
Abstract
Background:
The survival status of patients with breast cancer and brain metastasis (BCBM) receiving current treatments is poor.
Method:
We designed a real-world study to investigate using patients’ clinical and genetic aberrations to forecast the prognoses of BCBM patients. We recruited 146 BCBM patients and analyzed their clinical features to evaluate the overall survival (OS). For genetic testing, 30 BCBM and 165 non-brain-metastatic (BM) metastatic breast cancer (MBC) patients from Hunan Cancer Hospital, and 86 BCBM and 1416 non-BM MBC patients from the Geneplus database who received circulating tumor DNA testing, were compared and analyzed.
Results:
Ki67 >14% and >3 metastatic brain tumors were significant risk factors associated with poor OS, while chemotherapy and brain radiotherapy were beneficial factors for better OS. Compared with non-BM MBC patients, BCBM patients had more fibroblast growth factor receptor (FGFR) aberrations. The combination of FGFR, TP53 and FLT1 aberrations plus immunohistochemistry HER2-positive were associated with an increased risk of brain metastasis (AUC = 77.13%). FGFR aberration alone was not only a predictive factor (AUC = 67.90%), but also a significant risk factor for poor progression-free survival (Logrank p = 0.029). FGFR1 aberration was more frequent than other FGFR family genes in BCBM patients, and FGFR1 aberration was significantly higher in BCBM patients than non-BM MBC patients. Most FGFR1-amplified MBC patients progressed within 3 months of the late-line (>2 lines) treatment.
Conclusion:
A group of genetic events, including FGFR, TP53 and FLT1 genetic aberrations, and HER2-positivity, forecasted the occurrence of BM in breast cancers. FGFR genetic aberration alone predicted poor prognosis.
Background
Breast cancer (BC) is the most common malignancy in females. Metastases to the brain occurs in 10–16% patients with BC.1,2 Compared with hormone receptor (HR)-positive BCs, which are more likely to recur in bone, triple-negative BCs (TNBC) and HER-2 positive BCs more commonly recur in the brain. 3 BC with brain metastasis (BCBM) is a devastating cause of morbidity and mortality. The mean interval time from primary BC diagnosis to BCBM existence is about 35 months. The two main risk factors for developing BCBM are large primary tumor size and lymph node metastasis. 4 Clinically, brain metastases are treated with surgery, radiation therapy [whole brain radiation therapy (WBRT)] or stereotactic radiosurgery. In practice, no uniformly standard chemotherapy drugs are available for BCBM; in the National Comprehensive Cancer Center guideline, the category 2A recommendations include high-dose methotrexate, capecitabine, temozolomide monotherapy and cisplatin plus etoposide. 5 Despite a lack of consensus, preliminary data suggests that chemotherapy and targeting therapies after WBRT may improve survival outcomes. 6
The majority of BCBM patients receive a multimodality therapy approach, including anti
Magnetic resonance imaging (MRI) is a sensitive imaging tool which is widely used in the detection, treatment planning, and follow-up of BCBM. Circulating tumor DNA (ctDNA) testing is promising regarding to tumor treatment response and progression. 19 Derived from cell-free DNA (cfDNA), ctDNA analysis is a powerful surveillance tool for effective and continuous detection of potential tumor-related gene mutations.20–23 Compared with imaging and serum biomarkers, ctDNA testing provides valuable and sensitive information about gene mutations in tumors following drug-based therapies. 24 ctDNA does provide valuable information, but ctDNA is less likely to be informative about brain disease than extra-cranial disease. 25 However, metastatic BC (MBC) is a systematic disease, and often times BC patients develop brain metastases after metastases have appeared systemically in the lung, liver, and/or bone. 26 Our previous study reports a ctDNA gene mutation profile in MBC patients. 24 Thymidine phosphorylase (TP53), PIK3CA, and ERBB2 are the top mutated genes. Angiogenesis-related vascular endothelial growth factor (VEGF) variation is not detected. Instead, fibroblast growth factor receptor 1 (FGFR1) variations are detected in 4/68 (5.88%) of MBC patients. 24 A total of 18% of BC patients are reported to be affected with FGFR aberrations, and the most common of which is FGFR1 amplification (~14%). 27 The FGFR pathway plays a major role in angiogenesis and metastasis; FGFR alterations promote carcinogenesis, cell proliferation, angiogenesis, and drug resistance.28–30
In this study, we recruited 146 BCBM patients in our single center and retrospectively assessed the clinical risk factors. In addition, by using ctDNA testing, we examined the genetic risk factor in 195 single-center cases and in 1501 cases from Geneplus database.
