
Abstract
Background:
The aim of this work was to to evaluate the incidence and risk factors of adverse events (AEs), focusing on cardiovascular events (CVEs) and hypokalemia, in patients treated with abiraterone acetate (AA) and prednisone (PDN) outside clinical trials, and their association with survival outcomes.
Methods:
This was a retrospective cohort study of 105 patients treated from 2011 to 2016. Incidence of AEs was descriptively summarized in the whole cohort and by subgroup (pre- versus post-docetaxel). Multivariable Cox proportional hazards models assessed factors associated with progression-free survival (PFS) and overall survival (OS).
Results:
Overall, median PFS and OS were 14.9 and 24.6 months, respectively. Prostate-specific antigen (PSA) ⩾ 10 ng/ml (p = 0.007), Gleason Score >7 (p = 0.008), Eastern Cooperative Oncology Group (ECOG) performance status (PS)1–2 (p = 0.002), duration of androgen deprivation therapy (ADT) ⩽ 43.2 months (p = 0.01), and body mass index (BMI) > 25 (p = 0.03) were associated with worse PFS; presence of pain (p = 0.01), ECOG PS1–2 (p = 0.004), duration of ADT ⩽ 43.2 (p = 0.05), and BMI > 25 (p = 0.042) were associated with worse OS. Incidence of CVEs was as follows: hypertension 17.1%, fluid retention 4.8%, cardiac disorders 8.6%. 16.2% of patients developed hypokalemia. Age ⩾ 75 years was associated with higher probability of cardiac disorders (p = 0.001) and fluid retention (p = 0.03). CVEs did not impact on PFS or OS. Hypokalemia was associated with better median OS (p = 0.036). Similar associations were observed after stratification by subgroup.
Conclusions:
Median PFS and OS estimates and incidence of CVEs and hypokalemia in our series are consistent with those of pivotal trials of AA plus PDN, confirming the efficacy and safety of this regimen also in the real-world setting. Elderly patients have higher odds of developing/worsening CVEs. However, regardless of age, CVEs were not associated with worse outcomes. Treatment-related hypokalemia seemed to be associated with longer OS, albeit this finding needs confirmation within larger, prospective series.
Keywords
Introduction
Prostate cancer is the most common malignancy in men in western countries. 1 Androgen deprivation therapy (ADT) represents the cornerstone treatment for metastatic prostate cancer and indeed most patients do benefit from ADT. However, most of them are destined to progress and to become castration-resistant. 2 Median survival of metastatic castration-resistant prostate cancer (mCRPC) is highly variable and expected survival among these patients is associated with tumor bulk and disease spread to distant sites other than the skeleton. 3 Over the past few years, the increasing knowledge about the driving role of the androgen receptor, even in the castration-resistant setting, has dramatically improved survival for patients developing mCRPC. 4 In particular, based on this assumption, new endocrine therapies, such as abiraterone acetate (AA) and enzalutamide, have been developed. 4
Abiraterone acetate is a potent, selective inhibitor of steroidogenesis that interferes with androgen synthesis through the inhibition of the cytochrome P450 17α-hydroxylase/17, 20 lyase (CYP17). This enzyme catalyzes two sequential reactions, namely the conversion of pregnenolone and progesterone to their 17α-hydroxy-derivatives (17α-hydroxylase activity), and the subsequent formation of dehydro-epiandrosterone (DHEA) and androstenedione (17, 20-lyase activity). Androstenedione and DHEA are then converted to testosterone (TST) by 17-beta-hydroxy-steroid-dehydrogenase and eventually to dihydrotestosterone (DHT) by 5α reductase. 5 Thus, the inhibition of CYP17 decreases circulating and tissue levels of androgens, namely DHEA, TST and DHT, preventing the stimulation of androgen-sensitive neoplastic cell clones. The blockade of steroidogenic enzymes by AA leads to the suppression of adrenocorticotropic feedback, which results in an exceeding production of steroid precursors with high mineralocorticoid activity. 5 This effect is responsible for the most frequent adverse events (AEs) occurring during treatment with AA, including hypokalemia, hypertension and fluid overload. Therefore, the concomitant use of low-dose glucocorticoids is required to decrease the frequency and severity of these events and serial monitoring of potassium levels and blood pressure is recommended.6,7
AA plus low-dose prednisone (PDN) was first approved for patients with mCRPC failing prior docetaxel (DX) chemotherapy (CT), based on the COUAA-301 trial results, showing AA plus PDN to be able to improve overall survival (OS) compared with PDN plus placebo [14.8 versus 10.9 months, hazard ratio (HR) 0.65, 95% confidence interval (CI) 0.54–0.77, p < 0.001]. 7 This drug was subsequently tested in CT-naïve mCRPC, also producing a statistically significant OS benefit (median OS 34.7 versus 30.3 months in the AA and placebo group respectively, HR 0.81, 95% CI 0.70–0.9, p = 0.003) especially in men with asymptomatic or mildly symptomatic disease.8,9 As expected, in both trials, fluid retention, hypokalemia, hypertension and cardiovascular (CV) disorders (cardiac ischemia, rhythm disorders, valvular dysfunctions, stroke, peripheral thrombosis and arterial disease) were the most commonly observed AEs. In the COUAA-301 trial, fluid retention was observed in 33%, hypokalemia in 18%, hypertension in 11% and CV disorders in 16% of treated patients. 7 Findings in CT-naïve patients were comparable. In fact, in the COUAA-302 trial, fluid retention was observed in 31% and hypokalemia in 18% of patients. However, the incidence of hypertension (24%) and of CV disorders (22%) was higher.8,9 The higher incidence of CV disorders in CT-naïve patients is likely the result of the longer drug exposure of these patients: median radiologic PFS in the COUAA-302 trial was almost three times as long as that observed in the COUAA-301 trial (16.5 versus 5.6 months).7,9
Despite the widespread use of AA in clinical practice and according to the major guidelines,10–12 few data on the incidence of CV events in ‘real-life’ patients treated with AA and PDN are available, mostly regarding patients failing prior treatment with DX. In the Italian Named Patient Program, the clinical outcomes reported in the AA pivotal trial 7 were reproduced but the incidence of toxicities was lower (hypertension was observed only in 2.6% and hypokalemia only in 1.9% of treated patients). 13 This difference probably reflects lack of systematic monitoring of patients in this clinical practice setting. One single-institution retrospective study included 51 CRPC patients with concomitant CV risk factors, who were also pretreated with DX. Hypertension was observed in 16% while fluid retention in 18% of patients. Moreover, dose reductions due to unacceptable toxicity were necessary in 9.8% of patients. This study confirms that AA plus PDN can be safely delivered, even to patients bearing risk factors for CV diseases. 14 A data update of the same study, with longer follow-up time, confirmed the previously reported safety profile. 15 The results of an additional study, also including mCRPC patients previously treated with DX, were presented at the 2016 American Society of Clinical Oncology Annual Meeting. 16 This was a prospective study specifically aimed at monitoring cardiac functionality during treatment with AA and PDN. A total of 87 patients underwent electrocardiogram (ECG) and echocardiography with evaluation of left ventricular ejection fraction (LVEF) and diastolic function, both at baseline and at every 6 months until treatment discontinuation. Hypertension was observed in 34.6% of patients, without statistically significant variation of LVEF and diastolic function.
