
Abstract
Background:
The acute respiratory distress syndrome (ARDS) network low tidal-volume study comparing tidal volumes of 12 ml/kg versus 6 ml/kg was published in 2000. The study was stopped early as data revealed a 22% relative reduction in mortality rate when using 6 ml/kg tidal volume. The current generation of critical care ventilators allows the tidal volume to be set during volume-targeted, assist/control (volume A/C); however, some ventilators include options that may prevent the tidal volume from being controlled. The purpose of this bench study was to evaluate the delivered tidal volume, when these options are active, in a spontaneously breathing lung model using an electronic breathing simulator.
Methods:
Four ventilators were evaluated: CareFusion AVEA (AVEA), Dräger Evita® XL (Evita XL), Covidien Puritan Bennett® 840TM (PB 840), and Maquet SERVO-i (SERVO-i). Each ventilator was connected to the Hans Rudolph Electronic Breathing Simulator at an amplitude of 0 cm H2O and then 10 cm H2O. All four ventilators were set to deliver volume A/C, tidal volume 400 ml, respiratory rate 20 bpm, positive end-expiratory pressure 5 cm H2O, peak flowrate 60 L/min. The displayed tidal volume was recorded for each ventilator at the above settings with additional options OFF and then ON.
Results:
The AVEA has two options in volume A/C: demand breaths and V-sync. When activated, these options allow the patient to exceed the set tidal volume. When using the Evita XL, the option AutoFlow can be turned ON or OFF, and when this option is ON, the tidal volume may vary. The PB 840 does not have any additional options that affect volume delivery, and it maintains the set tidal volume regardless of patient effort. The SERVO-i’s demand valve allows additional flow if the patient’s inspiratory flowrate exceeds the set flowrate, increasing the delivered tidal volume; this option can be turned OFF with the latest software upgrade.
Conclusions:
Modern ventilators have an increasing number of optional settings. These settings may increase the delivered tidal volume and disrupt a low tidal-volume strategy. Recognizing how each setting within a mode affects the type of breath delivered is critical when caring for ventilator-dependent patients.
Introduction
The late 1990s brought a sweeping revolution to the world of mechanical ventilation and the treatment of patients diagnosed with acute respiratory distress syndrome (ARDS). The catalyst for this revolution was the ARDS network (ARDSNet) low tidal-volume strategy study. From 1996 to 1999, the study enrolled 861 patients and compared tidal volumes of 12 ml/kg of predicted body weight (PBW) with 6 ml/kg PBW. The study was stopped early as data revealed a positive association between tidal volumes of 6 ml/kg PBW and a reduction in mortality. At the trial’s conclusion, a 22% relative reduction in mortality rate was observed, and practitioners recognized that they had to limit the tidal volume delivered to patients with ARDS [ARDSNet, 2000].
Although the recommendations from the ARDSNet low tidal-volume study do not specify a particular mode of ventilation to be used to limit delivered tidal volume, the most common mode is volume-targeted, assist/control (volume A/C). The purpose of volume A/C is to control the tidal volume, allowing airway pressure to vary as airway resistance, lung and chest wall compliance, and patient effort change. Traditionally, volume A/C has been the primary mode of ventilation used to provide a low tidal-volume strategy for patients diagnosed with ARDS.
The current generation of mechanical ventilators allows the tidal volume to be set during volume A/C. However, some ventilators include options that may prevent the tidal volume from being limited. The purpose of this bench study was to evaluate the delivered tidal volume in a spontaneously breathing lung model using an electronic breathing simulator. The electronic breathing simulator was used to simulate an increased inspiratory effort, which is frequently seen in patients being ventilated with a low tidal-volume strategy. Options on each ventilator that might affect the delivery of the set tidal volume were turned OFF and ON with the corresponding results documented.
