
Abstract
Endourological techniques are used more often nowadays in the treatment of ureteric strictures of various etiologies. Advances in technology have provided new tools to the armamentarium of the endoscopic urological surgeon. Numerous studies exist that investigate the efficiency and safety of each of the therapeutic modalities available. In this review, we attempt to demonstrate the available and contemporary evidence supporting each minimally invasive modality in the management of ureteric strictures.
Introduction
Ureteric strictures, either benign or malignant, represent a therapeutic challenge [Ganatra and Loughling, 2006; Yossepowitch et al. 2001; Docimo and DeWolf, 1989]. Before the stent era, management largely relied on open reconstructive techniques, often troublesome because of the distorted anatomy and lack of expertise [Nassar and Alsafa, 2011]. Nowadays, endourological treatment of ureteric strictures has become the preferred initial option, reducing the need for hospital stay and considerably improving quality of life. There is considerable advancement in the field, with avid research and development of innovative stent technologies [Al-Aown et al. 2010]. To date, there is an abundance of literature and reviews with regard to the appropriate choice for primary treatment. More surgeons nowadays consider endourological interventions as initial management of ureteric strictures because of less invasiveness and operative time, minimizing postoperative pain and rapid recovery [Chung et al. 2004]. Various techniques are available, e.g. conventional and metal stents, percutaneous nephrostomy (PCN), balloon dilatation (retrograde or antegrade), ureteroscopic endoureterotomy, cautery wire balloon incision and combined ante-/retrograde approach (rendezvous procedure). In this review, we attempt to demonstrate the available and contemporary evidence supporting each minimally invasive modality in the management of ureteric strictures.
Ureteric stricture by etiology
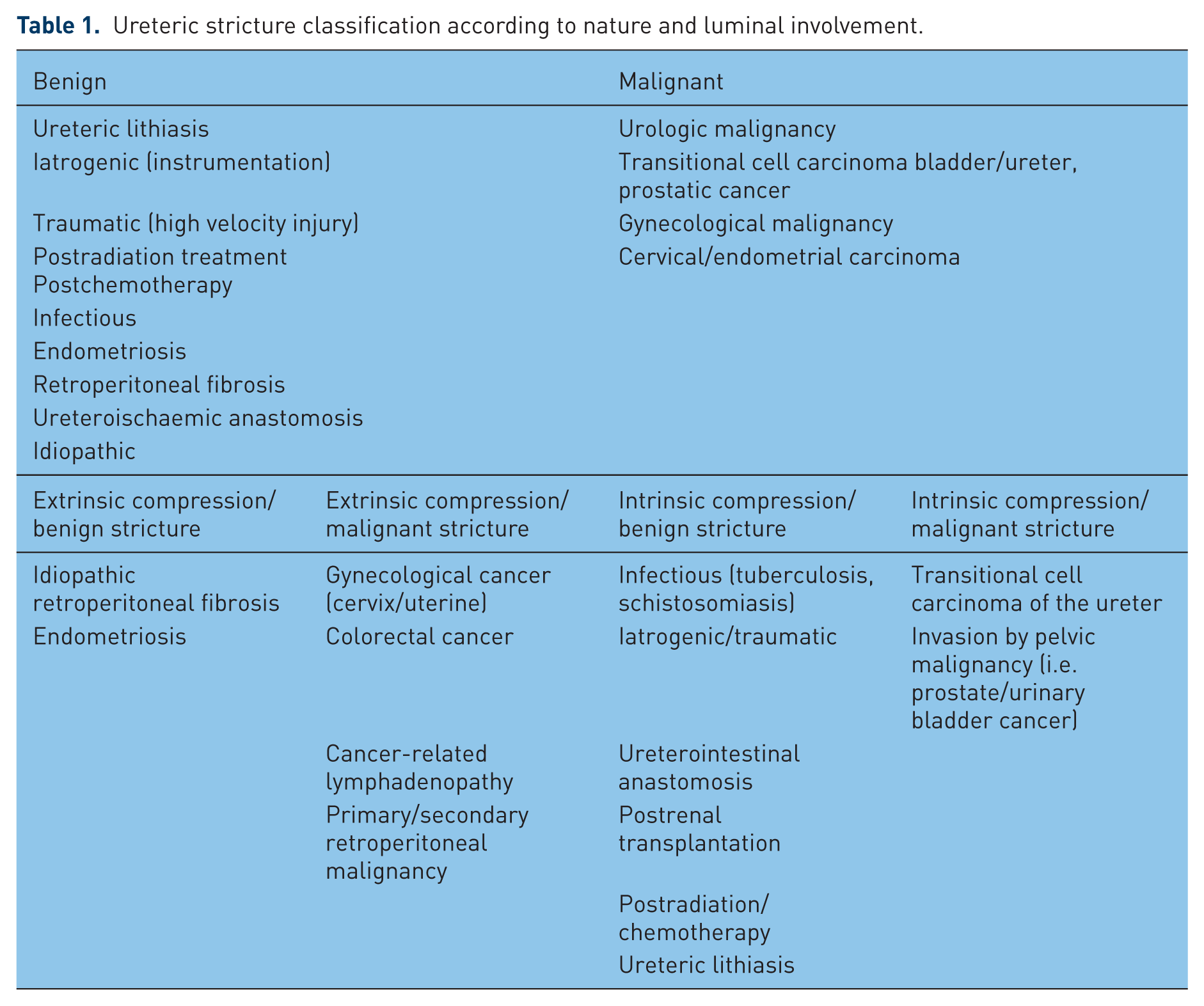
