
Abstract
Ureteral endometriosis is a rare manifestation of endometriosis that involves the infiltration of endometrial tissue into the ureters, leading to ureteral obstruction and potential renal dysfunction. However, its preoperative diagnosis is difficult. Herein, we report the case of a woman in her early 50s who presented with severe hydronephrosis of the right kidney, ureteral dilation, and suspicion of a ureteral tumor based on initial imaging studies. However, the pathological results after resection of the right kidney and right ureter revealed the presence of endometrial tissue in an ectopic location. This case highlights the importance of considering endometriosis as a differential diagnosis in cases of ureteral obstruction, even in atypical clinical scenarios, and emphasizes the need for prompt diagnosis and intervention to prevent irreversible renal damage and optimize patient outcomes.
Keywords
Introduction
Endometriosis is a chronic inflammatory condition characterized by the presence of endometrial-like tissue outside the uterine cavity. 1 It is classified into three subtypes: (a) superficial or peritoneal endometriosis; (b) ovarian endometriosis; and (c) deep infiltrating endometriosis (DIE).1–2 Among these, DIE is the most severe subtype and is characterized by subperitoneal invasion of endometriotic lesions to a depth of at least 5 mm. 2 It has an estimated prevalence of 1% in women of reproductive age and occurs in 14%–20% of all patients with endometriosis. 3
Although endometriosis predominantly affects the pelvic organs, such as the ovaries, fallopian tubes, and peritoneum, it can also involve extrapelvic sites, including the urinary tract. Urinary tract endometriosis (UTE), although rare, is a clinically significant manifestation of the disease and is considered a subtype of DIE. The incidence of UTE ranges from 0.3% to 12.0% among all patients with endometriosis and from 20.0% to 52.6% among those with DIE.1,3,4 Within the urinary tract, the bladder is the most commonly affected site (85%), followed by the ureters (10%), kidneys (4%), and urethra (2%).5–6
Ureteral endometriosis, a rare form of UTE, occurs when endometrial tissue invades or is implanted on the ureter, potentially causing obstruction and progressive renal impairment if left untreated.1,2,4 Although the exact prevalence remains unclear, ureteral endometriosis is estimated to affect 0.01%–1.70% of women with endometriosis. It typically affects women of reproductive age, with peak incidence occurring between the ages of 30 and 35 years. 2 However, cases arising in atypical age groups or those with unusual clinical manifestations can pose significant diagnostic and therapeutic challenges. 5 The risk factors identified for ureteral endometriosis include a history of pelvic surgery, advanced-stage endometriosis, and severe dysmenorrhea. 7 Despite advances in imaging techniques, preoperative diagnosis remains difficult, as the condition can mimic other pathologies such as ureteral tumors or fibrosis.2,8
Herein, we present a rare case of a woman with unilateral ureteral endometriosis, which initially masqueraded as a ureteral tumor and resulted in irreversible loss of renal function.
Case report
A woman in her early 50s initially presented to a local hospital with complaints related to a protrusion of an intervertebral disc. However, further investigation revealed severe hydronephrosis of the right kidney, along with right upper ureteral dilation and thickening of the ureteral wall below the obstructive segment, raising suspicion of a ureteral tumor. Based on these findings, she was referred to our clinic for further evaluation and management.
Upon presentation at our hospital, she denied experiencing flank pain, hematuria, or any urinary symptoms. Her medical history was significant for laparoscopic myomectomy performed to treat uterine fibroids 5 years ago. She reported regular menstrual cycles with dysmenorrhea but denied a history of infertility, chronic pelvic pain, or long-term use of combined oral contraceptives. She had one prior pregnancy, resulting in a live birth. There was no history of diagnosis of endometriosis or any related symptoms. Enhanced computed tomography (CT) revealed an enlarged right kidney with significant dilation and hydronephrosis of the right renal pelvis and calyces (Figure 1(a)). The renal parenchyma appeared thin, and the right ureter demonstrated dilation in the pelvis segment and above, with distal narrowing and a localized soft tissue nodular shadow measuring approximately 1.2 × 2.1 × 2.4 cm at the S1/S2 level (Figure 1(b)). After contrast administration, the nodular shadow enhanced, raising suspicion of a tumorous lesion. Notably, no contrast agent was evidently observed in the right renal pelvis and ureter, indicating the loss of renal excretory and perfusion function in the right kidney.

