
Abstract
Background & Objectives:
Percutaneous nephrostomy (PN) for malignant ureteric obstruction (MUO) is increasingly accessible with high success rates. However, it is not without associated risks and morbidity, impacting quality of life, while not improving overall survival. In two UK hospitals, we investigated the outcomes of undergoing PN for MUO, to inform future patient counselling and selection for this intervention.
Methods:
A retrospective audit of electronic records identified patients that received PN for bladder, and prostate cancer (PCa) between January 2015 and December 2018. Hospital 1 had a 24-h nephrostomy service, while Hospital 2 had a limited service; Group A: recurrent or treatment-resistant PCa, Group B: primary PCa, Group C: Bladder cancer.
Results:
A total of 261 patients (Hospital 1 = 186, Hospital 2 = 75), had PN insertion. Seventy-eight had prostate or bladder cancer. Group A n = 30, Group B n = 12, Group C n = 36. Median age = 79 [interquartile range (IQR) = 72–86]. Following PN insertion, 12-month mortality was significantly greater in Hospital 1 at 82%, versus 52% in Hospital 2 (p = 0.015). Median survival: Group A: 177 days (IQR = 80–266), Group B: 209 days (IQR = 77–352), Group C: 145 days (IQR = 97–362). There was no significant difference in same-admission mortality, although group A had the greatest same-admission mortality at 17%. A total of 69% of all patients received bilateral nephrostomies. Patients with bilateral versus unilateral PN had no difference in mortality or nadir creatinine.
Conclusion:
Most patients with malignant obstruction secondary to prostate or bladder cancer lived less than 12 months after PN insertion. When offering PN, careful consideration of disease prognosis should be made, and frank discussion of the implications of a life-long nephrostomy with patients and relatives.
Keywords
Introduction
Malignant ureteric obstruction (MUO) is an indicator of poor prognosis in many cancers, of which the commonest primary cause is urological.1–3 These patients are often comorbid and at high risk for a general anaesthetic intervention. The anatomical distortion of the ureteric orifices may also render retrograde intervention attempts more difficult and less favourable. Percutaneous nephrostomies (PNs) offer a 96–98% success rate, so is often the intervention of choice, followed by immediate or delayed antegrade ureteric stenting.4–6 Its accessibility under local anaesthesia, has broadened the pool of patients now eligible for decompression. However, it is not without its complications and impact on quality of life, with less than 2% of patients in poor risk groups that underwent PN for MUO surviving beyond 6 months. 7 Many of these patients spend a significant proportion of the last months of their lives with PN complications, and repeated hospital visits. Of a study of 105 patients, 39% had at least one hospital readmission after discharge, within 30 days. 8 There are many considerations in identifying patients who are most likely to benefit from MUO decompression. Considering that many more patients in hospital have nephrostomy in situ than ever before, this may be due to the increasing accessibility of PN across the country.
We sought to examine the outcomes of patients with MUO across two UK hospitals, one with a twenty-four seven PN service and another with a more limited service to inform future practice on identifying patients that would most benefit from decompression.
Methods
All patients that underwent PN between January 2015 and December 2018 across two hospitals were identified retrospectively through the radiology coding systems searching for ‘nephrostomy’, ‘kidney’ and ‘decompression’. This study was a registered clinical audit, as an evaluation of our service, examining electronic patient records to identify patients suitable for the study.
The inclusion criteria were patients who had undergone PN insertion for ureteric obstruction within both radiology departments. We then excluded patients that did not have MUO secondary to bladder or prostate malignancy. All patients had radiologically confirmed hydronephrosis prior to PN insertion. PNs were performed under local anaesthesia by a consultant interventional radiologist or a radiology trainee under direct supervision. Hospital 1 has a twenty-four seven interventional radiology service, while Hospital 2, a limited interventional radiology service during normal working hours. Outside hours, patients may need to be discussed with a neighbouring hospital and transferred for PN insertion.
We documented patient demographics, primary disease, histological diagnosis, previous cancer treatments, plans for further treatments, number of further radiological procedures, progression to antegrade or retrograde stent insertion, renal function, length of stay and survival.
Primary outcomes recorded were mortality, from time of nephrostomy insertion to time of death, and related morbidity post-PN insertion. This included the length of hospital stay, number of subsequent interventions required or retrograde stenting attempts at a later stage. Secondary outcomes included post-PN renal function which were recorded at its nadir, within the successive 2 months.