The classification of ureteric strictures may vary and be subject to location, length and inciting factor. We have developed a novel system of characterizing a stricture by distinguishing between primary and secondary elements that govern management. As such, the nature of the stricture (benign versus malignant) and the involvement of the ureteric lumen (extrinsic versus intrinsic) are considered the primary elements (Table 1). Stricture location, length, side, degree of ischaemia dependent on inciting factor and previous failed treatment constitute secondary elements that play a role in further management and are individualized. Common causes of ureteric strictures include pelvic and retroperitoneal malignancy, ureteral lithiasis, postradiation treatment, iatrogenic, traumatic, periureteric fibrosis due to abdominal aortic aneurysm, endometriosis or retroperitoneal fibrosis, tuberculous or other infectious ureteritis and also idiopathic. The obstruction may be a result of extrinsic compression or infiltration, most commonly due to malignancy. Stenosis may be also intrinsic, especially following instrumentation, lithiasis and radiation treatment. Strictures developing in ureteroenteric anastomosis and ureters of renal transplants merit special consideration, primarily as a result of the technical difficulties that are frequently encountered in the endourological management of such patients.
Ureteric stricture classification according to nature and luminal involvement.
Double J stent or PCN?
The development and subsequent widespread use of the double J stent since 1978 has revolutionized the treatment of obstructive uropathy due to ureteric stricture, whether of benign or malignant cause. The question for the choice between retrograde stenting and PCN as initial management still remains to this day. Modifications in design and evolution of biomaterials have improved efficacy and durability, as well as minimizing patient discomfort. Ureteric stents are inserted when there is need for temporary or permanent decompression of the upper tract and preservation of renal function. This may be achieved by the retrograde or antegrade (percutaneous) route. Most commonly used materials include polytetrafluoroethylene (PTFE), metal mesh and full metal-bodied stents. Practices vary greatly, although evidence exists now that percutaneous drainage is to be preferred upon impending sepsis, whereas retrograde stenting of the upper tracts may be chosen for uncomplicated cases and in coagulopathy [Lynch et al. 2008].