(a) Enhanced computed tomography (CT) showing an enlarged right kidney with significant dilation and hydronephrosis of the right renal pelvis and calyces and (b) the renal parenchyma appeared thin, and the right ureter demonstrated dilation in the pelvis segment and above, with distal narrowing and a localized soft tissue nodular shadow measuring approximately 1.2 × 2.1 × 2.4 cm at the S1/S2 level.
To further investigate the possibility of malignancy, the patient underwent three urine cytology examinations, all of which yielded negative results. Ureteroscopy revealed the presence of a blind-ending right ureter. Based on the clinical findings and diagnostic evaluations, we planned to perform laparoscopic surgery to remove the nonfunctional right kidney and right ureter.
During the surgical procedure, we observed significant enlargement of the right kidney with hydroureteronephrosis. A clear narrowing was noted in the lower segment of the right ureter, whereas the upper ureter showed significant thickening. The narrowed segment was hard and closely adhered to the adjacent muscle tissue. A complete resection of the right kidney and right ureter was performed, and the specimens were sent for pathological examination.
The final pathology report revealed the presence of normal endometrial glands and stroma in the excised ureter tissue, confirming the diagnosis of ureteral endometriosis (Figure 2). Following discharge, the patient continued to receive gynecological outpatient care and underwent subsequent medication treatment. At the 1- and 2-year follow-up visits, the patient remained asymptomatic and had no specific issues.
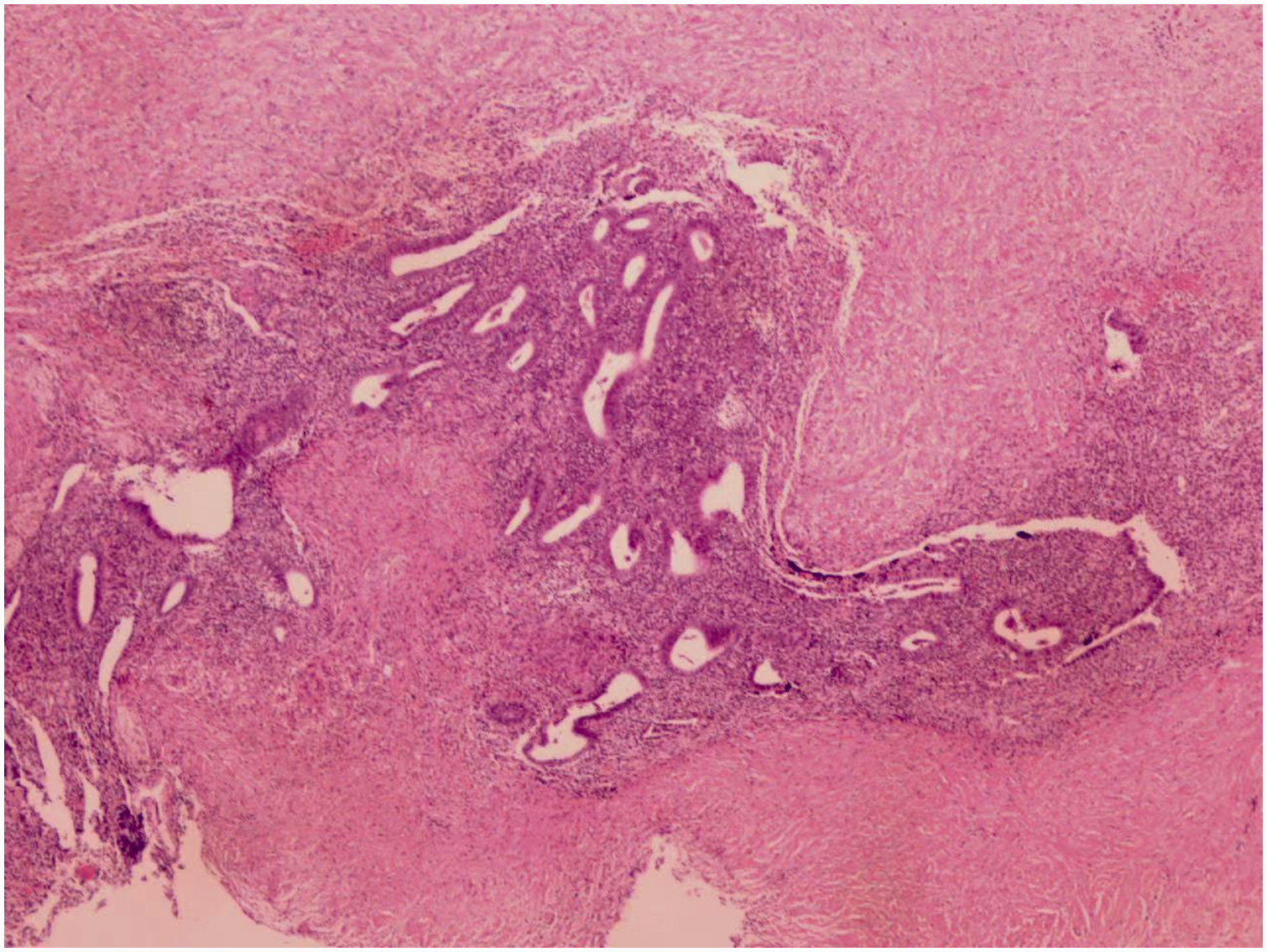
The presence of normal endometrial tissue glands and stroma in the excised ureter tissue, confirming the diagnosis of ureteral endometriosis (Hematoxylin and Eosin staining, 100×).
The reporting of this study conforms to the Case Report (CARE) guidelines. 9 All patient information has been deidentified, and written informed consent was obtained for treatment and publication of this article and accompanying images. Ethical approval was obtained from the Ethics Committee of West China Fourth Hospital, Sichuan University (HXSY-EC-2023051).
Discussion
Extragenital involvement of endometriosis in the urinary tract is a rare occurrence, with the urinary system being the second most commonly affected site following the gastrointestinal tract. 6 Histologically, ureteral endometriosis can be classified into two subtypes based on its location and characteristics: extrinsic and intrinsic. The extrinsic subtype is more prevalent than the intrinsic one; moreover, it is characterized by the invasion of endometrial glandular or stromal cells into the adventitia of the ureter or surrounding connective tissue. Conversely, the intrinsic subtype involves the presence of endometrial tissue within the muscularis propria, lamina propria, or ureteral lumen.2,4,6,8 In our patient, the pathological findings confirmed the presence of intrinsic endometriosis in the right ureter, evidenced by lumen invasion leading to ureteral obstruction and complete loss of renal function.
