
Abstract
This meta-analysis was conducted to assess the consistency and strength of the relationship between polymorphism of IL-2 -330T/G and susceptibility to pulmonary tuberculosis (TB). PubMed, Web of Knowledge and CNKI were searched to find eligible studies about the relationship between IL-2 -330T/G polymorphism and susceptibility to pulmonary TB. A total of eight studies comprising 971 cases and 1519 controls were grouped together for the purpose of elucidating the relationship between polymorphism of IL-2 -330T/G and pulmonary TB susceptibility. The allele model (G vs. T: odds ratio (OR) = 1.34; 95% confidence interval (CI) 1.05–1.71, Phet = 0.001) and the recessive model (GG+GT vs. TT: OR = 1.60; 95% CI 1.08–2.38, Phet = 0.0001) showed an increased risk of development of pulmonary TB. However, the homozygous model (GG vs. TT: OR = 1.74; 95% CI 0.98–3.09, Phet = 0.0005) and the dominant model (GG vs. TT + TG: OR = 1.30; 95% CI = 0.80-2.14, Phet = 0.001) failed to show an increased incidence of pulmonary TB. When analysis was stratified by ethnicity, no obvious associations were identified in the Caucasian subgroup under all four genetic models. Additionally, heterogeneity disappeared in the analysis of Caucasian subgroup. Our combined data suggested that there was no association between IL-2 -330T/G polymorphism and pulmonary TB among Caucasians.
Introduction
Today, tuberculosis (TB) remains a worldwide public-health problem, associated with an alarming increase in morbidity and mortality. It is usually caused by Mycobacterium tuberculosis, accounting for 10.0 million incident cases and 1.6 million deaths in 2017. 1 It is estimated that one third of the world’s population is infected with M. tuberculosis, with a great number of infections remaining asymptomatic defined as having latent TB. Of those with latent TB, only 5–10% will develop active disease. 2 The pathogenesis of TB, a transmittable killer disease, is complex and incompletely characterised, which hampers attempts to develop new tests, vaccines and treatments. The pathogenesis of M. tuberculosis infection likely involves a complex interplay between environmental factors and genetic differences in both host and bacterial pathogen. 3
The innate immune response to TB is a double-edged sword, with one edge clearing infection and the other triggering tissue damage. The cytokines are protein/glycoprotein messengers of the immune system. IL-2, a pro-inflammatory cytokine produced by T cells in response to antigenic stimulation, promotes the growth and differentiation of immune cells. The IL-2 gene is located in chromosome 4q26–q27 in humans, which includes five exons and five introns. Polymorphism of IL-2 rs2069762 (–330T/G) in the promoter region of the IL-2 gene lies near an important transcription factor which is a nuclear factor of activated T cells. On the cellular level, the G allele is associated with early and sustained enhancement of IL-2 production. 4 Polymorphism of IL2 -330T/G might also affect transcription and translation of the IL-2 gene through activation of the transcription factor. 5 Recently, it was estimated that IL-2 polymorphisms are related to susceptibility to several diseases, such as chronic spontaneous urticaria 6 and Graves’ disease. 7 However, there are conflicting results regarding the impact of IL2 -330T/G polymorphism on the risk of pulmonary TB.8–10 In this meta-analysis, we aimed to estimate more precisely the relationship between polymorphism of IL-2 -330T/G and pulmonary TB by combining all related publications to date.
Methods
Publication search
PubMed, Web of Knowledge and CNKI were searched to find eligible studies, using the keywords ‘IL-2’, ‘mutation’, ‘polymorphism’, ‘T330G’, ‘tuberculosis’ and ‘pulmonary tuberculosis’. An upper date limit of 31 August 2019 was applied; no lower date limit was used. Published studies with full-text articles were included.
Data extraction
Characteristics of each study, such as year of publication, name of first author, region, ethnicity, source of the control, number of cases and controls and distribution of IL-2 -330T/G genotypes were noted.
Statistical analysis
Crude odds ratios (ORs) with 95% confidence intervals (CIs) were used to represent the risk of pulmonary TB. Data from each study were pooled using both fixed-effects and random-effects models. Heterogeneity was assessed using Cochran’s Q statistic. Egger’s linear regression test was used to inspect the potential publication bias. Statistical analysis was performed using Review Manager v5.0 (The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen) and Stata v10.0 (StataCorp, College Station, TX).
