
Abstract
Breast cancer (BC) is the most commonly diagnosed cancer worldwide. Advanced BC with brain metastasis (BM) is a major cause of mortality with no specific or effective treatment. Therefore, better knowledge of the cellular and molecular mechanisms underlying breast cancer brain metastasis (BCBM) is crucial for developing novel therapeutic strategies and improving clinical outcomes. In this review, we focused on the latest advances and discuss the contribution of the molecular subtype of BC, the brain microenvironment, exosomes, miRNAs/lncRNAs, and genetic background in BCBM. The blood–brain barrier and blood–tumor barrier create challenges to brain drug delivery, and we specifically review novel approaches to bypass these barriers. Furthermore, we discuss the potential application of immunotherapies and genetic editing techniques based on CRISPR/Cas9 technology in treating BCBM. Emerging techniques and research findings continuously shape our views of BCBM and contribute to improvements in precision therapies and clinical outcomes.
Background
Based on data released from the International Agency for Research on Cancer in 2021, breast cancer (BC) has surpassed lung cancer as the most common cancer in the world. 1 One of the greatest challenges to BC treatment is distant metastasis to different organs, such as the lung, brain, bone, and liver. 2 Brain metastasis (BM) affects approximately 30–50% of patients with metastatic BC and has become a major cause of morbidity and mortality.3,4 In terms of epidemiology, the incidence of BCBM has increased significantly over the past decade due to earlier diagnosis by imaging techniques and more effective treatment of primary BC. The incidence of BM varies depending on the BC subtype.5–7 In triple-negative breast cancer (TNBC), the incidence ranges from 25% to 45% and is approximately 50% in human epidermal growth factor receptor 2 (HER2)-positive BC.8,9 The prognosis of breast cancer brain metastasis (BCBM) patients is usually poor, with a median survival time ranging from 3 to 25 months.6,10 BCBM is also associated with serious cognitive and emotional impairment. Therefore, quality of life and life expectancy are significantly impacted in patients with BM. Young age, high histological grade, large tumor size, TNBC type, HER2 enrichment, and extracerebral metastasis are currently thought to be high-risk factors for BCBM. 11 However, the pathological and molecular mechanisms underlying the development of BCBM remain unclear. A better understanding of the underlying mechanisms and exploration into novel therapeutic strategies are urgently needed.
The metastasis cascade of BCBM involves multiple steps consisting of proliferation, extracellular matrix (ECM) invasion, vascular intravasation, survival in the bloodstream, vascular extravasation, and brain colonization.12,13 The activation of epithelial–mesenchymal transition (EMT) is considered to be an important step for primary cancer cell dissemination. BC cells enter the bloodstream through EMT and ultimately can implant into the brain. 13 To survive and proliferate in the brain microenvironment, BC cells must acquire several properties needed to pass through the blood–brain barrier (BBB), accumulate around blood vessels, and promote neoangiogenesis until the BBB is modified to be the blood–tumor barrier (BTB), which is typical in BM. Compared to breast microenvironments, the brain has a distinct anatomy, cell types, metabolic pathways, and local immune microenvironment. The reverse of the EMT, the mesenchymal–epithelial transition, occurs in a process of disseminated tumor cells, enabling them to metastasize from the breast to the brain. Metastatic BC cells can arrive in the cerebellum, cerebral cortex, and other areas of the brain, and are referred to as parenchymal metastasis, leptomeningeal metastasis, and choroid plexus metastasis, respectively. 14 The most common type of BM is parenchymal metastasis (90%), leptomeningeal metastasis accounts for 8%, and choroid plexus metastasis is rare.
The currently used multimodal treatment approaches for BCBM patients, such as surgery, radiation, chemotherapy, and targeted therapy, have led to poor outcomes for most patients. Evidence obtained over decades has shown that, due to low permeability and poor penetration through the BBB/BTB, systemically administered chemotherapy and targeted therapies are largely ineffective as BCBM treatments.15,16 No specific agents for BCBM therapy have been approved by the FDA. 17 Recent advances in clinical trials and preclinical research, however, have confirmed that systemic delivery of therapeutic agents via various transporter systems such as receptor-mediated transcytosis (RMT), carrier-mediated transport (CMT), and absorptive-mediated transcytosis (AMT); nanoparticle-based delivery systems; molecular Trojan horse (MTH) technology; and engineered stem cells are promising approaches to treating BCBM. Identifying the molecular mechanisms and signaling pathways underlying BCBM may lead to the discovery of new targets and strategies for BCBM prevention and treatment.
In this review, we highlight the up-to-date understanding of BCBM molecular mechanisms and explore novel therapeutic strategies. We first introduce the BC molecular subtypes, aiming to provide a significant clinical context, which requires deeper scientific investigation. We next discuss the permeability of the BBB and BTBs, as well as the role played by the distinct brain microenvironment in BCBM. We also discuss the roles of genes, exosomes, miRNAs, and lncRNAs in BCBM. Furthermore, we provide perspectives on recent research that may lead to novel approaches for the treatment of BCBM patients (Figure 1).

The metastasis cascade of BCBM. The steps in the formation of BCBM consist of proliferation, ECM invasion, vascular intravasation, hematogenous dissemination, vascular extravasation, and brain colonization. BC cells acquire several properties needed to cross the BBB, accumulate around blood vessels and promote neoangiogenesis until the BBB is disrupted to be the BTB.
BC subtypes and their association with BM
In 2000, Perou et al. classified BC molecular subtypes on the basis of gene expression. Although more than 10 molecular subtypes of BC have been identified, only the luminal A, luminal B, HER2-positive, and basal-like subtypes are clinically relevant.18,19 In clinical practice, a surrogate classification system based on histological and molecular characteristics is used. Tumors that express estrogen receptor/ progesterone receptor (ER/PR) are grouped as hormone receptor-positive BCs, whereas tumors that do not express ER, PR, or HER2 are classified as TNBCs. 20 Ki67 is a tumor proliferation marker that can be used to distinguish low proliferating luminal A from highly proliferative luminal B. 21 Thennavan et al. recently expanded The Cancer Genome Atlas BC dataset by adding six rare histological subtypes. 22 BC subtype is important in BM development because the risk of developing BCBM varies by subtype, with HER2-positive and TNBC patients having a higher incidence of BCBM.10,23 Molecular subtype-based BM assessments aid in the identification of high-risk BC patients who may benefit from early monitoring, as well as in determining BM patient prognosis.
Although the brain is not the most easily accessible site for HER2-positive BC metastasis, some factors in these patients may lead to preferential BCBM. For example, after trastuzumab therapy, survival rates are significantly improved, but drug penetration across the BBB is limited, and HER2-positive BC cells tend to spread to the brain. From 30% to 55% of patients develop BM. 9 TNBC patients have a 25–46% chance of developing BM. 9 The formation of BM in TNBC is frequently accompanied by the progression of extracranial metastasis, but BM is an early manifestation, which may be due to the lack of effective medications and the high aggressiveness of these tumor cells. When TNBC patients develop BM, the prognosis is poor, with an average survival time of less than 6 months.
