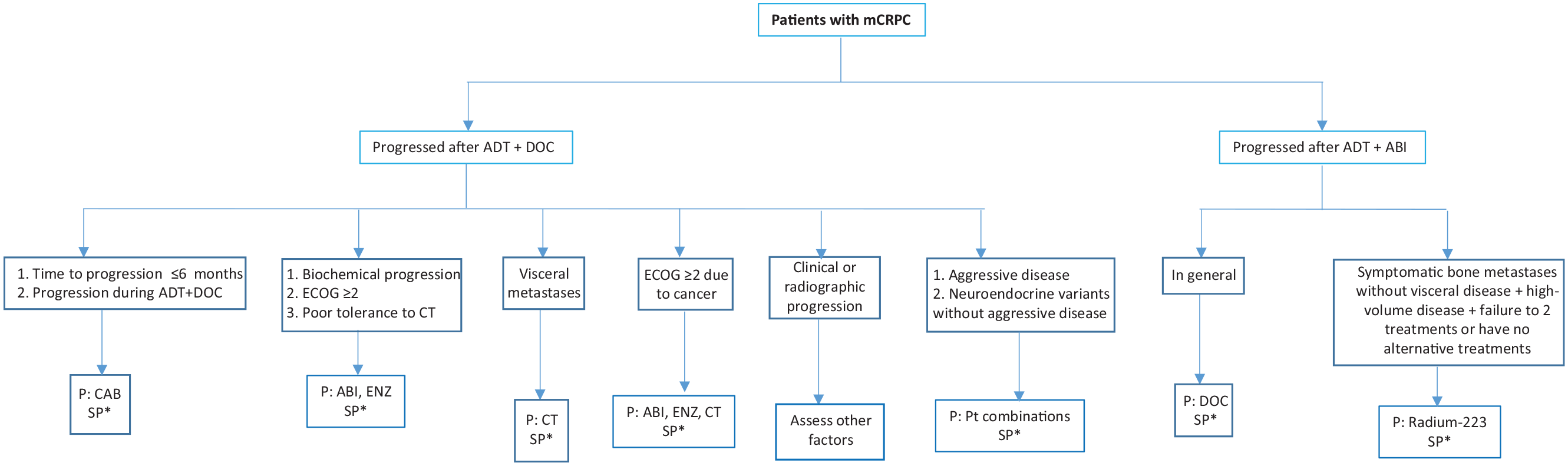
Treatment algorithm for patients with mCRPC upon DOC or ABI plus ADT (1st line) in metastatic prostate cancer.
Recommendations (general settings and specific profiles)
The panel considers it important to highlight that time-to-progression is an essential factor to consider. Although it is not possible to establish what this time should be, 6 months seem to be an acceptable cut-off. A small case series supports the use of CAB if the time-to-progression is less than 6 months following upfront DOC. 17 In any case, close monitoring is highly recommended.
As previously exposed, there are factors that must similarly be considered, such as previous toxicity of chemotherapy and the patient′s health status. For example, for patients with poor chemotherapy tolerance, ABI or ENZ should be considered. These drugs have shown benefits in a small-sized case series of patients who progressed after ADT+DOC treatment. 18
Similarly, for patients who develop asymptomatic or PSA-only progression, ABI or ENZ are alternative options, whereas in this setting, the panel recommends close monitoring of drug efficacy so as to allow for switching to other treatments in the event of inefficacy or of clinical doubts regarding efficacy.
Considering the rapid progression during ADT, it could be assumed or should be borne in mind that these patients will not respond as expected to second-generation antihormonal drugs. Although more studies are required to confirm this, CAB can be beneficial in patients with rapid progression during DOC.17,19
The COU-AA-3013,20 and AFFIRM trials 21 evaluated the efficacy and safety of ABI and ENZ versus placebo in patients with mCRPC progressing after DOC. Both trials depicted a dramatic PSA-response. Given that there is no direct comparison between ABI and ENZ and because of apparent similar efficacy and acceptable safety profiles, treatment selection must be individualized, taking into account both the patients comorbidities and drug characteristic features.
Given this clinical scenario, due to the lack of direct or indirect evidence in favor of a specific drug, the panel proposes to base treatment decisions on other variables and outcomes, (such as time-to-progression, the presence of symptoms and symptom intensity, previous therapeutic response and treatment toxicity, location of metastases, comorbidities, etc.)
