
Abstract
Remarkable progress in breast cancer treatment has improved patient survival, resulting in an increased incidence of brain metastasis (BM). Current treatment options for BM are limited and are generally used for palliative purposes. Historically, local treatment, consisting of radiotherapy and surgery, is the standard of care due to delivery limitations of systemic treatments through the blood–brain barrier. However, as novel biological mechanisms for tumors and BM have been discovered, several innovative systemic agents, such as small-molecular-targeted therapy and immunotherapy, have begun to change the treatment paradigm. In addition, efforts to maximize antitumor effects have been attempted using combination therapy, informed by tumor biology. In this comprehensive review, we will highlight various clinical trials investigating the treatment of BM in breast cancer patients, discuss presently available treatment options, and suggest potential directions of future therapeutic targets.
Introduction
Breast cancer (BC) is the second most common cancer which metastasizes to the brain. 1 Among patients with metastatic BC, up to 30% eventually develop brain metastasis (BM). 2 The incidence of BM is associated with molecular subtypes of BC and is likely to be higher with earlier occurrence in patients with human epidermal growth factor receptor 2 (HER2)-positive and triple-negative (TN) BC.3–7 In patients with metastatic HER2-positive and TNBC, the incidence of BM is 11–48% and 25–46%, respectively, while in patients with luminal A and B, incidences are 8–15% and 11%, respectively.7–13 Patients with BM experience neurological dysfunction 14 and have worse prognoses by molecular subtypes.15,16 The reported median overall survival (OS) for patients with luminal and HER2-positive disease was 7.1–18.9 and 13.1–16.5 months, respectively, while for patients with TNBC, OS was 4.4–4.9 months.6,17 Therefore, management of patients with BM from BC is a significant issue directly related to quality of life and survival. Moreover, the tumor subtypes should be considered when treating BM as well as when designing new clinical trials.
BC treatment has dramatically improved during recent decades, and effective treatment of extracranial disease has prolonged survival. 18 Based on the report by Sperduto et al. that the median interval from primary BC to BM in HER2-positive patients was 35.8 months, 4 the risk of developing BM would be increased as patients survive longer. Furthermore, intracranial spread is insufficiently controlled, also resulting in increased incidence of BM.8,19,20 After the introduction of trastuzumab, accelerated incidence of BM in HER2-positive patients has become common.21,22 Although surgical resection followed by radiotherapy could be curative for a small, solitary BM, 23 current treatment options for large or multiple BM remain mainly palliative. Therefore, effective treatments for BM continue to be an unmet medical need.
Historically, patients with BM were treated with whole-brain radiotherapy (WBRT) or surgical resection. 8 However, due to concerns regarding WBRT-induced neurocognitive decline, stereotactic radiosurgery (SRS) is an alternative for limited BM.24,25 In addition, following the emergence of innovative targeted therapies and immunotherapies, the paradigm of BM treatment is beginning to shift from local to systemic treatment. Clinical trials investigating combinations of these are also increasing.
In this article, we summarize current local treatments for BM and review clinical trials of systemic therapies, mainly focusing on BM in HER2-positive and TNBC. We then highlight different systemic therapies that have been used in combination with radiotherapy (RT). Our discussion of ongoing clinical trials may encourage the development of new management strategies for BM.
General local treatment for BM
Currently, local treatment options for BM consist of surgery, SRS, WBRT, or combinations of these, regardless of the primary solid tumor. Many factors are considered during treatment selection, including patient preference, other comorbidities, and the number and volume of BMs. 26 However, BM is classified into limited or extensive disease according to the number and volume of lesions, and treatment strategies are selected based on this classification. The definition of limited BM in National Comprehensive Cancer Network guideline is as follows: ‘Limited’ brain metastases defines a group of patients for whom SRS is equally effective and offers significant cognitive protection compared with WBRT. 27 In general, one to four BMs are considered limited, 28 and for these BMs, surgical resection and SRS are available local treatments. Patients with extensive BM or with symptomatic BM and uncontrolled extracranial disease could be candidates for WBRT, aimed at palliation; the median OS for patients receiving WBRT for BM from BC is approximately 4.2 months. 29
There is disagreement whether WBRT after complete surgical resection or SRS is necessary to eradicate microscopic disease at the primary BM or distant intracranial sites. Several randomized trials exploring this demonstrated that omission of WBRT resulted in significantly increased intracranial relapse (1-year local control rate was approximately 70% versus 90–100%) but did not affect OS except one trial (Table 1).24,30–32 Incidence of radionecrosis in those studies was 0.6–6.7% and 1.1–4.6% in the groups without and with adjuvant WBRT, respectively. Chang et al. reported the extremely high OS (63%) in the SRS-alone group, maybe due to more use of salvage therapies (87%) than other studies. 24 Interestingly, in an individual patient data meta-analysis, younger patients (⩽50 years old) with SRS alone had significantly improved survival than those with SRS+WBRT (10 versus 8.2 months; p = 0.04), with no difference in distant intracranial failure. 33 The inferior survival of SRS+WBRT in this age group was thought to be due to side effects of WBRT, without a positive effect on distant brain relapse rates. In addition, although Aoyama et al. reported no difference in neurocognitive testing after treatment between groups, 30 WBRT in patients with limited BM is not used due to the high risk of neurocognitive decline.31,32 Therefore, treatment guidelines recommend that SRS alone is preferred in patients with limited BM, while WBRT should be reserved for salvage.27,34,35 An ongoing phase II study [ClinicalTrials.gov identifier: NCT02898727] is assessing the salvage WBRT rate within 1 year after surgical resection, SRS, or both, in HER2-positive patients with 1–5 BMs (Table 2). This study has two purposes: (a) investigate tumor control after surgery and/or SRS; and (b) evaluate BM development at new sites when WBRT is not given.