Using the SEER database, Martin et al. 6 identified 968 patients with BCBM from a sample of 231,684 BC patients. The goal was to analyze the incidence rate and median survival of BCBM patients on the basis of their previously diagnosed cancer subtype. The findings showed that the incidence proportions of the HER2-positive and TNBC subtypes were the highest, with 1.1% and 0.7%, respectively, in the whole cohort, and 11.5% and 11.4%, respectively, in the metastatic patient subset. The median survival of BCBM for the patients in the overall cohort was 10 months, and among these patients, those with HR-positive/HER2-positive BC had a median survival of 21 months (the longest), whereas TNBC patients had a median survival of 6 months (the shortest). 6 Using the SEER database (2010–2014), Kim et al. investigated the effect of BC subtype on the incidence and prognosis of BCBM. The BM incidence of TNBC and HER2-positive patients was 30.8% and 28.0%, respectively. Patients with the BC luminal A, luminal B, HER2-positive and TNBC subtypes, and BM had median survival of 12, 23, 10, and 6 months, respectively, and the survival was increased to 14, 34, 17, and 8 months in patients with BM without other metastases. These findings suggest that the BC molecular subtype should be considered when evaluating the prognosis of BCBM patients. 10
According to a recent systematic review published by the Jerzak group, the incidence of BCBM was 31%, 32%, and 15% for HER2-positive, TNBC, and HR+/HER2− patients, respectively. Patients with HER2-positive BC and TNBC had a high incidence of BM. 7 Tseng et al. published a single-institution analysis on the relationship between BC subtype and the risk of BM, and they found that 164 (7.3%) of the 2248 BC patients developed BM and had a median survival of 54.2 months. The TNBC and HER2 subtypes were both significant risk factors for BM. BC subtypes are linked to varying risks for BM in different age groups. 24 The median interval between BC diagnosis and BCBM development of the 121 patients in this study was 46 months. BM has been shown to develop much faster in patients with advanced-stage cancer and TNBC. 25 This finding means that TNBC and HER2-positive patients have the shortest median time before BCBM development and the shortest median survival after a BCBM diagnosis (Table 1). 9
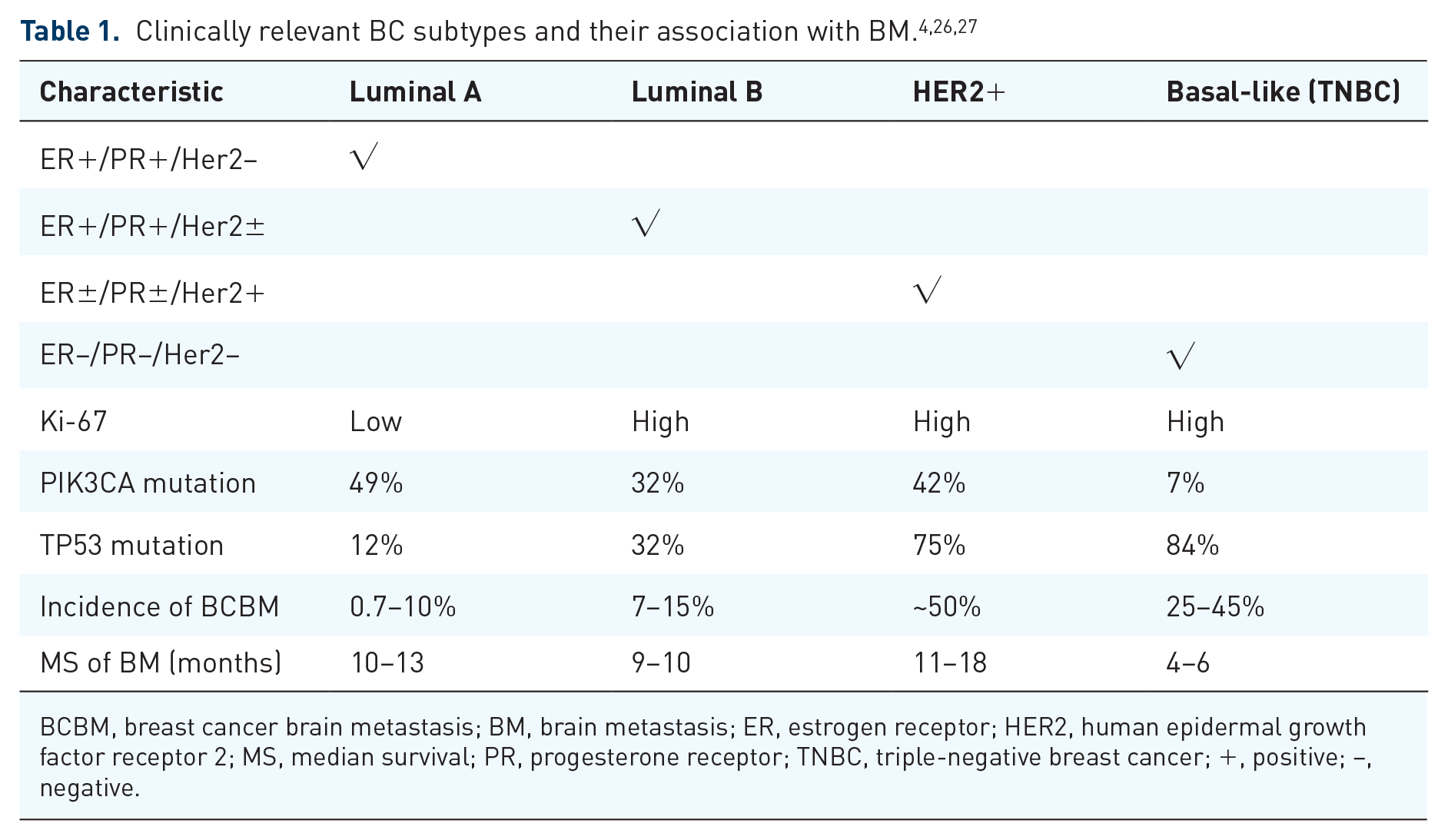
BCBM, breast cancer brain metastasis; BM, brain metastasis; ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; MS, median survival; PR, progesterone receptor; TNBC, triple-negative breast cancer; +, positive; −, negative.
Brain microenvironment and BCBM
The tumor microenvironment is made up of cellular, noncellular, and ECM components. The tumor and its surrounding microenvironment meet specific criteria to initiate cancer cell invasion, colonization, and growth in the distant brain. 28 A growing body of evidence shows that the brain microenvironment is closely related to the development of BCBM. Analyzing how tumor cells cross the BBB and interact with various components of the brain microenvironment can help in understanding BCBM development.