More recently, the results of two trials exploring the efficacy of AA and PDN (5 mg daily) in hormone-naïve patients were reported.17,18 In both trials the combination of AA plus PDN with ADT was compared with ADT alone, and both ones reported statistically significant and comparable reductions in the HR of all-cause mortality, the primary endpoint for both studies (LATITUDE trial: HR 0.62, 95% CI 0.51–0.76, p < 0.001; 17 STAMPEDE trial: HR 0.63, 95% CI 0.52–076, p < 0.001 18 ) as well as in the hazards of all other secondary endpoints. Though these trials were greatly heterogeneous regarding the patient populations accrued, the incidence of AEs, namely hypertension, cardiac disorders and hypokalemia, was comparable across trials. Indeed, hypertension (any grade) occurred in 37% of patients in the LATITUDE trial and in 32% in the STAMPEDE trial among patients in the AA plus PDN arm. The incidence of cardiac disorders (any) was 12% and 10% respectively while hypokalemia (all grades) was recorded in 20% and 12% of patients assigned to AA plus PDN, respectively. The incidence of hypertension, recorded in previous studies (37% and 32%) appears to be higher than the incidence of hypertension in the COUAA-302 trial (24%). However, the incidence of CV events (12% and 10%) and the incidence of hypokalemia (20% and 12%) were quite comparable, if not inferior, to the incidences recorded in the COUAA-302 trial (22% and 18% respectively). These differences are probably due to the different way of reporting AEs, though study population heterogeneity, treatment duration and lower PDN dose might contribute to the differences observed. The LATITUDE and STAMPEDE trials are both destined to soon become ‘practice changing’ and to expand the patient population candidates to receive long-term treatment with AA and PDN. However, both trials included very selected patient populations and ‘real-life’ data concerning AA plus PDN in hormone-naïve patients are not available yet; moreover, it should be better clarified which patients can benefit more from this therapeutic option and which ones, for instance, could better take advantage from adding DX to ADT.19,20 Finally, it will take a few years to obtain the permission of using AA in the castration-sensitive setting, since in most countries, including Italy, the use of AA plus PDN is still limited to CRPC patients. Therefore, we believe that it is still important to report on CRPC patients treated in the real world, outside of clinical trials, not only because they represent the widest setting in everyday clinical practice, but also in the perspective of future comparisons with the results obtained from similar, real-life studies among hormone-naïve patients.
In view of these premises, we report here the results of a retrospective study evaluating patients affected by mCRPC, who were referred to our unit and treated with AA and PDN, outside clinical trials. Defining the incidence of AEs, with a special focus on CV and biochemical events (including hypokalemia) in a ‘real-life’ mono-institutional patient population, looking for the factors putatively predisposing to them, and evaluating the impact, if any, of CV and biochemical events on patients outcome were study aims. The putative association between baseline clinical–pathological characteristics, the incidence of AEs and patient clinical outcome was also investigated, in the attempt to identify a priori among the patients, candidates to receive treatment with AA and PDN, those at higher risk to develop CV and biochemical events and those destined to derive the greatest benefit from this treatment.
Patients and methods
We reviewed the charts of 105 patients affected by mCRPC and consecutively referred to our unit to receive AA and PDN between June 2011 and 2016. Ethics approval and consequent informed consent were not required for this study, according to ‘Authorization n. 9/2016 – General Authorization for the Processing of Personal Data for Scientific Research Purposes – 15 December 2016’ (Published in Gazzetta Ufficiale No 303 of 29 December 2016). On the basis of this authorization, universities, research centers and scientific societies do not have to require ethics approval to perform observational studies on data previously recorded without significant influence on affected patients.
The following information, recorded at the time AA was started, was collected for each patient: age, Eastern Cooperative Oncology Group (ECOG) performance status (PS), body mass index (BMI), presence or absence of pain (evaluated through the Brief Pain Inventory Short Form scale), 21 prostate-specific antigen (PSA) value, type of metastatic sites involved, time on previous ADT, and Gleason score (GS) of primary tumor. Pre-existing cardiac events or CV comorbidities were also recorded. Baseline ECG findings and LVEF were available for all patients, since cardiologic examination before starting treatment with AA and PDN is required by the Italian Drug Agency (AIFA).