Although the exact pathophysiology of endometriosis remains unclear, several theories have been proposed to explain the development of endometrial tissue in ectopic locations. The most widely accepted theory is the retrograde menstruation theory, which suggests that endometrial cells are transported through the fallopian tubes during menstruation and implanted into the peritoneal cavity or other sites. Other proposed mechanisms include lymphatic or vascular dissemination, coelomic metaplasia, and embryonic cell rests.1,2,4,8
Preoperative diagnosis of intrinsic ureteral endometriosis can be difficult. Ureteral endometriosis typically affects women of reproductive age and is most often observed at the pelvic brim or the lower third of the ureter, particularly where the ureter crosses the broad ligament, making it susceptible to compression or infiltration by endometrial tissue.2,5 From the pathophysiological perspective, endometrial tissues within or surrounding the ureters undergo the same hormone-dependent periodic changes as normal uterine endometrium. This leads to cyclic bleeding, desquamation, and necrosis, which may promote fibrosis, ultimately resulting in ureteral stenosis and obstruction.2,10 Symptoms of ureteral endometriosis are often nonspecific and depend on the extent and location of the lesions. Common symptoms include renal colic, back pain, and, in some cases, cyclic hematuria, with symptoms often worsening around menstruation. More than half of the affected patients report dysmenorrhea, dyspareunia, and chronic pelvic pain, although asymptomatic cases are commonly observed.2,4,10
In this case, the patient, who was in her early 50s, exhibited an atypical age for the presentation of ureteral endometriosis, as it is more commonly diagnosed in younger, premenopausal women. Additionally, she did not report any of the characteristic symptoms associated with ureteral endometriosis, such as dysmenorrhea, dyspareunia, or cyclic hematuria, and had no history of infertility or chronic pelvic pain. The obstruction was observed on the right side, which is less common than left-sided involvement. The degree of renal dysfunction in this patient was severe, with imaging findings suggesting an atrophic right kidney. Enhanced CT revealed no perfusion of the right kidney. However, the significant degree of hydronephrosis, along with thinning of the renal parenchyma, strongly indicated complete loss of renal function. All these characteristics posed challenges in the initial diagnosis and management of her condition. Other studies reported the same situation.11,12 Thus, this study highlights the importance of considering endometriosis as a differential diagnosis even in older patients with atypical symptomatology and emphasizes the need for early diagnosis and intervention in cases of ureteral endometriosis, as prolonged obstruction can lead to irreversible renal damage.