Several technical difficulties and specific patient characteristics pertaining to quality-of-life issues may influence the decision of primary management. For example, inability to identify the ureteral orifices or severe cardiopulmonary compromise may significantly compromise the outcome of either method. The availability of an experienced interventional radiology team is another factor when planning for future antegrade stenting postnephrostomy placement. Complication rate, albeit small, is an additional issue, especially for the elderly or frail patient. However, perhaps the most crucial question to be answered is the real-life, contemporary benefit and long-term outcome of drainage for the given patient. Recent advances in guidewire and stent design and biocompatibility as well as in stenting technique have led to a significant improvement in results. The success rate of retrograde stenting of 75% to 88% has been reported in various studies for both extrinsic [Radecka et al. 2006; Chapman and Reid, 1991; Rosenberg et al. 2005], and intrinsic [Wenzler et al. 2008; Tal et al. 2007] obstruction. However, extrinsic malignant ureteral obstruction managed by double J stents has been associated with a high failure rate and significant morbidity in long-term follow up. One of the reasons for the failure is that the lumen occludes early by urinary debris or crystals and compression of the tumour prevents peri-stent drainage. Double J stents rely mainly on flow around the stent for drainage and to a lesser extent to intraluminal flow [Chung et al. 2004; Ganatra and Loughling, 2006]. Hyperplastic reaction, tumour ingrowth, encrustation and migration are principal causes that compromise patency and make additional intervention necessary. Mild urothelial hyperplasia around the proximal stent edge is common and does not compromise ureteral patency significantly. Tumour ingrowth, on the other hand, is associated with obstruction and renal insufficiency [Kouba et al. 2008]. The difference in success rates may be related to the type of pelvic malignancy. Obstruction by bladder, prostatic or cervical malignancy managed in retrograde fashion presented with a success rate of only 15–21% compared with colorectal and breast cancer [Ganatra and Loughling, 2006]. Irritative urinary symptoms seem to be the most bothersome feature affecting quality of life in patients with indwelling DJ stents. Febrile urinary tract infection, most commonly pyelonephritis, has been reported in up to 10% of patients following double J stent insertion [Ku et al. 2004]. It has also been shown that stent length is an important factor for urinary symptoms, especially if the coil crosses at the midline. The same is true of placement of the proximal coil with adverse symptoms associated with placement outside the renal pelvis [El-Nahas et al. 2006]. A summary of the principal studies on initial retrograde stenting for ureteric stricture according to site and initiating cause is depicted on Table 2. Decompression by PCN is a recognized method of improving renal function [Pappas et al. 2000; Carrafiello et al. 2007]. However, the impact on the already compromised quality of life of these patients is significant, as reported in recent studies [Aravantinos et al. 2007; Joshi et al. 2001]. Despite excellent drainage and no necessity for general anaesthetic, a urine collection bag is required and complications such as bleeding, dislodgement, urosepsis, and bowel and pleural injury can all be encountered when inserting a nephrostomy. In a recent report, up to one in five patients experienced pyelonephritis following PCN placement [Bahu et al. 2013]. Furthermore, nephrostomy-tube placement has not been shown to prolong significantly survival in patients with advanced cancer. One study demonstrated that only 11 out of 17 patients with a PCN had acceptable quality of life for 2 months or more [Emmert et al. 1997]. Other problems that can contribute to poor quality of life after PCN placement are urinary leakage and skin excoriation at the nephrostomy exit site [Schmidbauer et al. 2006].
The most important studies for initial management of ureteric strictures with endoluminal stents by etiology.

In an attempt to obtain the most of both methods, a staged approach may be desirable, in which a nephrostomy tube is initially placed using sedation and local anaesthesia, and 1–2 weeks after allowing the tract to mature, an antegrade ureteral stent is passed from kidney to bladder. In that way, patients may be spared the complications of acute renal failure and/or haemodialysis and may also be relieved of intractable flank pain due to the obstruction. In one such series, 59 out of 60 patients were able to overcome ureteral obstruction with 57 out of 60 successful after the first attempt at antegrade stenting [Chitale et al. 2002]. An extra-anatomic bypass was another concept described to improve quality of life, achieved by tunnelling a regular nephrostomy tube subcutaneously and connecting it to a suprapubic catheter [Hannapel et al. 1986]. Later, Nakada and colleagues reported urinary diversion with the insertion of a nephrovesical subcutaneous stent in two patients under general anaesthesia [Nakada et al. 1995]. The original report for extra-anatomical PTFE stent was by Jabbour et al. (Jabbour et al., 2001). A coaxial composite subcutaneous PTFE stent was developed by Desgrandchamps and colleagues and inserted between the renal pelvis and the bladder, producing good long-term results [Desgrandchamps et al. 2007]. However, the best studied extra-anatomic stent is the Detour (Mentor-Porges, Crawley, UK). This subcutaneous ureteral prosthesis has been assessed by validated questionnaires (European Organization for the Research and Treatment of Cancer, QLC-30) and was found favourable for patients with advanced malignancies up to 18 months after placement of the prosthesis. The results were largely attributed to the removal of the nephrostomy tube and the absence of complications related to the Detour [Schmidbauer et al. 2006; Desgrandchamps et al. 2007].
