
Abstract
Interferon-free regimens combine different second-wave direct-acting antiviral agents (DAAs), which target the main viral proteins involved in the replication cycle of hepatitis C virus (HCV): NS3/4A protease inhibitors (simeprevir or paritaprevir boosted by ritonavir), NS5B nucleos(t)idic (sofosbuvir) and nonnucleos(t)idic (dasabuvir) polymerase inhibitors, NS5A replication complex inhibitors (daclatasvir, ledipasvir, elbasvir, velpatasvir). Combinations of two or three DAAs, given for 8–24 weeks reach sustained virology response (SVR) rates greater than 90% with good tolerance. SVR rates and safety are similar in clinical trials and in real life, usually higher than 95% in the per-protocol analysis. Next-generation DAAs are now expected. To be competitive, these new combinations need to prove their added value regarding the pill burden, the reduced duration of treatment, the drug–drug interaction profile and safety. Zepatier is a fixed-dose combination product coformulating MK-5172 [grazoprevir (GZR), 100 mg QD] and MK-8742 [elbasvir or (EBR) 50 mg QD]: it combines highly potent inhibitors of the HCV NS3/4A protease and NS5A replication complex, respectively. This review provides a summary of the main evidence available for the use of GZR/EBR and highlights the strength of this combination.
Keywords
Introduction
An estimated 150 million people are chronically infected with hepatitis C virus (HCV) worldwide resulting in significant morbidity and mortality (500,000 to 1.4 million yearly) due to hepatic and extra-hepatic manifestations [European Association for the Study of the Liver (EASL), 2015; Lee et al. 2012]. The sustained virologic response (SVR), which corresponds to a complete recovery achievable with antiviral treatments, significantly reduces morbidity (hepatocellular carcinoma, liver transplantation) and extra-hepatic mortality [Fontaine et al. 2000]. The overall mortality in patients achieving SVR has reduced by 75%, especially in cirrhotic patients but also in HIV/HCV coinfected patients; the occurrence of hepatocellular carcinoma and the need of liver transplantation at 5-year follow up have dropped from 15% to 5% and from 10% to 1.2%, respectively, as shown in a recent meta-analysis of patients receiving an interferon-including regimen [Simmons et al. 2016]. In a prospective French study of more than 1300 HCV-infected patients with biopsy-proven cirrhosis (the Cirvir ANRS CO12 cohort), a significant decrease in the occurrence of hepatocellular carcinoma, bacterial spontaneous peritoneal infection or other cirrhosis complications was reported in patients achieving SVR as well as a 50% decrease in the occurrence of vascular disease (cardiovascular or cerebrovascular disease) at 3 or 5 years of post-treatment follow up [Nahon et al. 2016]. All of these data, in line with registry studies [Hsu et al. 2015; Nahon et al. 2016], underline the need to achieve SVR in most HCV-infected patients which means more extensive screenings, improvements in access to care and treatment.
Pegylated interferon alfa in combination with ribavirin (PR), which led to SVR rates of 45% in patients with HCV genotype (GT) 1, 65% in GT4 patients, 70% in GT3 patients and of 85% in GT2 patients, has been the standard of care for two decades [European Association for the Study of the Liver (EASL), 2011]. It has been replaced from 2011 to 2013 by a combination of PR and first-generation NS3/4A protease inhibitors (telaprevir or boceprevir) in patients with HCV GT1, allowing about 70% SVR to be reached and the duration of therapy to be reduced from 48 to 24 weeks in half of the treated patients [Hezode et al. 2014a]. These first-generation regimens unexpectedly disappeared in 2014 with the rapid availability of interferon-free regimens combining two or three second-wave direct-acting antiviral drugs (DAAs) with or without ribavirin (RBV). DAAs target specific nonstructural viral proteins involved in the replication cycle of HCV and include NS3/4A protease inhibitors (simeprevir or paritaprevir boosted by ritonavir), NS5B nucleos(t)idic (sofosbuvir) and non nucleos(t)idic (dasabuvir) polymerase inhibitors, and NS5A replication complex inhibitors (daclatasvir, ledipasvir, elbasvir, velpatasvir). The combinations are given for 8–24 weeks, according to baseline factors such as fibrosis stage, genotype and subtype, baseline viral load, prior therapeutic history of the patient (naive or experienced), pre-existing resistance-associated substitutions (RASs), and SVR rates greater than 90% with good tolerance. SVR and safety rates are similar in clinical trials and in the real-life studies, usually higher than 95% in per-protocol analysis [EASL, 2015].
Despite these great achievements, new treatments are about to be launched (grazoprevir/elbasvir: Zepatier) and next-generation DAAs are finalizing their phase III studies: sofosbuvir/velpatasvir in the Astral program, the pangenotypic triplet sofosbuvir/velpatasvir with the protease inhibitor GS9857 in the Polaris program and the pangenotypic Abbvie combination of a second-generation protease inhibitor (ABT-493) with a NS5A inhibitor (ABT-530, in the Endurance, Magellan, Expedition studies). To be competitive, these new combinations need to prove their added value regarding the pill burden, the duration of treatment, the RBV use, the drug-drug interaction profile and the safety/tolerability profile. A single tablet regimen (STR), RBV-free, with a low drug–drug interaction profile and a good safety profile appear to be prerequisites as well as the reduced duration of therapy (6 or 8 weeks instead of 12 weeks).
This review provides a summary of the available data for GZR/EBR combination and reviews the advantages that this combination offers over previous treatments.
The biology of grazoprevir/elbasvir combination therapy
Zepatier is an oral fixed-dose combination (FDC) of 100 mg GZR (MK-5172), an HCV NS3/4A protease inhibitor, and 50 mg EBR (MK-8742), an HCV NS5A inhibitor. This FDC single tablet has the potential to provide an all-oral, highly efficacious, simple, and well-tolerated regimen for the treatment of patients with chronic HCV GT1, GT4 or GT6 infection.