Results
Study characteristics
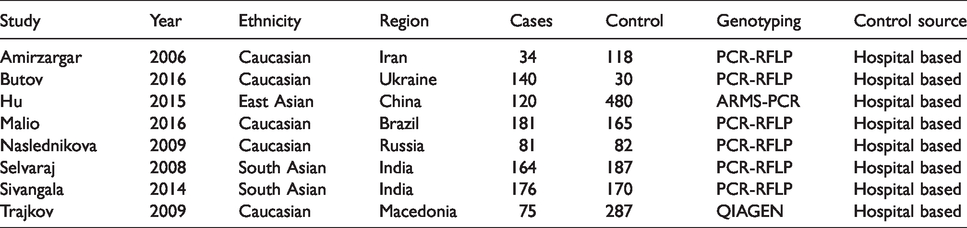
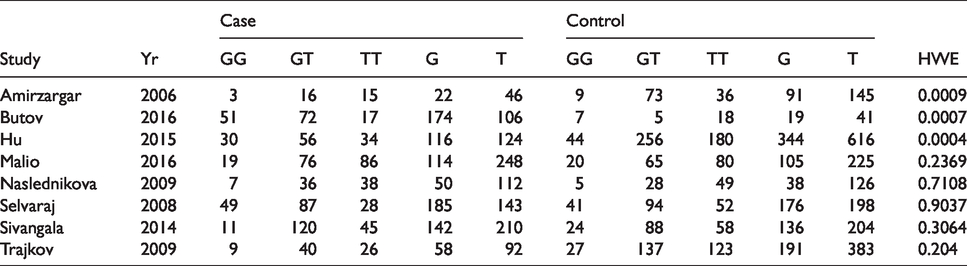
Our search strategy identified a total of 651 articles. After reading the titles and abstracts, 29 articles were selected for full reading. Finally, eight studies comprising 971 pulmonary TB cases and 1519 controls were included in this study.8–15 The characteristics of studies are shown in Table 1. Studies were done in different ethnicities: five studies were performed in Caucasians,8,9,11,12,15 one study was done in the Chinese population 10 and two studies were conducted in Indians.13,14 Genotypes and allele frequencies in each study are shown in Table 2. The frequency of homozygote TT was 29.8% in cases. We observed 51.8% heterozygous TG and 18.4% homozygous GG carriers. In control groups, the following genotypes have been identified: TT (39.2%), TG (49.1%) and GG (11.7) for XRCC1 Arg194Trp. The allele frequencies in the case and control groups were 55.7% and 63.8% for allele C.
The main characteristics of the included studies.
Distribution of IL-2-330T/G genotypes and allelic frequency.
Meta-analysis results
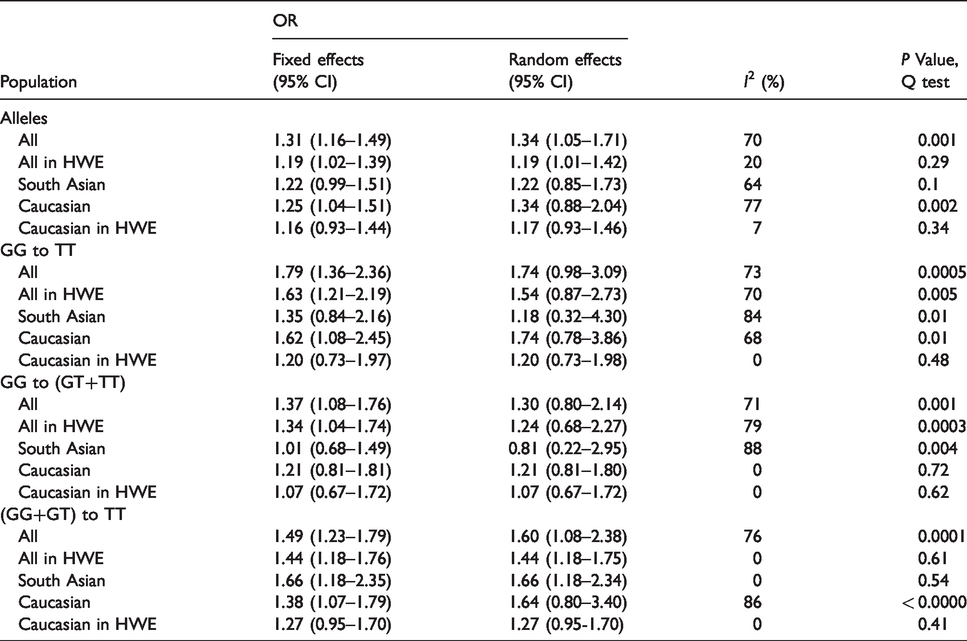
A total of eight studies comprising 971 cases and 1519 controls were grouped together for estimation of the association between polymorphism of IL-2 -330T/G and pulmonary TB. The allele model (G vs. T: OR = 1.34; 95% CI 1.05–1.71, Phet = 0.001) and the recessive model (GG+GT vs. TT: OR = 1.60; 95% CI 1.08–2.38, Phet = 0.0001) showed an increased risk of development of pulmonary TB. However, the homozygous model (GG vs. TT: OR = 1.74; 95% CI 0.98–3.09, Phet = 0.0005) and the dominant model (GG vs. TT+TG: OR = 1.30; 95% CI 0.80–2.14, Phet = 0.001) failed to find an association. Large heterogeneity was observed in allele model (I2 = 70%, P = 0.001). Subgroup analyses based on ethnicity (Indian and Caucasian) and Hardy–Weinberg equilibrium (HWE) were performed to eliminate heterogeneity. When limited to the studies in accordance with the HWE, no significant associations were observed in the Caucasian subgroup under all genetic models. Detailed results are shown in Table 3.
Odds ratios (ORs) and heterogeneity results for the genetic contrasts of IL-2 -330T/G polymorphism for pulmonary tuberculosis.
Publication bias
Publication bias was assessed using Egger’s test. No obvious publication bias was observed for the G allele versus the T allele (P = 0.314)
Discussion
Meta-analysis is the statistical procedure that integrates data from several independent studies on the same topic, and it is becoming a powerful tool to resolve discrepancies. Meta-analysis represents a quantitative analysis, synthesis and evaluation of genuine associations. 16 In this study, we have summarised all currently available data to examine the relationship between polymorphism of IL-2 -330T/G and pulmonary TB. The results showed that polymorphism of IL-2 -330T/G may not be correlated with pulmonary TB risk in Caucasians. To our knowledge, this is the first meta-analysis regarding the relationship between IL-2 -330T/G polymorphism and pulmonary TB.
