
Abstract
Systemic therapies for primary breast cancer have made great progress over the past two decades. However, oncologists confront an insidious and particularly difficult problem: in those patients with metastatic breast cancer, up to 50% of human epidermal growth factor 2 (HER2)-positive and 25–40% of triple-negative subtypes, brain metastases (BM) kill most of them. Fortunately, standard- of-care treatments for BM have improved rapidly, with a decline in whole brain radiation therapy and use of fractionated stereotactic radiosurgery as well as targeted therapies and immunotherapies. Meanwhile, advances in fundamental understanding of the basic biological processes of breast cancer BM (BCBM) have led to many novel experimental therapeutic strategies. In this review, we describe the most recent clinical treatment options and emerging experimental therapeutic strategies that have the potential to combat BCBM.
Introduction
Brain metastasis (BM) is an indication of poor prognosis for cancer patients with short overall survival and low quality of life. 1 The prevalence of breast cancer brain metastasis (BCBM) is increasing as treatment of primary cancers and imaging techniques improve. 2 In addition, the brain is a “sanctuary site” for breast cancer cells treated with pharmacological agents that have poor drug penetration into central nervous system (CNS). For example, among patients who received adjuvant trastuzumab (a monoclonal antibody targeting HER2) in the HERA study, the brain made up a larger proportion of initial relapse sites compared with controls. 3 Concentration of trastuzumab in cerebrospinal fluid (CSF) was detected to be 420-fold less than in sera of patients treated with trastuzumab before radiotherapy. 4 Although small molecules (e.g., neratinib, molar mass: 557.04 g/mol, or afatinib, molar mass: 485.94 g/mol) are more able to across the blood-brain barrier (BBB) than the monoclonal antibody trastuzumab (molar mass: 14,5531.5 g/mol),5,6 the discrepancy of treatment response between extracranial disease control and intracranial disease progression was also observed in metastatic HER2-positive patients treated with neratinib or afatinib,7–9 suggesting unique disease biology of BCBM and more complicated vulnerability to targeted therapies.
Indeed, BCBMs residing within the neural microenvironment confront a distinct set of structural (especially the BBB), physiological, and molecular factors, and undergo additional brain-adaptive modifications to support tumor survival and outgrowth. Recent studies focusing on tumor–neural microenvironment interactions have revealed novel therapeutic strategies, especially in repositioning existing drugs to target potent microenvironmental factors that promote tumor growth (Figure 1). Repurposing known drugs for new indications is a promising strategy to accelerate drug discovery of unmet medical need such as BCBM. Because of the profiled toxicity and pharmacokinetic information, drugs that are identified through repositioning have the potential for rapid clinical translation.10–13 In addition, other emerging clinical treatment options for BCBM patients include novel targeted therapy and immunotherapy, minimally invasive neurosurgery, and stereotactic radiotherapy (Table 1), have shown promise in many clinical studies to improve patient survival and quality of life.

Summary of recent translational therapeutic strategies in repositioning known drugs to target BCBM tumorigenic signaling especially the microenvironmental factors. Silibinin, a commercially available nutraceutical reduced BCBM in animal models and a cohort of 18 patients through suppressing STAT3 activation in the STAT3+ pro-metastatic As subpopulation. 14 Meclofenamate, a FDA-approved anti-inflammatory drug inhibited BCBM tumor growth by blocking PCDH7-Cx43 gap junction between Tu and astrocytes. 15 Edlfosine, a phase II clinical trial drug in treating leukemia with bone marrow transplants inhibited BCBM by suppressing the PCDH7-PLCβ signaling that mediates the crosstalk between astrocytes and brain-tropism CSC. 16 Letrozole, a clinical aromatase inhibitor for ER+ breast cancer treatment, decreased the large BCBM by suppressing ER+ pro-metastatic astrocytes. 17 Fludarabine, a FDA-approved chemotherapeutic drug for treatment of chronic lymphocytic leukemia, inhibited the tumorigenic property of XIST-low and the tumor suppressive M2 microglia that not only delayed onset, but also suppressed growth of BCBM. 18 CpG-C, a clinical trial TLR9 agonist, prevented BM by activating M1 microglial cells to kill and phagocytose the tumor cells during the early stages of invasion into the brain. 19
New clinical trials for BCBM patients.