All the patients included in the study cohort received AA orally, 1000 mg daily, and PDN, 5 mg twice daily, until disease progression, symptomatic deterioration, or unacceptable toxicity. Pharmacological suppression of gonadal function was maintained in all patients. The incidence of fluid retention, hypertension, hypokalemia, CV disorders, AST-ALT increase, diabetes and hypercholesterolemia were annotated and scored using Common Terminology Criteria for Adverse Events, version 4.0. 22 AE assessment was performed 2 weeks after the beginning of AA plus PDN and at monthly intervals thereafter. In patients at higher risk of developing cardiovascular events (CVEs) and with a baseline LVEF < 50%, assessment was performed every 2 weeks for the first 3 months. Disease progression was defined as per the Response Evaluation Criteria In Solid Tumors (RECIST) criteria, version 1.1 23 and Prostate Cancer Clinical Trials Working Group 2 criteria. 24 Radiographic assessments were performed every 6 months unless required before due to biochemical progression (as defined by an increase in PSA level of 25% or more in respect to nadir value) or clinical deterioration. The date of disease progression was recorded as well as the date of death. The cause of death was recorded whenever we were able to retrieve it. PFS was defined as the time between the initiation of AA plus PDN and the date of disease progression. OS was defined as the time between the initiation of AA plus PDN and the date of death.
Statistical analysis
All the patients treated with AA and PDN at our unit between 2011 and 2016 were included in the analysis.
Patient characteristics, the incidence of AEs (namely of CV and biochemical events) in the overall cohort and by subgroup, the association between patient characteristics, the incidence of AEs and patient outcome were descriptively summarized. The predictive value of AEs on treatment outcome was investigated by comparing outcome indicators in patients who developed CV and biochemical events (namely hypokalemia) and in those who did not.
OS and PFS curves were obtained using the Kaplan–Meier product-limit estimator and compared using the log-rank test. 25 To evaluate the possible interactions among aforementioned study variables with clinical outcomes, multi-parametric, Cox proportional hazard models were used. 26 We obtained separate models for PFS and OS, adjusting for all the covariates that predicted, after univariate analysis, for PFS or OS, as appropriate. The following covariates were included in the PFS models: baseline PSA level (<10 versus ⩾10 ng/ml); ECOG PS (0 versus 1–2); prior ADT duration (⩽43.2 versus >43.2 months); BMI (⩽25 versus >25); Age (<75 versus ⩾75); GS (⩽7 versus >7). In the OS model, we included PSA level (<10 versus ⩾10 ng/ml); ECOG PS (0 versus 1–2); prior ADT duration (⩽43.2 versus >43.2 months); BMI (⩽25 versus >25) and pain (present versus absent). A stepwise procedure was used with a significance level of p = 0.05 to retain variables in the model. HR estimates and their 95% CIs were obtained. The cumulative incidence function was used to describe cause-specific mortality and Fine and Gray’s proportional hazard regression models for competing risks were used to predict for the probabilities of prostate cancer-related and unrelated mortality. 27 HRs and respective 95% CIs for group comparisons were obtained after adjusting for baseline PSA value, ECOG PS, ADT duration, BMI and pain presence. The Chi-square test or Fisher’s exact test were used to compare the baseline characteristics between pre and post-DX patients and the incidence and severity of AEs. 28 All statistical tests were two-sided. We used the IBM software Statistical Package for Social Sciences (SPSS) version 21.0 for Windows (SPSS Inc. Chicago, Illinois, USA) and Stata/SE 11 (College Station, TX, USA) for data analysis.
Sample size calculation
No formal calculation of sample size was performed in this retrospective series, as it would not be possible, anyway, to change cohort size since it included all the patients treated with AA and PDN followed at our unit in the time period mentioned above. Moreover, as we have already pointed out in the premises, we intended to perform an explorative study, just to look at the incidence and different distribution of patient features, outcome indicators and AEs (namely CV and hypokalemia) in our cohort, including real-life patients treated outside of clinical trials.
Results
Cohort characteristics
As already mentioned, 105 consecutive mCRPC patients treated with AA plus PDN were included in the cohort: 75 had been previously treated with DX while 30 had received AA and PDN as front-line treatment. Median follow up was 26.8 (range 1.4–57.4) months for the whole cohort, 20.9 months (range 3.3–28.4) months for CT-naïve patients and 32.6 months (range 1.4–57.4) for patients previously treated with DX. Patient characteristics are summarized in Table 1. Characteristics of pre- and post-DX patients were comparable. Table 2 shows the prevalence of pre-existing CV disorders and of other conditions that might affect patient survival and treatment safety. Before starting treatment with AA and PDN, most of the patients were affected by hypertension (62.9%) and about half of them was overweight or obese (47.6%). However, again there were no major differences between subgroups.