Heterogeneity between studies for the overall data was evidently found in the four genetic models. It is important to speculate on the causes of heterogeneity because the heterogeneity might lead to overestimated effect sizes of the meta-analysis. In case of heterogeneity, there were wider CIs for the random-effects model than for the fixed-effects model. 17 From the forest plot in the allele model, we identified that the studies of Amirazargar et al. 8 and Butov et al. 9 might mainly contribute to heterogeneity as the outliers.
In three studies,8–10 the genotypes distributions in the control groups were not in accordance with HWE, indicating population stratification, genotyping errors or selection bias in the controls. The HWE refers to a situation in which the frequencies of genotypes should satisfy the Mendelian law. 18 The HWE must be determined for the compatibility between cases and controls because genotyping errors can cause deviations from HWE.
In the subgroup analysis of ethnicity, no obvious relationship was found in Caucasians. The effect of ethnicity on TB susceptibility was examined nearly 25 yr ago. At the cellular level, the growth ability of M. tuberculosis in macrophages varies because of the ethnicity of the donor. 19 Thus, IL-2 -330T/G polymorphism may exert different influences on TB risk among different races. In this meta-analysis, only three studies involving Caucasians were obtained. The insufficient number may give rise to limited statistical power to assess effect of race. It will be of interest in future studies to identify the association in other ethnicities.
Because of the limitations of this meta-analysis, our results should be interpreted with caution. First, among the studies included in this meta-analysis, most concerned Caucasians, and only one concerned Chinese. Data regarding Chinese were not sufficient. Second, subgroup analyses on age, sex and other factors (such as smoking and diabetes) were not performed in this study because relevant data were not available in the primary articles. Third, the number of studies was so small that we could not perform the corresponding analysis.
In conclusion, our study indicated that the IL-2 -330T/G polymorphism is not associated with pulmonary TB risk in Caucasians. Therefore, for practical reasons, more well-designed and large-scale studies are needed in future to validate or refute the results of this preliminary study.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.