
Abstract
Background
Physical restraint is widely used in intensive care units to ensure patient safety, manage agitated patients, and prevent the removal of medical equipment connected to them. However, physical restraint use is a major healthcare challenge worldwide.
Aim
This study aimed to explore nurses' experiences of the challenges of physical restraint use in intensive care units.
Methods
This qualitative study was conducted in 2018–2019. Twenty critical care nurses were purposively recruited from the intensive care units of four hospitals in Tehran, Iran. Data were collected via in-depth semi-structured interviews, concurrently analyzed via Graneheim and Lundman's conventional content analysis approach, and managed via MAXQDA software (v. 10.0).
Findings
Three main themes were identified (i) organizational barriers to effective physical restraint use (lack of quality educations for nurses about physical restraint use, lack of standard guidelines for physical restraint use, lack of standard physical restraint equipment), (ii) ignoring patients' wholeness (their health and rights), and (iii) distress over physical restraint use (emotional and mental distress, moral conflict, and inability to find an appropriate alternative for physical restraint).
Conclusion
Critical care nurses face different organizational, ethical, and emotional challenges in using physical restraint. Healthcare managers and authorities can reduce these challenges by developing standard evidence-based guidelines, equipping hospital wards with standard equipment, implementing in-service educational programs, supervising nurses' practice, and empowering them for finding and using alternatives to physical restraint. Nurses can also reduce these challenges through careful patient assessment, using appropriate alternatives to physical restraint, and consulting with their expert colleagues.
Introduction
Agitation and delirium are common problems among patients who are hospitalized in intensive care units (ICUs). One study reported that around 74% of patients experience these problems during their ICU stay. 1 Factors such as, unwanted noises, abnormal lighting, sleep deprivation, anxiety, and stress can contribute to agitation and delirium. 2 Agitation can cause serious life-threatening complications such as endotracheal extubation, removal of catheters and wires, and falling out of bed. 3 These complications can endanger a patient's life, prolong ICU stay, and increase healthcare costs. 4
Agitation and delirium may require ICU staff to use physical restraint (PR) to prevent physical injury to the patients, to themselves, and to others. 5 PR is the application of any physical method or device on a patient's body, which cannot be easily removed, to restrict body movements. 1
International studies in different countries show that the use of PR in different countries varies from 0 to 100%.6–8 Depending on geographical location, being 87% in a USA surgical ICU, 9 76% in a Canadian General ICU, 10 and 50% in France. 11 Prevalence was generally lower in Norway ICU, being 14.36%, 12 11% in Germany General ICU, 13 and 7% in Australia. 14 Moradimajd et al. reported the prevalence of PR in general ICUs, 47.60% in Iran. 15
PR use may cause different physical and mental complications for patient. 16 Unfortunately, there are no exact statistics on the amount and type of PR in Iran. It appears that, in most cases, the hands or upper limbs are restrained, but occasionally both hands and legs. 15 A quantitative study also reported edema, bruising, pressure ulcer, and death as the physical complications of PR use. 17 Emotional complications for the patient include fear, depression, and dignity. 18
Besides patients, nurses may also experience emotional, ethical, and mental problems 19 and face negative feelings such as sadness, guilt, and pity due to PR use. 20 Nurses may decide on PR use based on the non-maleficence principle of ethical practice and in order to ensure patient safety. 8 However, PR use negatively affects patient independence and freedom and violates the ethical principle of patient autonomy. 21
Constant exposure to PR-related challenges can gradually affect nurses' physical health and emotional and mental stability, cause them job burnout and absences from work and require them to eventually leave their profession. 22 Physical, emotional, and mental problems among nurses can also affect the quality of their care, increase the rate of nursing errors, and thereby endanger patient's safety. 3
Despite the wide use of PR in ICU and its numerous consequences for patients and nurses, previous studies into PR use were mainly conducted in neurologic and psychiatric care wards. Moreover, because of their quantitative designs, most of those studies dealt mainly with some aspects of challenges in PR use.23,24 The present study was conducted to address these evidence gaps. This study aimed to explore nurses' experiences of the challenges of using PR in ICUs.
Design
This qualitative study was conducted from September 2018 to March 2019.