According to the ‘seed and soil’ hypothesis, tumor dissemination is closely related to the interactions between cancer cells and the microenvironment. 29 When tumor cells metastasize to the brain, they face a complex microenvironment that is significantly different from that of the primary site. In the primary tumor environment, various cellular components, such as cancer cells, immune cells, mesenchymal stem cells (MSCs), and endothelial cells, can promote tumor growth. 30 The brain is known to consist of parenchyma and leptomeninges.31,32 The brain parenchyma is composed of dense neurons and glial cells. The crosstalk between tumor cells and these brain-specific cells is a distinguishing feature of BM. The leptomeninges (pia and arachnoid) are brain-specific structures. In addition, the brain metabolic environment differs from that of the primary tumor site. In comparison to the breast microenvironment, the brain microenvironment differs in terms of anatomy, cells, pathways, and immune environment, suggesting that tumor cells that metastasize to the brain must also possess unique features to cross the BBB and grow efficiently in this distinct environment. 33 The dynamic interaction between cancer cells and the brain microenvironment, which is mediated by stromal cells, immune cells and the ECM, is important for cancer development after cell implantation in the brain. 34
Molecular crosstalk between astrocytes and cancer cells during BCBM development has been extensively documented. 35 Astrocytes are highly abundant in the brain and are involved in forming the BBB and maintaining tissue homeostasis. To colonize and proliferate in the brain, BC cells must pass through the BBB. 36 The crucial roles played by tumor-killing or tumor-promoting astrocytes in BM have been well characterized. A1 and A2 are two kinds of reactive astrocytes. The A2 subtype accounts for the majority of astrocytes associated with tumor growth, and these cells express the phosphorylated form of STAT3 at a high level. During the early stages of BC, the STAT3 signaling pathway in BC cells is activated by cytokines and growth factor receptors, creating an immunosuppressive microenvironment that promotes tumor growth and tumor cell metastasis. 37 The evidence has indicated that STAT3 signaling plays a crucial role in the molecular crosstalk between BC cells and astrocytes. 34 For example, Yu et al. described the complex interaction between BC cells, astrocytes, and microglia. Exosomes secreted by astrocytes transfer PTEN-targeting miRNAs into cancer cells, where they mediate PTEN downregulation, resulting in increased CCL2 expression and microglial recruitment, and promoting BM. 38
The brain has long been thought to be an immune-privileged organ with circulating cells excluded from the brain parenchyma. However, this concept has recently been challenged. Functional lymphatic vessels have been discovered and characterized in the meninges of the dorsal and basal skull. 39 These structures can transport cerebrospinal fluid (CSF) and immune cells into deep cervical lymph nodes.39,40 Further research confirmed that they play crucial roles in regulating brain tumor immunity.41,42 The discovery of brain lymphatic pathways prompted scientists to investigate the neuroimmunology hypothesis, and provided an important breakthrough for understanding the mechanism and developing a treatment strategy for BM. Although the types of immune cells in the brain differ from those in peripheral organs, the brain is no longer considered an immune privileged organ, which increases the possibility that immunotherapy for BM can be developed. 43 Brain lymphocytes interact with the systemic lymphatic system through the meningeal lymphatic pathway in deep cervical lymph nodes, and reinvigorated T cells enter the brain to exert antitumor effects. This interaction may be the reason that, in previous immune checkpoint studies, scientists found immunotherapy to be effective against BM. Studies have shown encouraging results for the use of immune checkpoint inhibitors in BM patients. Notably, Ogiya et al. investigated differences in the immune microenvironment of primary BC patients and BCBM patients. The numbers of tumor-infiltrating lymphocytes (TILs) and CD4/CD8/Foxp3-positive cells were remarkably higher in the primary BC patients than in the BCBM patients. Moreover, the significantly shorter overall survival (OS) found in TNBC patients was associated with a low number of TILs. 44 Sambade et al. investigated the prognostic implications of the unique BCBM microenvironment in 203 BCBM patients who underwent craniotomy. HER2-positive BCBM with high immune cell infiltration and hemorrhage had a better prognosis. TNBC BM with gliosis was also associated with a better prognosis. In-depth research into the microenvironment of BCBM can greatly improve patient prognosis and lead to the development of new treatment strategies. 45
However, to date, immunotherapies have provided little benefit in treating BM due to low BBB permeability and poor penetration of the BBB. In addition, BC is one of the major causes of leptomeningeal metastasis, and little is known about the role that the brain microenvironment plays in leptomeningeal metastasis. How do BC cells influence the subarachnoid microenvironment? They secrete complement component 3, which opens BBB tight junctions, allowing growth factors to enter the CSF to promote metastatic growth 46 (Figure 2).

Crosstalk among BC cells, glial cells, and the brain microenvironment. Exosomes, miRNAs, and lncRNAs derived from BC cells can increase BBB permeability and promote BC cell crossing. In addition, the higher BTB permeability was due to upregulated astrocytic secretion of IL-6 and CCL2. The STAT3 signaling pathway in BC cells establishes an immunosuppressive microenvironment to promote tumor growth and metastasis. In addition, crosstalk between microglia and reactive astrocytes has the same effect. Astrocyte-released exosomes transfer PTEN-targeting miRNA into BC cells to mediate PTEN downregulation, resulting in CCL2 upregulation and recruitment of microglia and macrophages. Microglia promote colonization of brain tissue by BC cells in a Wnt-dependent way.
Bypassing the BBB and BTB
Scientists have made significant advances in their understanding of the biology of the BBB in recent decades. 47 The BBB is a neurovascular unit (NVU) that separates circulating blood and brain tissue and is composed of endothelium capillaries, a vascular basement membrane, pericytes, and astrocytic endfeet.48,49 Endothelial cells form the impermeable BBB by surrounding astrocytes and the basement membrane. The BBB is both a physiological and biochemical obstacle that protects the brain from potentially hazardous chemicals while also maintaining homeostasis. 50 By regulating ions, the BBB creates a stable microenvironment for neuronal function. However, the BBB also limits the transport of therapeutic agents to the brain, making systemic therapies less effective in treating BM than in treating other types of cancer. As BM develops from BC or other cancer cells, the BBB is disrupted, and a BTB is formed. 51 Although the structure is damaged, a BTB can impede the transport of anticancer medicines to brain tumors, leading to poor treatment results. Recent advances in scRNA-seq of NVU cells have provided distinct cell-specific transcriptional profiles of the BBB that have been previously unknown. 15 Undoubtedly, single-cell analysis of the BTB formed during the process of BM development will reveal more unique characteristics of the NVU and produce new treatment strategies.
Drugs cross the BBB/BTB through different mechanisms, which mainly include paracellular and transcellular pathways; AMT, RMT, CMT, and efflux transporters. 52 The dysregulation of transcellular movement involving heterogeneous changes has been observed in BTB transport pathways. Disruption of BBB tight junctions is most common in the BTB endothelium. The tumor vasculature becomes progressively heterogeneous as BCBM progresses. Both preclinical and clinical studies have shown the heterogeneity of BTBs. The permeability of the BTB is affected by its structural changes. BTB permeability was found to be significantly variable in more than 2000 BCBM cases. 53 Gril et al. found that reactive S1P3 signaling in astrocytes influenced BTB permeability in BCBM. The 231-BR BM model showed increased BTB permeability due to increased S1P3 expression and production of interleukin 6 and CCL2 by astrocytes, attenuating endothelial cell adhesion. 54 The BBB was more permeable in a BCBM model established using SUM190-BR3 and JIMT-1-BR3 cell lines than in that established with the 231-BR-HER2 cell line. 55 The BBB was permeable to doxorubicin and T-DM1 in a BCBM model (human BT474) generated by intracranial injection, but concentrated ultrasound-induced BTB rupture greatly improved drug delivery. 56 Brain uptake of nanoparticles and nanoparticle efficacy differed in three BCBM models established with BT474 cells and intracranial, intravenous, or intracardial injection. 57 Sodium-dependent NLS1 expression in patient-derived xenograft BM models was diminished, and the BBB was damaged in a heterogeneous manner. 58 The effect of cancer on the BBB/BTB is unique to a tumor subtype; for example, TNBC frequently leads to BBB disruption, but the BBB tends to be sustained in HER2-positive BC. Compared to BM that develops from other BC subtypes, BM originating from HER2-positive BC leads to significant increases in GLUT1 and BCRP levels. 59 Lyle et al. established a SUM190-BR3 experimental inflammatory BCBM model system. On the basis of this model, desmin+ pericytes and laminin α2 were identified as potential targets for increasing chemotherapeutic efficacy. 60 Positron emission tomography scans have suggested increased accumulation of lapatinib and trastuzumab in BCBM. 61 BTB leakage may lead to greater drug entry into the brain; for example, the accumulation of trastuzumab in human and mouse BM models has been confirmed. 62 Gril et al. investigated how a biparatopic anti-HER2-ATC antibody–tubulysin conjugate (bHER2-ATC) crossed the BTB. In mouse models, bHER2-ATC in BCBM was found to be distributed in a paracellular transport-independent manner, implying that endothelial pathways may be important for drug penetration. 63 Novel BBB-disrupting approaches are urgently needed to improve the delivery of therapeutic drugs into the brain.