Prospective randomized clinical trials for the treatment of brain metastases in breast cancer.

Primary tumors were not confined to breast cancer.
Bayesian probability of a higher neurocognitive decline in SRS+WBRT than SRS alone.
Defined as a ⩾50% volumetric reduction.
Defined as follows: (a) no progression of CNS per RECIST 1.1; (b) no worsening of tumor-related neurological signs or symptoms; (c) no corticosteroid dose increase; and (d) absence of extra-CNS disease progression.
Afatinib alone versus TPC, p = 0.37; afatinib+vinorelbine versus TPC, p = 0.63.
BM, brain metastasis; CNS, central nervous system; CT, chemotherapy; HER2, human epidermal growth factor receptor 2; HVLT-R, Hopkins Verbal Learning Test, Revised; OP, operation; ORR, objective response rate; PD, progressive disease; RECIST, Response Evaluation Criteria In Solid Tumors; RT, radiotherapy; SRS, stereotactic radiosurgery; TPC, treatment of physician’s choice; TT, targeted therapy; WBRT, whole-brain radiotherapy; WHO PS, World Health Organization performance status.
Ongoing clinical trials associated with radiotherapy for the treatment of brain metastases in breast cancer.
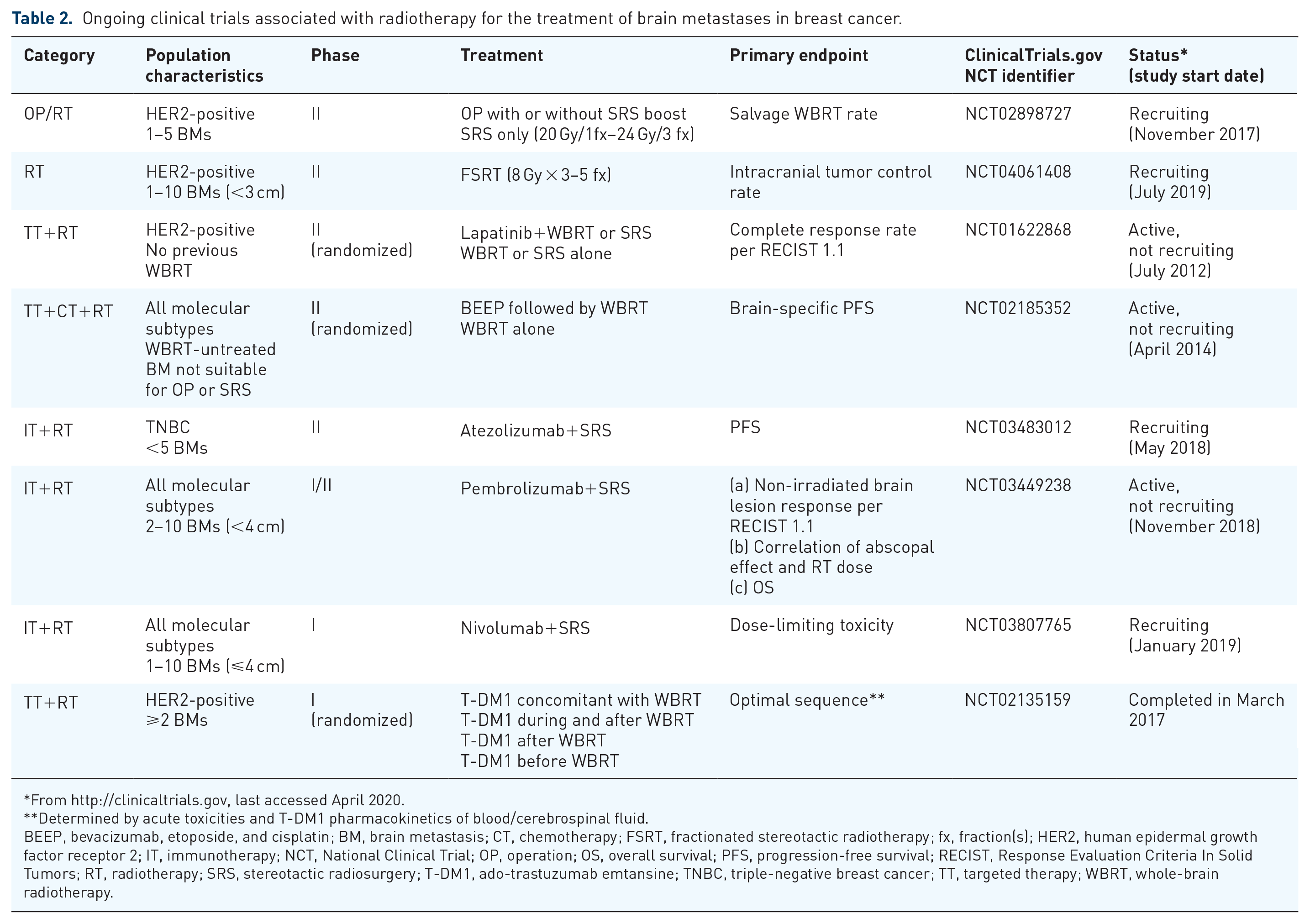
From http://clinicaltrials.gov, last accessed April 2020.
Determined by acute toxicities and T-DM1 pharmacokinetics of blood/cerebrospinal fluid.
BEEP, bevacizumab, etoposide, and cisplatin; BM, brain metastasis; CT, chemotherapy; FSRT, fractionated stereotactic radiotherapy; fx, fraction(s); HER2, human epidermal growth factor receptor 2; IT, immunotherapy; NCT, National Clinical Trial; OP, operation; OS, overall survival; PFS, progression-free survival; RECIST, Response Evaluation Criteria In Solid Tumors; RT, radiotherapy; SRS, stereotactic radiosurgery; T-DM1, ado-trastuzumab emtansine; TNBC, triple-negative breast cancer; TT, targeted therapy; WBRT, whole-brain radiotherapy.
