
Abstract
Background:
Ureteral rest refers to the removal of hardware across a ureteral stricture, allowing for stricture maturation and stabilization, before ureteral reconstruction.
Objectives:
We aimed to assess the potential impact of ureteral rest on lower urinary tract symptoms (LUTS) and health-related quality of life (HRQOL) in patients undergoing ureteral rest.
Design:
Prospective, longitudinal, self-controlled study
Methods:
We included patients undergoing ureteral reconstruction between April 2022 and April 2025. We defined ureteral rest as replacing an indwelling double-J stent (DJS) with a percutaneous nephrostomy tube (PCN) prior to ureteral reconstruction. Primary outcomes were patient-reported LUTS (via International Prostate Symptom Score) and HRQOL (via Patient-Reported Outcomes Measurement Information System 29 v2.0). The secondary outcome was the incidence of urinary tract infections (UTIs). Questionnaires were completed prior to initiating ureteral rest (with a DJS) and after at least 3 weeks of ureteral rest (with a PCN). Continuous and categorical variables were compared using paired t-tests and chi-squared tests, respectively.
Results:
Thirty-five patients met our study’s inclusion criteria. With regard to LUTS, patients undergoing ureteral rest were found to have reduced urinary frequency (p = 0.001), straining (p = 0.03), and urgency (p = 0.0002). With regard to HRQOL, patients undergoing ureteral rest were found to have improved sleep disturbance (p = 0.04). There was no difference in UTI rates before and after ureteral rest (p = 0.48).
Conclusion:
Patients undergoing ureteral rest prior to ureteral reconstruction may experience improvements in LUTS without compromising HRQOL outcomes or increasing the risk of UTIs.
Plain Language Summary
Why was the study done? Patients with ureteral stricture disease often need reconstructive surgery. Before surgery, it is often recommended to remove the internal ureteral stent (called a double J stent) and place a percutaneous nephrostomy or PCN tube temporarily to drain urine. Termed “ureteral rest” this period has been shown to improve surgical outcomes. However, many patients worry that the external tube and bag will decrease their quality of life. This study wanted to understand how this change affects urinary symptoms, quality of life, and infection risk before surgery. What did the researchers do? The team followed 35 patients who had their internal ureteral stent replaced with PCN tube for about six weeks before ureter surgery. They asked patients to complete surveys about urinary symptoms and quality of life both before and during this rest period. What did the researchers find? Patients had fewer urinary symptoms like needing to urinate less often, with less urgency, and straining to urinate after switching to the PCN. They also reported better sleep. Other aspects of physical and mental health stayed the same, and switching to the PCN did not increase the risk of urinary infections. What do the findings mean? This study shows that undergoing ureteral rest may not decrease quality of life. These results can help reassure patients and improve conversations between doctors and patients when planning ureteral reconstructive surgery. The change may not only help the surgery succeed but also reduce discomfort before the operation.
Introduction
The most definitive treatment option for patients with ureteral stricture disease (USD) is surgical reconstruction. 1 However, USD may be initially managed with decompression using a double-J stent (DJS). Maintaining a DJS during ureteral reconstruction can be problematic because it may dilate the ureteral stricture, preventing the surgeon from accurately determining stricture margins and luminal caliber. The theory behind ureteral rest parallels the concept of urethral rest, a well-established principle2–5 for optimizing stricture maturation and staging in the management of urethral stricture disease. In 2021, Lee et al. introduced the concept of ureteral rest, which was defined as the absence of hardware across a ureteral stricture ⩾4 weeks before robotic reconstruction. Patients undergoing ureteral rest were associated with a 20% increase in overall surgical success rates. 6
Despite counseling about improved surgical outcomes following ureteral rest, patients may be reluctant to exchange their existing DJS for a percutaneous nephrostomy (PCN) tube due to quality-of-life (QOL) concerns related to potential symptoms, cosmesis, and management of an external appliance. In the literature pertaining to nephrolithiasis, Shoshany et al. found that while patients with PCN tubes initially experienced less mobility and increased hygiene issues, these improved over time. By contrast, patients with DJS had persistent urinary discomfort, leading to lower overall QOL. 7 Mokhamlji et al. 8 further reported that PCN tubes required less analgesic use and a shorter indwelling time, with QOL improving for PCN patients but worsening for DJS patients. In another study by Joshi et al., they reported no significant QOL difference between PCN and DJS, though DJS patients had more urinary symptoms, and PCN patients needed more care assistance. 9 While these studies have examined differences in QOL and pain between PCN tubes and DJS in the management of nephrolithiasis, there remains a paucity of literature focusing on the QOL burden of PCN tubes versus DJS in the management of USD.