Exosomes and BCBM
Exosomes are small extracellular vesicles (30–150 nm in diameter) secreted by many different cell types, including BC cells. Exosomes are composed of a lipid bilayer and carry various functional molecules, such as lncRNAs, miRNAs, and proteins, which mediate complex cell–cell communication. 64 Intercellular communication is a key feature of tumor development and metastasis. Tumor cells are known to release more exosomes than normal cells, and tumor-derived exosomes have shown a profound ability to change microenvironments. 65 The unique characteristics of exosomes, such as their nanosize, ability to transport cargo to various cells, high biocompatibility and affinity, and ability to cross the BBB, make them suitable for a wide range of applications, such as anticancer therapy and drug delivery systems.66–68 Exosomes are important in the bilateral communication between tumors and nonmalignant cells in BC. 69 Exosomal miRNAs and lncRNAs have been shown to affect the transcriptome of receptor cells and promote BC metastasis. 70 They can be used as biomarkers for tumor prognosis and diagnosis and for targeted therapeutics. Exosomes are involved in the entire BCBM process, including disruption of the BBB and establishment of a brain metastatic microenvironment.
Chen et al. used a lentiviral vector to isolate exosomes from MSCs, and MSC-derived exosomes can cross the BBB. The results of this study showed a positive synergistic effect of exosomes and carboplatin in a BC mouse model, suggesting a potential therapeutic approach for BCBM patients. 71 Morad et al. found that exosomes derived from tumor cells disrupted the BBB through transcytosis in BM, and this finding was applied to the development of a drug delivery system that can cross the BBB and exert therapeutic effects in BM. 72 Exosomes secreted by BC adipocytes promote BC cell growth by activating the Hippo signaling pathway. 73
CEMIP (a Wnt-related protein) was found to be abundant in BC-derived exosomes and to promote BM. A proinflammatory vascular niche was induced by BM-promoting cytokines and chemokines in secreted CEMIP-carrying exosomes. CEMIP was identified in brain tissue-derived exosomes from BCBM patients. CEMIP overexpression in primary and metastatic tumors has been linked to BM progression and poor prognosis. These findings indicate that targeting exosomal CEMIP may be a promising approach for BM treatment. 74 The highly dynamic feature of the cytoskeleton in cancer cells during metastasis makes cytoskeletal proteins attractive targets for cancer treatment. Fazakas et al. 75 found that BC-derived exosomes increased the adhesive strength between cancer cells and brain endothelial cells. Arnold et al. found that overexpression of tubulin tyrosine ligase like 4 (TTLL4) in BC cells significantly improved polyglutamylation of β-tubulin, which changed exosome homeostasis. TTLL4-derived exosomes may facilitate the establishment of a premetastatic niche for BC cells by influencing the BBB. 76 Annexin II is one of the most abundant proteins in exosomes, particularly exosomes derived from malignant cells. Exosome-associated Annexin II is involved in angiogenesis and BCBM, and it may serve as a diagnostic biomarker and potential therapeutic target in BCBM. 77
Camacho et al. 78 found that nonmetastatic BC cells internalized BM-derived exosomes, suggesting that exosomes play roles in BM. The tGLI1 transcription factor promotes BCBM by activating astrocytes and cancer stem cells (CSCs) in the microenvironment. 79 Exosomal miRNA-mediated intercellular communication plays an important role in priming astrocytes for the formation of BCBM. It has been demonstrated that exosomal miRNAs regulate tumor angiogenesis and metastasis. For example, ZO-1 is a key endothelial cell tight junction protein, and exosomal miR-105 promotes cancer cell migration by targeting ZO-1. Zhou et al. 80 found that exosomal miR-105 could destroy ZO-1 and BBB integrity to promote metastasis in brain metastatic TNBC cells and xenograft tumor models. Zhou et al. showed that in endothelial monolayers, exosome-mediated transfer of cancer-secreted miR-105 efficiently destroys the tight junction protein ZO-1 and the integrity of these natural barriers against BM. Overexpression of miR-105 induces metastasis and vascular permeability in distant organs including the brain. miR-105 can be detected in the circulation at the premetastatic stage, and its levels in the blood and tumor are associated with ZO-1 expression and metastatic progression in early-stage BC. 80 Furthermore, exosomes can cross the BBB via transcytosis to help primary BCs metastasize into the brain. 72 BC cell-derived exosomal miR-181c induces an increase in BBB permeability by disrupting tight junctions to promote BCBM development. MiR-181c downregulates PDPK1 to disrupt the BBB and increase BBB permeability, which promotes the formation of BCBM. 81 Zhang et al. found that astrocyte-secreted exosomes containing miRNAs downregulate PTEN, increasing metastatic tumor cell proliferation and BCBM formation. Exosomal miR-19a transferred from astrocytes to BC cells is critical for cancer PTEN downregulation and BM. The results suggested that miRNAs may modulate the interactions of cancer cells and brain cells to produce a microenvironment conducive to the development of BCBM. 38 Cho et al. found that miR-4516 deficiency from exosomes derived from cancer-related fibroblasts is associated with TNBC progression. This result suggested that miR-4516 could be used as a promising target for TNBC therapy. 82 Fong et al. 83 found that primary BC-derived exosomes containing miR-122 reduced glucose uptake by normal cells, thereby promoting BM through improved nutrient utilization. Their results indicate that miR-122 can modulate the BM microenvironment and is a promising biomarker for early BCBM detection.
Watabe et al. found that lncRNA X-inactive specific transcript (XIST) loss promotes BCBM by increasing tumor cell stemness and aggressiveness. XIST loss in tumor cells induced local immune suppression via tumor-derived exosomal miR-503, converting microglia to the M2 phenotype. The lncRNA XIST plays an important role in BCBM by regulating tumor cells and the microenvironment, and the XIST-related pathway may be a useful target for treating BM. 84 Cao et al. found that exosomes derived from highly metastatic cells promoted BC cell invasion and metastasis in preclinical research. The lncRNA GS1-600G8.5 was overexpressed in BCBM cells. Exosomes with GS1-600G8.5 loss could not promote cancer cell crossing the BBB. This result suggested that BCBM cell-derived exosomes disrupt the BBB via the lncRNA GS1-600G8.5. 85 Although critical players have been identified in the BCBM of these exosomal miRNAs, the molecular mechanisms of their role in BM remain elusive.