Metal stents
Nitinol alloy is the latest metallic material used in ureteral stents and has enjoyed considerable success owing to its inherent shape memory and elasticity, establishing the development of full metal stents as the next step in stent design. The most widely studied and used representatives include the Resonance stent, the Memokath stent, the Allium stent and the recently introduced Uventa stent.
The Resonance stent (Cook Ireland, Limerick, Ireland) is made of a nickel-cobalt-chromium-molybdenum alloy without a lumen. Urine flows through a spiral groove fashioned along the entire length of the stent. It is 6 Fr calibre and is used mainly for extrinsic compression with a recommended indwelling time of 12 months. Liatsikos and colleagues have achieved 100% stricture patency rate in extraluminal malignant obstruction and only 44% in benign strictures in a total of 50 patients. Amongst complications, encrustation was found in 22% at the time of exchange. Obstruction, migration and stent-related symptoms were also reported. Mean follow up of the study was 8.5 months [Liatsikos et al. 2010]. In a recent retrospective series of 19 patients by Wang and colleagues stricture patency rate was 77.3% for a mean follow up of 5 months. Previous radiation therapy was identified as a risk factor in stent failure for malignant ureteral obstruction [Wang et al. 2011].
The Memokath 051 stent (Engineers & Doctors A/S, Copenhagen, Denmark) is a thermo-expandable shape memory stent made of nitinol with a lumen. It is introduced as a rigid cylinder that requires the injection of sterile water at a temperature of 60° C in order to expand into the desirable position; it needs the injection of cold water at 5° C in order to uncoil and be removed. It is recommended for long-term use in both intrinsic and extrinsic obstruction. Its segmental structure avoids lower urinary tract symptoms and reflux. It was first described in a series with early follow up that showed no patient rehospitalization for stent-related sepsis, pain or haematuria [Kulkarni and Bellamy, 1999, 2000]. The 11-year follow-up data on 74 patients showed an overall stent migration rate of 18% and 19% reinsertion rate at a mean time of 7.1 months, of which only 3 months were for stricture progression. Of the 28 patients with a malignant obstructive etiology, 89% (25/28) had postprocedural imaging showing normal or improved functional drainage [Agrawal et al. 2009]. In a recent study, results were reported for 37 patients (mean age 64 years) suffering from malignant ureteric strictures. The mean follow up was 22 months (range 5–60 months). Stent migration was reported in 13.5% (5/37), urinary tract infections in 8% (3/37) and blockage of stent due to progressive transitional cell carcinoma of the ureter in 5.4% (2/37) cases [Zaman et al. 2011]. The Memokath 051 stent has been found to be safe and efficient [Papatsoris and Buchholz, 2010], and also produce fewer stent-related symptoms compared with double J stents when evaluated with a validated questionnaire [Maan et al. 2010]. The latest advance in design consists of a dual-expansion stent, specifically designed to bridge the ureter for the treatment of complex ureteric and pelviureteric junction strictures [Masood et al. 2010].
The Allium stent (Allium Ltd, Caesarea, Israel) is the best studied representative of the group. It is a nickel-titanium alloy mesh invested with a biocompatible polymer to prevent tissue ingrowth and encrustation. Patency rates are high (> 95%), albeit follow up in recent series do not exceed 24 months. Stent placement requires initial ureteric balloon dilatation and it is difficult to adjust once in situ [Moskovitz et al. 2012]. In addition, the design allows for use only in distal (the vesico-ureteric junction) or proximal (pelviureteric) strictures. A full-length Allium stent is currently in production and clinical trials are awaited.
The Uventa stent (TaeWoong Medical Co., Ltd, Gveonggi-do, Korea) incorporates a layer of PTFE between two superelastic nitinol layers (triple layer) in a new expandable mesh capable of treating the entire length of the ureter. Preliminary results are promising; with patency rates of 100% and minimal complications at mean 7 months follow up [Kim et al. 2012].