Identifying any QOL differences between PCN tubes and DJS in USD may assist clinicians in counseling patients regarding the risks and benefits of undergoing ureteral rest in anticipation of ureteral reconstruction. Exploring the benefits of ureteral rest has become increasingly relevant with the growing use of robotic ureteral reconstruction. Flegar et al. reported a steady increase in minimally invasive ureteral reconstruction procedures in Germany, from 0.2% in 2009 to 18.3% in 2022. The purpose of our study was to compare lower urinary tract symptoms (LUTS) and patient health-related quality of life (HRQOL) before and after a period of ureteral rest in patients undergoing ureteral reconstruction. Given the previous literature regarding nephrolithiasis, we hypothesize that patients with DJS will experience worse LUTS compared to those with PCN tubes, but that both groups will have similar HRQOL.
Materials and methods
We conducted an Institutional Review Board-approved prospective, longitudinal study from April 2022 to April 2025 to evaluate the impact of ureteral rest on LUTS and HRQOL in patients undergoing ureteral reconstruction for a single unilateral ureteral stricture. Eligible participants included adults aged 18 years or older who were scheduled to undergo ureteral reconstruction for a unilateral ureteral stricture and who had undergone exchange of a DJS for a PCN tube for at least 6 weeks prior to surgery. All participants were required to be able to complete the International Prostate Symptom Score (IPSS) and Patient-Reported Outcomes Measurement Information System (PROMIS) 29 v2.0 (PROMIS Health Organization, River Forest, Illinois, USA) questionnaires in English. The requirement for informed consent was waived by the IRB due to the minimal-risk nature of the study and the use of de-identified patient data collected as part of standard clinical care. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. Patients were excluded if they had bilateral ureteral stricture disease, ureteroenteric strictures, or no prior ureteral hardware. We also excluded patients who were referred with a PCN already in place, patients whose DJS was removed without subsequent PCN exchange, and those with incomplete or missing questionnaire data. All PCN tubes were terminated within the renal pelvis, and there was no component present in any portion of the ureter.
The study’s primary outcomes were changes in LUTS and HRQOL before and after at least the first 3 weeks of the ureteral rest protocol. LUTS were assessed using the International Prostate Symptom Score (IPSS: frequency, urgency, nocturia, incomplete emptying, intermittency, weak stream, urinary symptom QOL, and straining). 10 HRQOL was measured using the PROMIS 29 v2.0 profile, which includes domains such as physical function, anxiety, depression, fatigue, sleep disturbance, pain interference, participation in social roles and activities, and pain intensity. 11 The secondary outcome was the incidence of urinary tract infections (UTIs) during the study period. We defined UTI as symptoms during the study period associated with a positive urine culture, such as fever, dysuria, flank pain, and bladder pain. Patients completed the IPSS and PROMIS 29 v2.0 questionnaires prior to initiating ureteral rest (DJS indwelling) and during ureteral rest (PCN tube in place without indwelling DJS).
Statistical analysis
Continuous variables, such as scores from the IPSS and PROMIS questionnaires, were compared using paired t-tests for each domain of the IPSS and PROMIS questionnaires to identify differences in LUTS and HRQOL before and after ureteral rest. Categorical variables, including UTI incidence, were compared using paired chi-squared tests. For all analyses, a p-value < 0.05 was considered statistically significant. Based on co-primary endpoints of IPSS and PROMIS scores, the study was powered at 80% with a Bonferroni-adjusted α of 0.025 per test, yielding a final target sample size of 32 participants.
Results
Among 153 patients undergoing unilateral ureteral reconstruction during the study period, 35 met the inclusion criteria. Most patients were excluded for not undergoing ureteral rest prior to reconstruction. Patient characteristics are presented in Table 1. The mean age was 61.2 years (SD 16.8), and the mean body mass index (BMI) was 28.5 kg/m2 (SD 6.7). The cohort was 57% female. Patients underwent ureteral reconstruction for a stricture at the ureteropelvic junction (42.9%), proximal ureter (11.4%), middle ureter (5.7%), distal ureter (31.4%), and multiple sites (8.6%; Table 1). All patients subsequently underwent robotic ureteral reconstruction.