MiRNAs and lncRNAs in BCBM
MiRNA
As noted above, exosomal noncoding RNAs (ncRNAs) may be crucial markers for diagnosis, prognosis, and therapy prediction. The most studied exosomal ncRNAs to date are miRNAs and lncRNAs. MiRNAs are small ncRNA molecules that negatively modulate gene expression by inhibiting target mRNA translation or degradation. Almost 50,000 papers on miRNA and cancer have been published to date. As upstream of oncogenes and tumor suppressor genes, miRNAs are involved in the regulation of all steps of BCBM formation, from EMT to invasion, intravasation, extravasation, and colonization in the brain. In the past decade, BMs have attracted much attention with the discovery of miRNAs inducing tumor metastasis. MiRNAs are thought to be promising therapeutic targets for BCBM 86 (Figure 3).

The role of miRNAs and lncRNAs in the formation of BCBM. For example, (a) miR-1258 decreased MMP9, cyclooxygenase-2 and EFGR by inhibiting heparanase, resulting in decreased permeability; (b) downregulation of miR-202-3p increased MMP-1 and disrupted tight junctions; (c) downregulation of miR-509 increased RhoC and TNF-α, resulting in decreased permeability; (d) downregulation of XIST activated EMT and MET, resulting in stemness, evasion, and migration, increased miR-503 levels and induced microglial polarization to promote BCBM. (e) Lnc-BM interacts with JAK2 to activate STAT3, leading to the activation of ICAM1 and CCL2 and inducing CCL2-dependent macrophage recruitment to BCBM.
Many studies have shown that miRNAs are specifically implicated in the development of BCBM. For example, the level of miRNA-7 is significantly downregulated in BC cell-derived CSCs that metastasize to the brain. Specifically, Okuda et al. 87 found that miRNA-7 suppressed BCBM by regulating downstream targets of KLF4. MiR-1258 was reported to act as a tumor suppressor by inhibiting heparanase, which was significantly decreased in BCBM. 88 Heparanase is important in cancer progression and has been shown to promote BCBM by modulating the downstream targets MMP9, cyclooxygenase-2, and EFGR, whereas heparanase inhibition resulted in the downregulation of these proteins. These study results suggest a novel approach for developing heparanase-based treatment for BCBM patients(Figure 3(a)).MiR-202-3p was downregulated in BCBM and had a direct effect on matrix metalloproteinase-1 (MMP-1). Harati et al. found that silencing miR-202-3p in BC cells increased the MMP-1 level and disrupted tight junctions, increasing the ability of tumor cells to cross the BBB. This research indicated that the miR-202-3p/MMP-1 pathway may be a promising target for BCBM therapy 89 (Figure 3(b)). MiR-509 is highly expressed in primary BC, but it is significantly reduced in BM. The upregulation of RhoC and tumor necrosis factor alpha (TNF-α) has been directly related to the downregulation of miR-509. 90 Specifically, miR-509 inhibited BM progression by reducing RhoC levels, thereby decreasing the migration of tumor cells. MiR-509 has also been found to indirectly inhibit the TNF-α-induced increase in BBB permeability. This result suggests that miR-509 suppresses BM through both pathways by targeting RhoC and preventing TNF-induced BBB penetration (Figure 3(c)).
MiR-802-5p and miR-194-5p have been identified as promising markers for the early detection of BM, indicating that their detection in liquid biopsy samples may be a novel approach for predicting the risk of BCBM. 91 MiR-211 was found to be a prognostic marker of BM both in TNBC mice and patients. 92 High levels of miR-211 promote tumor cell colonization in the brain by increasing BBB permeability and tumor cell stemness. MiR-211 drives brain colonization via the SOX11/NGN2 axis. High miR-211 levels are associated with BCBM and a poor prognosis in TNBC patients.
Wyss et al. found that the increase in PDGF levels in the brain triggered by activation of the HIF1 signaling pathway and disruption of the miRNA let-7d promoted the development of BM in preclinical BCBM models. These findings suggest a new treatment strategy for BCBM involving the pharmacological inhibition of the PDGF receptor. 93 Crossing the BBB of tumor cells is a key event in the formation of BM. Harati et al. 94 found that miR-101-3p could inhibit BC cell transmigration through the brain endothelium. MiR-101-3p expression is downregulated in BCBM cells. Downregulation of miR-101-3p increased BC cell transmigration by regulating COX-2-MMP1 signaling and degrading claudin-5 and VE-cadherin. It was suggested that miR-101-3p could be a potential therapeutic target for BCBM patients.
Although these pioneering studies suggest important roles for miRNAs in BCBM, there are still gaps in our understanding. Further research is needed to clarify the roles played by miRNAs to establish them as early biomarkers and potential targets in BCBM therapy. 95
LncRNA
LncRNAs, which are longer than 200 nucleotides in length, were discovered relatively recently. Extensive research has shown that lncRNAs are key regulators of cancer cell signaling pathways. Cancer cell invasion of tissues is the first step of tumor metastasis. Many lncRNAs have been identified as modulators of invasion and EMT; they regulate EMT via alternative pathways. 96 Lnc-BM is a lncRNA named by Wang et al. The expression of Lnc-BM was inversely related to patient survival and positively related to brain tumor recurrence. Intracardiac injection of BC cells depleted lnc-BM and reduced the burden of BM while also reducing tumor cells in blood vessels from entering the brain. 97 Wang et al. found that the expression of Lnc-BM predicted the progression of BCBM patients. In mouse models, BCBM was promoted by increased Lnc-BM expression and vice versa. JAK2 kinase activity was increased by Lnc-BM, which mediated STAT3 phosphorylation and increased the BCBM formation rate. These results show that the Lnc-BM/JAK2 pathway modulates the interaction between BC cells and the brain microenvironment, thereby promoting BCBM progression. Thus, Lnc-BM targeting may be a promising approach to the treatment of BCBM 97 (Figure 3(d)). The lncRNA XIST was inhibited in the BCBM compared with its level in bone, liver, or lung metastasis in mice. Hence, depleting XIST in BC cells resulted in an increase in metastatic brain tumor burden. Furthermore, the number of BM lesions was increased after genomic knockout of XIST in a BC metastasis model. Knocking out XIST expression increased the level of exosomal miR-503, which induced microglial polarization and thus changed the metastatic microenvironment 84 (Figure 3(e)). However, the roles played by lncRNAs in BCBM are still largely unknown. Notably, the contributions of lncRNAs to the invasion of BC cells in the brain have not been extensively characterized. 96
Molecular genetic of BCBM
The biological mechanisms underlying BM of HER2-positive and TNBC are largely unknown. The lncRNA XIST has been shown to be significantly downregulated in BM; XIST expression was lower in 48% of TNBC and 28% of HER2-positive BC samples compared with 19% of luminal A BC subtype samples. This finding suggests that EMT was suppressed and that the metastasis rate was reduced by XIST expression. 84 Both EGFR and HER-2 receptors are members of the ErbB family. In BCBM patients, EGFR mutations and overexpression of HER2/HER3 are common. 98 The HER2/HER3 association appears to be particularly important in BCBM, as it may drive BM by releasing MMPs that can damage the BBB. 99
HER2 can heterodimerize with TrkB and be activated by BDNF, implying that paracrine signaling promotes the survival of HER2-positive BCBM. 100 In BCBM, HER2 and EGFR can influence cell proliferation by modulating DNA topoisomerase I via nucleolar heparanase localization. 101 The HER2 signaling pathway activates the STAT3, Ras-MAPK, and PI3K pathways, and promotes the expression of tumor cell proliferation genes. 102 Increased HER2 signaling is linked to an increased risk of BM and reduced survival time. According to preclinical research, high HER2 expression causes a threefold increase in BM. 103 EGFR and HER2 mutations are more likely to be found in patients with BCBM. EGFR mutations are most common in the primary and metastatic tissues of patients with TNBC but are rare in HER2-positive tissues. 104