The mean half-life for EBR (50 mg) and GZR (100 mg) is about 24 and 31 hours, respectively, allowing once-daily dosing. EBR and GZR are partially eliminated by oxidative metabolism by CYP3A. Co-administration of moderate or strong CYP3A inducers with GZR/EBR may decrease GZR/EBR plasma concentrations and reduce its therapeutic effect. Co-administration of strong CYP3A4 inhibitors with GZR/EBR may increase GZR/EBR concentrations and cause harmful effects. In HCV/HIV coinfection, GZR/EBR is contraindicated with efavirenz (a CYP3A inducer) and with the HIV protease inhibitors atazanavir, darunavir, lopinavir, saquinavir and tipranavir (CYP3A4 inhibitors). Conversely, this DAAs combination can be co-administered with antire-troviral regimens that contain the integrase inhibitor, raltegravir and dual nonnucleoside reverse transcriptase inhibitors (e.g. tenofovir or abacavir + emtricitabine or lamivudine) without dosage adjustments [Yeh, 2015].
The main route of GZR/EBR elimination is through feces (greater than 90%) with extremely low renal elimination (less than 1% in urine), explaining why changes in exposure of GZR and EBR are not clinically significant in patients with renal impairment (including those on hemodialysis) [Yeh et al. 2014].
To date, there are no adequate data in humans to establish whether GZR/EBR combination is associated with any risk during pregnancy and lactation. Hence, GZR/EBR should not be used in pregnant women or in nursing mothers. The use in combination with RBV is contraindicated in pregnant women and in men whose female partners are pregnant.
Similarly to what was observed with other protease inhibitors, there is a risk of alanine transaminase (ALT) elevations [to greater than five times the upper limit of normal (ULN)], mainly appearing after 2 months of therapy which resolves after treatment discontinuation or completion of therapy. Hepatic laboratory testing should be performed prior to treatment and monthly during therapy [Yeh et al. 2014].
In in vitro and in vivo studies, the combination GZR/EBR showed a high genetic barrier to resistance and activity against the common RASs. In patients with GT1b and GT4 HCV infection, there is no impact of baseline NS3 or NS5A RASs on SVR rates with GZR/EBR in clinical trials but in HCV GT1a patients, the presence of one or more baseline NS5A polymorphisms (M28, Q30, L31 or Y93) is associated with lower SVR rates with GZR/EBR for 12 weeks.
GZR/EBR combination (Zepatier), with or without RBV, has been recently approved by FDA in the US for the treatment of patients with chronic HCV GT1 and GT4. The approval is expected in the near future also in Europe and Asia. The recommended dosage is one tablet taken orally once daily with or without food. No dosage adjustment is recommended in patients with any renal impairment or in patients with Child–Pugh (CP) A cirrhosis. Zepatier is contraindicated in patients with CP-B or CP-C cirrhosis and in patients receiving strong CYP3A inducers or inhibitors, such as some antiretroviral agents. Patients with GT1a infection should undergo a baseline evaluation for RASs.
Grazoprevir/elbasvir combination therapy: main studies
The safety, tolerability and efficacy of the once daily, oral combination of GZR/EBR with and without RBV has been evaluated for the treatment of HCV GT1, GT4 and GT6 infection in previously untreated or treatment experienced, cirrhotic or noncirrhotic patients, with and without HIV coinfection.
Phase II studies in HCV monoinfection
In phase II studies, an 8- to 12-week regimen of GZR and EBR (without RBV) resulted in high SVR rates among treatment-naive and experienced patients with HCV GT1 infection, including those with compensated cirrhosis [Buti et al. 2016; Forns et al. 2015; Hezode et al. 2014b; Lawitz et al. 2015].
C-WORTHY trial
In the C-WORTHY, randomized, open-label phase II trial (part B), two cohorts of patients received GZR/EBR FDC tablet once daily with or without RBV for 12 or 18 weeks (Table 1). A total of 253 patients were included in the study, of which 123 (cohort 1) were treatment-naive with cirrhosis and 130 (cohort 2) were patients with previous PR null response with or without cirrhosis [Lawitz et al. 2015].
C-WORTHY studies.

mITT: modified intention-to-treat, one patient who discontinued treatment early unrelated to adverse event or virological failure was excluded.
GT, genotype; RBV, ribavarin; SVR12, sustain virological response at 12 weeks.
Patients were predominantly men (58%), with a median age of 56 (18–82) years. The majority had cirrhosis (67%) and GT1a infection. SVR12 was achieved in 95% (240/253) of the total population. In cohort 1, SVR12 rates were achieved in 90% (28/31) and 97% (28/29) in a 12-week course regimen of GZR/EBR with and without RBV, respectively, and 97% (31/32) and 94% (29/31) in an 18-week course, with and without RBV, respectively. In cohort 2, SVR12 rates were achieved in 94% (30/32) and 91% (30/33) in a 12-week course regimen of GZR/EBR with and without RBV, respectively, and in 100% (33/33) and 97% (31/32) in an 18-week course with and without RBV, respectively.
A total of 10 (4%) patients had virological failure (8 relapses and 2 breakthroughs) and 3 patients were lost to follow up or discontinued early due to reasons other than virological failure.
Most common adverse events were headache, asthenia and fatigue. A total of seven out of 253 (3%) patients had serious adverse events but only one of these was drug related; two (1%) patients stopped treatment due to adverse event and one patient died.
In the C-WORTHY, randomized, open-label, phase II trial (part C), naive noncirrhotic GT1b-infected patients received GZR/EBV FDC tablet once daily with (n = 30) or without RBV (n = 31) for 8 weeks [Hezode et al. 2014b]. In a modified intention-to-treat analysis (excludes one patient who discontinued early due to causes unrelated to adverse events or virological failure), the SVR12 was achieved in 93% (27/29) of patients in the RBV arm and in 94% (29/31) of patients in the RBV free arm.
In summary, in GT1b-infected patients, a 12 week-course of GZR/EBR without RBV is recommended.
C Salvage: HCV GT1 patients, with or without cirrhosis, after failure with PR plus direct acting antiviral agent
In the C-SALVAGE open-label phase II trial, HCV GT1-infected patients with or without cirrhosis who failed to reach SVR after more than 4 weeks of PR plus either boceprevir (35.4%), telaprevir (54.4%) or simeprevir (10.1%) were given GZR/EBV FDC tablet once daily with RBV (n = 79) for 12 weeks (Table 2) [Forns et al. 2015].
C-SALVAGE studies.

GT, genotype; PI, protease inhibitor; PK, pharmacokinetic; PR, pegylated interferon alfa in combination with ribavirin; RBV, ribavarin; SVR12, sustain virological response at 12 weeks; SVR24, sustain virological response at 24 weeks.