Main characteristic of study patients at AA plus PDN start (disease related).
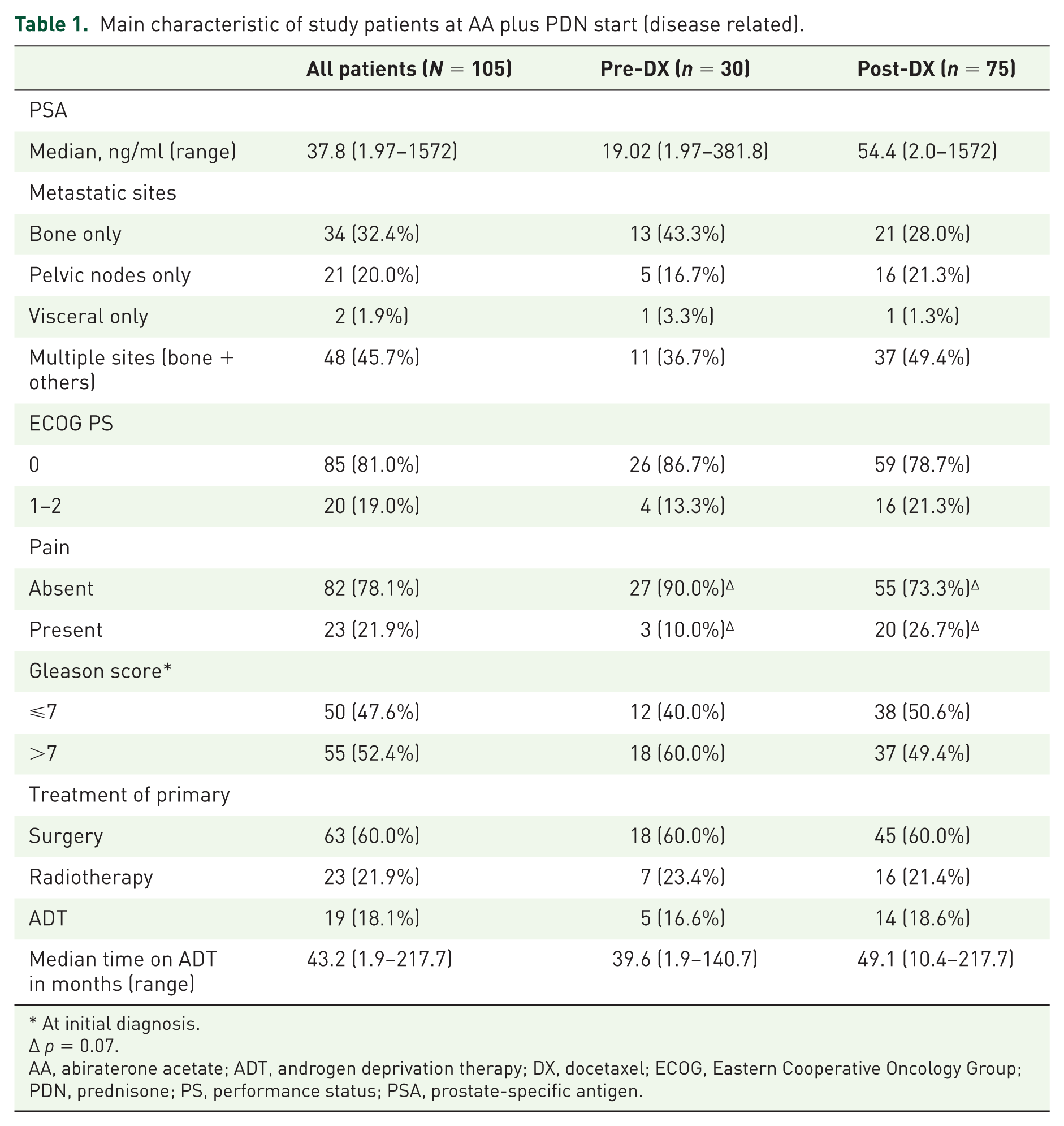
At initial diagnosis.
p = 0.07.
AA, abiraterone acetate; ADT, androgen deprivation therapy; DX, docetaxel; ECOG, Eastern Cooperative Oncology Group; PDN, prednisone; PS, performance status; PSA, prostate-specific antigen.
Main characteristic of study patients at AA plus PDN start (patient related).

AA, abiraterone acetate; BMI, body mass index; CV, cardiovascular; DX, docetaxel; LVEF, left ventricular ejection fraction; PDN, prednisone.
Efficacy data
Median PFS of the whole cohort was 14.9 months (range 1.4–45.7); as expected, PFS was longer in CT-naïve than in post-DX patients: 20.9 (range 1.8–28.4) versus 13.8 (range 1.4–45.7) months respectively. Median OS was 24.6 months (range 1.4–57.4) and it was also longer in CT-naïve patients compared with post-DX patients: 24.8 (range 3.3–28.4) versus 19.9 (range 1.4–57.4) months, respectively (Figure 1). Median time to PSA progression was 9.3 months (range 0.5–41.1) in the whole cohort, 12.2 months (range 0.5–27.9) in CT-naïve and 8.0 months (range 1.2–41.1) in post-DX patients. Patient age at diagnosis (p = 0.04), baseline PSA level (p = 0.002), GS (p = 0.004), ECOG PS (p = 0.017) and duration of prior ADT (p < 0.001) impacted PFS at univariate analysis in the overall cohort and in patients failing prior DX treatment (PSA level p = 0.002; GS p = 0.003; ECOG PS p = 0.003), but not in CT-naïve patients (complete data not shown). Among these variables, baseline PSA level, GS, ECOG PS and prior ADT duration retained statistical significance in multivariable models. Noteworthy, also BMI seemed to predict for PFS after multivariable analysis (Table 3).

PFS and OS curves in all cohort patients and subgroups.
Multivariable analyses of PFS and OS.

Variables not achieving the statistical significance after univariate analysis were not included into the models.
ADT, androgen deprivation therapy; BMI, body mass index; CI, confidence interval; DX, docetaxel; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; OS, overall survival; PFS, progression-free survival; PS, performance status; PSA, prostate-specific antigen.
Presence of pain (p < 0.001), baseline PSA level (p = 0.009) and ECOG PS (p < 0.001) were able to predict for OS duration at univariate analysis in the whole group while GS (p = 0.04) and duration of prior ADT (p = 0.016) were also significant predictors of OS in the post-DX group. Pain (p = 0.01), ECOG PS (p = 0.004), prior ADT duration (p = 0.05) and BMI (p = 0.042) were predictive of the risk of death at multivariable analysis; noteworthy, BMI > 25 was especially associated with a higher risk of death in CT-naïve patients (p = 0.018) (Table 3). Table 4 summarizes the results of multivariable analysis of mortality in the competitive risks model. None of the investigated covariates (baseline PSA value, ECOG PS, ADT duration, BMI value and presence of pain) proved significantly associated with prostate cancer-unrelated mortality, though a trend toward higher risks of death (p = 0.052) was observed for the presence versus the absence of pain.
Multivariable analysis of competitive risks of mortality (total patients: N = 105).

ADT, androgen deprivation therapy; BMI, body mass index; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; HR, hazard ratio; PS, performance status; PSA, prostate-specific antigen.
By contrast, all the variables on study, except for the presence of pain, were independently associated with prostate cancer-specific mortality, particularly BMI (p = 0.003) and duration of ADT (p = 0.02).
Safety data
Table 5 reports the incidence of AEs developed over the course of treatment in the whole series and in subgroups. As expected, hypertension (17.2%) and hypokalemia (16.2%) were the more commonly observed events, the incidence of both being more elevated in post-DX patients as compared with CT-naïve patients. All the other CV events, including fluid retention and cardiac disorders, were described in <10% of patients (fluid retention in 5/105 patients and cardiac disorders in 9/105 patients). No statistically significant reduction in LVEF compared with baseline was recorded. Worsening of hypertension or of pre-existing cardiac disorders occurred in 16.7% (from G1 to G2 in 9.1% and from G1–G2 to G3–G4 in 7.6%) and 11.1% (from G1 to G2 in 8.3% and from G1–G2 to G3–G4 in 2.8%) of patients, respectively. While 21% of patients affected by diabetes developed further worsening of tolerance to glucose, only 3.6% of patients affected by dyslipidemia showed worsening of this condition.