The unique molecular features of HER2-positive and TNBC tumor cells contribute to BM. Changes in the EGFR and HER2 signaling pathways are more frequent in HER2-positive and TNBC patients, and these changes have been related to a higher BM risk as well as a poorer prognosis. 12 In these two BC subtypes, XIST downregulation is more prevalent, promoting EMT and BC cell migration and specifically increasing the proclivity of circulating tumor cells to invade the brain. 84 Extravasation is more frequent in HER2-positive tumors because cells of this BC subtype bind to β4 integrin, allowing them to cross the BBB. Among BC subtype cells, TNBC cells exhibit the most CSC-like features. TNBC cells frequently overexpress genes involved in the stem cell pluripotency pathway, such as SOX2. A high level of SOX2 expression is related to a shorter survival time for patients with BCBM. In addition, the PI3k/Akt/mTOR pathway and the TP53 gene have been associated with increased BM in HER2-positive and TNBC patients. The impact of BC molecular subtypes, such as HER2-positive BC and TNBC, on BCBM development and prognosis is undeniable; however, many questions remain unanswered. Single-cell RNA sequencing (scRNA-seq) allows a better understanding of cell heterogeneity in BC and has great potential for clarifying the complex mechanisms of BM, potentially leading to new strategies for individualized treatment. 105
BM has been reported to involve a significant genetic component, with the expression of related genes either upregulated or downregulated. Many genes with increased expression and associated with BM have been identified. For example, HBEGF, COX2, and ST6GALNAC5 are mediators of cancer cell penetration of the BBB and regulation of the formation of BCBM. 106 The drivers of primary BC development, such as TP53, MLH1, PIK3CA, and KIT, are frequently mutated in BCBM. 107 Lee et al. investigated genes that are involved in BCBM. They found that 22 genes in one set were differentially expressed in BM compared with their expression in primary BC; the genes CXCL12, MMP2, MMP11, VCAM1, and MME were the most differentially expressed and distinctly upregulated in primary BC. However, the expression of two other genes in this set, SOX2 and OLIG2, was also increased in BM, indicating that these genes may play roles in metastatic colonization. These findings suggest that different genes are involved in BCBM. 107 However, additional functional validation is required to confirm the roles of these genes in BCBM. In a systematic review, Morgan et al. summarized the genes most commonly mutated in BCBM, and described their clinical significance. They highlighted the importance of collecting BM samples and analyzing the distinctions between primary BC and BM. 108
The activation of metastatic genes or the silencing of metastatic suppressor genes frequently leads to progression to BM. Mutation of metastatic genes such as MMP2 and CXCR4 may lead to abnormal protein products, which can promote tumor cell metastasis to distal organs. The expression of the COX-2 gene, which controls tumor invasion, extravasation, and metastasis, was downregulated in metastatic tissues. The RRM2, MMP1, FOXM1, BRCA1, and E-cadherin genes have also been implicated in BCBM. 109 The gene expression of nestin, prominin-1, CK5, and aSMA in BC has also been linked to BM. The patient survival rate after the development of BM has been reported to be as low as 2 months. 110 Villodre et al. 111 recently found that NDRG1 promotes BM in aggressive BC, and overexpression of NDRG1 is associated with poor clinical outcomes, which suggests that NDRG1 may be a therapeutic target for BCBM.
Cancer-related genes are typically classified as proto-oncogenes or tumor suppressor genes. Gene mutations at the nucleotide, transcriptional, or epigenetic level can cause abnormal or inhibited gene expression. CRISPR/Cas9 can be used to generate targeted mutations at every level. The CRISPR/Cas9 editing system is a powerful genome-altering tool that has shown great promise for use in cancer therapy, including BCBM. It is widely used to suppress the expression of various genes and repair mutations in genetic disorders.109,112 CRISPR/Cas9 can be used to knockout oncogenes and thus attenuate cancer development and metastasis. Scientists are using liposome-templated hydrogel nanoparticles that can penetrate the BBB to deliver CRISPR/Cas9 in vivo for cancer treatment. 113 Lipocalin2 is an oncogene involved in BC development and metastasis. CRISPR/Cas9-mediated knockout of lipocalin2 expression resulted in cell migration inhibition because EMT was suppressed, but it did not decrease the cell proliferation rate. This in vivo therapy markedly decreased tumor growth. These studies show that a tumor-targeted nanolipogel system can be used in vivo as a delivery vehicle for efficient and safe CRISPR-based genome editing in TNBC. 114 For example, the depletion of the E3 ubiquitin ligase UBR5 in a TNBC model via CRISPR/Cas9 editing significantly inhibited tumor growth and metastasis. 115 CRISPR/Cas9 technology has also been used to delete the YB-1 gene in CSCs. Yang et al. 116 found that downregulating YB-1 reduced BC stem cell proliferation, resulting in cell cycle arrest, and inducing apoptosis and irreversible differentiation. Novel engineering strategies, such as CRISPR/Cas9, should be investigated further to determine their usefulness in targeting BCBM because they have shown great promise in cancer treatment.
Novel therapeutic strategies for BCBM
To date, the preferred treatment option for BCBM treatment is based on localized strategies, such as surgery and/or radiotherapy. Treating BCBM with the same systemic therapy used to treat primary BC has been less effective in the past decade. However, the rapid development of anti-HER2 drugs has given new hope to BCBM patients. 117 Scientists have developed many anti-HER2 drugs, such as tyrosine kinase inhibitors, monoclonal antibodies, and antibody–drug conjugates (ADCs). Lin et al. 118 recently published the results of a randomized controlled trial that demonstrated the intracranial efficacy of HER2-directed small-molecule inhibitors. Specifically, of the HER2-positive BM patients treated with tucatinib plus trastuzumab and capecitabine, two-thirds showed a lower risk of intracranial progression or death, and nearly one-half showed a lower risk of death. When combined with capecitabine, another tyrosine kinase inhibitor, neratinib, was shown to be highly effective in treating HER2-positive BCBM patients. 119 Yan et al. 120 recently published the results of a multicenter, phase II trial that showed the benefit of pyrotinib (a pan-Her receptor tyrosine kinase inhibitor) plus capecitabine in treating HER2-positive BCBM patients. A variety of clinical trials for BCBM therapy are currently underway.117,121
Although the results of early clinical studies on therapies targeting BTB permeability-related pathways were disappointing, promising results have been obtained in recent clinical trials. Notably, in a recent clinical trial, tucatinib, a small-molecule HER2 kinase inhibitor, was the first targeted agent discovered to enter the brain. 122 In the phase II HER2CLIMB trial, trastuzumab and capecitabine plus tucatinib were administered to treat HER2-positive metastatic BC (48% of the patients had BCBM). The median progression-free survival (PFS) was 2.2 months longer with a median OS duration increased by 4.5 months in the Tucatinib treatment group compared with the placebo group. 123 Tucatinib increased the median intracranial PFS duration by 4.7 months and the median OS duration by 6.1 months in 291 BCBM patients. Tucatinib also increased the median PFS by 5.0 months and the median OS duration by 5.3 months in 66 BCBM patients who chose delayed radiotherapy. 118 The role played by the BBB and BTB in this therapy, however, remains unknown. The mechanisms of drug entry into brain tumors are poorly understood, and additional well-designed preclinical and clinical imaging studies are needed.