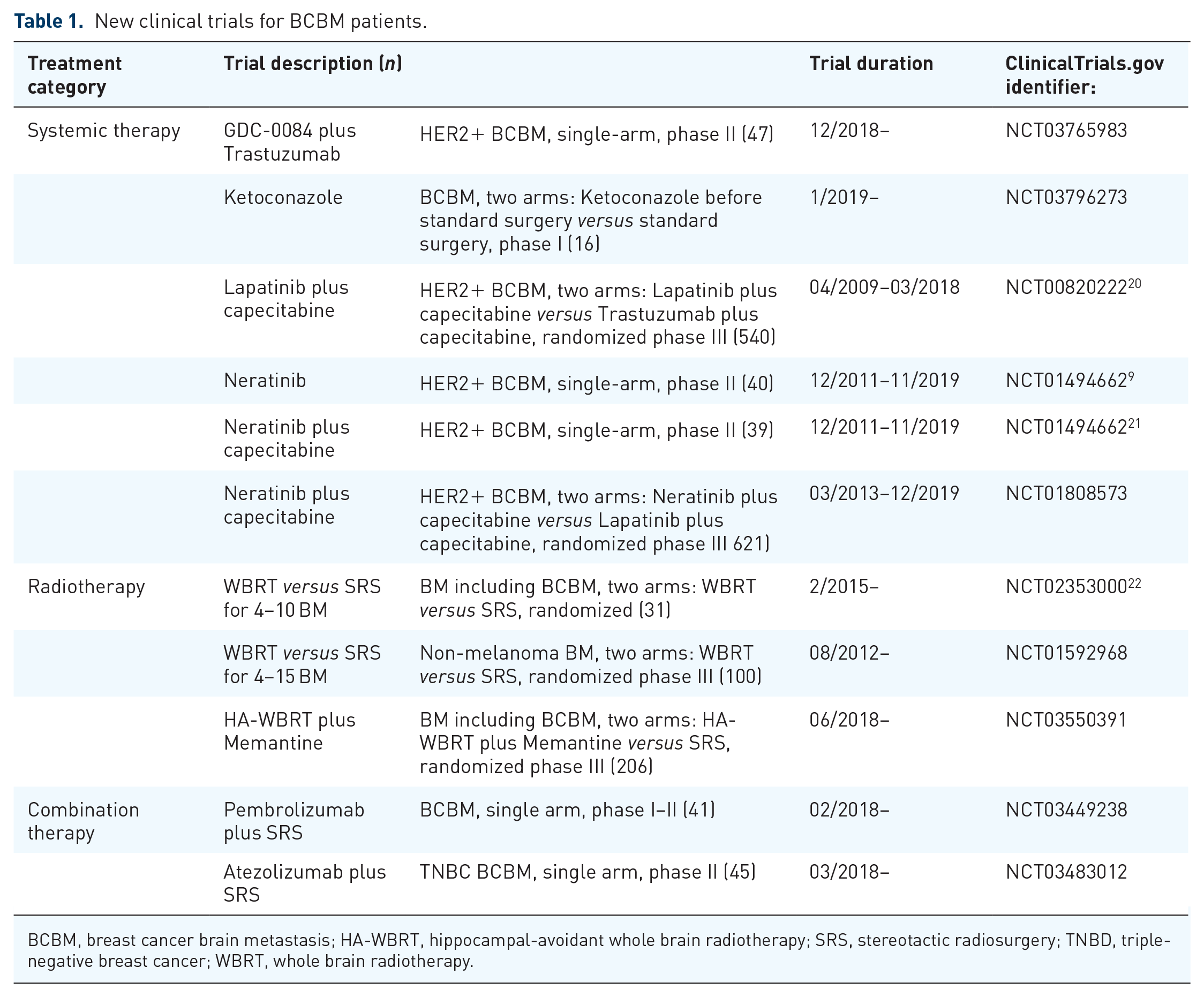
BCBM, breast cancer brain metastasis; HA-WBRT, hippocampal-avoidant whole brain radiotherapy; SRS, stereotactic radiosurgery; TNBD, triple-negative breast cancer; WBRT, whole brain radiotherapy.