A total of 79 patients were included (median age of 55 years, 58% men, 62% GT1b, 43% with cirrhosis, 83.5% had past history of virological failure); 34 of 78 evaluable patients had baseline NS3 RASs. SVR12 were 96.2% (77/79) overall, including 95.5% (63/66) of patients with prior virologic failure and 100% (13/13) of patients without baseline RAVs.
The most common adverse events were fatigue, headache, asthenia and gastrointestinal complaints. Five serious adverse events were reported but were considered non-drug-related. Only two (2.5%) patients had anemia (hemoglobin level lower than 9 g/dl) due to RBV association.
None of the patients experienced a late relapse [Buti et al. 2016] and SVR24 was overall 96.2%. In the three relapses which occurred at week 8 post-treatment, baseline NS3 and NS5A RASs were found at the time of relapse and persisted throughout follow-up. NS3 A156T emerged in two of the three patients and disappeared in one patient (data was not available for the other patient), while NS5A Y93H emerged in two patients and persisted for the whole follow-up period.
In summary, in GT1-infected patients, with or without cirrhosis, after failure with PR plus a direct-acting antiviral agent, a 12-week course of GZR/EBR with RBV is recommended.
C Salt: GT1 and CP-B cirrhosis
In this phase II, nonrandomized, open-label study C Salt, 30 patients with HCV GT1 infection and CP-B cirrhosis were included and 10 noncirrhotic patients with HCV GT1 infection were enrolled for pharmacokinetic (PK) analyses (PK arm) [Jacobson et al. 2015] (Table 3). GZR and EBR were administered in cirrhotic CP-B patients as separate entities: GZR 50 mg was used, modeled upon exposure of GZR in non-HCV-infected CP-B patients. In noncirrhotic patients FDC was used. Patients received treatment for 12 weeks without RBV.
C-SALT study.
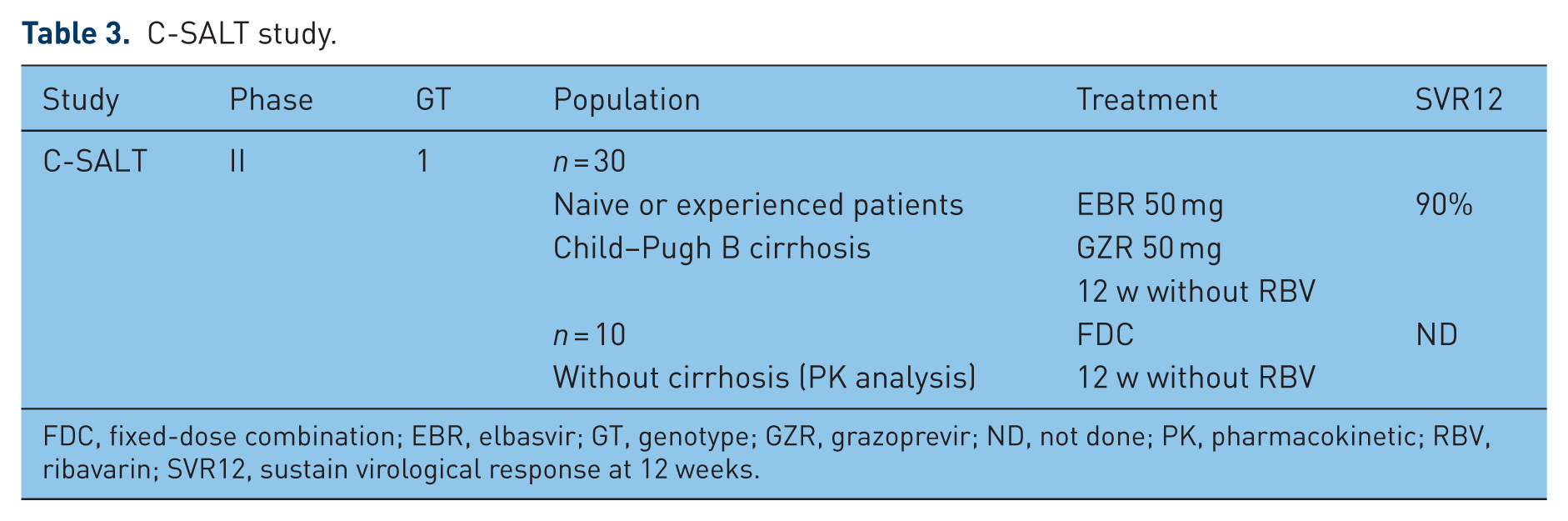
FDC, fixed-dose combination; EBR, elbasvir; GT, genotype; GZR, grazoprevir; ND, not done; PK, pharmacokinetic; RBV, ribavarin; SVR12, sustain virological response at 12 weeks.
In the CP-B arm, 17 patients (58%) were male, with a mean age of 58.3 (±7) years, 27 (90%) were GT1a, 19 (63.3%) were treatment naive, 21 (70%) were CP-B 7, 7 (23.3%) CP-B 8 and 2 (6.7%) CP-B 9. The mean MELD score was 9.9 (± 2.5).
The SVR12 rate was 90% in the CP-B arm. The MELD score decreased in 11 patients, was unchanged in 11 patients and increased in 6 patients at 12-week follow-up. One CP-B7 patient died (see below).
GZR exposure was slightly higher in patients with CP-B cirrhosis receiving 50 mg dose compared to noncirrhotic patients receiving 100 mg dose, while EBR (50 mg) PK was similar in both patient populations.
Fatigue, arthralgia, nausea, pyrexia and headache were the most common adverse events in both patient groups. Four (13.3%) patients had serious adverse event in the CP-B arm, all considered as unrelated to study drugs. No patient discontinued treatment due to adverse events but one patient died in the CP-B arm: he had a CP-B 7 cirrhosis at baseline and died of progressive liver failure at follow-up week 4 after having spontaneous bacterial peritonitis on-treatment with subsequent cerebral infarction, bacterial peritonitis and hepatic failure.
In summary, in GT1-infected patients and CP-B cirrhosis, a 12-week course of GZR 50 mg and EBR 50 mg was highly effective and well tolerated.