Participants
Participants were 20 critical care nurses who were purposively recruited from the ICUs of four hospitals in Tehran, Iran. Eligibility criteria were ICU work experience of more than three years and a bachelor's degree in nursing. To increase the diversity and representativeness of our sample, we purposefully recruited participants from four (approximately 20-bed) general ICUs in Tehran. Informed consent was signed by them. In qualitative research, generalizability is not a measure, but rather we consider theoretical data saturation. This was achieved by conducting 20 interviews.
Data collection
The first author conducted semi-structured interviews for data collection. Interviews were started with questions about participants' socio demographic and occupational characteristics. Then, broad questions about PR-related challenges were asked.
We had an interview guide with questions like: Can you please explain about care delivery in your ICU? How do you manage restless/agitated patients? Please explain your problems in care delivery to restless/agitated patients? Based on participants' responses, clarification was sought through specific questioning.
Interviews were conducted at participants' homes or workplaces depending on their preferences.
On average, the length of the interviews was 60 min (in the range of 40–90). Interviews were recorded using a digital voice recorder. Data collection was continued up to data saturation, i.e., a point at which no new data were obtained from the interviews.
Data analysis
The conventional content analysis approach proposed by Graneheim and Lundman 25 was used for data analysis. Each interview was transcribed word for word and reviewed several times to obtain a general understanding of its main ideas. Then, the transcript was read, and reviewed word for word and key words or sentences were coded. Simultaneously, generated codes were reviewed, compared, and categorized according to their similarities and differences. Categories were also compared, developed, and further categorized into themes. Data were managed through MAXQDA software (v. 10.0).