As mentioned previously, WBRT better controls intracranial disease, but is not widely used, especially in patients with limited disease, because of possible neurocognitive decline and lack of OS benefit. However, in one report, WBRT-induced tumor shrinkage resulted in better survival and preservation of neurocognitive function. 38 Li et al. concluded that neurocognition was adversely correlated with BM progression, rather than WBRT. As an alternative approach, prospective studies of patients who underwent hippocampal-sparing WBRT revealed that functional preservation was achieved by reducing the bilateral hippocampi radiation dose.39,40 Furthermore, Gondi et al. presented results of a phase III trial (NRG CC01), demonstrating that hippocampal-sparing WBRT plus memantine better preserved neurocognitive function than non-hippocampal sparing, with similar intracranial control and survival. 41 Several retrospective studies have reported improved survival after up-front WBRT in certain patient groups, including those with late-onset BM from a primary BC or a BC-specific graded prognostic assessment score of 0–2.16,42
SRS delivers a single fraction of high radiation dose characterized by a very rapid dose fall-off around the BM. This confers the advantage of sparing normal brain tissues and expands the role of SRS in patients with limited BM, replacing WBRT. Even, SRS has frequently been used in patients with BMs beyond four in real practices, and some case series show a wide range of local control rates. 43 Recently, a large multi-institutional retrospective study of 2089 patients analyzed treatment outcomes of initial SRS for BM. 44 The median OS for patients with 2–4 BMs (n = 882, 42%) and 5–15 BMs (n = 212, 10%) was 9.5 and 7.5 months, respectively, showing no significant difference. The 1-year distant brain failure was 41% for 2–4 BMs and 50% for 5–15 BMs, respectively. JLGK0901 was a prospective observational study that enrolled 1194 patients with 1–10 BMs receiving SRS alone. 45 Patients with 5–10 BMs had a similar OS as those with 2–4 BMs; there was no difference in acute toxicities. However, interpretation of these findings should be taken cautiously, as these studies were not randomized controlled studies. Future prospective studies are therefore needed to set appropriate indications for SRS alone.
Fractionated stereotactic radiotherapy (FSRT) introduces the radiobiological advantages of fractionation to SRS, including lower toxicity to normal tissues, and is an option for treatment of large BMs or those close to critical normal tissues and not amenable for SRS. A systematic review of 10 retrospective or prospective studies, concluded that FSRT provided a local control rate of 80% at 1 year and 69% at 2 years. 46 The rate of radionecrosis after FSRT for large BMs (median 1.7–4.4 cm in diameter or 2.04–17.5 cm 3 ) was 0–9%. 47 Considering the large volumes that were irradiated, these toxicity rates might be acceptable. A phase II study [ClinicalTrials.gov identifier: NCT04061408] is enrolling HER2-positive patients with 1–10 BMs, predicting better local control and lower radionecrosis after FSRT (Table 2).
In summary, there are currently no strict guidelines for local treatment strategies for patients with BM. Physicians should carefully weigh the benefits of local treatment based on individual patient and disease characteristics. Further studies are needed to select patients who will benefit from local treatments and to overcome the limitations of current options.
Advancement of systemic treatments for BM in BC
The brain is shielded from the body’s bloodstream by a physical barrier, the blood–brain barrier (BBB), which is formed by endothelial cells and their tight junctions, a thick basement membrane of pericytes, and astrocytic end-foot processes. 48 It acts as a selective filter, limiting the penetration of most cytotoxic agents, resulting in low efficacy of systemic agents. In fact, only a few drugs could penetrate the BBB.48,49 As BM develops, the BBB integrity weakens and lipophilic drugs could pass through the BBB more easily, but the efflux pumps of the BBB bring them out again. 50
Generally, because of the limitations of crossing the BBB, as well as the poor prognosis of BM and potential central nervous system (CNS) toxicities, many clinical trials investigating systemic treatments for metastatic BC have excluded patients with BM. 51 However, development of systemic treatments has improved the control of extracranial disease, and as survival increases, the necessity of clinical trials in patients with BM is emerging. Various approaches to enhance drug delivery through the BBB have been attempted, including: (a) designing new drugs with low molecular weight; (b) modifying existing agents; (c) implementing intermittent high-dose drug regimens with alternative schedules; and (d) disrupting the BBB using chemical or mechanical means. 52
In the following sections, we will discuss the advancement of systemic treatment options for BM in BC, especially in HER2-positive or TNBC. Table 1 lists prospective randomized studies enrolling only patients with BM, and Tables 2 and 3 list systemic therapies currently being developed, with the hope they will provide new insights for BM management.
Ongoing clinical trials of systemic treatment alone for the treatment of brain metastases in breast cancer.

From http://clinicaltrials.gov, last accessed April 2020.
Including trastuzumab and/or lapatinib, pyrotinib, and tucatinib.
Defined as the best overall response rate of complete response, partial response, or stable disease in the CNS, reported as sustained for ⩾24 weeks.
One of the following seven agents: eribulin, ixabepilone, vinorelbine, gemcitabine, paclitaxel, docetaxel, or nab-paclitaxel.
BEEP, bevacizumab, etoposide, and cisplatin; b.i.d., bis in die (twice daily); BM, brain metastasis; CNS, central nervous system; CT, chemotherapy; HER2, human epidermal growth factor receptor 2; ITM, intrathecal methotrexate; LMS, leptomeningeal seeding; NCT, National Clinical Trial; OP, operation; ORR, objective response rate; OS, overall survival; PD, progressive disease; PFS, progression-free survival; q.d., quaque die (four times daily); RANO-BM, Response Assessment in Neuro-Oncology Brain Metastases; RT, radiotherapy; SRS, stereotactic radiosurgery; T-DM1, ado-trastuzumab emtansine; TPC, treatment of physician’s choice; TT, targeted therapy; WBRT, whole-brain radiotherapy.