Methods
The Hans Rudolph electronic breathing simulator (HR 1101) (Hans Rudolph, Inc., Shawnee, KS, USA) was used to simulate patient effort. It allows the user to select the following parameters that will simulate a spontaneously breathing patient, as well as a patient who is not initiating any spontaneous breaths. (a) Resistance: this parameter is used to simulate the total average resistance of the patient and airway combined. (b) Compliance: this parameter is used to simulate the total compliance of the lung and chest wall. (c) Breath rate: this controls the respiratory rate at which the HR 1101 will initiate an inspiratory effort. (d) Amplitude: the amplitude controls the maximum patient effort or peak pleural pressure: an amplitude setting of 0 cm H2O will simulate a patient with no spontaneous effort; an amplitude setting of 10 cm H2O represents a mild inspiratory effort by the patient. (e) Effort slope: this parameter sets the shape of the simulated patient’s effort: it determines how quickly the set amplitude is reached. (f) Percentage inhale: this determines the percentage of total breath that is inspiratory time. (g) Target volume: this parameter limits the spontaneous tidal volume of the simulator, once it is reached, the simulator will cycle to exhalation. (h) Load effort: this allows a custom patient effort waveform and over-rides the values selected on the slope and % inhale.
Each ventilator was connected to the HR 1101 at the following settings: resistance 15 cm H2O/L/s; compliance 20 ml/cm H2O; rate 20 bpm; slope 1; % inhale 20; target volume 3000 ml; effort slope short I:E. Amplitude was set at 0 cm H2O to simulate a patient who is not breathing spontaneously and data were gathered. Amplitude was then set at 10 cm H2O to simulate a mild inspiratory effort and data were gathered.
Four ventilators were evaluated: CareFusion Avea (AVEA), Dräger Evita® XL (Evita XL), Covidien Puritan Bennett® 840TM (PB 840), and Maquet SERVO-i (SERVO-i). Each ventilator was turned on and allowed to run for 15 min prior to measurements. Each ventilator was set to deliver volume A/C, using the mode specific to that ventilator. Trigger sensitivity was set at a minimum value, allowing no missed triggers and no auto-triggering. Alarm settings were set to the minimum or the maximum value to prevent ventilator cycling due to an alarm condition.
AVEA settings:
mode = volume A/C
tidal volume = 400 ml
respiratory rate = 20 bpm
positive end-expiratory pressure (PEEP) = 5 cm H2O
peak flowrate = 60 L/min
flow waveform = decelerating
inspiratory pause = 0 s
trigger = 1 L/min
Options evaluated:
demand breaths = OFF and then ON
V-sync = OFF and then ON
Demand breaths are available on the AVEA during volume A/C. When the demand breaths setting is in the ON position, the intra-breath demand system (IBDS) is active. IBDS provides pressure support at a minimum of PEEP + 2 cm H2O and a maximum of two times the set PEEP. This occurs once the patient’s inspiratory effort exceeds the set peak inspiratory flowrate, causing a drop in airway pressure by 2 cm H2O. The breath is terminated (cycled to exhalation) once the set tidal volume has been delivered and flow equals 25% of the peak inspiratory flowrate [CareFusion, 2015]. This algorithm allows for variability in the peak flowrate and delivered tidal volume. Therefore, demand breaths have the potential to allow larger tidal volumes, even when trying to ventilate the patient with a low tidal-volume strategy.