Demographic and clinical characteristics of patients undergoing ureteral rest prior to robotic ureteral reconstruction.
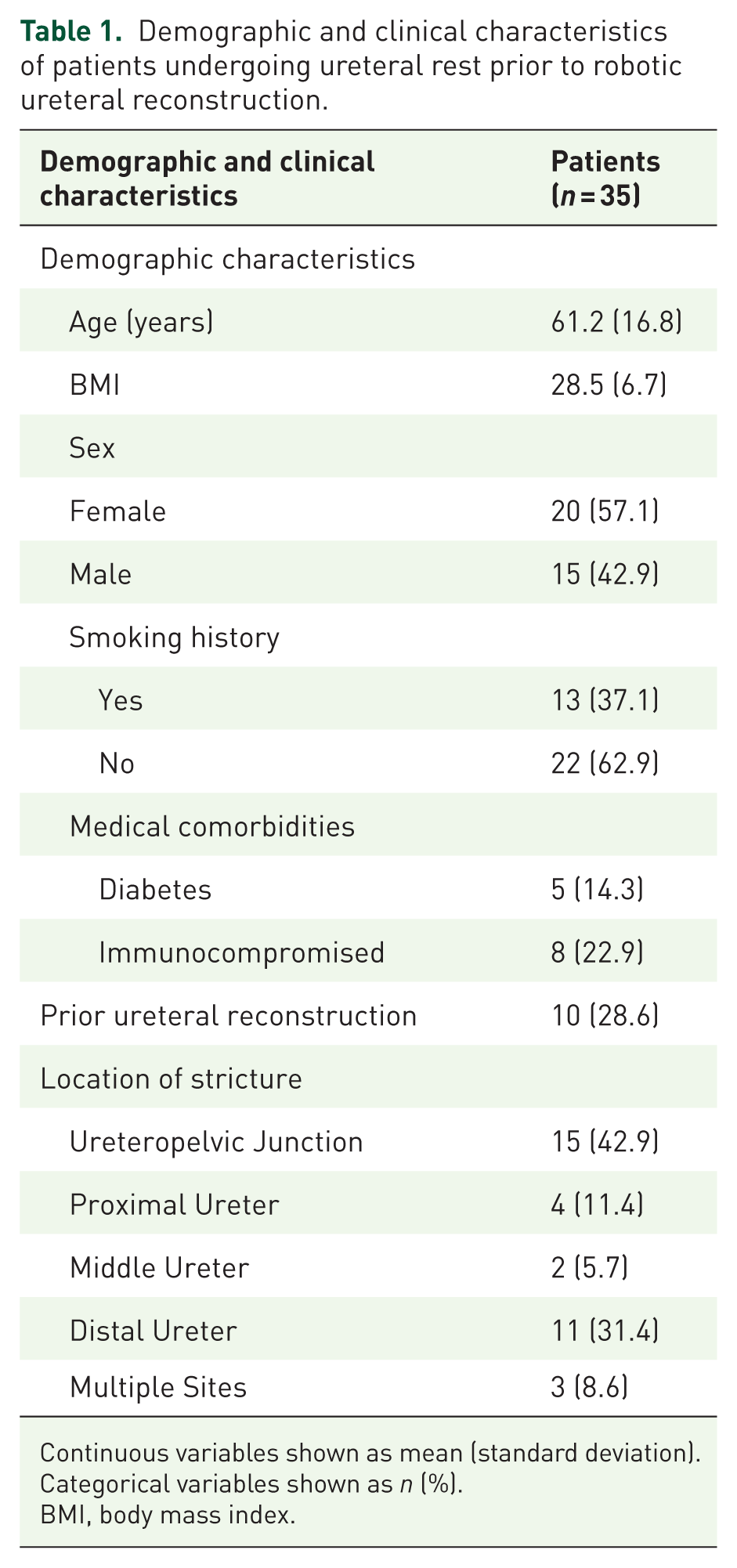
Continuous variables shown as mean (standard deviation). Categorical variables shown as n (%).
BMI, body mass index.