Era of new HER2-targeted therapy
Trastuzumab, the first anti-HER2 antibody, is effective at controlling extracranial disease in HER2-positive patients, and has dramatically improved survival. 53 However, due to its large molecular weight (~148 kDa), its delivery across the BBB is limited. 54 For this reason, new HER2-directed therapies are currently being developed.
Pertuzumab, a recombinant humanized monoclonal antibody (~148 kDa), binds to a different HER2 site than trastuzumab, preventing HER2/HER3 dimerization and providing complementary action when combined with trastuzumab. 55 The CLEOPATRA trial randomized metastatic HER2-positive patients with no prior chemotherapy or HER2-directed therapy into pertuzumab (or placebo)+trastuzumab+docetaxel groups. 56 Long-term follow up (median 50 months) revealed that the pertuzumab combination significantly improved OS with an absolute difference of 15.7 months [median (95% confidence interval (CI)), 56.5 months (49.3–not reached) versus 40.8 (35.8–48.3)]. Thus, pertuzumab in combination with trastuzumab and docetaxel became standard first-line therapy in this population. Despite the exclusion of patients with CNS metastases and almost similar incidence of CNS metastases in this trial, the onset of CNS metastases was delayed in the pertuzumab combination group compared with the placebo group [median 15.0 versus 11.9 months, hazard ratio (HR) 0.58, 95% CI 0.39–0.85, p = 0.005]. 57 This result shows the potential role of pertuzumab in the treatment of BM. PATRICIA [ClinicalTrials.gov identifier: NCT02536339] is a phase II study assessing the safety and efficacy of pertuzumab (loading dose 840 mg, followed by 420 mg every 3 weeks) with high-dose trastuzumab (6 mg/kg weekly) for HER2-positive patients with progressing CNS metastases after cranial RT (Table 3). In the planned interim analysis of 15 patients, the CNS objective response rate (ORR) per Response Assessment in Neuro-Oncology Brain Metastases (RANO-BM) criteria was 20%; no new safety signals were observed. 58
HER2-targeted tyrosine kinase inhibitors (TKIs) that penetrate the BBB are used in clinical practice and are being investigated in clinical trials, including: lapatinib,36,59–63 neratinib,64–67 afatinib,37,68 tucatinib,69–73 pyrotinib,74,75 and epertinib. 76 Lapatinib is an orally bioavailable and small dual TKI that binds HER2 and the epidermal growth factor receptor. 59 A phase II study of lapatinib as a single agent in pretreated patients was disappointing, with a volumetric CNS ORR of 6%. 60 However, when combined with capecitabine in a randomized phase II study, the response rate increased to 38% (Table 1). 36 LANDSCAPE, a phase II study, evaluated lapatinib+capecitabine for HER2-positive patients with previously untreated BM. 61 Surprisingly, CNS ORR (volumetric) was 65.9% (95% CI 50.1–79.5), suggesting that instead of cranial RT, up-front lapatinib+capecitabine is a feasible first-line treatment for BM in HER2-positive BC. However, this high CNS ORR should be interpreted considering that patients did not receive current, standard, first-line treatment for BM, and needs to be demonstrated in randomized control trials. Recently, a phase I study of 11 patients with CNS metastases illustrated that intermittent high-dose lapatinib (1500 mg bid) is tolerable when alternated with capecitabine. 62 The LAPTEM phase I trial assessed lapatinib+temozolomide and showed favorable safety and efficacy. 63 These novel strategies warrant further investigation.
Neratinib is an oral, irreversible TKI of the pan-HER family. 64 The Translational Breast Cancer Research Consortium (TBCRC) 022 initiated a phase II trial to investigate the efficacy of neratinib for patients with pretreated, progressive BM in HER2-positive BC. This trial consists of three cohorts: Cohort 1, neratinib monotherapy; Cohort 2, neratinib with surgical resection; and Cohort 3, neratinib+capecitabine without (3a) and with (3b) previous lapatinib treatment. In Cohort 1, 40 patients were enrolled, and 78% of patients had a history of receiving WBRT. 65 Only three patients showed a partial response in CNS lesions according to composite criteria (ORR 8%). The composite CNS ORR in Cohort 3a and 3b were 49% (95% CI 32–66) and 33% (95% CI 10–65), respectively. 66 Median progression-free survival (PFS) and OS were 5.5 and 13.3 months in Cohort 3a, respectively, and were 3.1 and 15.1 months in Cohort 3b, respectively. The most common grade ⩾3 toxicity was diarrhea in Cohort 1 (25%) and Cohort 3a/b (29%).65,66 TBCRC 022 also designed a Cohort 4 [ClinicalTrials.gov identifier: NCT01494662] to evaluate neratinib and ado-trastuzumab emtansine (T-DM1; Table 3). The results of NALA, a randomized phase III trial, were presented in 2019. 67 Neratinib+capecitabine was compared with lapatinib+capecitabine in metastatic HER2-positive patients, as a third- or later-line HER2-directed therapy. PFS improved (HR 0.76; p = 0.006), and OS tended to be longer (HR 0.88; p = 0.209) in the neratinib combination group. This trial excluded active BM, but asymptomatic CNS metastases were included. Neratinib+capecitabine postponed time to intervention for symptomatic CNS (overall cumulative incidence, 22.8% versus 29.2%; p = 0.043). However, grade 3 diarrhea in these patients was more frequent than in lapatinib+capecitabine-treated patients (24.4% versus 12.5%).