Phase III studies in HCV monoinfection
C Edge naive with or without cirrhosis patients
In the C Edge naive (C-EDGE N) phase III, randomized, placebo-controlled trial in GT1, GT4 and GT6 patients with or without cirrhosis, 316 patients were given GZR/EBR FDC tablet once daily, without RBV, for 12 weeks. After a 4-week follow-up period, placebo recipients (n = 105) received open-label GZR/EBR (Table 4) [Zeuzem et al. 2015]. There were 91% of GT1 HCV-infected patients (GT1a 50%, GT1b 41%), 6% of GT4 and 3% of GT6, respectively and 22% of patients had cirrhosis. In the full analysis set, the SVR12 was achieved in 95% (299/316) in all patients: 92% (144/157), 99% (129/131), 100% (18/18) and 80% (8/10) in GT1a-, GT1b-, GT4- and GT6-infected patients, respectively. There were nonvirological failures in four patients, breakthrough in 1 and relapse in 12, mostly in GT1a patients (3, 1 and 9, respectively). The SVR rates were 97.1% (231/246) in cirrhotic patients and 93.9% (68/70) in noncirrhotic patients, respectively. Patients with baseline low viral load (⩽ 800,000 IU/ml) achieved a SVR in 100% (94/94) and those with high viral load (> 800,000 IU/ml) in 92.3% (215/222).
C-EDGE studies.

GT, genotype; ITT, intention-to-treat; PK, pharmacokinetic; RBV, ribavarin; SVR12, sustain virological response at 12 weeks.
The most common adverse events were headache, nausea and fatigue, occurring at similar frequencies in patients receiving active and placebo drugs. The safety profile was similar in cirrhotic and noncirrhotic patients. A total of 9 of 316 (3%) patients had serious adverse events (none were considered drug related) and 3 of 316 (1%) patients discontinued treatment due to adverse events in the GZR/EBR arm compared with 3 of 105 (3%) patients and 1 of 105 (1%) in the placebo arm, respectively. Two patients died and both deaths were not considered to be related to the study treatment.
This study evidences the safety and efficacy of the GZR/EBR combination which should be given for 12 weeks without RBV in naive patients irrespective of the fibrosis stage.
C Edge experienced patients with or without cirrhosis
In the C Edge experienced (C-EDGE TE) phase III, randomized, open-label trial in HCV GT1, GT4 and GT6 patients with or without cirrhosis, who previously failed to PR, GZR/EBR FDC tablets were administered once daily, with or without RBV, for 12 or 16 weeks in 420 patients, randomized in a 1.1.1.1 ratio (Table 4) [Kwo et al. 2015]. There was a majority of GT1, 35% of patients had cirrhosis and 5% had HIV/HCV coinfection. There were 43% of prior null responders, 21% of prior partial responders and 36% of prior relapsers, respectively.
In an intention-to-treat analysis set, SVR12 was achieved in 94% (98/104) of patients treated with 12 weeks RBV, in 92% (97/105) of patients treated without RBV for 12 weeks, in 97% of patients (103/106) treated with 16 weeks RBV and in 92% (97/105) of patients treated for 16 weeks without RBV, respectively.
In patients with history of prior relapse, SVRs were 100% in all arms except in the GZR/EBR 16-week arm (92%). In patients with history of prior null or partial response, SVRs were both 91% in the 12-week GZR/EBR regimen with or without RBV, respectively, and 100% and 94% in the 16-week GZR/EBR arms with or without RBV, respectively.
There were nonvirological failures in 6/420 (1.5%) patients and virological failures in 19/420 (4.5%). In 12 GT1a patients with virological failures, 10 had baseline NS5A RASs.
Most common adverse events were headache, nausea and fatigue. A total of 420 (3.4%) patients had serious adverse events and 7 of 420 (1.7%) patients discontinued treatment due to adverse events. In the two RBV arms, hemoglobin levels were lower than 10 g/dl in 9/105 (8.7%) patients treated for 12 weeks and in 22/106 (20.8%) patients treated for 16 weeks, respectively. There were no deaths in the study.
In summary, 12 weeks of GZR/EBR without RBV achieved SVR12 in 100% of both GT1b-infected patients and patients with history of previous PR relapse whereas 16 weeks of GZR/EBR with RBV achieved high SVR rates (94–100%) with no virological failures regardless of the cirrhosis status, prior treatment history or the presence of NS5A RASs.
C Swift: naive patients with or without cirrhosis
In the C Swift trial, HCV GT1 and GT3 naive noncirrhotic or cirrhotic patients received the combination of GZR (100 mg QD)/EBR (50 mg QD) and sofosbuvir 400 mg QG [Poordad et al. 2015] (Table 5). GT1 noncirrhotic patients were randomized to 4 (n = 31) or 6 weeks (n = 30) while GT1 cirrhotic patients were randomized to 6 (n = 20) or 8 weeks (n = 21). GT3 noncirrhotic patients were randomized to 8 (n = 15) or 12 weeks (n = 14) and cirrhotic patients (n = 12) were assigned to 12 weeks of treatment.
C-SWIFT study.