Patients developing at least one AE during treatment.
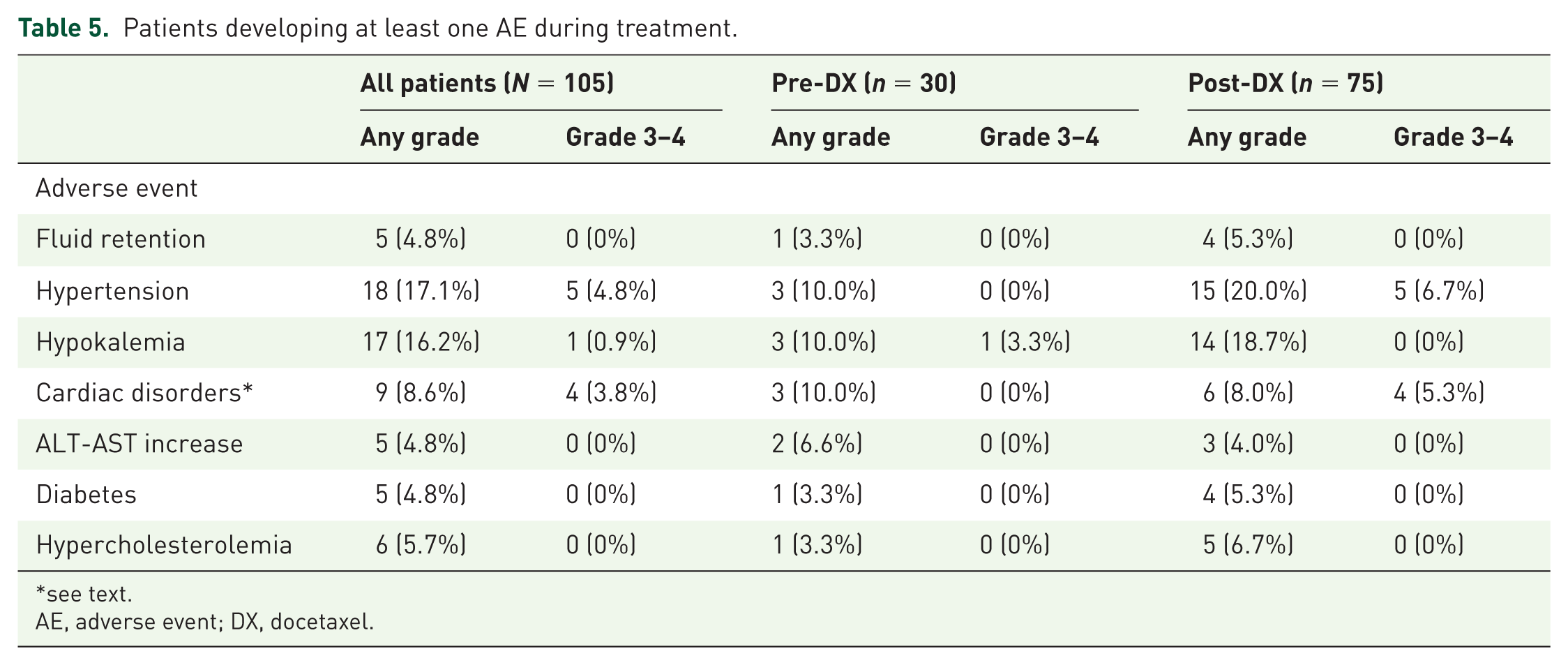
see text.
AE, adverse event; DX, docetaxel.
Presence of baseline hypertension and cardiac disorders was not associated with the development of new hypertensive episodes or cardiac disorders. Conversely, pre-existing diabetes was significantly associated with worsening of glycemic control (p = 0.02). As it is shown in Table 6, patient age was a significant risk factor predisposing to develop cardiac disorders (p = 0.001) or fluid retention (p = 0.03). Unexpectedly, patients with normal BMI showed a higher risk to develop cardiac disorders compared with overweight or obese patients (p = 0.03), even adjusting for baseline cardiac risk factors (p = 0.047). No relationship between baseline ECOG PS, LVEF, presence of pain and AEs occurrence was found (Table 6).
Incidence of CV, biochemical and metabolic events during treatment according to age, BMI, ECOG PS and LVEF.