Balloon dilatation and cautery wire balloon incision
Balloon dilatation of ureteric strictures, either retrograde or antegrade, was integrated in the urological armamentarium following the introduction of angiographic and vascular balloons into urological practice, allowing this technique to become an alternative mode of treatment. Researchers have reported mixed results with this method, ranging between 18% and 83%. This is largely due to the fact that most of the earlier series did not account for confounding variables such as cause of stricture, length, location, etc., when reporting the results. Banner and colleagues provided the original description in 1983 of the technique in 27 ureteric strictures with a 48% success rate [Banner et al. 1983]. In a study of 31 patients with ureteric strictures, O’Brien and colleagues achieved favourable results in 50% of the 24 patients treated (mean follow up 13 months) [O’Brien et al. 1988]. Ravery and colleagues presented their results of 25 ureteric strictures in 20 patients who were consecutively treated with high-pressure balloon dilatation. With a mean follow up of 16 months, the long-term success rate was 52%. Stricture etiology included ureteroenteric, postradiation and infectious parameters [Ravery et al. 1998]. Richter and colleagues concluded that balloon dilatation is appropriate for short, benign ureteric strictures with an intact vascular supply [Richter et al. 2000]. In a subsequent study, Byun and colleagues supported the finding that short (< 2 cm), benign strictures responded favourably to simple balloon dilatation (12/14) [Byun et al. 2003]. Those stricture characteristics are perhaps the reason for the extensive use of balloon dilatation in the treatment of strictures after renal transplantation; several series have reported the safety and efficacy of balloon dilatation of early (< 3 months) ureterovesical strictures in renal transplant patients, with success rates of 40–70% [Fontaine et al. 1997; Kim et al. 1993; Collado et al. 1998; Faenza et al. 1999; Streem et al. 1988]. Kristo and colleagues reported ureteral patency and graft-function rates at 100% after a median follow up of 24 months following balloon dilatation with or without laser endoureterotomy [Kristo et al. 2003]. The consensus from these studies seems to favour balloon dilatation with temporary stenting for ureteric strictures after transplantation as an initial first step, reserving open surgical correction for failures.
Patients with iatrogenic strictures such as following ureteroscopic instrumentation or inadvertent injury during pelvic surgery were also the subject of scrutiny after balloon dilatation, with early reports of success rates up to 85% [Goldfischer and Gerber, 1997; Preminger et al. 1997; Cohen et al. 1996]. However, later attempts were not as successful. Koukouras and colleagues reported technical success in 18 out of 25 (72%) patients with ureteric injury after pelvic surgery, with patency in only six at 1 week postprocedure [Koukouras et al. 2010]. High failure rates have also been reported with malignant extrinsic ureteric obstruction [Docimo and DeWolf, 1989]. Lang and colleagues reported a 7% success rate over a 2-year period with balloon dilatation of malignant ureteric obstruction [Lang et al. 1994].
Balloon dilatation with or without endoscopic incision has been studied extensively in children and young adults with primary obstructive megaureter (POM). Traditional treatment involves open surgery with ureteral reimplantation. Early studies reported patency in five out of seven patients aged 1–3 years at a mean follow up of 31 months (range 12–56 months) [Angerri et al. 2007]. Torino and colleagues reported the first experience of high-pressure balloon dilatation for POM of five patients in the first year of life (range 6–12 months) with relief of the obstruction demonstrated during a short follow up in all patients [Torino et al. 2012]. In a larger series, Christman and colleagues performed endoscopic incision and balloon dilatation with double stenting on 17 patients aged 3–12 years (mean age 7 years). Symptomatic improvement was reported for all patients followed up for 2 years postoperatively, while 12 patients presented with marked improvement of hydronephrosis on imaging. The authors favour the method for strictures shorter than 3 cm albeit with double stenting, and recommend follow up into adolescence [Christman et al. 2012]. Balloon dilatation has also been used for distal ureteric strictures with similar success. Initial attempts by Aliabadi and colleagues reported patency in five out of six patients with long-standing ureterovesical or ureterosigmoid anastomosic strictures at mean follow up of 12 months (mean age 9 years ) [Aliabadi et al. 1990]. Rivas and colleagues reported symptomatic and functional improvement after high-pressure retrograde balloon dilatation and placement of ureteric stenting on two children postureteric reimplantation (mean age 4 years) at 12 months follow up [Rivas et al. 2007]. Anastasescu and colleagues have performed antegrade dilatation of ureterovesical strictures in seven children, mean age 5 years, with successful outcome in four patients at 5-year follow up. Failures were attributed to the severity of the stenosis and ultimately required open surgical correction [Anastasescu et al. 2011].