Statistical methods
Patient demographics and clinical data were reported with descriptive statistics. Frequencies and percentages were used for categorical data, and median and interquartile range (IQR), or mean and standard deviations to express continuous variables.
All statistical analyses were performed using Stata 17.0 (StataCorp LLC, TX, USA). A p value of less than 0.05 was considered to indicate a statistically significant difference. Mortality and survival analyses were carried out with a combination of logistic regression tests, Kaplan Meier curves and logrank test, were indicated. A p value of less than 0.05 was considered to indicate a statistically significant difference.
Results
Between January 2015 and December 2018, 261patients were identified as having had a PN insertion for renal tract obstruction within the interventional radiology departments of Hospitals 1 and 2. A total of 186 patients had PN inserted in Hospital 1, and 75 patients in Hospital 2. A total of 78 patients met the inclusion criteria, of which there were 66 men and 12 women across both hospitals (Table 1).
Demographics by hospital.

The commonest indication for nephrostomy insertion was urinary tract obstruction secondary to bladder or prostate cancer at 30% (n = 78). After urological malignancy, obstructive stones accounted for PN in 26% (69), 10% (27) had gynaecological malignancies, 8% (22) colorectal malignancies, and 5% (12) other malignancies such as lymphoma, or metastasis from unknown primaries. 8% (21) of PN were inserted for non-malignant conditions such as ureteric strictures, aneurysms, or intraoperative ureteric injuries. A total of 9% (24) had PN for unknown reasons and eight patients were transferred in from neighbouring hospitals solely for nephrostomies before being repatriated, so details were unavailable.
Of the 78 patients with obstruction secondary to bladder or prostate malignancy, the median age was 79 (IQR = 72–86). These patients were divided into three groups (Table 2). Group A (n = 30) consisted of men with known prostate cancer which was recurrent or resistant to treatment. These men had local progression of prostate cancer to MUO despite either being on maximum androgen blockade (MAB), or with a history of radical prostatectomy, radiotherapy, or chemotherapy. Group B (n = 12) consisted of men with primary prostate cancer, either hormone naïve; diagnosed on presentation with obstructive uropathy, or men on single hormone therapy. Group C patients (n = 36) had malignant obstruction secondary to bladder cancer.
Demographics by group.

IQR, interquartile range.
Most patients in Group A, 9/30 men, had clinically diagnosed metastatic prostate cancer, 15/30 had either intermediate grade, or high-risk prostate cancer diagnosed histologically. Four men had historical low risk histology, and two men had no record of previous histology at the time of presentation with MUO. The treatment history varied with most men in Group A, (14/30) having received MAB at the time of presentation and 12/30 with a history of radical treatment for prostate cancer. Two men had received palliative radiotherapy, one man was on chemotherapy and another on the STAMPEDE clinical trial was receiving abiraterone and 3rd line hormone therapy. The median prostate-specific antigen (PSA) in Group A was 11 ng/mL (IQR = 1–69 ng/mL), and in Group B was 63 ng/mL (IQR = 13–106 ng/mL).
Within Group B, 8/12 men at the time of PN insertion had clinically diagnosed prostate cancer, while 3/12 had high grade prostate cancer, Gleason 8–10. Seven of the men in Group B were on single hormone therapy, while the other 5/12 patients were treatment naïve and diagnosed with prostate cancer on that admission.
Of the Group C patients, the majority 24/36 (67%) where known to have muscle invasive bladder cancer of which three had metastatic disease. Eight (22%) had T1 disease on historical histology and did not have repeat resections or biopsies following PN to confirm progression to muscle-invasive bladder cancer. The histology was unknown in four patients (11%).
The main treatment modality in Group C, was TURBT alone at 47% (Table 3). Eight patients (22%) had undergone radical cystectomy or radical radiotherapy, four patients (11%) received intravesical therapies, 2 (6%) palliative treatment and 2 (6%) received chemotherapy. There were two patients on presentation with newly diagnosed bladder cancer causing obstructive uropathy and had therefore had no prior treatment. Of the 36 patients in Group C, 6/36 (17%) were due to have further treatment for bladder cancer: three radical and three palliative treatments. Of the other 30 patients (83%), at the time of nephrostomy insertion there was no documented plan for further treatment. However, four patients within this group had clear documentation that they were unsuitable for further treatment, due to fitness.
Bladder cancer treatment modalities.