Targeting tumor–neural microenvironment interactions in BCBM
As opposed to molecular mechanisms involving cancer cell–host interactions shared by multiple cancer types that result in organ specific metastasis, a highly distinct set of structural, anatomic, physiological, and molecular factors regulate metastasis to the brain. Astrocytes, the most common glial cells comprising ~50% of all human brain cells, are a well-characterized perilesional component of BCBM.23–27 Recent discoveries, including ours, provide compelling evidence that molecular crosstalk between astrocytes and cancer cells is integral to BCBM development.14–16,28
The Valiente group showed in clinical BCBM samples and xenograft mouse models, including HER2+ and triple-negative (TNBC) subtypes, that a subpopulation of reactive astrocytes with activated signal transducer and activator of transcription 3 (STAT3) contributed to the pro-metastatic microenvironment. 14 These STAT3+ astrocytes benefit metastatic breast cancer cells by impeding CD8+ lymphocytic infiltration into the metastatic area through secretion of infiltration-suppressive proteins such as vascular endothelial growth factor A (VEGF-A) and tissue inhibitor of metalloproteinases-1 (TIMP-1), and inhibiting the acquired immune response as they also express programmed cell death 1 ligand 1 (PD-L1). In addition, the STAT3+ astrocytes crosstalk with CD74+ microglia/microphages through the MIF–CD74–midkine signaling axis in promoting the brain metastatic tumor growth. To this end, silibinin, a commercially available nutraceutical that crosses the BBB to impair STAT3 activation, was used to treat BCBM animal models and a cohort of 18 patients. Silibinin alone significantly reduced experimental BM even at advanced stages of colonization. In BCBM patients treated with Silibinin, as a single agent or in combination with additional chemotherapy, the overall response rate was 75% patients, including 3 complete responses (20%) and 10 partial responses (55%). Given the safety profile and oral bioavailability, silibinin supplementation provides great hope to increase survival in BCBM patients.
Recent reports from our group and the Massagué group identified other BCBM-astrocyte crosstalk signaling focusing on protocadherin7 (PCDH7). Using TNBC patient-derived BCBM samples and animal models, we demonstrated that a brain-tropic cancer stem cell population drives tumor metastasis in the brain, and interactions with astrocytes mediated by high PCDH7 expression promoted in vivo tumor growth through PCDH7-PLCβ signaling. 16 Notably, in animal studies immuno-reactive PCDH7 expression was redetected in brain metastatic lesions in the PCDH7 shRNA group, as well as tumor surrounding astrocytes. 16 The re-expression of PCDH7 in the surviving brain metastatic tumor cells suggests that selection for tumor cell PCDH7 expression promotes cell survival and tumor growth in vivo. In late stage TNBC and HER2+ BCBMs, elevated PCDH7 expression on tumor cells was required to establish PCDH7-Cx43 gap junctions that mediated paracrine signaling between brain metastatic tumor cells and astrocytes. 15 Through the gap junction channel between both cell types, Ca 2 and secondary messenger cGAMP contribute to chemoresistance in BCBM. Cancer cells from TNBC and HER2+ breast cancer cells co-opted the gap junction connection with astrocytes to reduce their excessive calcium burden, for which the excessive intracellular calcium could be detrimental for cancer cells by triggering DNA damage and inducing apoptosis. 29 As a consequence, the decrease of intracellular calcium facilitates resistance to chemotherapy and aggressive colonization in the brain. 15 Reciprocally and initiated by the transfer of second messenger from tumor cells to astrocytes, cGAMP activated astrocytic STING, which leads to phosphorylation of IRF3, 30 and subsequently induced expression and secretion of TNFα and INFα. These two cytokines in turn activated NFκβ and STAT1 in brain metastatic cells that contribute to an accelerated proliferation and resistance to chemotherapeutic stress. 