Afatinib is an oral, irreversible HER1 and HER2 TKI. 68 A total of 121 patients with progressive/recurrent BM while receiving HER2-targeted therapies (trastuzumab, lapatinib, or both) were randomized into afatinib alone, afatinib+vinorelbine, or treatment of physician’s choice (TPC) in a phase II study (Table 1). 37 The primary endpoint was clinical benefit 12 weeks after randomization and was assessed as follows: (a) no progression of CNS per Response Evaluation Criteria In Solid Tumors (RECIST) 1.1; (b) no worsening of tumor-related neurological signs or symptoms; (c) no corticosteroid dose increase; and (d) absence of extra-CNS disease progression. Unexpectedly, clinical benefit was mostly achieved in the TPC group (41.9%), though was not statistically significant. In addition, toxicity profiles were worse in afatinib-containing treatments. These disappointing results have almost put an end to further afatinib research. A randomized phase II trial [ClinicalTrials.gov identifier: NCT04158947] is preparing, which will investigate the combination of another HER2-targeted agent, T-DM1, with afatinib (Table 3).
Another promising agent is tucatinib, an orally administered, selective, and reversible HER2 TKI, which reduces diarrhea and rash compared with other HER2 TKIs. 69 Tucatinib with capecitabine and trastuzumab was tested in a phase I study for metastatic HER2-positive patients with or without treated stable BM. 70 Twelve patients treated with 300 mg twice-daily tucatinib had measurable BM and five patients (42%) experienced brain-specific objective response by modified RECIST. A phase II randomized, double-blind study, HER2CLIMB, validated the treatment outcomes of this regimen and further included patients with BM which did not need immediate local intervention. 71 The tucatinib combination prolonged PFS (HR 0.54, 95% CI 0.42–0.71; p <0.001) and OS (HR 0.66, 95% CI 0.50–0.88; p = 0.005) compared with placebo. For patients with BM, the addition of tucatinib still improved PFS (HR 0.48, 95% CI 0.34–0.69; p < 0.001). As other combination regimens, phase I studies of tucatinib combined with trastuzumab [ClinicalTrials.gov identifier: NCT01921335; Table 3] or T-DM1, even enrolling patients with progressive CNS lesions unless requiring immediate local therapy, reported CNS ORR as 8% and 36%, respectively.72,73 Now, a randomized, double-blinded, phase III study [ClinicalTrials.gov identifier: NCT03975647], also known as HER2CLIMB-02, is recruiting patients with advanced or metastatic HER2-positive BC. The criteria for enrollment of patients with BM are the same as in the previous phase I study. Patients will be randomly assigned to T-DM1+tucatinib or placebo, and the primary endpoint is PFS. Tucatinib has received US Food and Drug Administration approval in combination with trastuzumab and capecitabine for women with previously treated advanced HER2+ breast cancer, with or without BM.
Pyrotinib is an oral, irreversible TKI targeting HER1, HER2, and HER4. 74 In a randomized phase III study, pyrotinib was assessed against placebo, both administered with capecitabine, for patients with metastatic HER2-positive BC who had prior taxane and trastuzumab treatment. 75 Pyrotinib+capecitabine achieved significantly longer PFS (median 11.1 versus 4.1 months; p <0.001); however, this trial did not enroll patients with untreated, symptomatic BM. Two phase II trials [ClinicalTrials.gov identifiers: NCT03691051, NCT03933982] have been initiated to investigate the antitumor activity of pyrotinib on BM (Table 3).
In January 2020, a phase I/II study of epertinib in refractory metastatic HER2-positive including BM BC reported that combination of epertinib with trastuzumab±capecitabine had promising antitumor activity with favorable toxicity profiles. 76 These results encourage more studies to investigate new HER2-directed combination therapies.
Other innovative molecular-targeted therapy
Based on the advances in the understanding of the underlying mechanisms of BC and BM, several molecular-targeted therapies have been developed in the last decade and have become some of the main therapeutic interventions for metastatic BC.
Bevacizumab, a humanized vascular endothelial growth factor (VEGF) monoclonal antibody, is thought to transiently normalize peritumoral vessels, resulting in enhanced drug delivery to BM. 77 The following three phase II trials attempted to demonstrate this hypothesis using a combination of bevacizumab and other cytotoxic agents. Thirty-eight patients with progressive BM were assigned to bevacizumab on day 1 of a 3-week cycle, followed by carboplatin and trastuzumab if HER2-positive on day 8 of one cycle and day 1 of subsequent cycles. 78 CNS ORR by composite criteria and RECIST was 63% and 45%, respectively. A second study in patients with WBRT-refractory BM investigated bevacizumab followed by etoposide and cisplatin (BEEP) with a 1-day window period. 79 Notably, this treatment schedule achieved a high CNS ORR according to the volumetric criteria of 77.1%, and 54.3% by RECIST. A third study [ClinicalTrials.gov identifier: NCT01281696] tested a similar regimen and included patients with leptomeningeal seeding, who would be treated with intrathecal methotrexate (Table 3). Pilot studies showed promising efficiency in leptomeningeal seeding patients. 80 Additional investigation is needed to optimize the proper treatment period and chemotherapeutic agent combination.
Cabozantinib is a small, multiple TKI that inhibits MET and VEGF receptor-2, penetrates into the CNS, and has significant antitumor activity for BM in non-small cell lung cancer and renal-cell carcinoma.81,82 In patients with heavily pretreated BM in BC, cabozantinib was well tolerated but did not show sufficient CNS response [CNS ORR (per RECIST 1.1) 5.6%], 83 in contrast with the previous studies showing higher CNS ORR after anti-VEGF.78,79 Therefore, further investigations are needed to find out more detailed antitumor mechanisms underlying the VEGF pathway of BM from BC, which could explain the different antitumor activities of these two agents.