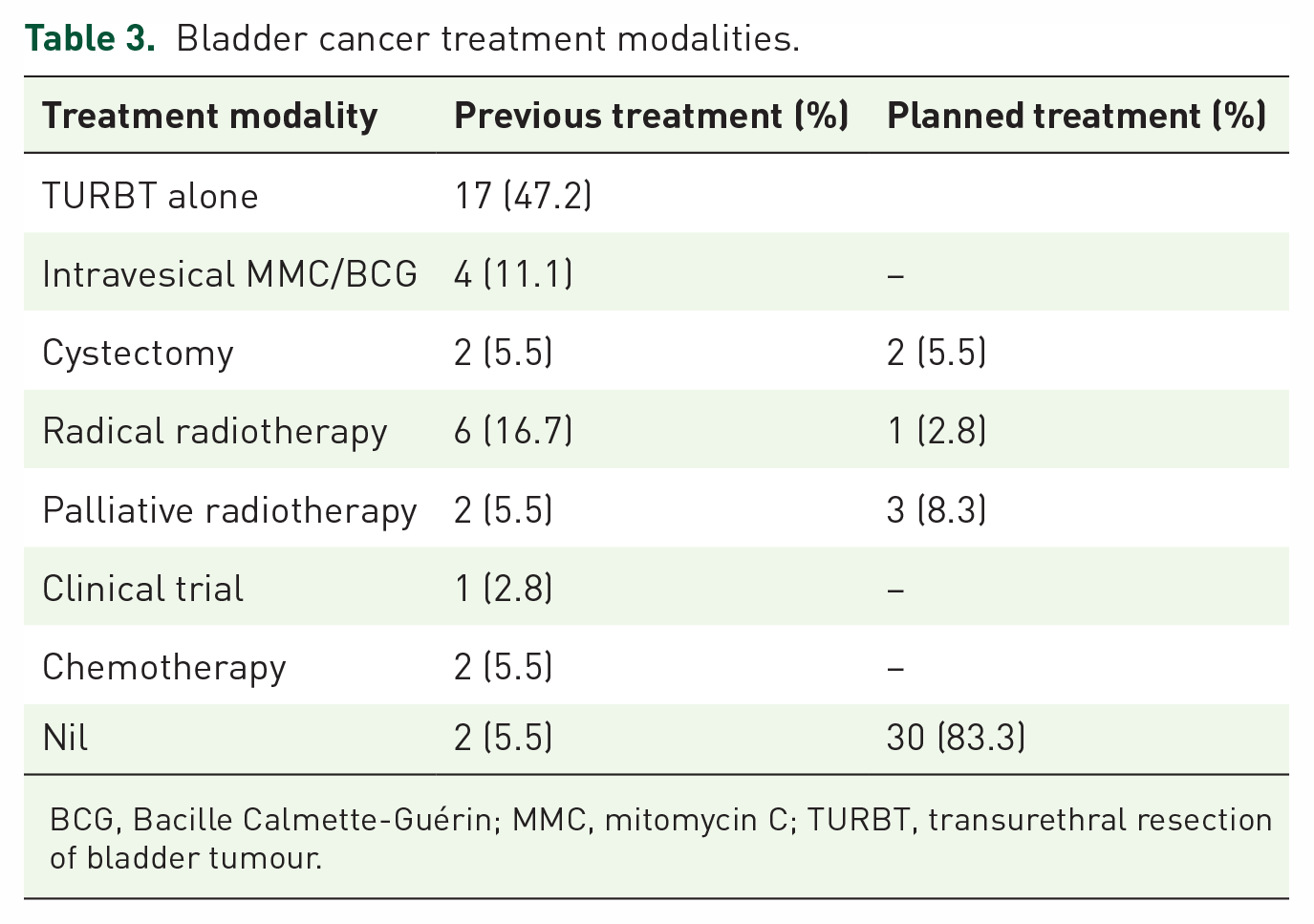
BCG, Bacille Calmette-Guérin; MMC, mitomycin C; TURBT, transurethral resection of bladder tumour.
Mortality by cancer groups
The same-admission mortality was greatest in the treatment resistant Group A, at 20%, and lowest in Group C at 6% (Table 4). The median survival across all three groups was 165 days (IQR 80–319), with a 28-day mortality of 14% (11/78), 6-month mortality at 55% (43/78) and 12-month mortality at 74% (58/78). By 12 months, the mortality across the three groups were similar at 77% in Group A, 75% in Group B, and 72% in Group C. There was no statistically significant difference in same-admission mortality between cancer groups (p = 0.09), 28-day (p = 0.76), 6-month (p = 0.493), or 12-month (p = 0.68) mortality.