As discussed above, the BBB and BTB are impediments to therapeutic intervention. Therefore, additional new BBB disruption techniques are needed to improve the permeability of drugs to metastatic tumors in the brain. Invasive and noninvasive approaches for improving antitumor agent delivery across the physical, cellular, and molecular barriers of the BBB and BTB are being developed as discussed in this review.
Given the poor prognosis of BCBM in patients receiving currently available treatments, the development of novel and more effective therapies is urgently needed. Notably, no FDA-approved treatments are specifically available for the treatment of BCBM. 17 Surgery and radiotherapy are the conventional cancer therapies applied for BCBM patients. Systemic therapy, such as chemotherapy and targeted therapy, is a challenging to administer in BCBM treatment because of the BBB. To address the challenges associated with BCBM, basic and clinical research has been directed to developing novel drug targeting and delivery approaches to enhance drug efficacy in the brain. 50
Focused ultrasound
Focused ultrasound (FUS) is a special noninvasive approach for safely and reversibly opening the BBB/BTB and increasing the accumulation of antitumor agents in metastatic brain tumors. FUS can be used to specifically target brain areas and damage the BBB/BTB. 56 Low-intensity FUS can cause microbubbles to oscillate, which increases vessel pressure, expands tight junctions, and increases membrane permeability. 124 The degree of BBB/BTB opening is proportional to the degree of drug permeation. Numerous preclinical studies have shown that FUS can be used to increase the amounts of several systemically administered drugs that penetrate the BBB/BTB and are thus delivered to brain tumors by more than fourfold. 125 Applying FUS in a preclinical model, Wu et al. studied the transport and therapeutic efficacy of pegylated liposomal doxorubicin (PLD) in BCBM. The results showed that short-term FUS treatment significantly increased the amount of PLD delivered into brain tumors and that PLD + FUS treatment alone effectively inhibited tumor growth. An immunohistochemical analysis confirmed the effect of PLD + FUS on BCBM. Short-term FUS applications can improve nanomedicine delivery and BCBM therapy.126,127 Low-intensity FUS treatment induced increased permeability of the BBB/BTB to increase doxorubicin accumulation by sevenfold and ADC ado-trastuzumab emtansine T-DM1 accumulation by fivefold in a HER-2-positive BCBM preclinical model. 56 Arsiwala et al. investigated the effects of FUS to facilitate the delivery of trastuzumab through the BBB/BTB in a HER2-positive BCBM model. The tumor volume of the FUS + trastuzumab group was significantly decreased after trastuzumab was administered via the tail vein, followed by FUS. 124 FUS is a novel method for increasing antitumor agent penetration into the brain by promoting the reversible opening of the BBB/BTB. Further functional and clinical trials are needed to investigate the FUS approach in the treatment of BCBM (Figure 4).

Novel approaches to overcome the BBB/BTB. (a) FUS; (b) (MTH) for BBB transport; (c) nanocarriers. The details of the techniques are shown in the text.
Molecular Trojan horse
The MTH approach depends on monoclonal antibodies or engineered peptides bound to endogenous receptors for RMT delivery of biologics through the BBB. 52 Most chemotherapeutic and targeted drugs are large molecules and cannot penetrate the BBB in adequate therapeutic quantities. By attaching these drugs to MTHs, the so-called bifunctional molecules are formed, which can promote antitumor drug penetration of the BBB by binding to receptors on endothelial cells. 128 Different classes of high-molecular-weight biologics have been fused with different MTHs and delivered into the brain. 52 For example, antitumor agents fused to IgG monoclonal antibodies can cross the BBB mediated by a BBB receptor, such as the transferrin receptor (TfR); in this case, an anti-TfR monoclonal antibody is the MTH, and the antitumor agent-anti-TfR fusion molecule can be delivered into the brain. 129
Schackert et al. found that macrophages derived from circulating monocytes can penetrate metastatic brain tumors with an intact BBB. In a follow-up study, Choi et al. 130 aimed to determine whether systemic injection of nanoparticle-laden macrophages, acting as cellular Trojan horses, can infiltrate the BCBM. They found that this Trojan horse specifically delivered various nanoparticles across the BBB in a BCBM model. This delivery approach solves challenges to cancer nanotherapy posed by the tumor microenvironment. T cells are recruited by CDK4/6 inhibitor-treated BC cells via metabolic stress-induced chemokines, suggesting a Trojan horse strategy for cancer immunotherapy.131,132 Although the MTH method shows promise for the delivery of large molecules for BCBM treatment, widespread distribution throughout the body often limits the therapeutic response. Therefore, additional research is needed to increase the specificity and selective tumor-targeted delivery of anticancer agents via Trojan horse peptides. ANG1005 is a novel taxane derivative that consists of three paclitaxel molecules. It was designed to penetrate the BBB/BTB barriers via transcytosis mediated by LRP1, which is highly expressed on endothelial cells in the BBB. 133 ANG1005 infiltrates the cell via LRP1-mediated endocytosis, and then, lysosomal esterases cleave paclitaxel from the peptide backbone. ANG1005 uptake by the brain was found to be higher than that of paclitaxel in preclinical models. 134 A multicenter phase II study was conducted with BCBM and leptomeningeal carcinomatosis patients. Every 3 weeks, 600 mg/m2 of ANG1005 was administered intravenously. ANG1005 treatment led to significant antitumor activity in the brain and showed clinical benefit, and a phase III study is currently underway. 133
Antibody–drug conjugates
Trastuzumab emtansine (T-DM1) is a HER2-targeting ADC that consists of the cytotoxic agent emtansine (DM1) conjugated to trastuzumab that delivers DM1 to cancer cells, leading to inhibited tubulin polymerization and cell death. 117 Trastuzumab deruxtecan (T-DXd) was the second ADC to be approved for use in metastatic BC patients who had at least two types of anti-HER2 treatment. 135 Endocytosis of a biparatopic anti-HER2 ADC into endothelial cells in vitro has been demonstrated without the need for conjugation to a known transcytotic ligand. 63 Despite the limited paracellular permeability observed in preclinical research, ADCs have significantly inhibited BCBM formation, indicating that delivering a small number of highly effective agents into the brain may be a promising approach. 15
Nanomedicines