Another treatment strategy actively being investigated is inhibition of the phosphoinositide-3-kinase/mammalian target of rapamycin (PI3K/mTOR) pathway. Hyperactivation of this pathway is a mechanism of trastuzumab resistance. 84 A phase II study, LCCC 1025, investigated whether inhibition of PI3K/mTOR and HER2 might lead to more significant responses in patients with HER2-positive BM. 85 Everolimus, a small molecule of the mTOR complex 1 inhibitor, was given with trastuzumab and vinorelbine; the intracranial response rate was very low (4%) and only one patient experienced a partial response. However, a similar time to progression and OS as previous studies, and a clinical benefit rate of 65% at 6 months, indicated further research is needed. Several agents targeting PI3K, such as BKM120 [ClinicalTrials.gov identifier: NCT02000882] and GDC-0084 [ClinicalTrials.gov identifier: NCT03765983], are currently under investigation (Table 3). One thing to note is that PI3K inhibitors crossing the BBB have been reported to cause mood alterations.86,87 In a phase I, dose-escalation study, 20% of all patients experienced altered mood, suspected to be related with BKM120. 87 Therefore, investigators of PI3K trials should pay attention to the psychological toxicities and monitor them properly.
Cyclin-dependent kinase (CDK) 4/6 inhibitors have been developed, especially focusing on hormone receptor (HR)-positive/HER2-negative metastatic BC, and have significantly improved PFS in these populations.88–90 However, previous clinical trials of CDK4/6 inhibitors excluded patients with CNS metastasis or included patients with pretreated and stable BM, demonstrating limited evidence of their CNS efficacy. 91 In a phase II study, abemaciclib, one of the CDK4/6 inhibitors, showed an intracranial clinical benefit of 25% among 58 patients with heavily pretreated BM from HR-positive/HER2-negative BC. 92 In HER2-positive and TNBC, the use of CDK4/6 inhibitors (palbociclib, ribociclib, and abemaciclib, etc.) in metastatic settings with or without untreated BM, are currently under investigation. 93 Disappointingly, a phase II study [ClinicalTrials.gov identifier: NCT02774681] of palbociclib in patients with HER2-positive BM was terminated due to slow accrual.
In TNBC, poly-adenosine diphosphate-ribose polymerase (PARP) inhibitors have been of interest. TBCRC 018 demonstrated that iniparib+irinotecan showed a slight benefit of time to progression in patients with progressive TNBC BM. 94 However, iniparib is not currently considered a bona fide PARP inhibitor. 95 Other PARP inhibitors, olaparib and veliparib, are currently not candidates for the treatment of BM. A case report demonstrated the potential role of olaparib in BM, 96 while a phase II study [ClinicalTrials.gov identifier: NCT02595905], including BM patients, has been initiated to investigate cisplatin with or without veliparib.
Return of classic chemotherapy
One approach for facilitating penetration of chemotherapeutic agents through the BBB for BM treatment is to modify their structures through conjugation with a peptide vector or via pegylation. 97 ANG1005 (GRN1005) makes Angiopep-2, a peptide vector that facilitates paclitaxel transport into the CNS. 98 Importantly, ANG1005 showed no CNS toxicity in a phase I trial. 99 In addition, a phase II study of ANG1005 in patients with recurrent BM showed excellent antitumor activity in intracranial and extracranial lesions. 100 A phase II trial [ClinicalTrials.gov identifier: NCT01480583] testing ANG1005 (+trastuzumab, if HER2 positive) was completed, but results are not available (Table 3). Other randomized trials are being pursued to validate this novel agent.
Etirinotecan pegol (NKTR-102), the prodrug of irinotecan, is a novel long-acting topoisomerase-I inhibitor, consisting of a four-arm polyethylene glycol with one irinotecan at the end of each arm. 101 It slowly hydrolyzes in vivo, and continuously produces SN38, the active irinotecan metabolite, which prevents high plasma concentrations of irinotecan and SN38, as well as unwanted side effects. 102 The phase III BEACON trial assessed the superiority of etirinotecan pegol to the currently available TPC in patients with locally recurrent or metastatic BC, who had prior treatment with an anthracycline, a taxane, and capecitabine. 103 Patients were randomized to etirinotecan pegol or single-drug TPC (one of: eribulin, ixabepilone, vinorelbine, gemcitabine, paclitaxel, docetaxel, or nab-paclitaxel). This trial failed to show an OS improvement in the etirinotecan pegol arm, but in the subgroup analysis of OS, patients with BM had superior OS (median 10 versus 4.8 months) with an HR of 0.51 (95% CI 0.30–0.86). 104 Although a small number of patients with BM were included in this analysis, the survival benefit of etirinotecan pegol was clear with favorable safety. Based on these results, another phase III trial in this population with BM (ATTAIN) [ClinicalTrials.gov identifier: NCT02915744] is underway (Table 3).
Tesetaxel is of the taxane class of drugs, with an advantage of oral administration. In phase II study with locally advanced or metastatic HER2-negative and HR-positive BC patients, tesetaxel showed significant activity as a single agent, with an ORR per RECIST 1.1 of 45% (95% CI 29–62). 30 Tesetaxel with or without capecitabine is being investigated in the randomized phase III study, CONTESSA [ClinicalTrials.gov identifier: NCT03326674], for these patients. CONTESSA TRIO [ClinicalTrials.gov identifier: NCT03952325] is a two-cohort, phase II study of tesetaxel. In Cohort 1, patients with locally advanced or metastatic TNBC will be randomized to tesetaxel or three inhibitors of programmed cell death-1 (PD-1) or its ligand (PD-L1; nivolumab, pembrolizumab, or atezolizumab). In Cohort 2, elderly patients (⩾65 years old) with HER2-negative locally advanced or metastatic disease will receive tesetaxel monotherapy. In this study, stable or progressing CNS metastases, excluding leptomeningeal disease are permitted but not required.