Mortality by cancer groups.

IQR, interquartile range.
There was no significant difference in overall survival between cancer groups (p = 0.51) (Figure 1). Only one patient, in Group C was still alive at follow-up. He had undergone bilateral PN insertion and successful antegrade stenting, with two further retrograde stent changes.

Survival by cancer group.
Three patients within Group C had known metastatic bladder cancer at time of presentation. These patients died within 24–149 days of nephrostomy insertion. Of the patients within Group C, three were also found to have significantly raised PSA during admission at 265, 311, and 1893 ng/mL. They died within 124–259 days of nephrostomy insertion.
Mortality by hospital groups
There was a similar same hospital admission mortality in both groups at 12% and 10%, in Hospital 1 and Hospital 2 respectively. There was no statistically significant difference in same-admission mortality, 28-day or 6-month mortality between the two hospitals. However, 12-month mortality was significantly higher in Hospital 1 (p = 0.015), with an odds-ratio of 3.83 (95% CI = 1.30–11.32) than in Hospital 2. The 12-month mortality in Hospital 1 was 82% (47/57) and 52% (11/21) in Hospital 2 (Table 5).
Mortality by hospital.

IQR, interquartile range.
Survival
The median survival was 157 days (IQR 82–262) in Hospital 1, and 232 days (IQR 72–620) in Hospital 2. Overall survival was significantly higher in Hospital 2 (p = 0.011), with the mean predicted survival 196 days higher in Hospital 2 (95% CI 46.05–347.22). Using the log-rank test, survival between the curves were statistically significantly different (p = 0.0307) (Figure 2).
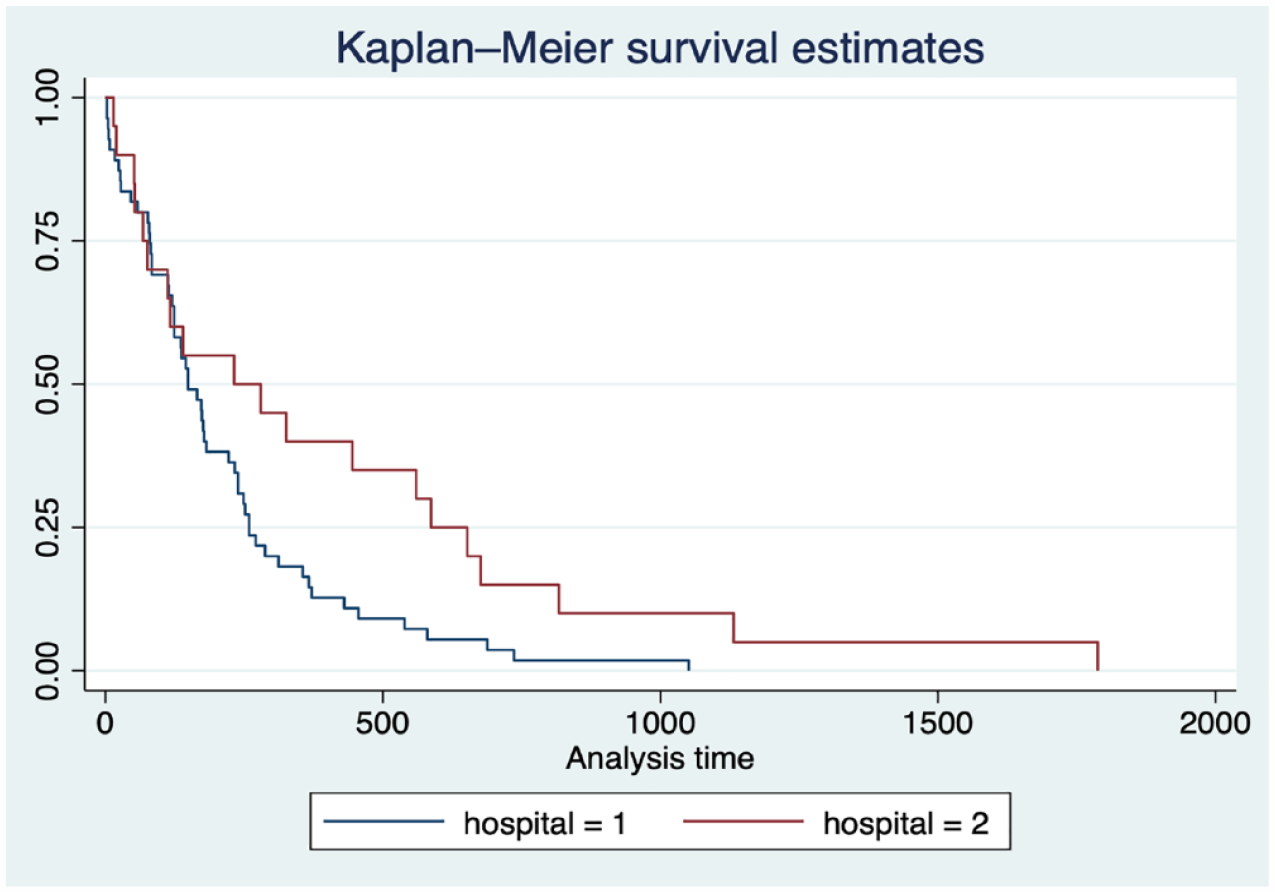
Survival by hospital.