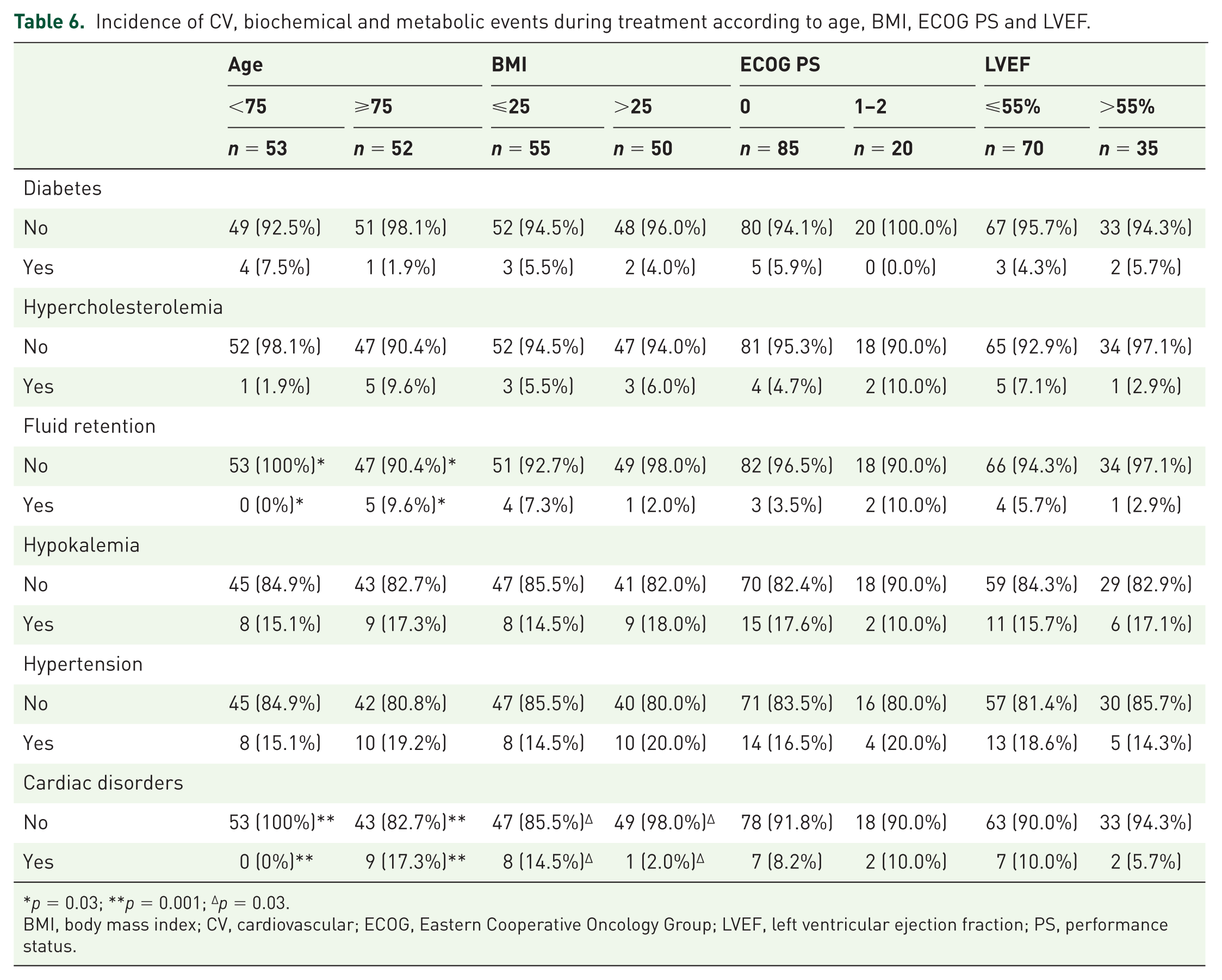
p = 0.03; **p = 0.001; Δp = 0.03.
BMI, body mass index; CV, cardiovascular; ECOG, Eastern Cooperative Oncology Group; LVEF, left ventricular ejection fraction; PS, performance status.
No association between the development of cardiac AEs and PFS or OS duration was observed (Table 7). In particular, patients developing one or more of such events did not appear to progress or to die earlier. No association between hypokalemia and PFS was observed, though a trend was found in favor of patients who developed hypokalemia. However, patients developing hypokalemia appeared to live significantly longer (p = 0.013; Table 7). The association between the occurrence of hypokalemia during treatment and longer OS was confirmed also by multivariable analysis [adjusted HR (95% CI) versus no hypokalemia: 0.40, (0.17–0.94), p = 0.036; Figure 2].
PFS and OS as a function of the incidence of all AEs and of CV and biochemical events.

AE, adverse event; CI, confidence interval; CV, cardiovascular; HR, hazard ratio; OS, overall survival; PFS, progression-free survival.
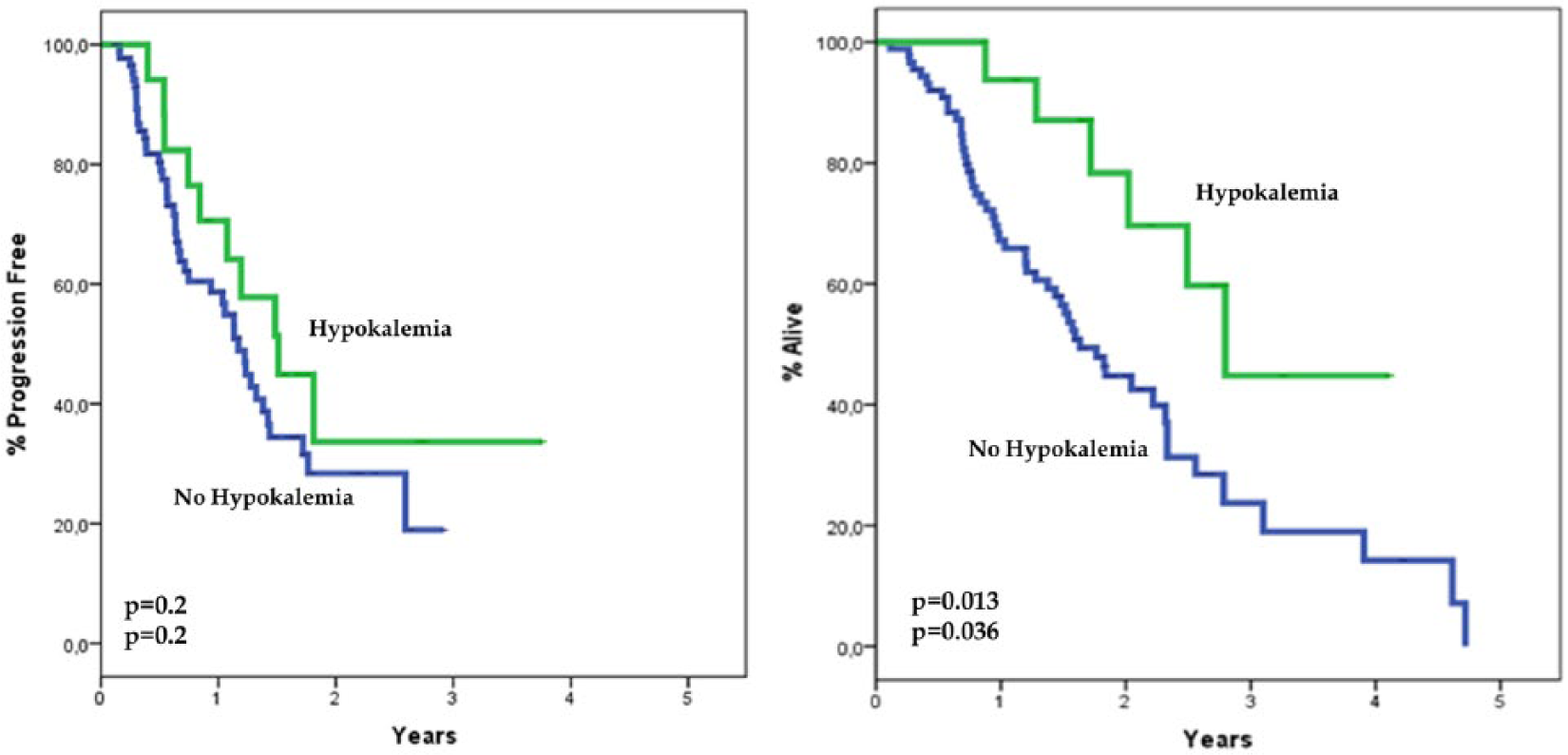
PFS and OS curves in patients who developed hypokalemia and in those who did not.