Acucise balloon incision (Applied Medical Technologies, Laguna Hills, CA, USA) was regarded as a radical innovation in the treatment of ureteric strictures. Knowles and colleagues reported a 90% patency rate in 10 patients with benign distal strictures using cautery wire balloon incision at 36 months of follow up, three patients required a combined approach [Knowles et al. 2001]. Bhayani and colleagues treated eight patients with transplant ureteric strictures with success in six patients at a mean follow up of 2 years [Bhayani et al. 2003].
Results were poor for ureteroenteric strictures. Lin and colleagues achieved a success rate of only 30% with mean follow up at 9 months after Acucise treatment before secondary intervention was necessary [Lin et al.1999]. Similarly, Tutti and colleagues reported a success rate of 83% for ureterovesical strictures but only 50% for ureteroileal strictures [ Touiti, et al. 2002].
Schwartz and colleagues also achieved satisfactory patency in five out of six patients (83%) with persistent ureteric transplant strictures using balloon cautery endoureterotomy. The response was durable for a mean of 27 months without any perioperative complications [Schwartz et al. 2001]. Cautery wire balloon incision has been applied to iatrogenic ureteric strictures as well. Seseke and colleagues performed the procedure in 18 patients with an overall success rate 61% at mean 21.5 months of follow up. The authors concluded that the time period from the primary operation to the appearance of the stricture (> 6 months), the length of the stricture (< 1.5 cm) and renal function (> 25% of the total function) constitute selection criteria for a successful outcome [Seseke et al. 2002]. Latest evidence appears promising for a newly developed device, the peripheral cutting balloon microsurgical dilatation device, which has received US Food and Drug Administration approval. At 1-year follow up, patency was achieved in all patients in the study [Boylu et al. 2010].
Endoureterotomy
Endoureterotomy, whether performed in retrograde or antegrade fashion, is another minimally invasive treatment option for the management of ureteric strictures strictures. Davis and colleagues were the first to describe the ability of an incised ureteric stricture to regenerate and re-epithelialize [Davis et al. 1948]. The success rates of endoureterotomy have been described as between 53% and 82% for benign ureteric strictures by use of electrocautery and/or cold-knife incision [Meretyk et al. 1992; Esghi and Lifson, 1995; Wolf et al. 1997]. The holmium laser is the latest tool and preferred modality for endourological procedures due to its ability to cut and coagulate tissue with satisfactory haemostasis and the availability of a flexible optical fibre delivery system. The procedure is performed under ureteroscopic control and frequently combined with balloon dilatation. The incision is made from the ureteral lumen out to periureteral fat in a full-thickness fashion and should encompass 2–3 mm of normal ureteral tissue. Stricture characteristics influence the success rates of endoureterotomy as much as any minimally invasive technique. Length of stricture and degree of ischaemia are the most important prognostic factors for success. Gnessin and colleagues retrospectively reviewed 69 patients who underwent retrograde laser endoureterotomy for a benign ureteric stricture. At a median follow of 27 months, 82% of patients were symptom free and 78.7% were free of radiographic evidence of obstruction. The success rate was higher for nonischaemic strictures and lengths of 1 cm or less [Gnessin et al. 2009]. At 3 years follow up, Lane and colleagues reported success in 68.4% (13/19) of patients with iatrogenic strictures. Failure was identified within the first 3 months of treatment for all patients. A longer stricture length (> 2 cm) correlated with treatment failure [Lane et al. 2006]. In another study with similar follow up (3.5 years), Razdan and colleagues identified stricture length (> 2 cm) as the most important predictor of success, while the site of the stricture did not seem to affect outcome [Razdan et al. 2005]. However, earlier series reported the superiority of endoureterotomy performed for benign strictures in the mid-ureter compared with the success for distal strictures [Yamada et al. 1995; Wolf et al. 1997].