Unilateral versus Bilateral PN
Bilateral PN were inserted in 69% (48/70) and the other 31% (22/70) had unilateral PN (Table 6). Unfortunately, eight patients had unclear documentation on whether they required unilateral or bilateral PN insertion.
Unilateral versus bilateral PN.
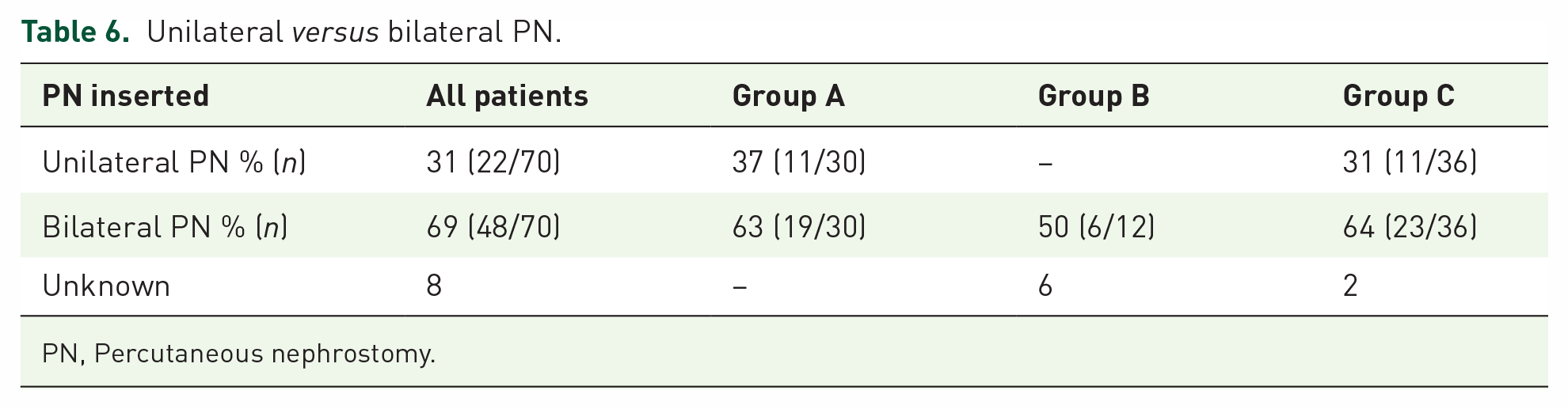
PN, Percutaneous nephrostomy.
The patients with bilateral PN insertion had a longer hospital stay with a median of 10 days (IQR 6–22) in comparison to the unilateral PN patients at 4 days (IQR 2–10) (Table 7). However, there was no apparent survival benefit of a bilateral PN insertion over unilateral PN with an identical 28-day mortality rate of 13%, 6/45 versus 3/23 respectively. A total of 12-month mortality was greater in the group that had bilateral nephrostomies at 84% (38/45) versus 61% (14/23) in the unilateral group.
Mortality in unilateral versus bilateral PN.

IQR, interquartile range; PN, percutaneous nephrostomy.
Renal function
A total of 68 of the 78 patients had an elevated creatinine >120 µmol/L prior to PN insertion; however, one patient with bladder cancer did not have any renal function tests prior to PN insertion. In that case, unilateral PN was inserted based on imaging. Furthermore, four patients, also with PN for bladder cancer had renal function tests within normal range pre-PN, with creatinine levels at 65, 95, 117 and 119 µmol/L. Post-PN creatinine for these patients were 76, 78, 125 and 132 µmol/L respectively at nadir.