The AVEA has another option called V-sync that may alter the delivered tidal volume. V-sync is available in advanced settings and can allow a varying tidal volume when active in the volume A/C mode. Once V-sync is turned ON, the ventilator switches into an adaptive pressure-control breath. An initial volume-targeted test breath is delivered with a 40 ms pause. A pressure target necessary to deliver that tidal volume is then determined based upon the end inspiratory pressure from the volume test breath. On subsequent breaths, the AVEA measures the delivered tidal volume and will vary the inspiratory pressure by no more than 3 cm H2O between breaths to achieve the desired set tidal volume [CareFusion, 2015]. Even though the tidal volume and peak flowrate settings must be set, these settings no longer reflect the actual delivered volume or flowrate when V-sync is active. Instead, the tidal volume and flowrate settings, along with inspiratory pause, indirectly determine the inspiratory time when V-sync is ON.
When testing the AVEA, data were gathered at the following conditions:
demand breaths OFF and V-sync OFF: amplitude 0
demand breaths OFF and V-sync OFF: amplitude 10
demand breaths ON and V-sync OFF: amplitude 0
demand breaths ON and V-sync OFF: amplitude 10
demand breaths OFF and V-sync ON: amplitude 0
demand breaths OFF and V-sync ON: amplitude 10
Evita XL settings:
mode: continuous mandatory ventilation (CMV)
tidal volume = 400 ml
respiratory rate = 20 bpm
PEEP = 5 cm H2O
peak flowrate = 60 L/min
AutoFlow = OFF and then ON
inspiratory time = 0.5 s
trigger = 3 L/min
Option evaluated:
AutoFlow = OFF and then ON
The Evita XL offers an option, AutoFlow, which may affect delivered tidal volume. When AutoFlow is turned ON, the ventilator delivers an adaptive pressure-control breath, similar to that described for the AVEA. The ventilator measures the expiratory tidal volume and will vary the inspiratory pressure by no more than 3 cm H2O per breath, to deliver the set tidal volume [Drägerwerk, 2015]. The delivered volume will be determined by the delivered pressure, patient’s resistance and compliance, and patient’s effort. Even though a tidal volume is set, the actual tidal volume delivered to the patient may be less than, equal to, or greater than the set tidal volume.
When testing the Evita XL, data were gathered at the following conditions:
AutoFlow OFF: amplitude 0
AutoFlow OFF: amplitude 10
AutoFlow ON: amplitude 0
AutoFlow ON: amplitude 10
PB 840 settings:
mode = A/C
mandatory type = volume
tidal volume = 400 ml
respiratory rate = 20 bpm
PEEP = 5 cm H2O
peak flowrate = 60 L/min
flow waveform = decelerating
inspiratory pause = 0 s
trigger = 3 L/min
Options:
no options are available on the PB 840 during volume A/C [Covidien, 2015].
When testing the PB 840, data were gathered at the following conditions:
amplitude 0
amplitude 10
SERVO-i settings:
mode: volume control
tidal volume: 400 ml
respiratory rate: 20 bpm
PEEP = 5 cm H2O
Ti = 0.5 s
Tpause = 0 s
Trise = 0 s
trigger = 4 L/min
AutoMode = OFF
Option evaluated:
demand flow = ON
The SERVO-i allows the patient to access the demand flow if the inspiratory flowrate does not meet the patient’s inspiratory needs and the inspiratory pressure drops by 3 cm H2O; this may result in an increased tidal volume. The latest software upgrade allows access to the demand flow to be turned OFF, limiting the tidal volume to the set tidal volume [Maquet, 2015].
When testing the SERVO-i, data were gathered at the following conditions:
demand flow ON: amplitude 0
demand flow ON: amplitude 10
Tidal-volume measurement
In each condition tested, the ventilator was allowed to stabilize, and after the tidal volume had remained constant for 10 breaths, the delivered tidal volume, which was displayed on the ventilator, was recorded and used for the tidal-volume measurement. The HR 1101-measured tidal volume was not used because the purpose of this project was not to evaluate the accuracy of the displayed tidal volume on each ventilator. Rather, the purpose was to evaluate how the changes in inspiratory effort affect the delivered tidal volume on each ventilator, as this is the value the clinicians will utilize when ventilating a patient.
Results
Table 1 lists the displayed tidal volume for each ventilator during each condition.