15 Two proof-of-concept therapeutic strategies were verified in the TNBC BCBM animal models, one is the repositioning of edelfosine, a phase II clinical trial drug in treating leukemia with bone marrow transplants that blocks PLCβ, and the other is the gap junction directed therapy of repositioning meclofenamate, a FDA-approved anti-inflammatory drug that inhibits Cx43 gap junction gating. To recapitulate clinical situation where BM tumors are established before treatment, edelfosine treatment in mice started when micro-metastases were detected (around 10 days post tumor cell inoculation into left ventricle). During a 15-day treatment regimen (i.p., once daily, 30 mg/kg/day), brain metastatic tumor growth was continuously suppressed in the edelfosine group, and it was noted that the formation of macro-metastases (>50 cells) in the treated mice was inhibited by 90% at the end of 15-day treatment (p < 0.01). Activations of cellular PLCβ and Ki-67-positive tumor cell proliferation were repressed remarkably by the edelfosine treatment. 16 In the same animal model, meclofenamate (i.p., once daily, 20 mg/kg/day) in combination with chemotherapeutic drug carboplatin profoundly inhibited BM. 15
Of importance, in independent studies, shRNA-mediated PCDH7 depletion in TNBC and HER2+ breast cancer cells inhibited brain metastatic growth in immunocompetent and xenograft models. This suggests that PCDH7, a brain-specific gene, may be a robust multi-functional mediator of BCBM-astrocyte crosstalk and a new potential therapeutic target. PCDH7 is a brain-specific gene.31,32
Adult human brain endothelial cells and primary microglia have no detectable, or very low, level of PCDH7 expression. 15 Primary astrocytes have moderate expression of PCDH7, whereas astrocyte PCDH7 expression exhibits a dramatic increase in response to the brain metastatic tumor insult.15,16 These data suggest that astrocytic PCDH7 has a pro-metastatic role in BCBM. Pharmacological blocking or targeting the astrocytic PCDH7 may not have profound side-effects on other brain resident cells, especially given that overexpression of PCDH7 inhibits neuronal survival. 32 To this end, we are exploring small molecules to block the PCDH7 homophilic and PCDH7-Cx43 heterophilic binding for potential BCBM treatment.
In a series of studies by the Cittelly group, estrogen receptor (ER)-positive astrocytes were pro-metastatic in BM in the TNBC subtype.33,34 Astrocytes express classical ERs (ERα and ERβ). In vitro, estrogen treatment up-regulated epidermal growth factor receptor (EGFR) ligands and brain-derived neurotrophic factor in astrocytes and activated EGFR and tropomyosin kinase receptor B in TNBC brain metastatic cells. Estrogen also stimulated release of astrocyte-derived paracrine factors to promote tumor proliferation. In TNBC BCBM mouse models, ovariectomy decreased the magnetic resonance imaging (MRI) detectable lesions by 56% compared with estrogen supplementation, and the combination of ovariectomy and letrozole further reduced the large lesions to 14.4% compared with control. 33 Letrozole is a clinical aromatase inhibitor that blocks the enzyme that produces estrogen, and is used widely for ER+ breast cancer treatment. These important findings provide a therapeutic rationale to use estrogen-depletion therapies to prevent or delay development of BM in younger women, especially letrozole and other aromatase inhibitors with good BBB permeability. 17
In addition to astrocytes, microglia, being resident macrophages of the brain, normally exhibit tumor-defensive function by phagocytosis and release of cytotoxic factors. However, the tumor-interacting microglia can be polarized into immunosuppressive and tumor-supportive roles by tumor-derived soluble factors, thereby promoting tumor progression. 35 Xing et al., identified a specific long noncoding RNA, X-inactive–specific transcript (XIST) significantly down-regulated in brain metastatic tumors from breast cancer patients and several BCBM cell lines. The researchers concluded that the loss of the XIST promotes BCBM. 18 BCBM tumor cells with reduced expression of XIST showed elevated exosomal miRNA-503, which triggered M1–M2 polarization of microglia and augmented release of immune suppressive cytokines in microglia that suppressed T-cell proliferation. The Prestwick FDA-approved drug library was screened on the XISTlow breast tumor cells and fludarabine was identified as a synthetic lethal drug in inhibiting BM. Fludarabine is an FDA-approved chemotherapeutic drug for treatment of chronic lymphocytic leukemia. However, the IC50 for fludarabine on XISTlow BCBM cells was 10-fold lower than the effective dose for leukemic cells. A low-dosing treatment (i.p., once every 2 days, 10 mg/kg) was used in BCBM mouse models, and fludarabine not only significantly delayed onset of BM, but also suppressed growth of tumor cells in the brain without notable toxicity on neuronal cells. 18