Of the three cancer groups, Group C had the lowest mean improvement of creatinine at 160 µmol/L (IQR 28–348) (Table 8). Renal function pre- and post-PN were compared in patients that received unilateral PN, versus bilateral PN. All the patients that had bilateral PN showed improvement in creatinine and urea levels; however, of the unilateral PN group, three patients had worse creatinine levels, and five patients no improvement of urea levels. Of all the patients that had an overall improvement of renal function, there was a greater improvement in patients that received bilateral PN. The median reduction of creatinine was 326 µmol/L (IQR = 99–583 µmol/L) in the bilateral PN patients, and 51 µmol/L (range 22–227 µmol/L) in the unilateral group. The nadir creatinine of both groups however was similar with a median of 136 µmol/L (IQR = 102–190 µmol/L) in the bilateral group, and 142 µmol/L (IQR = 110–236 µmol/L) in the unilateral group.
Renal function and morbidity.

IQR, interquartile range.
Associated morbidity
The median number of days patients were admitted in hospital were similar in Groups A and C, at 9 days (IQR = 5–15) and 8 days (IQR = 3–17) respectively. It was shortest in Group B at 3 days (IQR = 2–11). The number of subsequent PN-related emergency presentations ranged between 0 and 9 across the groups. On average, most of the patients had 2–3 additional visits to the radiology department for re-siting, change of nephrostomy or antegrade stenting. Only 17 patients (22%), went on to have retrograde stenting procedures, while the other 61/78 patients (78%), remained with life-long nephrostomies. A particular patient in the bladder cancer group had 12 further interventional radiology procedures, and 7 nephrostomy-related emergency admissions within the remaining 18 months of his life.
Discussion
We chose to evaluate the nephrostomy services in two UK hospitals to assess patient outcomes, and whether the relative ease with which PN can be acquired may influence patient selection. We also sought to identify patient or disease factors that may aid identification of patients offered PN that would most benefit in the long-term, after the acute admission episode. In hormone-naïve prostate cancer, where there are available treatment options, the assumption was that this cohort may have a longer life expectancy and therefore more likely to benefit in the long-term from a PN. Whereas, in the group with recurrent or resistant prostate cancer, and advanced bladder cancer, we wanted to assess whether there was a significant gain in decompressing the kidneys, considering the associated morbidity with PN, and the prognosis associated with these patient groups. This study would allow us to potentially predict their outcome to guide future patient selection and aid counselling of patients that are offered PN.
We know from previous studies that there is a high success rate of PN insertion, with a relatively low complication rate of 1–3%. 4 This can often influence the decision to proceed with PN, particularly if readily available. We specifically looked at patients with PN to relieve obstruction from urological malignancies, as we urologists may not be consulted where obstruction occurs secondary to non-urological conditions, until after it’s insertion for future planning.
A systematic review of the use of PN in end stage prostate cancer patients showed a median survival post-PN insertion of 4–21 months in four studies, and in three other studies, a mean survival of 4.4, 15 and 31 months. 4 The overall median survival of our cohort was 165 days (5.4 months), (IQR 80–319). This led us to consider the indications for PN in malignant obstruction in these hospitals and assess the need to refine our patient selection. Of the three groups, Group A, with recurrent or resistant prostate cancer appears to have had a worse outcome in comparison to Group B and C, in terms of same-admission mortality at 20% (9/30). However, by 28 days, mortality was similar in Group A and B at 17% and 14% respectively, and by 12-months, all three groups had similar mortality at 77% in Group A, 75% in Group B and 72% in Group C.
A 2006 study by Harris et al. consisted of three groups: hormone naïve, hormone responsive and hormone resistant prostate cancer. Overall survival for these groups were 226.5 days, 114.3 days and 100.2 days respectively. 9 Romero et al. however found no survival difference between newly diagnosed, and previously diagnosed cancer. 10 Our study found that men with primary prostate cancer with single therapy, lived longer than men with resistant or recurrent prostate cancer with a median survival of 206 days (IQR = 77–352) in Group B, compared to 177 days (IQR = 80–266) in Group A.