AVEA
The displayed tidal volume on the AVEA, when evaluating the demand breaths, is listed below.
Demand breaths OFF, amplitude 0, displayed inspiratory tidal volume 400 ml.
Demand breaths OFF, amplitude 10, displayed inspiratory tidal volume 399 ml.
Demand breaths ON, amplitude 0, displayed inspiratory tidal volume 400 ml.
Demand breaths ON, amplitude 10, displayed inspiratory tidal volume 535 ml.
Figure 1 illustrates a graphic tracing during volume A/C with demand breaths turned OFF with an amplitude of 10. Figure 2 illustrates a graphic tracing during volume A/C with demand breaths turned ON with an amplitude of 10.

AVEA during volume A/C with demand breaths turned OFF and the amplitude set at 10. PEEP, positive end-expiratory pressure; volume A/C, volume-targeted, assist/control.

AVEA during volume A/C with demand breaths turned ON and the amplitude set at 10. PEEP, positive end-expiratory pressure; volume A/C, volume-targeted, assist/control.
The displayed tidal volume on the AVEA, when evaluating V-sync, is listed below.
V-sync OFF, amplitude 0, displayed inspiratory tidal volume 400 ml.
V-sync OFF, amplitude 10, displayed inspiratory tidal volume 400 ml.
V-sync ON, amplitude 0, displayed inspiratory tidal volume 400 ml.
V-sync ON, amplitude 10, displayed inspiratory tidal volume 538 ml.
Figure 3 illustrates a graphic tracing during volume A/C with V-sync turned OFF and an amplitude of 10. Figure 4 illustrates a graphic tracing during volume A/C with V-sync turned ON and an amplitude of 10.

AVEA during volume A/C with V-sync turned OFF and the amplitude set at 10. PEEP, positive end-expiratory pressure; volume A/C, volume-targeted, assist/control.

AVEA during volume A/C with V-sync turned ON and the amplitude set at 10. PEEP, positive end-expiratory pressure; volume A/C, volume-targeted, assist/control.
Evita XL
The displayed tidal volume on the Evita XL, when evaluating AutoFlow is listed below.
AutoFlow OFF, amplitude 0, displayed inspiratory tidal volume 400 ml.
AutoFlow OFF, amplitude 10, displayed inspiratory tidal volume 448 ml.
AutoFlow ON, amplitude 0, displayed inspiratory tidal volume 405 ml.
AutoFlow ON, amplitude 10, displayed inspiratory tidal volume 744 ml.
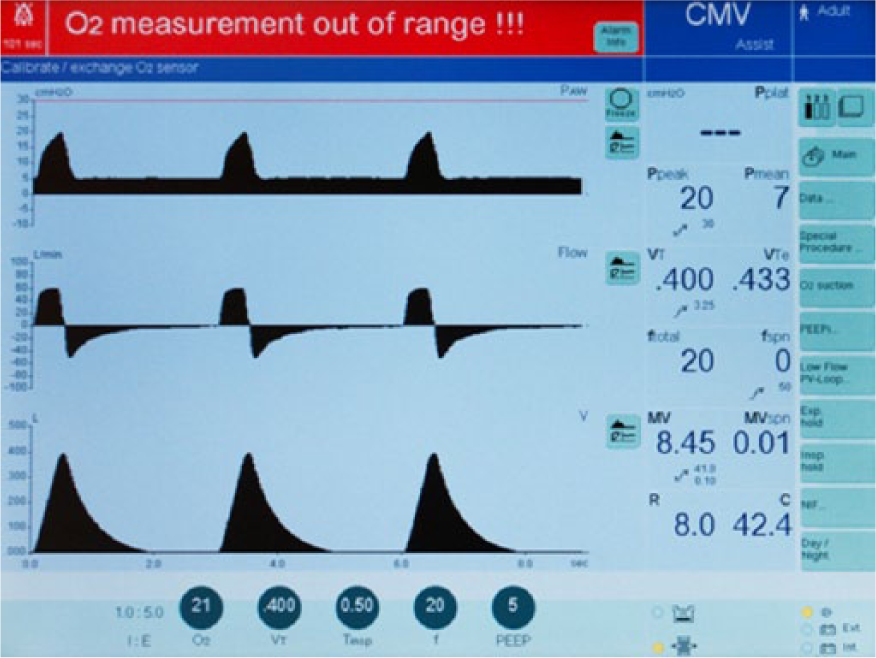
Figure 5 illustrates the Evita XL during CMV with AutoFlow OFF and amplitude set at 0. Figure 6 illustrates the Evita XL during CMV with AutoFlow OFF and amplitude set at 10. Figure 7 illustrates the Evita XL during CMV with AutoFlow ON and amplitude set at 0. Figure 8 illustrates the Evita XL during CMV with AutoFlow ON and amplitude set at 10.
Evita XL during continuous mandatory ventilation with AutoFlow OFF and the amplitude set at 0. CMV, continuous mandatory ventilation; PEEP, positive end-expiratory pressure.