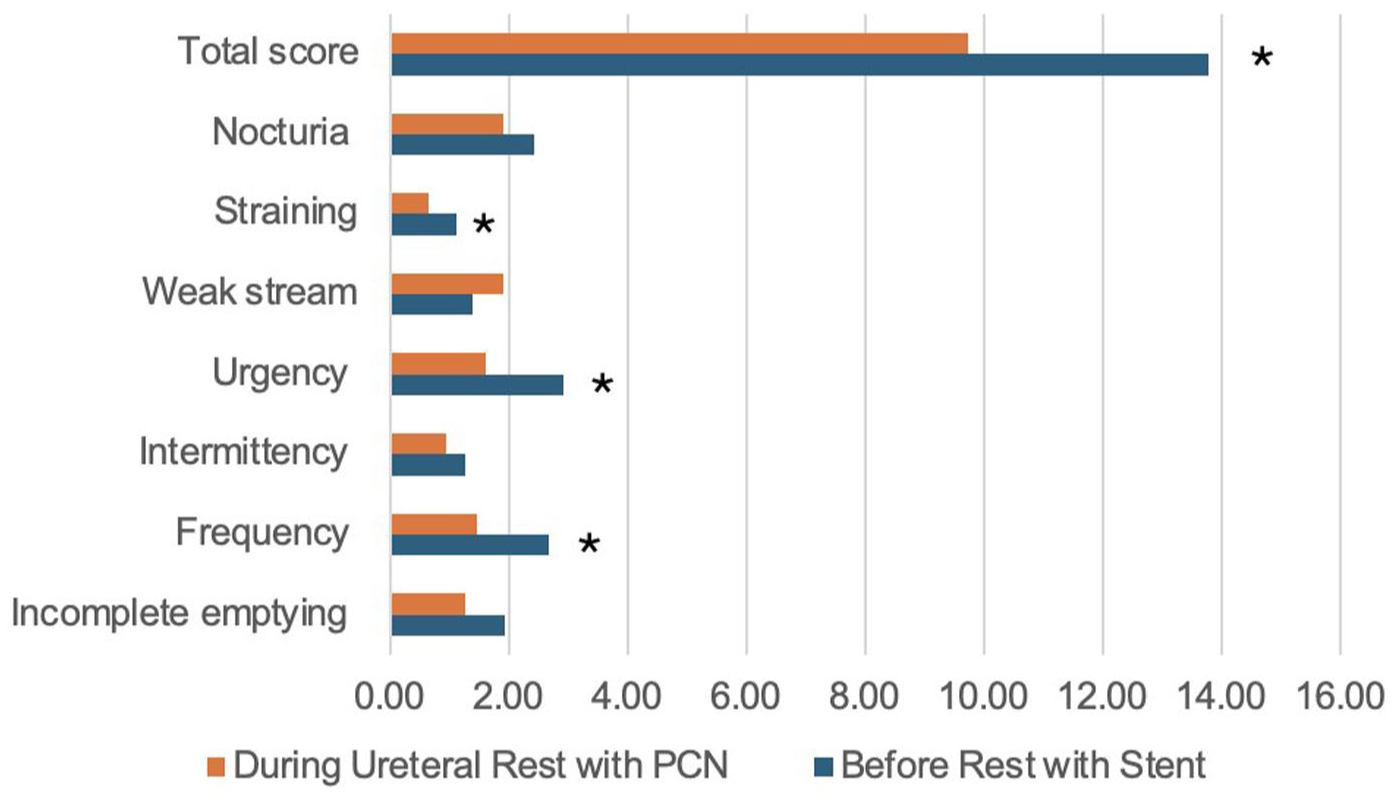
Results for LUTS assessment before and after ureteral rest are found in Table 2. For patients completing a course of ureteral rest (PCN tube without indwelling DJS), significant improvements in urinary frequency compared to the preceding DJS phase were reported, with the mean score decreasing from 2.7 to 1.5 (p = 0.001; Figure 1). Similarly, urgency and straining improved with mean scores decreasing from 2.9 to 1.6 (p = 0.0002) and 1.1 to 0.7 (p = 0.03). Furthermore, among patients undergoing ureteral rest, there were reductions in total IPSS symptom scores, which decreased from 13.8 to 9.7 (p = 0.003). However, ureteral rest demonstrated no significant differences in the rates of incomplete emptying (p = 0.052), intermittency (p = 0.24), weak stream (p = 0.09), nocturia (p = 0.08) or urinary symptom QOL (p = 0.20) when compared to DJS alone preceding ureteral rest.