The enhanced permeation and retention effect is the main hypothesized benefit of using nanocarriers for cancer therapy. 136 Cancer therapy has been remarkably improved over the past few years because of the development of different antitumor agents at the nanoscale. 137 More recently, biomaterial-based nanodrugs have been developed and applied in preclinical studies and clinical trials as cancer immunotherapies. 138 Nanoparticles used in targeted drug delivery systems exhibit unique advantages, such as reliable delivery, sufficient loading capacity, nanosized, and drug-loading plasticity. 137 Nanodrugs have increased the efficacy and reduced the toxicity of parent drugs in clinical trials of BC treatment. 139 Nanoparticle-mediated targeted delivery of chemotherapeutic drugs to BM is currently among the most frequently used approaches. Different nanoparticles, such as polymeric nanoparticles, liposomes, and micelles, have been investigated for their potential as drug delivery systems because they can cross the BBB. 16 These new drug delivery methods can be used to gain spatial and temporal control over BCBM treatment. Several nanoparticle-based strategies have been evaluated for their ability to enhance drug transport across the BBB. 47 However, studies have shown very low levels of nanoparticle accumulation in the brain. Although various promising nanoparticles are continuously being developed, the rules for designing BBB-/BTB-penetrable nanoparticles must first be established. 140 Li et al. developed a nanomedicine system to deliver imaging and therapeutic agents to metastatic BC brain tumors, but these agents did not cross the BBB. Therapy with doxorubicin-loaded nanoparticles significantly reduced the growth of metastatic BC brain tumors. 141 Mittapllli et al. developed a hyaluronic acid–paclitaxel nanoconjugate that passively diffuses through the BTB. The effect of the nanoconjugate in vivo was evaluated using a preclinical model of BCBM. The results showed that the OS was much longer in the mice given this hyaluronic acid–paclitaxel nanoconjugate than in the control mice. 142 Graphene-based nanomaterials (GBNs) have the advantages of target selectivity, easy functionalization, and high-drug-loading capacity, making them potential drug carriers. 143 Recent studies have shown that GBNs are capable of passing through the BBB 144 and can be used as carriers to facilitate large molecule transport across the BBB, resulting in drug accumulation at metastatic brain lesions. GBNs conjugated with specific drugs have been used to treat BCBM. Moreover, the combination of nanoparticles with tumor-penetrating peptides decreased BCBM progression in a preclinical model. 145 Only a few nanodrugs are being administered to BCBM patients, and they are still in the early stage of clinical application. 139
Nanoparticles can reestablish the effectiveness of conventional chemotherapy by improving permeation and retention, thereby reducing side effects, extending treatment windows, and shortening drug delivery intervals. However, the translation of nanomedicines has not been as successful as originally anticipated. Moreover, although clinical benefits have been demonstrated, the number of nanomedicines available for BCBM treatment remains limited. 146
Immunotherapies
Various lines of evidence have shown that tumor cells hijack immune regulatory mechanisms in the brain to perpetrate their survival and development. 147 The development of immunotherapy with immune checkpoint inhibitors and targeted therapy has greatly improved the prognosis of various cancers. Immunotherapy is one of the most promising advances in BM therapy because it stimulates the immune system to specifically attack cancer cells. Although the brain was previously considered an immune-privileged organ, BM is now thought to be a potential target of various immunotherapeutic drugs. 148 Immunotherapies have shown promise in preclinical research and produced significant clinical outcomes in BM patients. Checkpoint inhibitors are the most frequently studied immunotherapeutic agents for BM. Although checkpoint immunotherapy has been shown to be less effective in BM, some novel targeted therapies have been approved, and they have increased the median 5-year survival from 18.4% to 32.6%. 149
As previously stated,44,45 BM occurs in an environment with fewer immune cells than in primary BC tissues; therefore, a high TIL content in the BCBM is associated with better outcomes. Changing the brain immune microenvironment may be a novel strategy for treating BCBM. 150
T-cell immunotherapy with chimeric antigen receptors (CARs) is being studied as a treatment for solid tumors and metastatic brain tumors.151,152 Priceman et al. developed second-generation HER2-specific CAR T cells to treat BCBM. They also investigated the efficiency of HER2-CAR T cells in BCBM models. The results showed strong antitumor activity in orthotopic xenograft HER2-CAR models established via local intracranial delivery. This result suggested that CAR T-cell therapy may be effective in HER2-positive BCBM patients. 153 A phase I clinical trial to evaluate the effect of intraventricular CAR T-cell treatment with HER2-positive patients with brain or leptomeningeal metastasis is ongoing. 148 Several phase II clinical trials combining stereotactic radiosurgery with atezolizumab, nivolumab and pembrolizumab to increase TIL content are underway. 14 Lu et al. investigated the genomic landscape of the BCBM immune microenvironment and found that it was immunosuppressed. Therefore, targeting macrophages or plasma cells may be a novel approach for BCBM immunotherapy. THY1 and NEU2 have been found to be potential targets for BCBM treatment; furthermore, THY1, CD1B, and DOCK2 may be prognostic markers for BCBM survival. 154 However, to date, immunotherapy has not shown significant benefits for BCBM patients, in contrast to patients with metastatic melanoma or lung cancer.
Conclusions
For the past decade, effective treatment has significantly increased the life expectancy of BC patients. However, the incidence of BM has been steadily increasing as well. Unfortunately, despite improved systemic treatments, the prognosis for BCBM patients remains poor. Understanding the molecular characteristics of BCBM, as well as the development of new and more effective therapies, is urgently needed. In this review, we focused on the latest advances in understanding the molecular mechanism of BCBM and novel therapeutic strategies.
BC is molecularly heterogeneous and can be classified into several subtypes. The TNBC and HER2-positive subtypes are undeniably linked to an increased risk of BM and a worsened prognosis. To date, local management, such as surgery or radiotherapy, has been the preferred treatment option for BM. Developing effective drug delivery and systemic therapies for BCBM remains pharmacological challenges due to the highly selective permeability and protective function of the BBB. Various approaches for overcoming BBB/BTB limitations have been investigated, including FUS, nanodrugs, and MTHs, to improve drug delivery and distribution into the brain. The brain microenvironment and region-specific genomic alterations in the brain are emerging as potential targets for BCBM therapy. Furthermore, the application of novel genome-altering approaches as well as new engineering strategies such as CRISPR/Cas9 editing has resulted in an unprecedented shift in our understanding of the heterogeneity of BCBM and has provided novel insight into more effective therapeutics. New immunotherapy-based treatment strategies, such as immune checkpoint inhibitors, targeted therapies, and nanomedicines that enhance BBB penetration, may improve efficacy while limiting side effects. Furthermore, ongoing trials and prospective treatments are expected to improve outcomes for BCBM patients. Understanding the mechanism of BCBM will help us to develop additional more effective antimetastatic strategies. However, more research is needed to validate the identified gene and molecular mechanism targets in potential clinical applications. For example, CRISPR screening could be used to further link genetic mutations with phenotypic changes and ATAC-seq could be used to detect epigenetic changes in BCBM. 155 The discovery of the molecular mechanisms underlying BCBM has opened up new avenues for future research aimed at the development of novel targeted therapies. Hopefully, ongoing studies and novel research approaches will be beneficial in addressing current challenges and improving treatment strategies for BCBM patients.
Footnotes
Acknowledgements
None.