In their study involving reimplanted ureters, Gdor and colleagues reported overall success rate in six out of eight strictures (75%) of up to 1 cm at 52 months mean follow up, five of which were treated with laser endoureterotomy and were all successful [Gdor et al. 2008]. Mano and colleagues had a success rate of 83% in nine ureterovesical anastomotic strictures of less than 1 cm treated with retrograde laser endoureterotomy; mean follow up was 44.4 months [Mano et al. 2012]. He and colleagues have retrospectively reviewed endoureterotomy in eight patients with ureterovesical strictures and achieved 62.5% patency at 16 months follow up. It appears that endoureterotomy has a place in the initial treatment of transplant anastomotic strictures of 1 cm or less in experienced hands [He et al. 2008].
Radiation-induced and malignant strictures generally respond poorly to endoureterotomy. This is largely due to the ischaemic nature of the lesion, as well as the segmental distribution that is frequently encountered, especially in advanced malignancy. The distal ureter is mostly affected. A combined antegrade and retrograde approach is often required for these patients (rendezvous procedure).
The obliterated ureter
A completely obliterated ureteric segment is particularly challenging to treat and reports in the literature are few. Endoscopic ureteroureterostomy aims to establish patency by recanalization. This is achieved by successful guidewire placement in proper alignment between normal segments. Subsequent channel incision and balloon dilatation with long-term stenting aim to provide optimal conditions for epithelization and mucosal regeneration. This method has been used for strictures less than 2 cm. Early series have produced promising results. Bagley and colleagues in their initial experience with two patients established patency by use of a combined retrograde and antegrade approach [Bagley et al. 1985]. Muench and colleagues met with similar success in restoring patency of ureteroileal anastomosis in three patients [Muench et al. 1987]. Strup and Bagley tested the procedure in seven patients with both benign and malignant stricture etiology. Continuity was restored in six out of seven patients, the failure being due to recurrent upper tract transitional cell carcinoma [Strup and Bagley, 1996]. Lingeman and colleagues reported a successful outcome in nine patients with total occlusion at a mean follow up of 22 months. They used the ‘cut-to-the-light’ technique in six patients and a facial-incising needle in five [Lingeman et al. 1995]. Watson and colleagues described their version of the rendezvous procedure to cross complicated ureteric strictures. The procedure involves serial dilatation or use of balloon catheter over a previously advanced guidewire for near-total ureteric obliteration. Results from interventional radiology series also support the effectiveness of the technique [Watson et al. 2002]. Macri and colleagues performed the procedure successfully in 16 patients with obliterated ureteric segments of benign cause without complications. The authors admit that the combined approach improved the stenting success rate from 78.6% to 88.09%. Of note, the procedure was the first-line approach in 12 cases (75%) and second-line approach in four cases (25%) [Macri et al. 2005]. Overall, the available evidence indicates that endoscopic ureteroureterostomy is safe and efficient as the first choice for the management of totally obliterated ureteric anastomoses less than 2 cm long.
Conclusion
Minimally invasive endourological techniques in managing ureteric strictures provide a viable alternative to open surgery for repair and recanalization, either as primary, secondary or palliative procedures. Stricture etiology and inherent characteristics, especially length and vascularity, have a pivotal role in the choice and prospective success of the available treatment modalities. Ureteric stents and percutaneous drainage are commonly used as an interim procedure until a definite treatment is decided, or may serve as such in selected cases. Endoureterotomy may be considered as the procedure of choice for intrinsic benign strictures and in obliterated ureteral segments. Malignant and postradiotherapy strictures respond poorly in long-term follow up and are possibly best treated with long-term metallic stents. Special categories include transplant and ureteroenteric strictures, where a combination of balloon dilatation and endoureterotomy appears to produce satisfactory results. Further research into the histopathology of strictures and correlations to the various treatment options available may provide additional information to aid in choosing the optimal therapeutic strategy for the individual patient.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.