Discussion
In this retrospective analysis, we report our experience about the efficacy and safety of AA plus PDN in mCRPC patients, either CT-naïve or previously treated with DX, focusing on CV, biochemical (i.e. hypokalemia) and metabolic events. Unfortunately, our study is retrospective, includes a relatively small number of patients, which implies a low statistical power, and is unbalanced relative to the proportion of patients receiving AA plus PDN after DX failure compared with the proportion of those receiving these drugs as their front-line treatment. Moreover, observation times recorded in the two groups also differed. Both of the mentioned disproportions reflect the fact that AA was first licensed for the post-DX setting and that it obtained the approval for the management of CT-naïve patients only subsequently. All these factors might bias findings both in the whole cohort and by subgroup, and limit both direct comparisons between subgroups and indirect comparisons with the COU-AA 301 and 302 trial findings. Nevertheless, we believe that our study provides some interesting information regarding the efficacy and safety of AA plus PDN in ‘real-life’ mCRPC patients, which can prove useful in every day practice.
Efficacy data
Overall, the efficacy results obtained in our series are comparable with those achieved in the two pivotal trials, which contributed to drug approval. Indeed, in post-DX patients, we observed a median PFS of 13.8 months and a median OS of 19.9 months. In the COUAA-301 trial, which comparably accrued post-DX patients, the median duration of PFS and of OS were 5.6 and 15.8 months respectively. The better outcome recorded in our series is probably due to the different selection criteria [patients enrolled in the COUAA-301 trial were younger, had a higher tumor burden (median PSA level was 128.8 versus 54.4 ng/ml in our cohort subgroup) and were more frequently symptomatic] and possibly to the differences in the criteria used to define disease progression. Notably, PSA free-survival duration was comparable in the two series, median PSA free-survival in our series and in the COUAA-301 trial being 8.0 and 10.2 months, respectively. 7 Moreover, the choice of subsequent treatment upon progression in the COUAA-301 trial and in our series might differently affect OS duration. Our cohort of patients was, in fact, referred to us for treatment between 2011 and 2016 while the patients enrolled in the COAA-301 trial were recruited between 2008 and 2009. In consideration of this, it is possible that our patients progressing on AA plus PDN had the chance to receive new generation treatments (like cabazitaxel or enzalutamide) which have been proven to significantly prolong the survival of patients affected by CRPC.29,30 This might be the case especially for the patients who had received DX prior to AA and PDN, who represent most of the patients included in our cohort. In the patients who were CT-naïve, we observed a median PFS of 20.9 months and a median OS of 24.8 months. Median time to PSA progression was 12.2 months. Among patients recruited in the COUAA-302 trial, corresponding figures were 16.5, 34.7 and 11.1 months respectively.8,9 Also in this case, there were no major differences between the two series in terms of PFS and PSA free-survival. Apparently, OS duration in our series was much shorter than OS duration in the COUAA-302 trial. However, median follow up of our cohort was also shorter (20.9 versus 49.2 months in COUAA-302) and our survival data are not mature yet. Indeed, the percentages of patients alive at 1 and 2 years in our study (88.4 and 65.2%, respectively) do not differ much from those recorded at the same time points in the COUAA-302 trial (88 and 70%, respectively), 9 in spite of differences in patient demography [patients enrolled in the COUAA-302 trial were younger, had a higher tumor burden (median PSA level was 42 ng/ml compared with 19 ng/ml in our cohort subgroup)] and treatment administered upon progression. Therefore, we can state that the effectiveness of AA and PDN in our real-life cohort was substantially comparable with the efficacy figures achieved with this regimen in pivotal trials.
In the COUAA-301 and COUAA-302 trials, clinical benefits achieved by AA and PDN compared with PDN and placebo were obtained in all patient subgroups. However, these trials were not designed ad hoc to identify the patients who might derive the greatest benefit from AA and PDN.