Establishing the efficacy of existing drugs against BM is as important as development of new agents. In a phase II trial, epothilone B did not achieve prespecified efficacy criteria, but increased diarrhea. 105 In addition, a recent article suggested that irinotecan+temozolomide could be a treatment option for progressing CNS diseases. 106 Eribulin mesylate, an approved agent for metastatic BC, is being tested in phase II trials [ClinicalTrials.gov identifier: NCT02581839 and NCT03412955; Table 3] for BM. A temozolomide and T-DM1 combination is being evaluated in a recruiting phase I/II study in patients with HER2-positive BM with prior local treatment [ClinicalTrials.gov identifier: NCT03190967; Table 3).
Prospects of immunotherapy
Over the past several years, the most revolutionary advancement in cancer treatment has been the discovery of immune-checkpoint inhibitors (ICIs). A mechanism of tumor survival and metastasis is activation of the immune-checkpoint pathway to induce immunosuppressive conditions; 107 ICI blocks this activation, thereby increasing immune-mediated tumor cell killing. After approval of ipilimumab, which targets cytotoxic T-lymphocyte antigen-4 (CTLA-4), for advanced melanoma treatment in 2011, several immunotherapeutic monoclonal antibodies have been developed to interrupt PD-(L)1 and CTLA-4 activity and have antitumor activity. The efficacy of immunotherapy in BM is well established in melanoma, non-small cell lung cancer, and renal-cell carcinoma (Table 4). Importantly, a review by Di Giacoma illustrated that intracranial ORR in melanoma was 5–26% with ICI monotherapy and 46–55% with ICI combination, suggesting that future studies should focus on the synergism of ICI-based therapeutic combinations (Table 4). 108
Prospective trials of immunotherapy for patients with brain metastases from other solid tumors.

Pooled analysis of the three prospective trials: CheckMate 063 (phase II), 017 (phase III), and 057 (phase III).
BM, brain metastasis; irORR, immune-related objective response rate; LMS, leptomeningeal seeding; mWHO, modified World Health Organization criteria; NA, not applicable; NSCLC, non-small cell lung cancer; ORR, objective response rate; OS, overall survival; PD-L1, programmed cell-death ligand 1; PR, partial response; RCC, renal-cell carcinoma; RECIST, Response Evaluation Criteria In Solid Tumors; SD, stable disease; VEGFR, vascular endothelial growth factor receptor.
In metastatic TNBC, atezolizumab, a monoclonal antibody against PD-L1, in combination with nab-paclitaxel, was approved recently as first-line therapy based on the results of the IMpassion 130 trial. In this randomized phase III trial, 902 patients with untreated metastatic TNBC were assigned to receive atezolizumab or placebo, combined with nab-paclitaxel. 122 Addition of atezolizumab to nab-paclitaxel significantly improved PFS compared with placebo (median 7.2 versus 5.5 months; HR 0.80, 95% CI 0.69–0.92; p = 0.002). Median OS was longer in the atezolizumab+nab-paclitaxel group (21.3 months) than in the placebo+nab-paclitaxel group (17.6 months; p = 0.08). Although subgroup analysis showed no PFS benefit in patients with BM, approximately only 7% of patients in each arm had BM, and combined chemotherapy was not optimal for CNS metastases. Future clinical trials of atezolizumab might be designed to evaluate clinically meaningful benefit in patients with BM from TNBC.
Another randomized phase III study, the KEYNOTE-355 trial [ClinicalTrials.gov identifier: NCT02819518], was released in a press in February 2020. 123 This trial recruited patients with locally recurrent unresectable or metastatic TNBC, not previously treated with chemotherapy, and did not exclude patients with BM if they were treated and stable. This study consisted of two parts: in part one, pembrolizumab, an anti-PD-1, was administered with one of three chemotherapeutic agents chosen by investigators (nab-paclitaxel, paclitaxel, or gemcitabine/carboplatin); in part two, 847 patients were randomized to receive pembrolizumab or placebo, in combination with one of the three chemotherapy regimens. The interim analysis demonstrated that pembrolizumab with chemotherapy significantly improved PFS compared with the placebo group (i.e. chemotherapy alone) in patients with a PD-L1 combined positive score of ⩾10 tumors. This trial continues to assess OS, the other primary endpoint.
Currently, other randomized phase III studies using pembrolizumab [ClinicalTrials.gov identifier: NCT02555657] and atezolizumab [ClinicalTrials.gov identifier: NCT03125902] in metastatic TNBC have been initiated. However, these trials exclude active CNS metastases, and are therefore unable to address the efficacy of ICIs on BM. We summarize the currently available prospective trials of ICI for patients with BM from other solid tumors in Table 4.
A systematic review of 13914 patients found the highest incidence of tumor-infiltrating lymphocytes of at least 50% both in TNBC (20%, range 4–37%) and HER-2 positive BC (16%, range 11–24%), 124 suggesting that proper modulation of the tumor microenvironment could boost antitumor activity of ICIs. Recent approaches have focused on the role of RT in this process, discussed further in the following.
Combined approach of systemic therapies with RT
The BBB is a critical obstacle to the efficacy of systemic treatments for BM, and researchers have explored mechanical and chemical methods to overcome this. One approach includes inducing transient opening of the BBB using a hyperosmolar solution. 125 Since September 2019, a study [ClinicalTrials.gov identifier: NCT03714243] of BBB disruption using magnetic-resonance-imaging-guided focused ultrasound began recruiting patients with HER2-positive BM at Sunnybrook Health Sciences Centre in Canada. Among several approaches to weakening the BBB, we will focus on studies using RT. For local treatment, addition of systemic treatment may help eradicate subclinical micrometastases and act as a radiosensitizer.