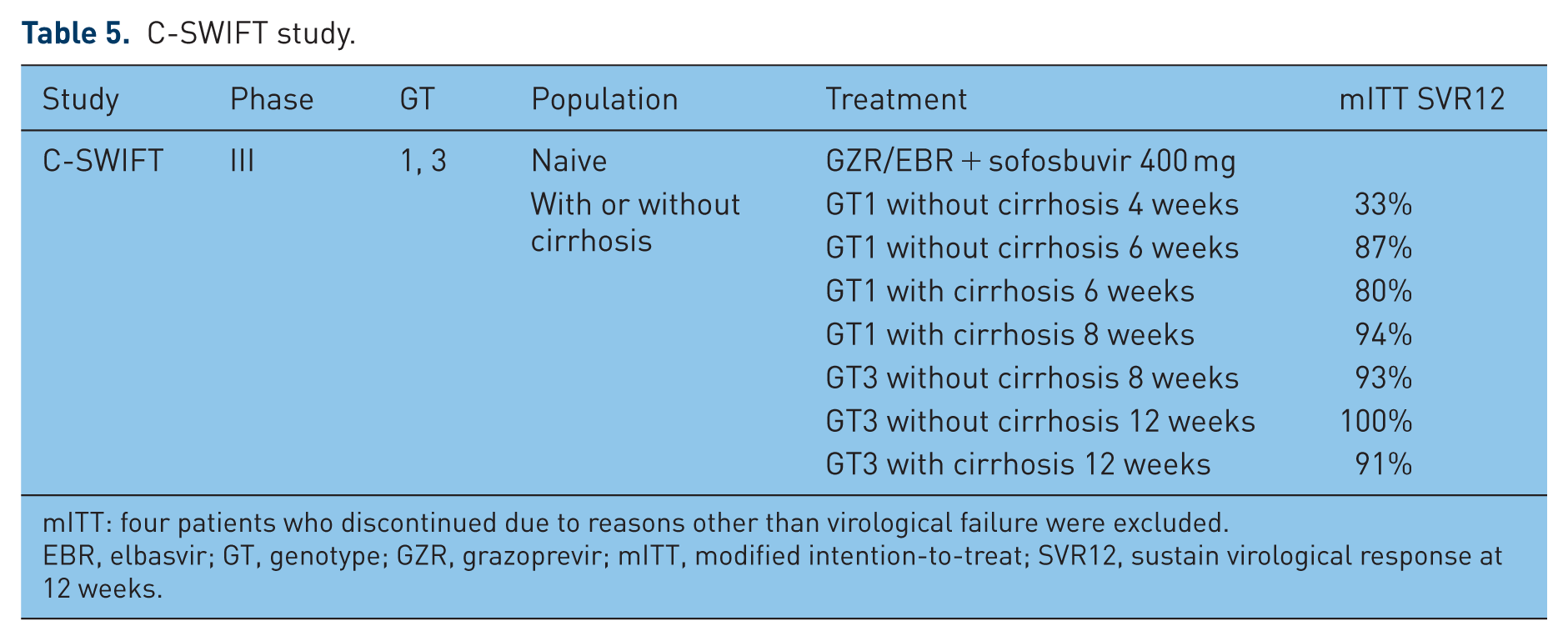
mITT: four patients who discontinued due to reasons other than virological failure were excluded.
EBR, elbasvir; GT, genotype; GZR, grazoprevir; mITT, modified intention-to-treat; SVR12, sustain virological response at 12 weeks.
The SVR12 rates modified in intention-to-treat analysis (four patients who discontinued due to reasons other than virological failure were excluded) were 33% and 87% in GT1 noncirrhotic patients treated 4 and 6 weeks, respectively, and 80% and 94% in GT1 cirrhotic patients treated 6 and 8 weeks, respectively. A total of 20 patients had relapse in the 4-week arm, eight patients in both 6-week arms (four noncirrhotic and four cirrhotic patients) and one patient in the 8-week arm.
The SVR12 rates modified in intention-to-treat (one early discontinuation due to reasons other than virological failure) were 93% and 100% in GT3 noncirrhotic patients treated for 8 and 12 weeks, respectively, and 91% in GT3 cirrhotic patients treated for 12 weeks. One patient had relapse in the 8-week arm.
The most common adverse events were headache, fatigue and nausea. Only two patients had serious adverse events, one patient discontinued at week 4 due to B-cell lymphoma and no patient died.
In summary, reduction to 6 weeks or less of GZR/EBR + sofosbuvir combination is associated with lower SVR rates in GT1, naive, cirrhotic and noncirrhotic patients. The triple combination provides encouraging results in GT3-infected patients, naive, cirrhotic and noncirrhotic patients treated for 8–12 weeks according to the fibrosis stage.
Special populations
C Worthy and C Edge in HCV/HIV-infected patients
HCV coinfection is common among people living with HIV infection: among the 150 million HCV-infected persons worldwide, approximately 5 million are coinfected with HIV (Table 6) [Wandeler et al. 2012]. Hepatitis C is one of the three leading causes of death among people living with HIV, due to the more rapid progression of HCV disease which leads to cirrhosis, end-stage liver disease, hepatocellular carcinoma (HCC), liver transplant and death [Ly et al. 2012; Van der Helm et al. 2013; Wandeler et al. 2012]. Although SVR has been associated with a lower risk of HCV-related morbidity and mortality in patients with HCV monoinfection and HIV/HCV coinfection [Berenguer et al. 2009; Limketkai et al. 2012; Simmons et al. 2016], interferon-including HCV treatments had limited effectiveness in coinfected patients and was associated with several clinically significant adverse effects [Pol and Soriano, 2008; Salmon et al. 2013].
Special population HIV/HCV, stage 4–5 CKD and PWIDs: C-WORTHY, C-EDGE, C-SURFER and C-EDGE CO-STAR studies.
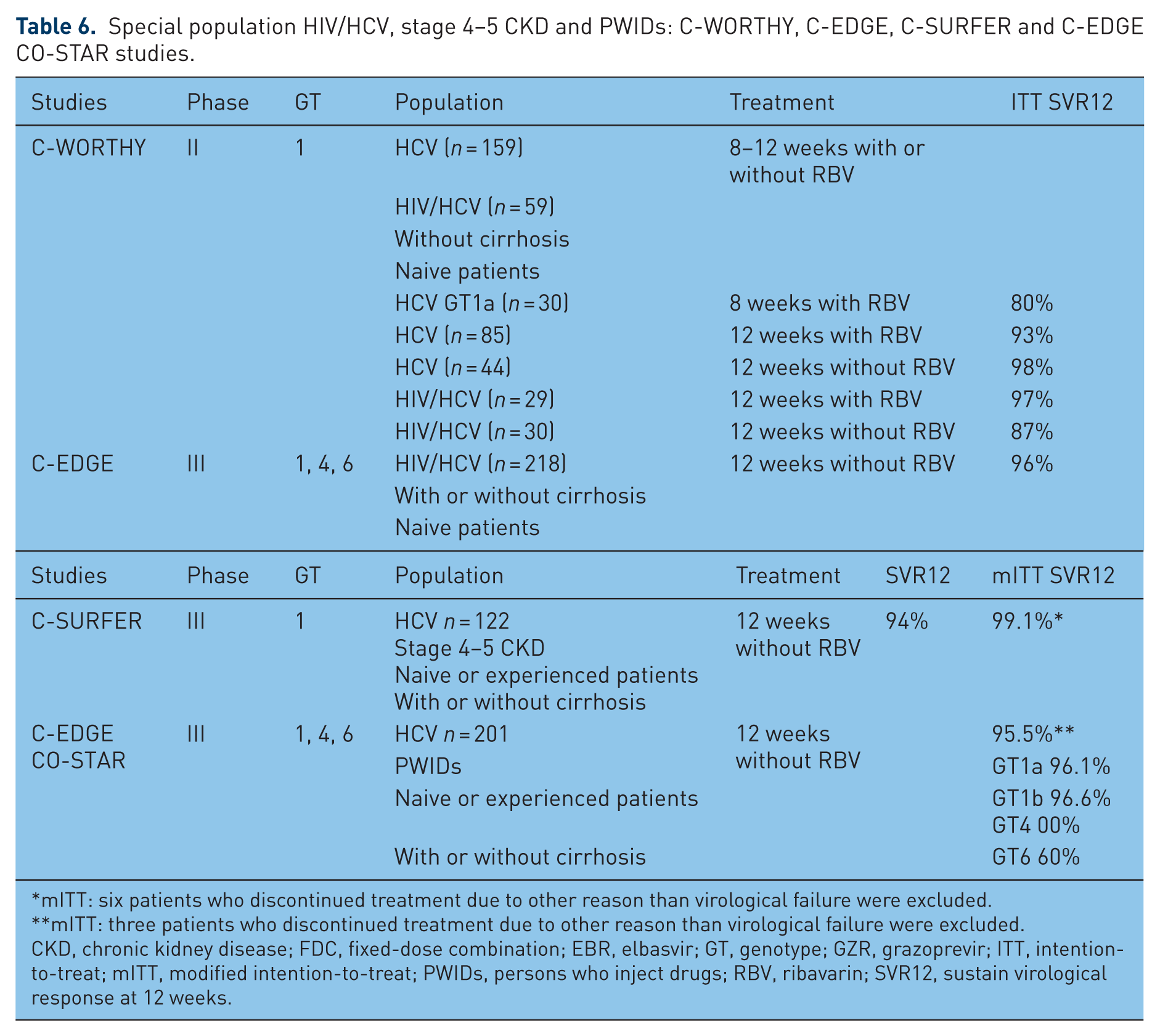
mITT: six patients who discontinued treatment due to other reason than virological failure were excluded.
mITT: three patients who discontinued treatment due to other reason than virological failure were excluded.
CKD, chronic kidney disease; FDC, fixed-dose combination; EBR, elbasvir; GT, genotype; GZR, grazoprevir; ITT, intention-to-treat; mITT, modified intention-to-treat; PWIDs, persons who inject drugs; RBV, ribavarin; SVR12, sustain virological response at 12 weeks.
The DAAs combinations have minimized the negative impact of host factors, such as race/ethnicity, IL28B, genotype and HIV coinfection, on the likelihood of achieving SVR: HCV/HIV coinfected patients achieve SVR rates similar to those observed in HIV-negative patients [Naggie and Sulkowski, 2012].