Research into the modulation of other mechanisms of BM is also emerging. For example, a recent study by Benbenishty et al. showed that prophylactic administration of CpG-C, a Toll-like receptor 9 (TLR9) agonist, significantly reduced development of BM in mouse models from lung cancer and melanoma.19,36 Systemically administered CpG-C can be taken up by brain endothelial cells, astrocytes, and microglia in mice. The CpG-C-activated microglia displayed elevated mRNA expression of apoptosis-inducing and phagocytosis-related genes and phagocytized tumor cells when microglia and tumor cells were physically contacted at early tumor invasion into the brain. Although no breast cancer model was explored in the study, the similar anti-tumor microglia mechanism among breast cancer, lung cancer, and melanoma BM should warrant investigation into the use of CpG-C in BCBM. Other experimental therapeutic strategies, including targeting various steps in metastatic cell colonization and early tumor growth, such as integrin, matrix metallopeptidase (MMP), and VEGF functions, have been reviewed by Achrol et al., 37 and promising anti-BM effects were seen in animal models. In addition, intriguing new mechanistic pathways in BCBM are continuously being explored. For example, tumor exosomal CEMIP protein was taken up by brain endothelial and microglial cells, and induced endothelial cell branching and inflammation in promoting BCBM. 38 Astrocytic sphingosine-1 phosphate receptor 3 (S1P3) up-regulated the permeability of blood–tumor barrier (BTB) through secretion of IL-6 and CCL2 and reduced endothelial cell adhesion, thus facilitating extravasation and colonization of brain metastatic tumor cells. 39 Genetically, depletion of these molecules not only showed suppression of tumor growth but also had BCBM prevention effects. Despite the lack of available therapeutic agents, these novel scientific findings will drive continued discovery and development of potential therapeutic opportunities to target these mechanisms.
In addition, targeted carrier or drug delivery systems that selectively increase drug penetration through BBB or BTB have been actively pursued for years. This strategy addresses the low and heterogeneous permeability of therapeutic agents to brain disorders including BCBM. Progress in this field has been nicely reviewed by several groups recently.40–42
Targeted therapy and immunotherapy in BCBM
In the past, BCBM patients were excluded from the clinical testing of targeted treatments because their limited life span confounded assessment of drug efficacy on overall survival. However, recent clinical trials have started to elucidate the potential utility of targeted agents, mostly on HER2-positive BCBM patients. In the newly published HER2CLIMB trial, 43 tucatinib, an investigational oral tyrosine kinase inhibitor that is highly selective for HER2 with minimal inhibition of EGFR, was combined with trastuzumab and capecitabine in patients with previously treated HER2-positive BCBM patients from 155 sites across 15 countries. Impressively, the estimated progression-free survival at 1 year was 24.9% in the tucatinib-combination group and 0% in the placebo-combination group, and the risk of disease progression or death was 52% lower in the tucatinib-combination group than in the placebo-combination group. This is the first demonstration of a drug that can prevent or delay disease progression in patients with pretreated HER2-positive breast cancer and brain metastases. The HER2CLIMB trial is important because it allowed patients with active brain metastases to enroll, which indicates that more trials need to be designed to include this patient group.