Owing to the poor cancer prognosis when associated with many visceral metastases (in general), but especially hepatic metastases, the panel agreed on recommending chemotherapy. Yet, there may be patients, such as those with elevated PSA levels or poor health status, in whom ENZ administration could be assessed. If ENZ turns out to be the final treatment decision, close monitoring of ENZ efficacy must be performed. In other cases, such as small number/size of metastases, certain metastasis localizations, or longer time-to-progression, a different treatment to chemotherapy could be considered as well.
Recommendation 7. In patients with mCRPC who have progressed after ADT+DOC treatment (1st line) and present an ECOG score ⩾2, deemed to be cancer-related, the panel considers chemotherapy to be a potential treatment option (LE 5; GR D; LA 85%).
A patient with an impaired performance status may, in general, be ruled out for chemotherapy, as this setting is associated with both poor prognosis and reduced drug tolerance. 22 However, if the performance status is deemed to be related to disease progression and when the clinician considers it to be possibly reversible, chemotherapy could be discussed with the patient and, if agreed upon, delivered following appropriate dose and schedule adjustments.
The sequence of first-line carboplatin plus DOC followed by second-line etoposide plus cisplatin was evaluated in a phase II trial that involved 120 mCRPC patients with at least one anaplastic clinical criterion. 23 It was found that, of the seven “anaplastic” criteria, bulky tumor mass was significantly associated with poor outcome, lactic acid dehydrogenase strongly predicted OS (and rapid progression), and serum carcinoembryonic antigen concentration strongly predicted OS (but not rapid progression), whereas neuroendocrine markers were unable to predict outcome or response to therapy. The authors conclude that patients with “anaplastic” prostate cancer are a recognizable subset, characterized by a high response rate of short duration to platinum-containing chemotherapies. More recently, a phase I–II RCT has shown promising activity with carboplatin added to CAB in metastatic castration-resistant prostate cancers. 24 Although the results require further confirmation, these findings may support decision-making in patients with mCRPC and aggressive disease.
Different non-randomized, retrospective studies have demonstrated platinum-based chemotherapies to be active in men with neuroendocrine prostate cancer.25–27 Therefore, platinum-based chemotherapy is a treatment option for these patients with poor prognosis.
Poor tolerance to previous chemotherapy generally guides the selection of a different drug class for subsequent treatment lines.28,29 Nevertheless, as ABI and ENZ are also associated with undesirable effects, clinicians must be familiar with the diagnosis and management of these undesirable effects. 29
As in other general settings, patients with poor ECOG performance status may benefit from other treatment options. The panel has additionally considered the possibility of cross-resistance between ABI and ENZ.30,31 It should indeed be noted that cross-resistance among different treatments for mCRPC was reported.19,32
We have previously commented that, as a consequence of the EMA restriction press release during the first Delphi round, the original recommendation that stated that radium-223 could be considered in patients with mCRPC who have progressed after ADT+ABI treatment (1st line) and present symptomatic bone metastases without visceral disease was rephrased, thereby clearly limiting the indications for radium-223. Despite the EMA restrictions, this recommendation reached the stated agreement level.
The original recommendation claimed that, in this patient group, radium-223 could be considered in those with symptomatic bone metastases without visceral disease, or for palliative care. Following the EMA restrictions, this recommendation was, however, rephrased the same way as the previous recommendation, thereby restricting the use of radium-223. Nonetheless, the level of agreement obtained for this case scenario turned out to be poor.
This recommendation will be further discussed in the next section.
To select the optimal treatment for a given patient, the decision-making process must undeniably seek the patient′s participation, evidence-based information regarding treatment options, and experience and knowledge of the treatment provider.
Discussion
The results of CHAARTED and LATITUDE trials,2,3,33 along with the approval of several new drugs,4–8 have raised new questions and issues as for the management of mCRPC. In this setting, the impact of upfront DOC or ABI plus ADT on subsequent therapies has so far been poorly explored.
In this research, we sought to create practical recommendations for different clinical scenarios, which prove to be quite common in daily practice. As there are no randomized controlled trials pertaining to this clinical setting, we performed a comprehensive literature search using not only the main medical databases, but also the proceedings of international congresses and scientific meetings. We decided to deliver a treatment algorithm and formulate recommendations for general clinical scenarios, and provide some guidance for specific situations within these scenarios. Finally, we limited our work so as to define the first-line treatment for mCRPC following progression in the metastatic hormone-naïve state.