Variation in IPSS before and after ureteral rest.

Each categories scores are out of a possible 5 points. Bold refers to p < 0.05.
IPSS, International Prostate Symptom Score; PCN, percutaneous nephrostomy, QOL, quality of life.
Variation in IPSS before and after ureteral rest.
Results for HRQOL assessment before and after ureteral rest are found in Table 3. For patients undergoing ureteral rest, improvements were seen in sleep disturbance, with mean scores decreasing from 10.7 to 9.3 (p = 0.04; Figure 2). No significant changes were observed before or during ureteral rest for physical activity (p = 0.11), anxiety (p = 0.14), depression (p = 0.37), fatigue (p = 0.74), social interference (p = 0.99), pain interference (p = 0.32), and pain intensity (p = 0.09).
Variation in PROMIS before and after ureteral rest.

Mean of each continuous variable. Each categories scores are out of a possible 20 points except pain Intensity scores were out of a possible 5 points. Bold refers to p < 0.05.
PCN, percutaneous nephrostomy; PROMIS, patient-reported outcomes measurement information system.

Variation in PROMIS before and after ureteral rest.
With regard to UTIs, no difference was observed in UTI incidence before and during ureteral rest, with 8 (23%) patients experiencing UTIs with DJS compared to 10 (29%) patients with a PCN tube (p = 0.48; Table 4).
Variation in UTIs before and after ureteral rest.

PCN, percutaneous nephrostomy; UTI, urinary tract infection.
Discussion
Ureteral rest involves removing hardware from the ureter to allow for stricture maturation. Although ureteral rest prior to ureteral reconstruction is based on an established reconstructive principle and has been shown to be associated with improved surgical success rates, patients may be hesitant to undergo nephrostomy tube placement. 6 Despite this, our study found statistically significant improvements in multiple key QOL parameters during ureteral rest compared to before ureteral rest.
We identified three principal findings regarding QOL outcomes among patients with USD who were initially managed with a DJS and then transitioned to ureteral rest with a PCN tube. First, patients undergoing ureteral rest experienced improvements in LUTS, specifically regarding straining, urinary frequency, urgency, and total IPSS. While these findings align with existing literature in the nephrolithiasis space regarding the impact of DJS on QOL, they represent a novel contribution in the context of USD, a condition that has been largely unexplored in this regard. 12 For instance, studies such as Harper et al. have documented the impact of DJS on LUTS and QOL in patients with nephrolithiasis, noting that urinary symptoms peak shortly after DJS insertion and remain elevated until removal. Similarly, Joshi et al. highlighted the prevalence of urinary symptoms, stent-related pain, sexual dysfunction, and reduced work capacity in nephrolithiasis patients.13,14 We believe that the improvement in LUTS is largely secondary to the absence of irritation of the bladder by the distal curl of the DJS. However, not all LUTS showed significant improvement with ureteral rest. For example, underlying detrusor underactivity, chronic bladder outlet obstruction, or long-standing inflammation may contribute to incomplete emptying and a weak stream rather than stent-induced irritation. Similarly, nocturia can be due to comorbid conditions, such as obstructive sleep apnea, rather than to stent irritation alone. Overall, our results underscore the broader implications of stent management strategies in patients with USD.
Second, ureteral rest was associated with improved sleep disturbances without worsening other HRQOL parameters. Our findings dovetail with HRQOL studies comparing PCN tubes and DJS in managing nephrolithiasis. Previous studies indicate that PCN offers a superior HRQOL compared to a DJS.7,15 Shoshany et al. found that patients with PCN tubes experienced significantly less discomfort and interference with daily activities. Similarly, Jiang et al. highlighted fewer hardware-related complications and better preservation of kidney function with PCN tubes.7,15 Our finding that HRQOL did not significantly worsen with a PCN compared with the discomfort caused by DJS may be influenced by psychological and physical factors. Leibovici et al. 16 found that 20% of patients with a DJS reported sleep disturbances, primarily due to nocturia. One reason for the difference in HRQOL could be that patients with PCN tubes may be more mentally prepared for the discomfort, recognizing it as a temporary and necessary intervention prior to definitive reconstruction, which could make it more tolerable. By contrast, 23% of patients with DJS reported anxiety and stress, which may heighten their perception of discomfort and contribute to sleep disturbances. 16 Stent-related pain at rest has also been reported in up to 7% of patients. 13 The internal nature of DJS may lead to underestimated bother, as patients might not fully anticipate the significant impact of stent-related symptoms. By contrast, the external visibility of a PCN tube might give patients a greater sense of control or adjustment. At the same time, the DJS’s internal placement, causing frequent urinary symptoms such as urgency, dysuria, and hematuria, can feel more intrusive and more challenging to manage.