Recently, neratinib, another HER2 targeted tyrosine kinase inhibitor combined with capecitabine was shown highly active in treating HER2-positive BCBM.21,44 Nearly 50% of patients experienced an objective response, which exceeds the point for either neratinib monotherapy (8%) or capecitabine and temozolomide (18%). 9 The neratinib and capecitabine combination was active for those with prior lapatinib exposure. Lapatinib, a small molecule inhibitor of EGFR and HER2, has good penetration across the BBB, 45 but, with limited activity as a single agent for HER2-positive BCBM, it therefore has been used in combination with capecitabine. 37 A meta-analysis of 12 trials with 799 patients revealed the disease control rate of 65.1% for the lapatinib and capecitabine treatment in HER2-positive BCBM. 46 Lapatinib and capecitabine, however, have overlapping gastrointestinal toxicities, limiting clinical dose intensification and efficacy. In a recent phase I study, a new administration regimen was explored, and escalated high-dose lapatinib was well tolerated when given intermittently and sequentially with flat-dose capecitabine, and antitumor activity of such treatment regimen was noted in both CNS and non-CNS sites of disease. 47 In addition, a retrospective study evaluated the addition of concurrent lapatinib to stereotactic radiosurgery (SRS), and concluded with improved complete response rates among patients with HER2-positive BCBM. 48 The antibody drug conjugate trastuzumab-emtansine (T-DM1) is an approved second line treatment for metastatic HER2-positive tumors after trastuzumab. Patients with BMs treated in the phase III EMILIA trial had improved survival with T-DM1 compared with lapatinib plus capecitabine.49,50 Intracranial trastuzumab levels can be dramatically increased after radiation therapy, 51 and concomitant T-DM1 with whole brain radiation therapy (WBRT) induced a complete response in a patient with HER2-positive brain and leptomeningeal metastasis. 52
There are several other targeted therapies for BCBM under clinical evaluation, including GDC-0084 in combination with trastuzumab for HER2-positive BCBM [ClinicalTrials.gov identifier: NCT03765983] in which GDC-0084 is a PI3K/Akt/mTOR-pathway inhibitor; everolimus in combination with trastuzumab and vinorelbine for HER2-positive BCBM in which everolimusis a brain-permeable mTOR inhibitor 53 ; and ketoconazole in treating patients with recurrent glioma or BCBM in which ketoconazole is an antifungal drug in blocking the function of protein tGLI1 [ClinicalTrials.gov identifier: NCT03796273]. In addition, derivates of traditional chemotherapy agents could have better CNS penetration and intracranial activity. ANG 1005, which is a modified form of paclitaxel, is one such molecule showing promising activity in early clinical trials. 54 Viral vector delivery of agents like trastuzumab is another novel strategy that has promising preclinical data in BCBM prevention and treatment. 55
Immunotherapy has activity for BMs from lung cancer and melanoma,56–58 but BCBMs have a lower immune content compared with primary tumors, yet improved outcomes are associated with higher TIL content in the BCBM.59,60 Thus, strategies were proposed to alter the complex brain immune microenvironment, including concurrent SRS, bi-specific antibody armed activated T cells, 61 and HER2-chimeric antigen receptor (CAR) T cells in BCBM treatment. 62 It was hypothesized that SRS treatment would damage BCBM cancer cells and make them more visible to the immune system, and SRS plus atezolizumab (Tecentriq, a PD-L1 antibody), is currently under clinical evaluation in patients with TNBC BM [ClinicalTrials.gov identifier: NCT03483012]. The use of bi-specific antibody activated T cells or HER2-CARTs for BCBM treatment is still under experimental examination. Saul et al. showed that HER2-CARs containing the 4-1BB costimulatory domain conferred an improved tumor targeting effect and reduced T-cell exhaustion phenotype. Local intracranial delivery of these HER2-CARs showed potent in vivo antitumor activity against multifocal brain and leptomeningeal metastases in orthotopic xenograft models. 62
Minimally invasive neurosurgery for BCBM
Surgery is typically reserved for BM patients with solitary and accessible lesions, or symptomatic lesions, good neurologic function, and/or those with good systemic control of the primary tumors. Modern advances in minimally invasive neurosurgical techniques, intraoperative imaging-guided neuronavigation, and brain mapping have allowed for safer resection of BCBM, even within deep or eloquent brain regions. Stereotactic laser ablation or laser interstitial thermal therapy, which involves inserting a small laser catheter through a burr hole, have shown promise for treating inaccessible lesions or those that have undergone radiation necrosis.63–67 Similarly, convection-enhanced delivery is a minimally invasive approach using image-guided catheter placement that circumvents the limitations of BBB to potentially enhance drug delivery to BCBMs. 68 In addition, intraoperative fluorescence-guided surgery has been applied to visualize and resect aggressive microscopic tumor margin in BCBM. 69 The role of neurosurgery in the management of BCBM is evolving rapidly, and is expected to become an increasingly important part of the global management of BCBM patients, whether to alleviate the effects of symptomatic mass lesions, deliver therapy, or mitigate treatment-related toxicity. Another role for surgery stems from the observations that molecular and immunologic profiles of BM are distinct from those of the primary or non-CNS metastatic tumor sites, whereas multi-regional BMs in the same patient are similar. 70 Therefore, resection or biopsy may have an expanded indication to guide tailored therapy unique to each patient’s BCBM.