Sorafenib, an oral multi-targeted TKI, administered concurrently with WBRT or SRS in BM from solid tumors, including BC, was safe and tolerated in a phase I study.126,127 A phase I study of HER2-positive BM treated with lapatinib in combination with WBRT followed by trastuzumab did not meet the prespecified feasibility criteria due to toxicity. 128 However, the high volumetric CNS ORR (79%, 95% CI 59–92) suggested this treatment strategy could be used in future studies. Accrual of a randomized phase II study has completed (RTOG 1119) [ClinicalTrials.gov identifier: NCT01622868], in which patients with unirradiated HER2-positive BM were randomized to WBRT/SRS with or without lapatinib (Table 2).
The phase I REBECA study of 19 patients with untreated BM from solid tumors (n = 13 with BC) was performed to identify the recommended phase II bevacizumab dose when combined with WBRT (30 Gy/15 fractions) from day 15. 129 The regimen of 15 mg/kg bevacizumab for three cycles, with 2-week intervals, was deemed most appropriate, and 10 patients across all dose levels experienced an objective response per RECIST 1.1. Paradoxically, these synergistic effects might be explained by the fact that bevacizumab-induced vascular normalization before WBRT might reduce the hypoxic portion of tumors, leading to enhanced radiosensitivity rather than BBB disruption. Previous findings demonstrating that BEEP resulted in high CNS ORR 79 initiated a phase II randomized study [ClinicalTrials.gov identifier: NCT02185352], in which patients with WBRT-untreated BM not suitable for surgery or SRS were randomized into induction BEEP followed by WBRT (30 Gy/10 fractions) or WBRT alone (Table 2).
In addition to BBB disruption, RT plays a crucial role in immuno-oncology by engaging antigen-specific immune responses, which serves as the rationale for RT and immunotherapy combinations. 130 The ICI and SRS combination has been largely investigated for BM in melanoma, and several retrospective studies have shown promising results.131–133 The largest meta-analysis assessing impact of combination treatment on BM from solid tumors (mainly melanoma) reported that concurrent ICI and SRS improved OS (64.6% versus 51.6%; p <0.001) and regional brain control (38.1% versus 12.3%; p = 0.049) at 1 year compared with nonconcurrent therapy. 134 Local control rates marginally differ between the two groups (89.2% versus 67.8%; p = 0.09), and incidence of radionecrosis was 5.3%. In recent years, three phase I or II studies have been launched to test the efficacy and safety of this innovative regimen in BM in BC: atezolizumab [ClinicalTrials.gov identifier: NCT03483012], pembrolizumab [ClinicalTrials.gov identifier: NCT03449238], and nivolumab [ClinicalTrials.gov identifier: NCT03807765], all concurrently administered with RT. More information about these trials is detailed in Table 2.
Another consideration when combining RT with systemic therapy is the timing of RT. SRS is highly effective when used concurrently in combination with ICI. 134 In terms of WBRT, a phase I randomized study [ClinicalTrials.gov identifier: NCT02135159] examined the optimal sequence of T-DM1 in HER2-positive BM treatment: T-DM1 after, before, during and after, or concomitant with WBRT, respectively (Table 2); the trial is complete and awaiting results, which will likely inform the design of subsequent clinical trials.
Conclusion
Although cancer treatments have evolved in recent decades, effective treatments for BM are lacking. In patients with BM from BC, especially HER2-positive and TNBC, BM is the leading cause of mortality. Therefore, new treatment strategies for BM are an unmet clinical need.
Traditionally, local treatment for BM is most common, although recently, several innovative systemic therapies are being investigated. However, although BM is frequent in patients with BC, there is insufficient evidence to support established treatment strategies due to a lack of phase III randomized trials. In addition, given variation in biological features and intracranial failure patterns in different tumor subtypes, treatment for BM will likely have to be designed for each tumor molecular subtype. In recent years, treatment combinations with different systemic agents or integration of local therapy have shown outstanding results compared with monotherapy, demonstrating that comprehensive investigations of multimodal approaches are needed in treatment for BM from BC.
Molecular characterization of BMs before treatment may also be necessary, as treatment may be based on tumor molecular subtype; however, there are many challenges with this approach. Therefore, there is also a need for research on alternative techniques for predicting tumor molecular subtypes with high precision using brain imaging or circulating tumor deoxyribonucleic acid in serum or cerebrospinal fluid. In addition, research on the prevention, reduction, or management of side effects caused by treatment will be needed to increase patient tolerance.
Much progress on BM treatment strategies has been made in recent years, but many gaps still remain to be filled before a standard-of-care regimen is established. On the other hand, although not covered in this paper, screening for BC in women should be actively performed to improve PFS and OS by diagnosing BC at an early stage, and we have to pursue further investigations to find out proper neoadjuvant and adjuvant treatments along with complete surgical resection of BC to reduce locoregional recurrences and/or distant metastases. Early detection of asymptomatic BM through imaging follow up of the brain is essential in metastatic HER2-positive and TNBC patients, who are susceptible to the development of BM. Studies on proper intervals of imaging follow up are also important issues. However, BM screening in non-metastatic patients could not yet be justified, unlike patients with lung cancer. These strategies on early detection of BC and secondary prevention of BM might provide promising treatment outcomes and patients’ quality of life.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Ministry of Science and Information & Communication Technology (NRF#2020R1A2C2005141), SNUBH Research Fund (#14-2019-031), and Seoul National University AI Institute through the Data Science Research Project 2019 to In Ah Kim.