The C Worthy phase II trial compared the GZR/EBR combination for 8 or 12 weeks, with or without RBV in noncirrhotic HCV monoinfected GT1 patients (n = 159) and in HIV/HCV coinfected patients (n = 59) [Sulkowski et al. 2015]. The 218 patients were mostly white (88%), male (59%), median age was 50 years, 56% had baseline HCV-RNA >2,000,000 IU/ml, 72% were HCV GT1a and 73% were IL28B non-CC genotype (there are three genotypes CT, TT or CC). HIV/HCV coinfected patients as compared with HCV monoinfected patients were more frequently males (80% versus 51%), younger (median age = 47 versus 51 years), with higher baseline HCV RNA (27% versus 16% with >10 × 106 IU/ml) and lower BMI (23.0 versus 26.4 kg/m2). The rates of HCV RNA decline on-treatment were similar between HIV/HCV coinfected and HCV monoinfected patients and between patients treated with or without RBV. SVR12 rates in the intention-to-treat analysis were not different between both HIV/HCV coinfected or HCV monoinfected patients and those who were treated with or without RBV. SVR12 was achieved in 91.5% (54/59) and 94.6% (122/129) of HIV/HCV coinfected patients and HCV monoinfected patients, respectively, treated with 12 weeks of GZR/EBR with or without RBV. GZR/EBR for 12 weeks without RBV achieved SVR12 of 87% (26/30) and 98% (43/44) in HIV/HCV coinfected patients and HCV monoinfected patients, respectively. SVR12 rate was only 80% (24/30) in HCV monoinfected patients with GT1a who received GZR/EBR with or without RBV for 8 weeks. The rates of virological failure were 4% (7/188; three breakthroughs and four relapses) in the 12-week treatment group and 17% (5/30; five relapses) in the 8-week treatment group: 10/12 virological failures were HCV GT1a. The only predictor of absence of SVR between coinfected and monoinfected patients was IL28B non-CC genotype (SVR12 rates were 85% (34/40) and 95% (95/100), respectively).
In summary, in GT1, naive, noncirrhotic, HIV/HCV coinfected patients a 12-week course of GZR/EBR with or without RBV should be given.
The C Edge phase III study confirmed the high potency (95% SVR) and the good safety profile (no discontinuation) of the all-oral, FDC GZR/EBR in 218 HIV/HCV coinfected patients [Rockstroh et al. 2015], including 16% of cirrhotic patients, with HCV GT1, GT4 and GT6, with comparable response rates: 1. to other studies in HCV monoinfected patients; 2. across all patient subgroups, including Black/African American, and cirrhotic and noncirrhotic patients. In addition, persistent loss of HIV suppression and/or antiretroviral failure was not observed.
This study confirmed that HIV coinfection does not impair the efficacy of the GZR/EBR combination. This should be given for 12 weeks to HCV/HIV coinfected patients with a careful attention to the choice of antiretroviral therapies in order to avoid any risk of drug–drug interactions.
C Surfer in patients with renal failure
Although the prevalence of HCV infection has markedly decreased in patients who are candidates for renal transplantation, since the introduction of screening, hygiene and prevention measures (including systematic screening of blood and organ donations, use of erythropoietin and compliance with universal hygiene rules), it remains high in dialysis patients and in kidney transplant patients [Kidney Disease: Improving Global Outcomes (KDIGO), 2008] when compared with the general population (Table 6). HCV chronic infection increases the risk of renal disease and results in significant morbidity and mortality, in both dialysis and kidney transplant patients [KDIGO, 2008]. This negative impact evidences the need of regular screening, fibrosis evaluation and antiviral treatment, however, in patients with advanced renal dysfunction treatment options are currently limited [Pol et al. 2016].