Methods
BCBM patient cohort and data flow
The study was approved by the Ethics Committee at Hunan Cancer Hospital, the Affiliated Cancer Hospital of Xiangya School of Medicine/Central South University. As shown in Online Supplemental Figure S1 data flow, a total of 146 BCBM patients were enrolled in this study. Inclusion criteria were as follows: (a) CT/MRI confirmed BCBM; (b) tolerable to chemotherapy or target therapy with normal heart, liver, and renal function. Basic demographic and clinical information includes age of primary BC diagnosis, age of BCBM diagnosis, time-to-brain metastasis (TTB, from primary BC diagnosis to BCBM diagnosis), primary BC laterality, HR/HER2 status, TNM (T, primary tumor; N, nodal involvement; M, distant metastasis) stage of the primary BC at diagnosis, treatment history before BCBM diagnosis, treatment after BCBM diagnosis, and other metastatic sites.
Sample collection and plasma ctDNA testing
To investigate the genetic risk factor, plasma ctDNA test was performed. As shown in Figure S1, a total of 195 MBC patients received plasma ctDNA testing at the Department of Breast Cancer Medical Oncology in Hunan Cancer Hospital. Other inclusion criteria included: (a) ⩾1 measurable metastatic lesion; (b) age 18–70 years old; (c) normal liver and renal function (aspartate aminotransferase (AST) and alanine aminotransferase (ALT) > 0.5 upper limit of normal value (ULN), total bilirubin (TBIL) < 1.5 ULN, and creatinin (Cr) < 1.0 ULN); (d) routine-blood test: neutrophil count >2.0 × 109/l, Hb >11 g/l, platelet count >100 × 109/l. The exclusion criteria were: (a) serious heart disease; (b) multiple primary malignancies; (c) immune-deficiency; (d) organ-transplantation history. The plasma ctDNA testing study was also approved by the Ethics Committee of Hunan Cancer Hospital. Of these 195 patients, 30 were BCBM patients as described above, whereas the other 165 were non-brain-metastatic (BM) MBC patients. To compare the different genetic aberrations between BCBM patients and non-BM MBC patients, 1:1 propensity score matching (PSM) was performed to reduce the potential bias between these two subgroups. Propensity scores were calculated through logistic regression with covariates including age, treatment history, and metastatic disease (lung, liver, bone, and lymph node metastases) and recurrent disease. After PSM, 28 BCBM patients and 28 non-BM MBC patients were selected for genetic aberration comparison (heatmap).
From 2016, the Geneplus database pool collected 1501 BC samples; among these BC patients, 86 were BCBM patients. We collected the peripheral blood samples from the patients, and then extracted the DNA content according to the protocol. 24 We sequenced the genomic DNA (gDNA) and used the gDNA sequence as the control.
Target capture, next-generation sequencing, and data analysis
Sequencing libraries of ctDNA were prepared using the DNA Library Preparation Kit for Illumina (New England Biolabs, Ipswich, MA, USA). Custom biotinylated oligonucleotide probes (IDT, Coralville, IA, USA) covering the exons of 1021 genes that are highly mutated in 12 common solid tumors were used for hybrid capture, as described previously. 31 The Illumina HiSeq 3000 Sequencing System (Illumina, San Diego, CA, USA) was used for DNA sequencing with a 2 × 101-bp paired-end strategy, as described previously. 24
Terminal adaptor sequences were removed from the raw sequencing data. Subsequently, reads with more than 50% low-quality bases, or more than 50% undefined bases, were discarded. The remaining reads were mapped to the reference human genome (hg19) using the Burrows-Wheel Aligner with default parameters. Picard’s Mark Duplicates tool (version 1.98) was used to identify duplicate reads. Local realignment and quality recalibration were performed using the Gene Analysis Toolkit. Single-nucleotide variants and small insertions and deletions were called using the MuTect2 algorithm, and further filtration and validation was performed according to established criteria. 31 The Contra algorithm was used to identify somatic copy-number alterations defined using the ratio between the adjusted depths of ctDNA and control gDNA. After automatic calling, candidate variants were manually validated using an online visualization tool.
ctDNA gene aberration frequency
Total cfDNA included ctDNA and other normal cfDNA. Aberrations in ctDNA were identified by comparing the reference genome (hg19) and gDNA. The ctDNA aberration frequency was defined as the proportion of ctDNA gene aberrations in the total cfDNA.