Clinical radiotherapy
Whereas surgery and systemic therapies are treatment options for selected BCBM patients, radiotherapy remains the cornerstone of treatment in most patients. Because the side effects of WBRT in cognitive deterioration and quality of life are better understood, 71 a big shift toward stereotactic radiosurgery (SRS) has occurred over the past decade. The SRS technique relies on multiple radiation beams intersecting at a target localized with three-dimensional image guidance navigation. This results in precise deliver of a high radiation dose with rapid dose fall-off to optimize treatment effects and minimize damage to any adjacent tissue. This is most commonly delivered as a single session (SRS) but can be delivered in up to five fractions (stereotactic radiotherapy to mitigate side effects in larger lesions.
Currently, SRS is an established treatment for patients with <4 BMs. 72 For patients with ⩾4 BMs, several clinical trials are ongoing, including the Netherlands randomized phase III trial [ClinicalTrials.gov identifier: NCT02353000] in comparing the standard treatment WBRT with SRS is patients with 4–10 BMs, to evaluate the primary endpoint of quality of life at 3 months after radiotherapy 22 ; another randomized phase III trial [ClinicalTrials.gov identifier: NCT01592968] at the MD Anderson Cancer Center for patients with 4–15 BMs compares SRS alone versus WBRT alone. The primary endpoints are cognitive function and local tumor control at 4 months. In addition, a recently registered randomized phase III trial [ClinicalTrials.gov identifier: NCT03550391] compares effects of receiving SRS versus hippocampal-avoidant WBRT for patients with 5–15 BMs to establish whether this approach can mitigate the cognitive morbidity associated with WBRT.
Other promising strategies include SRS combined with systemic therapy and novel applications of SRS. For example, lapatinib, which has shown improved complete response rates among patients with HER2-positive BCBM, 48 or immunotherapy pembrolizumab (Keytruda) [ClinicalTrials.gov identifier: NCT03449238] and atezolizumab in patients with TNBC BM [ClinicalTrials.gov identifier: NCT03483012]. Individualized isotoxic dose prescription (IDP) has been advocated to mitigate the risk of radionecrosis and further enhance local control probability of SRS.73–75 For large lesions not amenable to single-session treatment, staged SRS has shown promise, 76 whereas preliminary studies of re-treated lesions report promising rates of tumor control and side effects.77–79 Finally, new approaches that use metabolic and functional imaging for treatment planning may provide more precise and safe targeting for recurrent treated tumors and those near functional structures such as the corticospinal tracts. 80
Conclusion
Treatment options for BCBM continue to increase with exploitation of the molecular characterization of BCBM tumors and their interactions with the brain microenvironment. The identified repositioned drugs target BCBM tumorigenic signals can be tested in clinical settings in a fast-track way. Advances in minimally invasive neurosurgery and stereotactic radiotherapy also improve the localization of the BM treatment, improving the long-term survival and quality of life of the BCBM patients. In contrast to a one-size-fits-all approach in cancer treatment, with more and more clinical options and different therapeutics strategies becoming available, a multi-disciplinary approach for treatment decision-making is needed in order to best meet individual patient’s needs. Eventually, as prevention of BM has been seen in certain experimental therapeutic strategies in animal studies, preventive clinical studies in high-risk BCBM patients are on the horizon.
Footnotes
Acknowledgements
The authors would like to thank Dorothy Lewis and Rebecca Danforth for proofreading the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by National Institutes of Health (NIH) 1R01CA238727 to H.Z and S.T.W, and U54 CA149196, NIH U01CA188388, John S. Dunn Research Foundation, and TT and WF Chao Foundation to S.T.W. PLA Navy NO.905 Hospital Management Project to D.R. Dunn foundation to RCP.