Patients in Group C had the lowest median survival at 145 days (IQR = 97–362). This is not unexpected as three patients within this group had metastatic bladder cancer, and three others incidentally had a significantly raised PSA. These patients did not go on to have prostate biopsies, but two of them went on to have bone scans which did not find metastasis. Previous data has shown that in groups of patients that undergo PN insertion, those patients with bladder cancer did poorly in comparison to those with prostate cancer, even with castrate-resistant disease. 5 This was reflected in our study although, in comparison to Misra et al.’s smaller bladder cancer cohort with a mean survival of 58 days (range 4–128), 5 our bladder cancer group had better survival with a mean of 279 days (range 3–1788).
Hospital 1 has a twenty-four seven PN service, whereas Hospital 2 a limited service with PN largely available during normal working hours. Outside of these hours, patients at Hospital 2 requiring PN intervention are transferred out to a neighbouring hospital with an available PN service. These patients would generally require senior urology involvement in the assessment and decision-making on a patient’s suitability to be transferred out for the intervention. We found that patients from Hospital 2, had a greater median survival at 232 days (IQR = 72–620), compared to Hospital 1 with a median survival of 157 days (IQR = 82–262). Patients of Hospital 1 also had a statistically significantly greater 12-month mortality of 82% than Hospital 2 at 52%. A more limited PN service, and therefore senior urology input in the decision-making may result in more careful selection of patients offered the intervention. These patients may therefore have a better prognosis and therefore likely to benefit from PN in the long-term.
In the use of bilateral and unilateral PN, Nariculum et al.’s study of 25 patients demonstrated that nadir creatinine post-PN insertion was similar in both groups. 11 Malik et al. also found no statistical difference in creatinine improvement in patients with bilateral and unilateral PN insertion. Our study further supported this. Although there was a greater improvement of renal function returning closer to baseline in the patients that received bilateral PN, there was little difference in the nadir creatinine of both groups. The patients with bilateral PN also had a much longer median hospital stay compared with unilateral PN, at 10 days and 4 days respectively, and there was also no apparent survival benefit to it. Shekarriz et al. also reported that overall survival was dependant on the type of primary cancer. 12
Although the success rate of PN is high it is not without complications. A multi-factorial approach and case-by-case discussion are required in making the decision to proceed with a PN, particularly in an otherwise terminal patient. Patient factors such as age, comorbidities, prognosis, available treatments, social factors, and the possibility of the patient becoming permanently nephrostomy dependant. The complication rate has been reported as 1–3% and include pain/discomfort, infection, sepsis, malposition, occlusion, perirenal haematoma, injury to surrounding structures, haematuria, and death. 4 Within our patient cohort, a significant proportion, 78% remained with lifelong PN. Although we did not specifically record our complications, we documented the morbidity of long-term PN, with patients requiring a range of 0–12 further interventional radiology visits for PN-related procedures, and 0–9 emergency admissions for PN-related complications. These patients required re-siting of dislodges and occluded PN as well as regular replacement.
The presence of a PN can be associated with recurrent infections, tube displacement, blockage or dislodgement, skin irritation, urine leakage, and multiple readmissions and reinsertions. Many patients also experience anxiety and fear related to PN changes, maintenance, and difficulty with everyday tasks. A quality of life study following PN for urological malignancy by Bigum et al. found that patients had restricted physical and social activities, and mental health consequences. 13 Communication was key in managing patient expectations, and the patients that were grateful for it were those who had a symptomatic benefit from it.
Our greatest limitation of our study was its size, as with many of the previously published nephrostomy studies. This limited statistical analysis of our data to translate our outcomes to other clinical settings outside of these two hospitals. This can largely be overcome with a multicentre prospective study. The retrospective nature of the study also presented a challenge with loss of some data as well as lack of standardisation. For example, two patients did not have post-procedure creatinine tests to assess improvement of renal function following PN insertion. There was also a patient that had PN insertion based on radiological evidence of renal tract obstruction, without pre-procedure renal function tests. This is a situation that should be avoided, and PN should only be offered in the presence of abnormal serum renal function tests confirming that renal function has been compromised.
There was also limited documentation of performance status, and testosterone levels to determine if prostate cancer patients on treatment were castrate resistant. This led to the categorisation of the prostate cancer patients into their groups of treatment recurrence or resistance versus primary prostate cancer/single hormone treatment. However, knowledge of castrate levels of testosterone may have influenced the categorisation of patients between Group A and Group B and may have influenced the decision for PN. Men with available treatment options for prostate cancer are likely to be prioritised for PN due to the likelihood of longer survival than men with castrate-resistant prostate cancer. However, this was not reflected in our data, and men in Group B may have been at castrate levels at the time of presentation with malignant obstruction. Group A group largely presented with metastatic prostate cancer and malignant obstruction, so likely to have lower survival than patients with locally advanced, but non-metastatic prostate cancer.