Statistical analyses
Categorical variables were recorded as counts with percentage, and continuous variables were calculated as the mean with standard deviation and median with interquartile range. Chi-square tests were used to compare categorical variables between subgroups. When the sample size was less than five in the comparing subgroup, Fisher’s exact test were applied. Mentel–Haenszel chi-square tests were used when the number of compared subgroups was more than two. To compare continuous variables with symmetrical distributions across subgroups, an analysis of variance test was used. Both the univariate and multivariate Cox proportional hazards regression analyses were used to evaluate the prognostic factors for OS. Log rank tests and drawn Kaplan–Meier curves were also performed to assess the overall survival OS.
To search for significant ctDNA aberrations for BCBM, R package “ComplexHeatmap” was applied to rank the hot genetic aberrations in PSM BCBM and non-BM MBC subgroups. The top aberrations were put into a logistic model for BM prediction. A receiver operating characteristic (ROC) curve was drawn to determine the areas under the ROC curve (AUC) for BM. All statistical analyses were conducted by using SAS 9.4 or R 3.6.0 software. All tests of hypotheses were two-tailed and conducted at a significance level of 0.05 and at a marginal significant level of 0.15.
Results
Clinical risk factors for poor prognosis in BCBM patients
For the 146 recruited BCBM patients, the mean age at BC first diagnosis was 45.30 (±9.80) years old and the mean age at BCBM diagnosis was 48.48 (±9.64) years old. The mean TTB was 3.18 (±2.98) years (Online Supplemental Table S1). A total of 64.83% BCBM patients had bone metastasis and 76.56% BCBM patients had visceral metastasis. Both univariate and multivariate Cox regression analyses were performed to evaluate the potential clinical risk factors for poor OS in BCBM patients. Ki67 > 14% and metastatic brain tumors >3 were significant risk factor for OS in both univariate and multivariate Cox regression analyses (Table 1). Brain radiotherapy and chemotherapy after BM diagnosis were significant beneficial factors for longer OS in both univariate and multivariate Cox regression analyses. In multivariate Cox regression analysis, HER2-positive was a marginally significant favorable factor for OS (p = 0.10, Table 1). A Kaplan–Meier curve with Logrank test analyses showed that the median OS of all the enrolled 146 BCBM patients was approximately 31.8 months (Online Supplemental Figure S2a). The OS were longer in the patients with ⩽3 metastatic brain tumors than in the patients with >3 metastatic brain tumors (Logrank test p = 0.04, Online Supplemental Figure S2b). In the patients with Ki-67 ⩽ 14%, the OS were longer than in the patients with Ki-67 > 14% (Online Supplemental Figure S2c). After 18 months, the OS was longer in the patients with HER2 positive as compared with that of the patients with HER2 negative (Figure S2d).
Univariate and multivariate analysis of the clinical risk factors for OS.

Age at diagnosis was evaluated by using univariate Cox regression; but this variable did not exist in the multivariate model because age at brain metastasis and TTB were analyzed in a multivariate model (Age at diagnosis=Age at brain metastasis-TTB).
TTB indicated the time from diagnosis of BC to the diagnosis time of brain metastasis.
Capecitabine usage represents the capecitabine usage history before or after BCBM diagnosis.
Other metastasis indicated the metastatic sites other than brain.
BC, breast cancer; BCBM, breast cancer and brain metastasis; CI, confidence interval; ER, estrogen receptor; HER2, human epidermal growth factor receptor-2; PR, progesterone receptor; TTB, time-to-brain metastasis.
Genetic aberration of BCBM patients
BCBM group and non-BM MBC group had distinct ctDNA aberration patterns (Figure 1). BCBM patients had a significantly higher FGFR aberration rate compared with non-BM MBC patients (32.14% versus 3.57%, Fisher’s Exact test p = 0.01). FLT1 gene aberration was also higher in BCBM patients, while ALK, CCNE1 and CDK12 aberrations were more frequent in non-BM MBC patients.

Circulating tumor DNA gene mutation profiles for matched 28 brain metastatic breast cancer (BC) patients (a) and 28 non-brain-metastatic metastatic BC patients (b).