In order to answer to this question, we analyzed our PFS and OS results as a function of a number of variables which have been previously shown to significantly predict for patient clinical outcome in mCRPC. 31 In our analysis, we also included two additional variables: BMI and duration of prior ADT. BMI was included because it was shown that an elevated BMI is associated both with an increased risk of cancer-specific mortality in healthy people and with a higher risk of biochemical recurrence in prostate cancer patients. 32 A trend for an increased risk of progression to CRPC was also observed in patients with a BMI > 25. 33 An association between obesity and the aggressiveness of the disease, as well as a higher incidence of complications following ADT, was observed in another study. 34 Different mechanisms, involving the insulin/IGF-1 axis, sex hormones and adipokine signaling, have been proposed to explain the association between obesity and aggressiveness of prostate cancer. 35 Addressing this issue in detail was not the scope of the present study. However, two additional considerations support our choice of including BMI among the selected covariates: (1) the metabolic dysfunction caused by ADT can accelerate CRPC and increase the risk of CV events; (2) human adipose tissue has been shown to be capable of active androgen synthesis and this, in principle, might interfere with the therapeutic activity of AA. 36
Duration of prior ADT has been associated with longer survival in patients receiving AA in a previous study. 37 In our study both BMI and the duration of previous ADT were confirmed to be associated with a longer PFS and OS after multivariable analysis. In particular, overweight patients showed a significantly increased risk both to progress and to die, which was even higher for CT-naïve patients. These findings should be interpreted with caution, due to the small numbers and the retrospective nature of our analysis. However, multivariable competitive risks analysis showed that a BMI > 25 was specifically associated with a higher risk of dying for prostate cancer, but it showed no association with prostate cancer-unrelated mortality, independently of the other covariates included in the model. Of course, these findings might deserve confirmation in larger series. As shown in Table 3, we also confirmed that a longer duration of prior ADT almost halved the risk of progression and of death. In contrast to what we expected, visceral metastases were not significantly associated with prognosis in our cohort, but this finding might be due to the limited number of patients with baseline visceral involvement. Duration of response to previous ADT did also predict for prostate cancer mortality in the competing risk model. This and the borderline predictive value of PSA level, confirm that tumor burden and biology are specific determinants of AA efficacy in CRPC. Taken all together, our data suggest that patients with a lower PSA level, an initial GS ⩽ 7, an ECOG PS 0, no pain, a duration of ADT > 43.2 months and a BMI ⩽ 25 are likely to benefit the most from AA plus PDN treatment, independently of their age, the presence of visceral metastasis and of having been previously treated or not with DX.
Safety data
AA plus PDN proved to be a well tolerated regimen among our cohort. In particular, focusing on CV and biochemical events, in CT-naïve patients we observed a lower incidence of AEs as compared with that reported in the COUAA-302 trial8,9 and only one episode of grade 3–4 hypokalemia. In the post-DX setting, we observed a higher incidence of hypertension (20% versus 10% in the CT-naïve group) which was grade 3–4 in 6.7% of patients. Furthermore, in our post-DX cohort we found a comparable incidence of hypokalemia with respect to COUAA-301 trial findings (18.7% versus 18.0%, respectively). 7 Overall, the incidence of fluid retention and cardiac disorders in our series was much lower than the incidence recorded in the two pivotal trials.7,9 Interestingly, pre-existing hypertension and CV disorders were not associated either with an increased risk of worsening CV AEs or the onset of new CV AEs. These results are consistent with those obtained in other real-life experiences; indeed, as already mentioned, one retrospective study in mCRPC patients previously treated with DX, showed that AA plus PDN can be safely administered even in patients bearing CV risk factors.14,15 A prospective evaluation of the incidence of CV events during AA administration in patients with CV comorbidities showed no change in LVEF values during AA treatment, which is consistent with our findings, but it did show worsening of pre-existing hypertension in 30% of patients. 16 In our cohort, we also evaluated whether patient age might increase the risk of CV AEs and indeed patients aged ⩾75 showed a significantly increased risk of developing fluid retention (p = 0.03) and cardiac disorders (p = 0.001) as compared with younger ones, regardless of previous administration of CT. A trend toward developing or worsening of dyslipidemia was also observed in elderly patients in our study. Interestingly, this patient subgroup did not prove to be more prone to develop diabetes. Even though a more accurate cardiologic and metabolic monitoring may be advisable among elderly patients, it is certainly reassuring that there was no difference in survival according to age. Moreover, the fact that in our study age >75 was associated with a longer PFS (both at univariate and at multivariable analysis) might suggest that the increased incidence of CV events did not interfere with patient compliance to treatment, probably for the more closely monitoring adopted in elderly patients to control these adverse conditions. Our results confirm the findings of pivotal trials7–9 and of previously mentioned ‘real-life’ experiences where elderly patients treated with AA did not show any difference in survival duration compared with younger ones.38–41 Noteworthy, patient weight did not appear to predict the incidence of CV events. Obese patients showed a slight increase in the probability of developing hypertension but a lower probability of developing CV disorders, though the role played by chance in this association cannot be ruled out, considering the very small numbers of patients developing cardiac disorders in our cohort (n = 9). Most importantly, patients developing CV AEs during treatment with AA and PDN in our cohort did not experience a worse prognosis than those who did not. Conversely, hypokalemia appeared to be associated, even after multivariable analysis, both with a longer PFS (though this trend was not statistically significant) and OS, (Figure 2; Table 7). Neither has this observation been reported before, thus requiring confirmation in larger, prospective studies, nor it is easily explainable; thus, we might only postulate that hypokalemia might represent a marker of treatment activity, to the same extent as hypertension appears to be for anti-angiogenic treatment in other solid tumors, such as renal and colorectal cancer.42,43
Conclusion
Our findings confirm that AA and PDN is an effective and well tolerated regimen also in ‘real-life’ patients, including elderly ones. Though the incidence of AEs, and especially CVEs, was lower with respect to the figures initially reported in pivotal trials, and though no evidence emerged that AEs might imply a worse clinical outcome, appropriate patient selection and monitoring is recommended. Lower PSA levels, an initial GS ⩽ 7, ECOG PS 0, absence of pain, longer duration of previous ADT manipulations and a BMI ⩽ 25 appear to be associated with a greater benefit from AA treatment, independently of patient age, presence of visceral metastasis and of patients having been previously treated or not with DX. Interestingly, patients developing treatment-related hypokalemia seem to have better outcomes as compared with those who did not. However, this finding requires confirmation in larger, possibly prospective trials. Studies focused on more specific markers able to predict for the effectiveness and safety of AA and PDN are needed in order to improve decision-making and patterns of care among patients with mCRPC. Similar studies are also warranted in hormone-naïve patients in view of the results achieved by adding upfront AA and PDN to standard ADT.
Footnotes
Acknowledgements
The authors are extremely grateful to Dr Claudia Casella (Descriptive Epidemiology Unit: Tumor Registry, San Martino Polyclinic Hospital, Institute for Cancer Research and Treatment, Genoa, Italy) for helping in data collection.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.