Third, no difference in UTI incidence was observed before or during ureteral rest, a finding supported by the literature. 17 DJS are commonly associated with an increased risk of UTIs due to biofilm formation.18,19 Studies suggest that UTI rates in patients with DJS can range from 42% to 90%.18,20 By contrast, UTI rates in patients with PCN tubes have been shown to be approximately 20% within 90 days of placement. 21 This also aligns with findings by Al-Hajjaj et al., 22 who studied patients with obstructive uropathy due to nephrolithiasis and observed lower rates of fever and septicemia in the PCN tube group compared to the DJS group. These findings are noteworthy, as one may predict PCN tubes to carry a higher risk of UTI, given their external exposure. However, the risk of external exposure is balanced by a closed drainage system, minimizing the chance of bacterial contamination from the external environment. While these reported UTI risks differ from our studies, these differences are likely due to variations in study design, patient populations, underlying etiologies of obstruction, and differing definitions of infection. For instance, many prior studies focused on malignant or stone-related obstruction rather than benign ureteral strictures, and some defined infection based solely on culture results without correlating with clinical symptoms. Overall, our findings provide valuable insights into the benefits of this preoperative protocol for symptom relief and QOL while also equipping clinicians with evidence to better communicate the risks and benefits of ureteral rest, thereby addressing any stigma associated with lesser QOL when using PCN tubes instead of DJS.
The strengths of this study include the methodological design that employs a self-controlled model, minimizes confounding variables, and enhances the validity of the causal relationship between ureteral rest and observed improvements in LUTS and HRQOL. This approach ensures a real-world case-controlled evaluation of the intervention’s impact. Notably, the findings demonstrate significant enhancements across a broad spectrum of QOL metrics, highlighting the comprehensive benefits of ureteral rest on patient wellness. It contributes to the literature by being the first study to specifically address the effects of ureteral rest on LUTS and HRQOL prior to ureteral reconstruction, expanding upon prior studies that focused on surgical advantages and comparisons between PCN and DJS.
Our study is not without limitations. First, the sample size is relatively small. However, as the majority of our patients are referred from outside centers, our referring doctors generally place PCN and remove the DJS prior to evaluation at our center. We also excluded patients who underwent ureteral rest with no hardware and not a PCN tube as part of their ureteral rest. Nevertheless, we were still able to identify significant differences in LUTS and HRQOL metrics, suggesting a clinically meaningful impact despite the modest sample size. We included a wide range of patients with different etiologies and surgical management for USD in our cohort. However, we controlled for this variability by comparing outcomes before and after rest within the same patient. Third, the optimal duration of ureteral rest is not well established. We chose 6 weeks based on our clinical judgment, but there is limited evidence to guide this decision. Future research could explore the optimal duration for ureteral rest.
Conclusion
Initiating ureteral rest by exchanging an existing DJS for a PCN was associated with significant improvements in LUTS and sleep quality without worsening other health-related parameters in comparison to indwelling ureteral hardware. In addition, implementing ureteral rest did not increase the risk of UTI. These data may be used to counsel patients, especially those who may be concerned about exchanging their internal DJS for an external PCN.
Supplemental Material
sj-docx-1-tau-10.1177_17562872261436896 – Supplemental material for Assessment of lower urinary tract symptoms and health-related quality of life in patients undergoing ureteral rest prior to ureteral reconstruction
Supplemental material, sj-docx-1-tau-10.1177_17562872261436896 for Assessment of lower urinary tract symptoms and health-related quality of life in patients undergoing ureteral rest prior to ureteral reconstruction by Jonathan Rosenfeld, Aurash Naser-Tavakolian, Devin Boehm, Rebecca Arteaga, Aidan Raikar, Jaewoo Kim, Emily Ji and Ziho Lee in Therapeutic Advances in Urology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.