Compared with non-BM MBC patients, more BCBM patients were HER2-positive (40% versus 23.75%, p = 0.06, Table S2), and more BCBM patients had bone or liver metastases (p = 0.04 and p = 0.001, respectively). Based on these features, a panel of genetic events (including aberrant FGFR, TP53, FLT1, and wild-type ALK, CDK12 and CCNE1) and HER2-positive were correlated with an increased risk of BM (AUC = 0.8050, Online Supplemental Figure S3a). An even smaller panel of genetic aberrations (FGFR, TP53, FLT1) and HER2-positive were still significantly correlated with an increased risk of BM (AUC = 0.7713). But such a panel of genetic and HER2-positive events was less likely correlated with liver, lung, bone, and lymph node metastases (AUC: 0.6136 ~ 0.7075, Online Supplemental Figure S3b–e).
Differences of metastases/recurrence between FGFR-aberrant group and wild-type FGFR group.

p-values were calculated by using Chi-square tests or Fisher’s exact tests (n < 5) for categorical variables.
FGFR aberration in MBC patients
FGFR pathway plays a major role in angiogenesis, metastasis, cell proliferation and drug resistance.28–30 In squamous cell lung cancer and BC, FGFR inhibitors showed promising antitumor activity, especially for patients with FGFR1 and/or FGFR3 amplification. 32 Here, among 195 MBC patients, FGFR aberration was not only significantly related to poor PFS (Logrank test p = 0.029, Figure 2), but also had AUC of 0.6790 in predicting brain metastases (Online Supplemental Figure S3b–e), suggesting a strong correlation of FGFR aberration with poor prognosis and brain metastases. Compared with non-FGFR aberrant group, FGFR-aberrant group had significantly more brain, liver, lung, and lymph node metastatic patients (p < 0.05, Table 2).

Kaplan–Meier curves for progression-free survival (PFS) probabilities (probs.) stratified by circulating tumor DNA FGFR aberrations.
Among 197 MBC patients, 22 patients had FGFR aberrations, including 14 FGFR1 aberrations, 4 FGFR2 aberrations, 3 FGFR3 aberrations and 1 FGFR4 aberration (Figure 3). Besides TP53 and PIK3CA, MAP3K1 mutation was the most frequent in FGFR-aberrant patients (Figure 3 and Table 3, p = 0.001). A small panel of genetic aberrations (including TP53, PIK3CA, MAP3K1, ESR1, and DNMT3A) could potently predict the FGFR aberration in MBC patients (AUC = 0.7349, Online Supplemental Figure S3f). Our findings suggested that FGFR aberration was coupled with multiple oncogenic pathways and drug-resistant pathways, such MAPK/ERK signaling pathway and mTOR pathway. 33