Trustworthiness
Trustworthiness was determined through Guba and Lincoln's criteria, namely credibility, dependability, confirmability, and transferability. 26 The first author, who collected the data, worked for a whole year in the study setting before data collection to gain participants' trust, better understand the study setting, and ensure credibility of the findings. Moreover, the generated codes were provided to four participants to confirm whether the study findings were congruent with their experiences. Another technique to ensure credibility was peer checking, through which two qualitative researchers and three PhD students in nursing assessed the congruence of the findings with the data. Sampling from four different hospitals also helped ensure credibility. Close collaboration among the members of the research team helped ensure dependability. Confirmability was also maintained through carefully documenting all phases of the study. Also, a clear description and word-for-word quotations of the interviews were provided to ensure transferability.
Ethical considerations
This study was approved by the Ethics Committee of Iran University of Medical Sciences, Tehran, Iran (IR.IUMS.REC.1397.495). At the beginning of the interviews, participants were informed about the aim of the study, the confidentiality of the study data, their freedom to unilaterally withdraw from the study, and their access to the study findings. Then, we asked them to read and sign the consent form if they agree to participate.
Findings
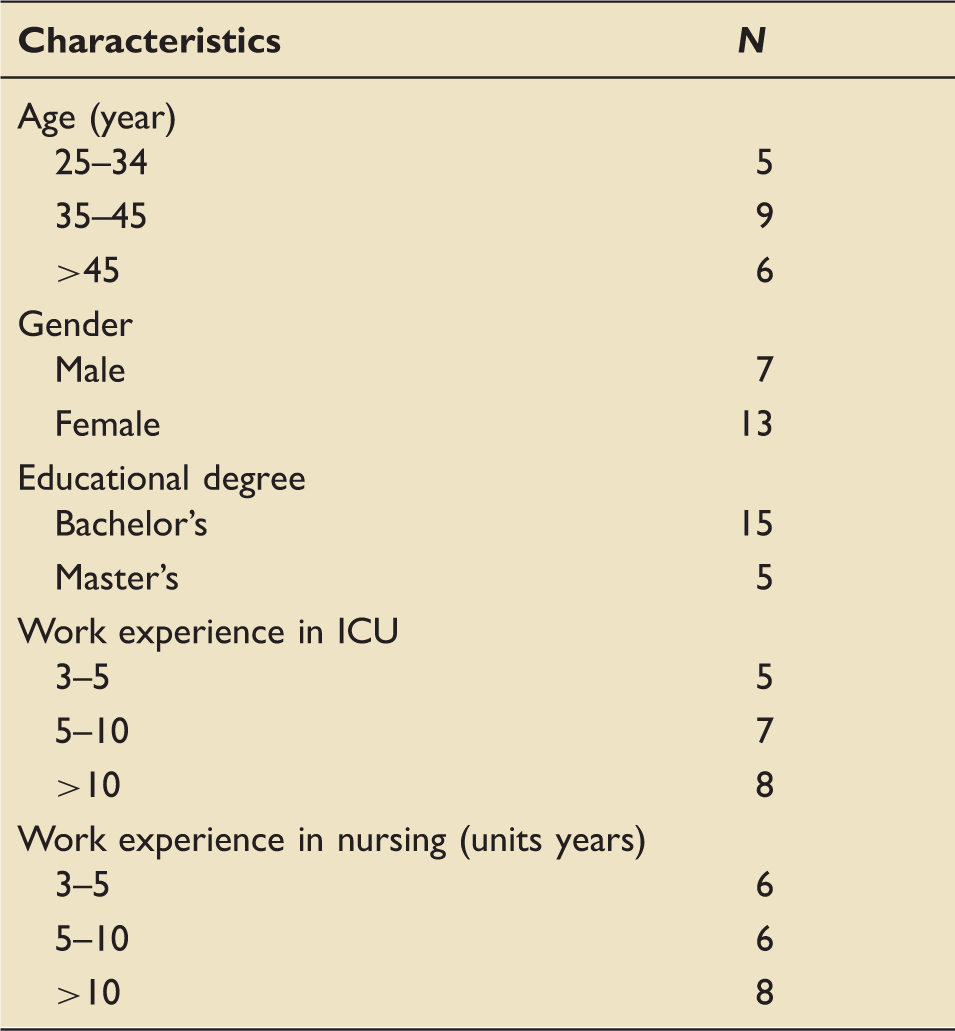
Study participants were 13 female, and 7 male critical care nurses with age mean of 35 years. About 75% of participants had a bachelor's degree and 5% a master's degree. Most nurses in Iran have a bachelor's degree. The mean ICU work experience was 16 years (range 3–30).
Participants' demographic characteristics (n = 20).
The main themes and their categories.
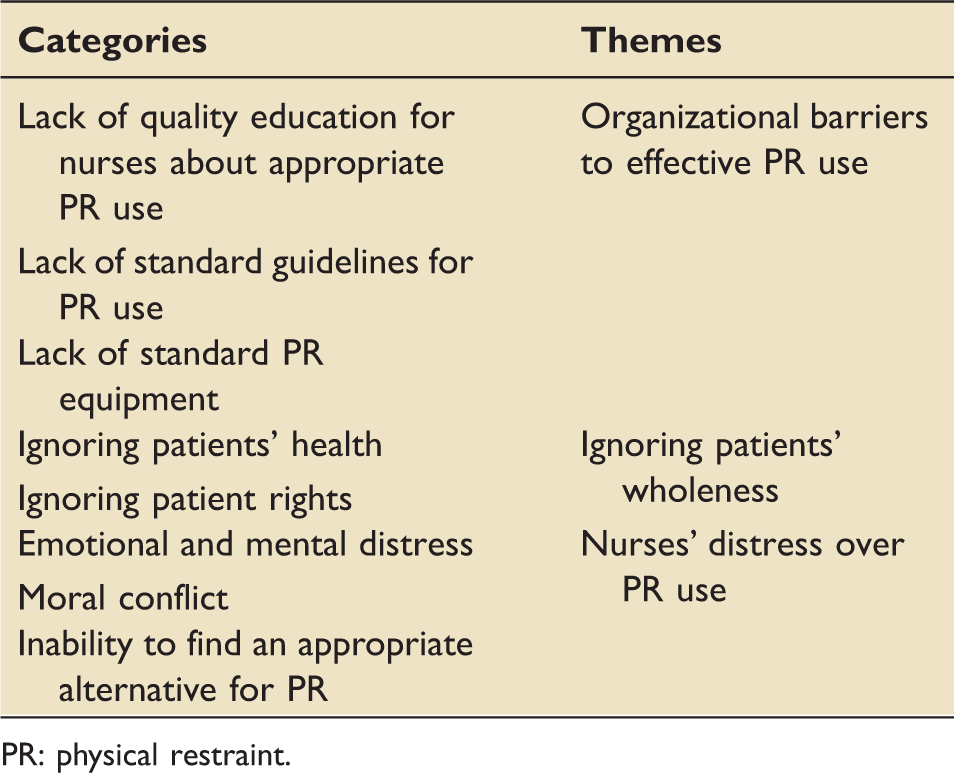
PR: physical restraint.