Evita XL during continuous mandatory ventilation with AutoFlow OFF and the amplitude set at 10. CMV, continuous mandatory ventilation; PEEP, positive end-expiratory pressure.

Evita XL during continuous mandatory ventilation with AutoFlow ON and the amplitude set at 0. CMV, continuous mandatory ventilation; PEEP, positive end-expiratory pressure.

Evita XL during continuous mandatory ventilation with AutoFlow ON and the amplitude set at 10. CMV, continuous mandatory ventilation; PEEP, positive end-expiratory pressure.
PB 840
The displayed tidal volume on the PB 840 is listed below.
Amplitude 0, displayed exhaled tidal volume 398 ml.
Amplitude 10, displayed exhaled tidal volume 403 ml.
Figure 9 illustrates the PB 840 during volume A/C with the amplitude set at 0. Figure 10 illustrates the PB 840 during volume A/C with the amplitude set at 10.

PB 840 during volume-targeted, assist/control with the amplitude set at 0. PEEP, positive end-expiratory pressure.

PB 840 during volume-targeted, assist/control with the amplitude set at 10. PEEP, positive end-expiratory pressure.
SERVO-i
The displayed tidal volume on the SERVO-i is listed below.
Demand flow ON, amplitude 0, displayed inspiratory tidal volume 398 ml.
Demand flow ON, amplitude 10, displayed inspiratory tidal volume 975 ml.
Figure 11 illustrates the SERVO-i during volume A/C, demand flow ON with the amplitude set at 0. Figure 12 illustrates the SERVO-i during volume A/C, demand flow ON with the amplitude set at 10.

SERVO-i during volume-targeted, assist/control with demand flow ON and the amplitude set at 0. PEEP, positive end-expiratory pressure.