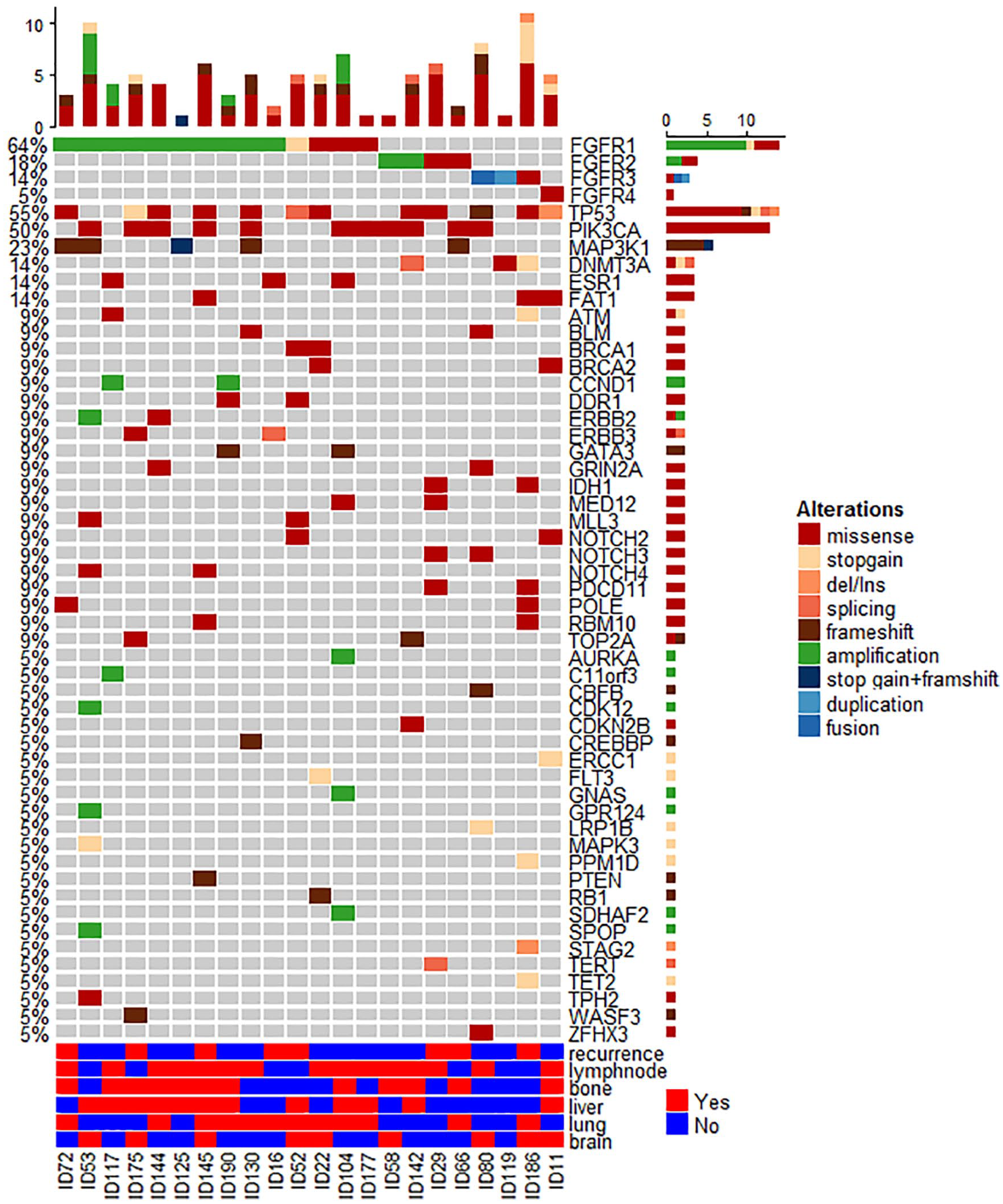
Circulating tumor DNA gene mutation profiles (top) and metastases (bottom) for 22 FGFR-aberrant metastatic breast cancer patients.
Differences of ctDNA mutation pattern between FGFR-aberrant group and wild-type group.

p-values were calculated by using Chi-square tests or Fisher’s exact tests (n < 5) for categorical variables.
FGFR1 aberration increased in MBC patients with brain metastases
FGFR1 aberration was the most frequent FGFR aberration in BCBM patients (Figure 3). To further explore the FGFR1 aberration pattern in MBC patients, we used ctDNA surveillance data from Geneplus database. Among 1501 BC patients in Geneplus database (Table 4), 379 patients had bone metastases but the FGFR1 aberration rate was almost the same with non-bone metastatic BC patients (4.75% versus 3.48%, p = 0.26). In lung metastatic BC patients, the FGFR1 aberration was significantly higher than the rate in non-lung metastatic BC patients (5.83% versus 3.26%, p = 0.04). For liver metastatic and brain metastatic BC patients, the FGFR1 aberration rates were even higher (8.18% and 8.14%, respectively), significantly higher than those without liver- and brain-metastases (p < 0.0001 and p = 0.03, respectively, Table 4). Based on these findings, we hypothesized that patients with more aggressive metastases would have higher FGFR1 aberration rate.
FGFR1 aberration rate comparison in bone-, brain-, lung-, and liver-metastatic breast cancer patients in Geneplus database.

p-values were calculated by using Chi-square tests or Fisher’s exact tests (n < 5) for categorical variables.
Among 57 FGFR1-aberrant BC patients from Geneplus database, 61 FGFR1 aberrations were identified. More than half were FGFR1 amplification (35/61 [57.38%], Online Supplemental Table S3), one (1.64%) was splicing variation, three (4.92%) were stop-gain mutations, and the rest twenty-two (36.07%) were missense mutations. Among seven FGFR1-aberrant BCBM patients from Geneplus database, eight FGFR1 aberrations were identified. Five (62.5%) were copy number amplification, one (12.5%) was stop-gain mutation and two (25.0%) were missense mutations. Among 14 FGFR1 aberrant BCBM patients (Figure 3), ten were amplification, one was stop-gain mutation and three were missense mutations. The average level of FGFR1 amplification was 4.05 (±2.32) copy number. The median level of FGFR1 amplification was 3.2 [range = (2.1, 10)] copy number.