The routine involvement of palliative care with a senior multidisciplinary approach including urology input should take place for patients with MUO considered for PN. This discussion should include the prognosis of the patient, available treatments the patient is eligible for, as well as the patient’s wishes. This can prove logistically difficult, as cancer patients at Hospital 1 are usually under the care of oncologists at a different hospital site. In this case, there is no out-of-hours access to treatment history, patient prognosis, and planned treatments. Within Group A, 16/30 (53%) of the men had already received radical, palliative or chemotherapy treatment for prostate cancer at the time of PN insertion. Similarly, 13/36 (36%) of the patients in Group C had already received radical, palliative or chemotherapy treatment for bladder cancer, and only 6/36 (17%) of this group had any plans for future further treatment documented in their notes.
It has been suggested that advanced directives for patients with progressing prostate and bladder cancer should be included with do not resuscitate (DNR) orders, which are often kept with the patient, in case of an emergency hospital admission. In a similar way that DNR orders should be thoroughly discussed, with next of kin present in an elective clinic setting when the patient is well, discussion should be had on how to proceed should they develop MUO. Patients should be presented with details on what PN involves, its risks and benefits, including the possibility of life-long PN and its implications, as well as the alternative sequalae of renal failure and death, drifting into a painless uraemia, with supportive treatment alone. The alternative of making this decision in a rushed emergency setting, without the patient’s complete medical information would be a disservice to the patient if it could have been avoided.
Considering the significant effect of PN on quality of life and a urethral catheter that many of these patients also have, we also propose consideration of unilateral PN insertion in the presence of bilateral obstruction in selected cases. This may provide adequate improvement of renal function to slow down uraemia, while reducing the number of external lines, and perhaps length of hospital stay as demonstrated in our study. In this circumstance patients should be informed of the pros and cons thoroughly. They should be informed that although a unilateral PN is easier to manage than bilateral, with a potentially shorter hospital stay, there is a potential risk of urinary tract infections and urosepsis which can be life threatening if the other kidney is not decompressed with PN. This approach may well suit patients that are not suitable for further oncological treatment but may want more time to gather their affairs in order before they further deteriorate.
Within our cohort, three patients with unilateral nephrostomies developed a worse creatinine post-PN, and some patients had normal renal function tests prior to PN insertion. Their PN were inserted based on radiological evidence of malignant obstruction. We therefore also propose that patients with MUO, particularly with end-stage bladder or prostate cancer, and unilateral hydronephrosis may be considered for conservative management and follow-up if renal function is not significantly impaired. This should be the case particularly if they are asymptomatic, with a second normal functioning kidney, and in the absence of infection. These patients, if asymptomatic should be monitored for an acceptable new baseline renal function.
In attempting to validate and update a prognostic model for the overall survival after PN for malignant obstruction, Alawneh et al. conducted a retrospective analysis of 211 patients. 2 The four risk factors that predicted a poorer survival were the type of malignancy, serum albumin <3.5 g/dL, bilateral hydronephrosis and the presence of a pleural effusion. They found that two or more of these risk factors equated to a short, expected survival time. This is a further area we hope to investigate in future studies, along with quality-of-life data. Other prognostic indicators include low serum sodium, ascites, tumour type and raised inflammatory markers. 3
Conclusion
Malignant obstructive uropathy should prompt consideration of the patient’s prognosis, and extensive patient discussion of the implications of a life-long nephrostomy. The treatment options available to patients with prostate and bladder cancer should be factored into the decision for PN with full and frank discussion with patients and their relatives, with the alternative of supportive care. Further alternatives may involve offering a patient a single nephrostomy in the better functioning kidney, where there is bilateral obstruction, or watchful monitoring in unilateral obstruction in the absence of significant symptoms or infection.
Senior urologist vetting and counselling of patients offered PN, and early liaison with oncologists on prognosis and further available treatment option should be had. With all things considered, patients that are willing to accept the risks and potential impact on quality of life, should not be denied treatment, if they understand that it will not prolong survival from the primary disease.
We hope to undertake future work on the quality-of-life experience of patients with PN, as we increasingly consider the benefits and harm caused to otherwise terminal patients.