Organizational barriers to effective PR use
Most participants pointed to the failure of hospital managers and authorities to provide nurses with quality PR-related educations, standard PR-related guidelines, and standard PR equipment.
Lack of quality education for nurses about appropriate PR use
Our participants' experiences showed that despite the wide use of PR in ICU, critical care nurses received little if any, education about its appropriate use. Therefore, they resorted to non-standard and even inappropriate methods for PR which they had learned during their clinical practice. No education has yet been provided to us about PR. Thus, neither nurses nor physicians have accurate information about appropriate PR use, PR assessment, and PR removal. Nurses' knowledge in this area comes mainly from their clinical self-learning. (a male nurse with 21-year work experience)
Lack of standard guidelines for PR use
Most participants noted the lack of standard context-based guidelines for PR use. PR guidelines in Iran are either ambiguous and non-practical or adapted from the guidelines developed in other countries and hence, cannot be used in the context of hospital settings in Iran. On the other hand, nurses' adherence to available guidelines is limited due to the lack of supervision. There is no clear guideline in our setting and each nurse resorts to his/her own methods for PR use. There are some guidelines that have not been developed based on the context of our setting. For instance, a guideline says that PR should be applied using standard equipment and with medical prescription. However, we have neither standard equipment nor medical residents in our ICU. (a female nurse with sixteen-year work experience)
Lack of standard PR equipment
Most participants referred to the lack of standard equipment for safe PR in their settings. They highlighted that despite the wide use of PR in ICUs, managers and authorities do not greatly value the provision of standard PR equipment. Sometimes, PR use can produce positive outcomes if standard equipment is available. For instance, beds with special hand restraint and flexible equipment can be used for PR. However, in most hospitals, PR is applied using stripes rolled by ICU staff, most of which inflict wound to patients' limbs. (a female nurse with eleven-year work experience)
Ignoring patients' wholeness
Participants noted that in some cases, they had no option but to ignore patients' wholeness and use PR. The two categories of this theme included ignoring patients' health and ignoring patient rights.
Ignoring patients' health
Participants' experiences showed that they sometimes ignored patients' health and used PR due to their own interest such as heavy workload, staff shortage, and tiredness. Such use of PR helped them perform their other personal and clinical tasks more easily. Yet, inappropriate use of PR can endanger patients' physical and mental health and cause complications such as a wound, edema, shoulder dislocation, blisters, depression, aggression, fear, and anxiety. Sometimes, the ward is too busy, and the nurse is tired and bored. Sometimes, the nurse–patient ratio is low. In these cases, the nurse may use PR even for patients who don't really need it and fasten patients' hands so tightly that they cannot unfasten PR. The nurse may forget to check PR and eventually, it may inflict wound to patients. Such inappropriate use of PR can cause patients discomfort, inflict pain on them, bring them joint stiffness, prevent them from changing their position, and thereby, upset them, affect their souls, and make them aggressive or depressive. (a female nurse with fourteen-year work experience)
Ignoring patient rights
Despite their awareness of patient rights, such as the rights of selection, freedom, and comfort, our participants sometimes ignored such rights and used PR for the peace of mind and to reduce their stress over patient safety. They referred to heavy workload and staff shortage as factors behind their decision to ignore patient rights and use PR. I admit that PR makes patients unhappy and causes them discomfort. However, it prevents falls and subsequent fall-related injuries. Most of the time, the ward is too busy, and there is a limited number of staff. In such situations, I experience high levels of stress over patient fall and its subsequent troubles for me; thus, I use PR for peace of mind. In particular, at night shift I have to work alone with no colleague, and hence, I use PR even for conscious patients. (a male nurse with eight-year work experience)
Nurses' distress over PR use
The third main theme captured from the participants' experiences was related to nurses' distress over PR use. This theme included three categories, namely emotional and mental distress, moral distress, and inability to find an appropriate alternative for PR.