FGFR aberrations predict poor PFS
Kaplan–Meier curve with lifetest showed that FGFR aberrations were also significantly related to poor PFS (Logrank test p = 0.029, Figure 2), suggesting a strong correlation of FGFR aberration with poor treatment response. The median PFS for FGFR-wild type patients and FGFR-aberrant patients was 7.5 (95% CI = 5.3–9.3) months and 4.7 (95% CI = 2.0–7.1) months, respectively. As shown in Table 5, 13/18 (72%) FGFR aberrant MBC patients progressed within 6 months. 60% FGFR1-amplified patients progressed within 3 months. Only one FGFR1 amplified HR+/HER2+ patient (ID53) with capecitabine + lapatinib + Herceptin treatment had a PFS longer than 6 months, and the ctDNA surveillance data also suggested a decrease in tumor mutation burden. The treatment response for FGFR1 stop-gain and missense mutant patients (ID52, 22, 104 and 177) was better than FGFR1-amplified patients, with a longer PFS (patients with PFS > 6 months were highlighted in red). Besides FGFR1 amplification, FGFR2 and FGFR3 aberrant patients also had short PFS, except one FGFR2-amplified patient with Exemestane plus Chidamide treatment (ID58). Consistent to the RECIST evaluation, ctDNA surveillance showed FGFR aberration sustained or increased in resistant patients (PFS < 6 months) and FGFR aberration decreased in sensitive patients (PFS > 6 months, Table 5).
Treatment response for BC patients with FGFR aberrations.

Patients with PFS > 6months were highlighted in red.
Level of amplification indicated the copy number of FGFR1/2 gene amplifications.
ctDNA surveillance represented the change trend of aberrant levels of FGFR genes in response of treatment, detected by ctDNA testing. Increase indicated an increase of FGFR aberration during treatment; decrease indicated the decreasing trend of FGFR aberration during treatment.
Progression indicated whether patient progressed (1) or not (0) till the date of last follow-up.
PFS represented the progression-free survival (months) for progressed patients (progression = 1), or the duration to the date of last follow-up for censored patients (progression = 0).
COSMIC record represented the pathological effect of FGFR mutations that were recorded in COSMIC.
BC, breast cancer; BM, brain metastasis; COSMIC, Catalogue Of Somatic Mutations In Cancer; ctDNA, circulating tumor DNA; HER2, human epidermal growth factor receptor-2; HR+/-, hormone receptor positive or negative; PFS, progression-free survival; TNBC, triple-negative breast cancer.
Specifically, FGFR1 missense mutant HR-positive MBC patient had longer PFS than FGFR1 amplified HR-positive MBC patient. ID144 and ID177 were both HR-positive MBC patients with CDK4/6 inhibitor plus Fulvestrant treatment. ID144 had FGFR1 amplification and progressed within 2 months of treatment. ID177 had FGFR1 p.N546K missense mutation, and she kept partial response for more than 1 year (Table 4). Everolimus plus exemetane also showed potency in FGFR1 p.N546K missense mutant HR-positive patient (ID104). Compared to epirubicin plus cyclophosphamide plus taxel (ECT) regimen (ID142), chidamide plus exemestane was more effective in FGFR2-amplified HR-positive patient (ID58). By using the ctDNA test, we could find more specific drug-resistant mutations, such as ESR1, PIK3CA p.E545K/E525K mutations, FGFR1 amplification, etc.
FGFR aberrations concentrated in HR-positive BCBM patients
Compared to non-BM MBC patients, more BCBM patients were HER2-positive (40% versus 23.75%, p = 0.06, Table S2). But compared with FGFR-wild type patients, more FGFR-aberrant patients were ER-positive or PR-positive (ER: 68.18% versus 48.55%, p = 0.08; PR: 68.18% versus 43.93%, p = 0.03; Table S4). Both FGFR aberration and HER2-positive were correlated with BM, but their combination showed a more significant correlation. As shown in Online Supplemental Figure S3a, the combination of FGFR aberration and HER2-positive was significantly correlated with the increased risk of BM (AUC = 0.7228), but such a correlation of individual aberration was not as significant as their combination (FGFR aberration alone AUC = 0.6790, HER2-positive alone AUC = 0.5431, Figure S3A).
Discussion
In practice, we found that some other brain metastases sequentially occurred after bone or other visceral metastases, especially in HR-positive BC patients, suggesting brain metastases as the final deadly stage for this group of patients; some brain metastases appeared earlier than bone and other visceral metastases, especially in HER2-positive BC patients. In this study, we found that FGFR aberrations concentrated in HR-positive patients (Online Supplemental Table S4); the FGFR aberrant group also had significantly more liver, lung, and brain metastases than the non-FGFR aberrant group (Table 3), implying a role of FGFR aberration in the late stage (migration and metastases) of HR-positive patients (especially in luminal B subtype Ki > 14%). HER2 was another important factor related to BM: the proportion of HER2-positive tumors was higher in BCBM patients, compared with non-BM MBC patients (Online Supplemental Table S2). The combination of HER2-positive and FGFR aberration could reach an AUC of 72.28% in the prediction of brain metastases (Online Supplemental Figure S3a), indicating that 72.28% BCBMs were either HER2-positive and/or FGFR-aberrant.