Concerning the different clinical scenarios, we would like to comment on several issues that were discussed during the project. Recent observational studies have shown that baseline characteristics of CRPC disease could help identify the best therapy option for patients previously treated with DOC or ABI+ADT in mHSPC.34,35 The same way data from RCTs in mHSPC patients like the ENZAMET and TITAN trial might also contribute.33,36,37 To formulate recommendations, we therefore considered several different scenarios, such as pattern of progression, time to develop mCRPC, presence of clinical aggressive disease, patient health status, prior tolerance to chemotherapy, cross-resistance between drugs, as well as tumor histology.
The lack of evidence in mCRPC following the referred schemes thus resulted in recommendations with a very low evidence level. Nevertheless, we would like to highlight that following the Delphi process, for all except one recommendation, agreement was reached with a high level of agreement for most recommendations. In our view, this markedly increases the validity of the recommendations herein presented.
As described in the results section, two recommendations that included radium-223 were rephrased following the release of EMA restrictions, with one not reaching the pre-established level of agreement. This recommendation proposed ENZ to be the first preference in patients with mCRPC who have progressed after ADT+ABI treatment and are unfit according to SIOG criteria. Given this context, the disagreement may be partly accounted for by the fact that DOC could be a therapeutic option, yet with some reservation as for the patient health status. This could still be an option, bearing in mind the possibility of cross-resistances between ABI and ENZ. Yet, this could be a clear scenario for radium-223 administration in other patients. Nevertheless, radium-223 is now recommended for patients who have either previously failed in two treatments or have no alternative cancer treatments available. Likewise, this may explain the disagreement concerning this recommendation.
In summary, treating metastatic prostate cancer is proving increasingly complex and challenging. While the introduction of the CHAARTED, STAMPEDE, and LATITUDE schemes have clearly improved the prognosis of patients with metastatic hormone-naïve prostate cancer, they have also altered the traditional sequencing when castration-resistance occurs, yet with only scarce evidence available to guide treatment decisions. Therefore, we are now confident that our recommendations for different clinical scenarios will support health professionals involved in the care of these patients.
Supplemental Material
Supplementary_data – Supplemental material for Expert recommendations on the management of patients with metastatic castration-resistant prostate cancer who progress after CHAARTED or LATITUDE
Supplemental material, Supplementary_data for Expert recommendations on the management of patients with metastatic castration-resistant prostate cancer who progress after CHAARTED or LATITUDE by Javier Puente, Urbano Anido, Miguel Ángel Climent, Enrique Gonzalez-Billalabeitia, Nuria Lainez, Julio Lambea, José Pablo Maroto, Maria Jose Mendez-Vidal, Álvaro Montesa, Angel Rodriguez, Curro Zambrana and Aránzazu González-del-Alba in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We would like to thank Luis León Mateos, Natalia Fernández Nuñez, Martín Lázaro Quintela, Sergio Vázquez Estevez, Ovidio Fernández Calvo, Francisco Javier Afonso Afonso, Rodrigo Lastra, Pablo Gajate Borau, Carlos Aguado, Guillermo de Velasco, Carlos Álvarez Fernández, María Sereno Moyano, and Diego Soto de Prado for their participation in the Delphi process.
Author contributions
All of the authors contributed in the study design, analysis and interpretation of data, drafting the article, and revising it critically. All of them have also approved the final draft.
Conflict of interest statement
Javier Puente has received honoraria as consultant on advisory boards from Pfizer, Astellas, Janssen, MSD, Bayer, Roche, BMS, Boehringer, Astra Zeneca, Ipsen, Novartis, Eusa Pharma, Eisai and Sanofi; and as speaker from Kyowa, Celgene, Lilly and Merck; Aranzazu González del Alba has received honoraria for advisory boards, consultancy, speaker and for travel support from Pierre Fabre, Roche, Bristol-Myers Squibb, MSD, Pfizer, Novartis, Bayer, Janssen, Sanofi, Astellas, EUSA pharma, Ipsen, EISAI and Astra-Zeneca; Pablo Maroto has received honoraria for consulting or advisory role from Sanofi, Janssen, Astellas, and Bayer. Urbano Anido has received honoraria from Pfizer, Novartis, Bayer, Bristol-Myers Squibb, EUSA Pharma, and Eisai; Nuria Lainez has received honoraria for consulting or advisory role from Pfizer, Sanofi, Ipsen, BMS, Roche, and Astra Zéneca. The rest of authors declare no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by an unrestricted grant from Sanofi.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.