Medical therapy, such as hormonal treatments or gonadotropin-releasing hormone agonists, has limited efficacy in cases of ureteral endometriosis with significant obstruction and renal dysfunction.2,5 Although these treatments may provide symptomatic relief or temporarily halt the progression of endometriosis, they are unlikely to reverse established ureteral obstruction or restore renal function. Surgical therapy is the mainstay of treatment for ureteral endometriosis, with the primary goals being the relief of ureteral obstruction, preservation or restoration of renal function, and prevention of recurrence. The specific surgical approach depends on the extent of ureteral involvement, degree of renal dysfunction, and patients’ fertility desires.2,3,5 In cases of severe ureteral obstruction with significant renal impairment, as in the current patient, the surgical options may include ureterolysis, segmental ureteral resection with end-to-end anastomosis, or nephroureterectomy. In this case, considering the complete loss of renal function in the right kidney, nephroureterectomy was deemed the most appropriate approach. The chosen surgical approach for this patient was justified by the severe hydronephrosis, loss of renal function, and the extent of ureteral involvement, including the adherence of the obstructed segment to the psoas muscle. This approach effectively addressed the underlying pathology and prevented potential complications such as recurrent infections or malignant transformation.
Conclusion
Ureteral endometriosis is a rare but serious condition that requires early diagnosis and prompt intervention to prevent irreversible complications such as renal function loss. This case underscores the importance of maintaining a high index of suspicion for ureteral endometriosis even in patients with atypical presentations or advanced age. Multidisciplinary collaboration and previous use of exploratory procedures, including imaging and surgical evaluation, are crucial for optimizing patient outcomes. Further research is needed to refine diagnostic strategies and expand treatment options for this challenging condition.
Footnotes
Acknowledgements
None.
Contribution statement
Rui QU: Manuscript writing and revising. Luo YANG: Manuscript writing and revising. Yi DAI: Performing surgery and manuscript writing and revising. All authors read and approved the final manuscript.
Data availability
All data in this manuscript can be made available based on reasonable request to the corresponding author.
Declaration of conflicting interests
All authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author biographies
Rui Qu, MD, Department of Urology and Andrology, West China Fourth Hospital, Sichuan University, Chengdu, 610041, PR China. Research interest: urological tumor, prostatic disease, male sexual dysfunction, male infertility. ORCID: 0000-0002-1722-9835
Luo Yang, MD, Department of Urology and Andrology, West China Fourth Hospital, Sichuan University, Chengdu, 610041, PR China. Research interest: urinary tract infection, prostatic disease, male sexual dysfunction, male infertility. ORCID: 0000-0003-3214-7691
Yi Dai, MD, Department of Urology and Andrology, West China Fourth Hospital, Sichuan University, Chengdu, 610041, PR China. Research interest: urinary incontinence, urinary tract infection, female sexual dysfunction.