Genetic risk factor FGFR aberration was identified to relate to BCBM in both our single-center and Geneplus database. Similarly, in the brain metastases of lung adenocarcinomas, FGFR1 amplification is also reported to be higher than the expected rate. 44 FGFR1 amplification is identified in up to 10% of all BCs, 16–27% of luminal B type BCs, and is correlated with endocrine therapy resistance.35,36 In HER2-positive BCs, the co-amplification of FGFR1, ERBB1, and ERBB2 results in a worse prognosis compared with patients with individual amplification or without amplification. 45 In this study, among 22 detected FGFR-aberrant patients, 16 were HR-positive MBC patients (14 were HR+/HER2- and 2 were HR+/HER2+), 5 were TNBC and 1 was HR–/HER2+ (Table 5). Moreover, ctDNA FGFR aberrations were more frequently detected in ER-positive [15/99 (15.15%) versus 7/96 (7.29%), p = 0.08] or PR-positive [15/91 (16.48%) versus 7/104 (6.73%), p = 0.03, Online Supplemental Table S2] MBC patients than ER-negative or PR-negative MBC patients. FGFR aberrant HR+/HER2- patients had short PFS and poor drug response (Table 5), suggesting FGFR aberrations might result in therapy resistance and tumor progression in HR-positive MBC patients. Among 22 detected FGFR-aberrant patients, 5 mutations were not ones that were known to be pathogenic (no record in Catalogue Of Somatic Mutations In Cancer), including FGFR1 p.G459R missense mutation, FGFR2 p.V463D missense mutation, FGFR3 p.l16_A18dup frameshift mutation, FGFR3 p.R571W missense mutation, and FGFR4 p.R3128 missense mutation (Table 5). Some patients with these non-pathogenic mutations had poor response to anti-cancer treatment, so in future we need to focus on the function of these mutations.
Recently, due to the application of new targeting agents, such as pertuzumab, ado-trastuzumab emtansine, and lapatinib, the survival outcome has been improved for HER2-positive BC patients with brain metastases. Anti-HER2 therapies could extend the median OS from a few months up to 16–20 months.46,47 Lapatinib plus capecitabine regimen is, at present, the most effective option for HER2-postive BCBM patients, with favorable tumor response, disease control, and survival rates.10,48,49 Lapatinib is a lipophilic, small-molecular inhibitor of EGFR and HER2. 50 For patient ID53 in this study, we found that the brain metastatic lesion shrank after capecitabine plus lapatinib and trastuzumab treatment. Besides lapatinib, a recent study suggests neratinib plus capecitabine is active against refractory HER2-positive BCBM 51 ; Tucatinib in combination with capecitabine and trastuzumab also shows preliminary anti-tumor activity in advanced HER2-positive BCBMs 48 (HER2Climb trial to be presented at the San Antonio Breast Cancer Symposium 2019). In addition, pyrotinib plus capecitabine exhibits efficacy in HER2-positive BCBM (Phoenix TRAIL, 2019 American Society of Clinical Oncology).
Besides FGFR, TP overexpression correlates with the pro-angiogenic (VEGF) to promote angiogenesis and metastasis in human tumor tissues.52,53 Since capecitabine is a prodrug which is activated to 5-fluorocytidine by carboxylesterase, cytidine-deaminase and TP, capecitabine is supposed to be more effective in TP-positive tumors, including BC. 52 In this study, capecitabine-based treatment showed activity in FGFR-aberrant BCBM patients (ID52 and 53), suggesting a potential crosstalk of TP and FGFR in BCBM. In HER2-positive BCBM patients, lapatinib (small molecule tyrosine kinase inhibitor) is particularly active when combining with capecitabine. 54 By using the clinical and genetic features, we successfully constructed BM prediction models. Both FGFR aberration and HER2-positive were important elements in the prediction model.
Novelty and impact statement
A group of genetic events could forecast the occurrence of brain metastases in BCs (BCBM), including FGFR, TP53 and FLT1 genetic aberrations, and HER2-positive. FGFR aberration alone not only increased BCBM, but also was associated with poor prognosis in metastatic BCs (MBC). FGFR aberration, especially FGFR1 amplification, correlated with short progression-free survival in MBC patients.