Phase I studies demonstrated that <1% of GZR and EBR have renal elimination. A phase I trial also demonstrated that dose adjustments of GZR or EBR are not required in the setting of non-dialysis-dependent CKD 4/5 and dialysis-dependent CKD 5 [Yeh et al. 2014]. The C Surfer (
A total of 224 patients were randomized in a double-blind, placebo-controlled study to receive EBR and GZR [immediate treatment group (ITG), n = 111] or placebo [deferred treatment group (DTG), n = 113], allowing blinded comparison of AEs; 11 treated patients were assigned to the intensive PK arm. After 4 weeks of follow up (study week 16), patients in DTG started GZR/EBR.
Overall, 76% were hemodialysis-dependent, 52% had HCV GT1a infection, 80% were HCV treatment naive, 6% were cirrhotic and 46% were African American. Of the 122 patients receiving GZR and EBR, 6 were excluded from the primary efficacy analysis for nonvirologic reasons. SVR12 in ITG/intensive PK arms was 99% (115/116), with one relapse 12 weeks after the end of treatment. None of the patients in the ITG/intensive PK and 4% in DTG discontinued due to an adverse event. Most common adverse events were headache, nausea and fatigue, occurring at similar frequencies in patients receiving active and placebo drugs.
Thus, once-daily GZR/EBR for 12 weeks was highly effective with a low rate of adverse events in HCV GT1-infected patients with stage 4/5 CKD.
There is still an issue regarding patients with stage 4–5 CKD who are candidates to renal transplantation and the timing of antiviral therapy before or after transplantation: we assume, at least in Europe, that HCV treatment and cure should be considered before transplantation, given the usual unpredictable time of renal replacement, the higher risks of vascular, metabolic and tumorous disease in HCV-infected dialysis patients compared to non-infected dialysis patients, and the risk of drug–drug interaction with calcineurin inhibitors.
C Edge CO-STAR in persons who inject drugs receiving opioid agonist therapy
Injection drug use is the major risk factor for HCV transmission in many settings. Access therapy in persons who inject drugs (PWIDs) remains limited despite meta-analysis which have clearly indicated that safety and efficacy of PR were similar in PWID and non-PWID population (Table 6) [Aspinall et al. 2013; Zanini et al. 2010]. However, in these patients, the HCV reinfection risk is higher than in non-PWID patients, estimated around 2.4% in 2010 [Aspinall et al. 2013] and recently reported at 10.67% at 5 years of follow up in PWID achieving SVR [Simmons et al. 2016].
The efficacy of GZR/EBR has been nicely evaluated in a phase III trial [Dore et al. 2015]. A total of 301 of PWID receiving opioid agonist therapy (OAT; methadone in 79% or buprenorphine in 21%) were randomized (2:1) in the C-EDGE CO-STAR, a double-blind, placebo-controlled study, to an ITG or a DTG. The patient characteristics were as follows: mean age 47 years, 76% male, 12% Black, 76% GT1a, 21% cirrhotic and 7% HIV coinfected. The ITG received GZR/EBR for 12 weeks while the DTG received placebo for 12 weeks, followed by 12 weeks of open-label GZR/EBR.
Noteworthy, the use of nonprescribed drugs was monitored by urine drug screening, but was not exclusionary to study participation. Medication adherence was high in both groups.
In the ITG, 99% (199/201) completed 12 weeks of treatment, despite 79% having evidence of drug use (amphetamines 16%, benzodiazepines 39%, cannabinoids 40%, cocaine 19% and opioids 41%) during treatment. In the ITG, in modified intention-to-treat, SVR12 was achieved in 95.5% (189/198) overall: 96.1%, 96.6%, 100% and 60% in HCV GT1a, GT1b, GT4 and GT6 patients, respectively, although the numbers of GT4 (11) and GT6 (5) patients were limited. A total of 12 patients did not achieve SVR12 (virological failures in seven, discontinuations in two, missed visits in three). All cases of virological failure (4/201, 2%) were detected following the completion of therapy. Five patients had HCV reinfection after achieving SVR12. Comparing the ITG and DTG, ⩾1 adverse event was reported by 83% in both groups. Both groups reported serious adverse events of 4% including one death in the deferred treatment group while on placebo. Drug-related adverse events were reported by 41% of the ITG versus 34% of the DTG. In the overall population the most common adverse events included fatigue (20%), headache (15%), nausea (12%) and diarrhea (12%). There were no ALT/AST elevations greater than five times the ULN after normalization while on therapy.
In summary, these data indicate that GZR/EBR is safe and highly effective in patients with chronic HCV GT1, GT4 or GT6 receiving OAT, and supports enhanced efforts to address barriers to HCV treatment access for PWID.
Safety
In all of these studies, the GZR/EBR combination with or without RBV was generally well tolerated and has been detailed for some studies (see above). Common adverse events (around 56% of patients) were fatigue, headache and nausea, and they were mild to moderate in intensity. Serious adverse events occurred in around 3% but usually no patients discontinued due to adverse events and no deaths occurred. The incidence of drug-related adverse events, bilirubin elevations or hemoglobin decreases was higher in the regimens containing RBV compared with those without RBV.
RASs
The HCV RNA sequences from patients prior to treatment and at virological failure were examined for potential RASs. Among the NS3 loci associated with resistance to GZR, amino acid substitutions were observed at positions 56 and 168 in 6% and <1% of patients at baseline, respectively, based on population sequencing. All patients with amino acid substitutions at positions 56 and 168 at baseline achieved SVR. High-level GZR-resistant variants were not detected at baseline in any patients. Q80K and S122A/G/R have been associated with reduced efficacy in clinical studies with simeprevir. Baseline variants at positions Q80 and S122 were detected in 24% and 11% of patients, respectively. All patients who had these baseline variants at Q80 and S122 achieved SVR12 with FDC ± R. Among the NS5A loci associated with resistance to EBR, Q30H/L/R in GT1a or R30Q/H in GT1b, or Y93H/N/F were detected in 7% of patients at baseline. Even though variants at positions 30 and 93 have been shown to cause significant potency loss (100- to 2000-fold) to EBR in vitro, most patients (7/8 and 4/7) with baseline variants at positions 30 and 93, respectively, achieved SVR12. RASs for NS3 or NS5A were detected in most patients (7/12) who experienced virological failure. The most prevalent RASs associated with virological failure were NS3:Y56H, A156T and D168A/N, and NS5A:Q30R/H and Y93H/N. In the label of the FDC GZR/EBR, testing RASs in GT1a is mandatory prior to initiation of treatment with Zepatier to determine dosage regimen and duration and the ‘significant’ NS5A resistance-associated polymorphisms are at amino acid positions 28, 30, 31 or 93.