SERVO-i during volume-targeted, assist/control with demand flow ON and the amplitude set at 10. PEEP, positive end-expiratory pressure.
Discussion
When evaluating tidal volume, a number of patient and ventilator factors determine the actual delivered tidal volume. As our findings demonstrate, options available during volume A/C can alter the delivered tidal volume. Several other ventilator factors, including alarm limits and the ventilator manufacturer’s preprogrammed electronic components, also influence tidal-volume delivery.
When using the AVEA during volume A/C, the delivered breath type may be a volume- controlled breath, a pressure-support breath, or an adaptive pressure-control breath, depending on options selected and patient effort. The volume A/C mode can be changed drastically by having the demand breaths option in the ON position, which serves as the ON/OFF switch for the IBDS, as described in the Methods section. This allows for variability in peak flowrate and tidal volume, having the potential to eliminate attempts to implement a low tidal-volume strategy. The AVEA’s V-sync advanced setting can also generate varying tidal volumes when active in the volume A/C mode. Once V-sync is engaged, the ventilator switches into an adaptive pressure-control mode of ventilation, as described in the Methods section. It is important to note that when V-sync is turned ON, the flowrate and tidal volume have the potential to vary significantly from the set value. On the AVEA, to control tidal volume and achieve a low tidal-volume strategy, demand breaths and V-sync must be deactivated or turned OFF. Once these have been set to the OFF position, a patient will no longer be able to exceed the set tidal volume or peak flowrate. Also included as a V-sync feature is another setting called volume limit, which is available in the advanced settings. This option will cycle the breath to exhalation when a specified tidal volume is reached.
The Evita XL offers an option, AutoFlow, which may affect delivered tidal volume during CMV (volume A/C). As described in the Methods section, when AutoFlow is turned ON, the ventilator delivers an adaptive pressure-control breath. The delivered volume will be determined by the delivered pressure, patient’s resistance and compliance, and patient’s effort. Even though a tidal volume is set, the actual tidal volume delivered to the patient may be less than, equal to, or greater than the set tidal volume. To control the tidal volume when using the Evita XL, AutoFlow must be turned OFF.
The PB 840 does not have any features that can be turned OFF or ON that will alter the delivered tidal volume in volume A/C. Therefore, the set tidal volume is generally delivered, regardless of patient effort.
When the SERVO-i is in volume A/C with demand flow ON, the clinician selects the tidal volume, but this is the minimum tidal volume delivered for mandatory and assisted breaths. If the patient’s inspiratory flowrate exceeds the set flowrate and the airway pressure decreases, the patient can access the demand valve, resulting in an increased tidal volume. As such, the SERVO-i cannot limit the delivered tidal volume to the set tidal volume. Even with a mild inspiratory effort (amplitude 10), delivered tidal volume was more than twice the set tidal volume. The latest software upgrade allows access to the demand valve to be turned OFF, limiting the tidal volume to the set tidal volume.
Patient–ventilator synchrony
It is important to note that if the set tidal volume is maintained at the set flowrate during volume A/C, and if these settings do not satisfy the patient’s inspiratory effort, it has the potential to result in an increased work-of-breathing. As such, this observation emphasizes the importance of patient comfort and synchrony with any mechanical ventilator. As stated by Epstein: “Patient–ventilator asynchrony can confound attempts to deliver a lung-protective strategy” [Epstein, 2011].
When a patient’s inspiratory effort exceeds the set flowrate resulting in patient–ventilator asynchrony, this may place a considerable workload upon the patient resulting in muscle fatigue, longer duration of mechanical ventilation, and even a trend toward worse mortality [MacIntyre, 2011]. As noted by Branson, patient–ventilator asynchrony is associated with an increased number of ventilator days, an increase in the number of days in the intensive care unit, and an increase in mortality [Branson, 2013].
As noted by Yoshida and colleagues spontaneous breathing may result in an increased transpulmonary pressure, which may worsen lung injury [Yoshida et al. 2013; Akoumianaki et al. 2014]. One would expect that as the patient’s inspiratory effort increases during volume A/C, the airway pressure would decrease, resulting in no change in the transpulmonary pressure. However, if patients are ventilated in volume A/C with options turned on that allow the patient’s effort to exceed the set tidal volume, without resulting in a significant reduction in alveolar pressure, the transpulmonary pressure is likely to increase; this may worsen lung injury.
During volume A/C on any ventilator, if the patient is allowed to trigger a second breath before exhaling the volume delivered on the previous breath, the tidal volume is actually double the set tidal volume; this is frequently referred to as double-triggering. The common cause of double-triggering is that the set inspiratory time is shorter than the patient’s neural inspiratory time. Double-triggering also complicates the intent of ventilating a patient with a low tidal-volume strategy.
Alarm limits
Although it was not directly evaluated in this study, it is also important to discuss ventilator alarm limits in tidal volume delivery. On most critical care ventilators, if the airway pressure reaches the high-pressure limit, the ventilator will cycle into exhalation, terminating the breath before delivering the set tidal volume. All four ventilators in this study will limit the tidal volume if the high-pressure limit is reached.
Another alarm setting commonly available on critical care ventilators is some form of a high tidal-volume alarm. On the Evita XL and PB 840, an upper mandatory tidal-volume alarm will cycle the breath to exhalation if this limit is reached. Conversely, the high expiratory tidal-volume alarm on the AVEA will only produce an audible alarm and will not limit the breath delivered to the patient.
Conclusion
Modern ventilators have options, alarms, and preprogrammed settings that impact the type of breath that is delivered to patients. Therefore, it remains the responsibility of the healthcare provider to fully understand the ventilator’s intricacies during mechanical ventilation. In addition, the ventilator’s functions and settings can cause excessive or diminished tidal volumes that can significantly affect patients ventilated with a low tidal-volume strategy. Understanding how each option and setting within a mode affects the type of breath delivered is critical as each ventilator manufacturer approaches volume A/C settings differently. Further research needs to be completed in evaluating the impact of attempting to limit tidal volumes while utilizing nonvolume-control modes of ventilation.
Options and additional settings may be difficult to detect, and as such, ventilator waveform recognition, as well as clinician familiarity with ventilator operation, are important skills to maintain. Ultimately, setting precise values for both tidal volume and flowrate is imperative to the utilization of a low tidal-volume strategy for the safety of patients in the prevention of ventilator-induced lung injury.
Footnotes
Conflict of interest statement
The authors declare no conflict of interest in preparing this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.