Supplemental Material
Table_S1 – Supplemental material for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients
Supplemental material, Table_S1 for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients by Ning Xie, Can Tian, Hui Wu, Xiaohong Yang, Liping liu, Jing Li, Huawu Xiao, Jianxiang Gao, Jun Lu, Xuming Hu, Min Cao, Zhengrong Shui, Yu Tang, Xiao Wang, Jianbo Yang, Zhe-Yu Hu and Quchang Ouyang in Therapeutic Advances in Medical Oncology
Supplemental Material
Table_S2 – Supplemental material for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients
Supplemental material, Table_S2 for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients by Ning Xie, Can Tian, Hui Wu, Xiaohong Yang, Liping liu, Jing Li, Huawu Xiao, Jianxiang Gao, Jun Lu, Xuming Hu, Min Cao, Zhengrong Shui, Yu Tang, Xiao Wang, Jianbo Yang, Zhe-Yu Hu and Quchang Ouyang in Therapeutic Advances in Medical Oncology
Supplemental Material
Table_S3 – Supplemental material for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients
Supplemental material, Table_S3 for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients by Ning Xie, Can Tian, Hui Wu, Xiaohong Yang, Liping liu, Jing Li, Huawu Xiao, Jianxiang Gao, Jun Lu, Xuming Hu, Min Cao, Zhengrong Shui, Yu Tang, Xiao Wang, Jianbo Yang, Zhe-Yu Hu and Quchang Ouyang in Therapeutic Advances in Medical Oncology
Supplemental Material
Table_S4_FGFR – Supplemental material for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients
Supplemental material, Table_S4_FGFR for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients by Ning Xie, Can Tian, Hui Wu, Xiaohong Yang, Liping liu, Jing Li, Huawu Xiao, Jianxiang Gao, Jun Lu, Xuming Hu, Min Cao, Zhengrong Shui, Yu Tang, Xiao Wang, Jianbo Yang, Zhe-Yu Hu and Quchang Ouyang in Therapeutic Advances in Medical Oncology
Supplemental Material
Table_S5-brain – Supplemental material for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients
Supplemental material, Table_S5-brain for FGFR aberrations increase the risk of brain metastases and predict poor prognosis in metastatic breast cancer patients by Ning Xie, Can Tian, Hui Wu, Xiaohong Yang, Liping liu, Jing Li, Huawu Xiao, Jianxiang Gao, Jun Lu, Xuming Hu, Min Cao, Zhengrong Shui, Yu Tang, Xiao Wang, Jianbo Yang, Zhe-Yu Hu and Quchang Ouyang in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
We would like to thank the researchers from Geneplus Beijing Institute as these individuals sequenced all patients’ ctDNA and gDNA samples for this study.
Author note
Jianbo Yang is also affiliated with Fujian Medical University Union Hospital, Fuzhou, China.
Author contributions
Dr. Quchang Ouyang and Zhe-Yu Hu have the full access to all data in the study and take responsibility for the integrity and accuracy of the data analysis. Study concept and design: Zhe-Yu Hu, Quchang Ouyang. Data acquisition: All authors. Data analysis and interpretation: Zhe-Yu Hu and Quchang Ouyang. Drafting of the manuscript: Zhe-Yu Hu. Critical revision of the manuscript for important intellectual content: All authors
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The study was approved by the Ethics Committee at Hunan Cancer Hospital, the Affiliated Cancer Hospital of Xiangya School of Medicine/Central South University. The ethical board approval number is 2018119. The authors declare that they have obtained ethical approval and patients consent to participate.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Hunan Provincial Natural Science Youth Foundation Project Grant No.2019JJ50356 (Recipient: Zhe-Yu Hu); Hunan Provincial Health and Sanitation Committee Project Grant No. C2019070 (Recipient: Zhe-Yu Hu); Key Research Program in Hunan Social Development Grant No. 2019SK2032 (Recipient: Zhe-Yu Hu); Changsha Science and Technology Project Program No.30749 (Recipient: Zhe-Yu Hu).
Statement about data availability
We used the data from Geneplus database and from the Hunan Cancer Hospital. Geneplus database is not a public database. Its data will be made available upon reasonable request. ctDNA data from Hunan Cancer Hospital is available in supplemental Table S5 (BM patients) and ![]() (non-BM MBC patients).
(non-BM MBC patients).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.