Final FDA recommendations
GZR/EBR FDC with or without RBV is indicated in HCV GT1 and GT4 infected patients but is contraindicated in patients with moderate or severe hepatic impairment (CP-B or CP-C).
Dosage regimens and durations for GZR/EBR are summarized in Table 7.
GZR/EBR: initial US approval 2016.
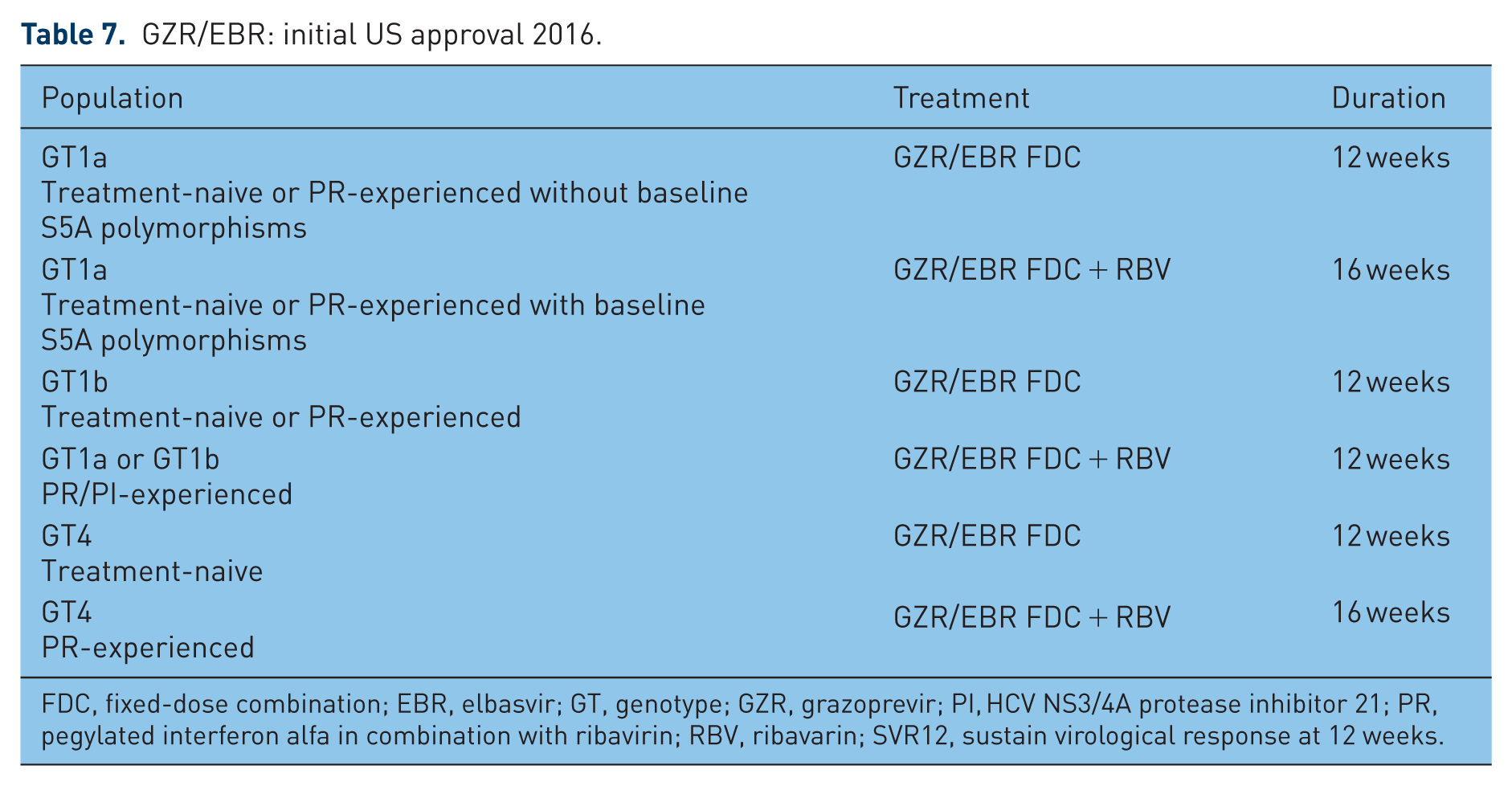
FDC, fixed-dose combination; EBR, elbasvir; GT, genotype; GZR, grazoprevir; PI, HCV NS3/4A protease inhibitor 21; PR, pegylated interferon alfa in combination with ribavirin; RBV, ribavarin; SVR12, sustain virological response at 12 weeks.
Conclusion
The low rates of adverse events, once-daily administration, and suitability for use in different patients populations which have been explored in phase III studies (naive or experienced, with or without cirrhosis, HIV coinfected also receiving antiretroviral therapy, patients with hemophilia or hemoglobin diseases, patients under opiate substitution therapy as well as patients with renal failure) suggest that GZR/EBR may represent a highly effective treatment option for all these patients infected by GT1, GT4 and GT6. The current recommendations are as follows: FDC 12 weeks without ribavirin in treatment naive and experienced patients infected by GT1a without baseline NS5A polymorphism, GT1b, naive patients infected by GT4; FDC 12 weeks with ribavirin in protease inhibitors/PR-experienced patients infected by GT1a/GT1b and 16 weeks in GT4-infected PR-experienced patients. These different schemes, the potential of DDI, the absence of pangenotypic efficacy, the need for baseline evaluation of RASs in GT1a-infected patients as well as putative hepatotoxicity of protease inhibitor in ‘severe’ cirrhosis may however limit the prescription of the FDC GZR/EBR in a minority of clinical situations.
Footnotes
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Stanislas Pol is a speaker for GSK, BMS, Boehringer Ingelheim, Janssen Gilead, Roche, MSD, Sanofi, Novartis, Vertex and Abbvie, has received grants from BMS, Gilead, Roche and MSD and is a board member of BMS, Boehringer Ingelheim, Janssen, Gilead, Roche, MSD, Sanofi, Novartis, Vertex and Abbvie.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.