Emotional and mental distress
Participants noted that while using PR, they experience negative feelings such as sadness, guilt, pity, sorrow, pain, suffering, and pangs of consciousness. These feelings reduced their self-confidence, undermined their morale, and gave them feelings of despair and disability. The patient was a ten-year-old conscious and awake girl with a tracheostomy. We had to fasten her hands to prevent her from touching the tubes. She continuously cried and appealed to us to unfasten her hands. Watching that scene was torturing for me. I was very sad for her. When I looked at her, I remembered my daughter. She finally died, but her image stayed in my mind for a long time. I was on the verge of depression for her. (a female nurse with twelve-year work experience)
Moral conflict
Participants highlighted that they experienced moral distress in difficult moral situations when they needed to decide on either maintaining patient safety or patient autonomy and freedom. Moreover, neglecting the ethical principles of autonomy and freedom to prevent patients from potential damages caused them ethical conflicts. Sometimes, we need to choose between the worse and the worst. I know that fastening patients' hands and feet limits their activities and annoys them but if I don't use PR, they may remove their tubes, which necessitates re-intubation. Re-intubation, in turn, can traumatize the airways. Sometimes, patients frequently appeal to me to remove PR. Such appeal causes concerns over the accuracy of my PR-related decisions and preoccupies me for a long time. (a male nurse with seventeen-year work experience)
Inability to find an appropriate alternative for PR
Participants highlighted that PR use is unpleasant to them; yet, they have no effective alternative for ensuring patient safety and managing agitation. Moreover, using PR alternatives is not always possible due to staff shortage, equipment shortage, nurses' lack of knowledge, and their heavy workload. I really feel sad when I have to use PR, but there is no more option. For instance, the ward is too busy, and we have no staff to continuously monitor patients for possible harms. Moreover, we don't have a walkman to play music for patients. We cannot trust any other method for ensuring patient safety, except for PR.
Discussion
This study explored critical care nurses' challenging experiences of using PR in ICUs. Findings fell into the three main themes: organizational barriers to effective PR use, ignoring patients' wholeness, and distress over PR use.
Our findings showed that although nurses are the main decision-makers for PR use, they have limited knowledge about it and its complications because they do not receive PR-related education during their university education or clinical practice. Similarly, a study reported that PR-related educations are not integrated into nurses' academic curricula and in-service training programs. 27
Lack of knowledge and skills about appropriate PR use may result in its extensive use which can cause serious physical and mental complications for patients. 28 Several studies found that PR-related educational programs for critical care nurses significantly reduced PR use and its physical and mental complications.28,29
Study findings also revealed the shortage of standard and clear culturally appropriate guidelines for PR use. Our participants noted that PR-related guidelines in Iran are mostly adopted from the guidelines developed in other countries and hence, are not necessarily applicable in the healthcare settings of Iran. The first PR-related guideline was developed in 1980 by the Healthcare Financing Administration following the increasing rates of falls and physical and mental injuries caused by inappropriate PR use. 30 A study in Turkey reported that 71% of nurses in ICU had access to and used PR-related guidelines. 31
Nurses are allowed to use PR based on the patient's condition and with a physician's order. 32 The findings of Moradi in Iran indicated that PR standards are not followed completely, because the physician is not present on time and nurse is the only person who has to decide. The other reasons for non-compliance of standards are nurses' lack of knowledge and high workload. 15
The findings of Henrich in Canada indicated that inadequate resources, such as appropriate equipments can cause moral distress for ICU nurses, because of the impact on their ability to provide the best possible care. 33 This supports another finding of the present study indicating the shortage of standard PR equipment which made participants use non-standard handmade devices for PR. Non-standard PR equipment can cause irreparable physical complications and even death. 29 A study in Turkey showed that the rate of physical complications associated with the use of non-standard PR equipment was 23%. 34
In this study, ignoring the patients' wholeness means ignoring the patient's physical, mental, and legal health. Study findings also showed that in case of fatigue, heavy workload, or staff shortage, nurses might ignore patients' wholeness and freely use PR for self-interest reasons like reducing their workload. Although such use of PR may reduce nurses' workload and stress in a specific time, it may cause different undue physical and mental complications for patients such as arm fracture, thoracic wounds, pressure ulcer, anger, agitation, and depression. 35
Our findings also indicated that despite being aware of patient rights and the principles of ethical practice, nurses sometimes were forced to ignore these principles and rights and freely use PR, particularly during night shifts. Factors to with such use of PR were staff shortage, fatigue, peace of mind, as well as concerns over the removal of connections, fall from the bed, and patient safety. Similarly, previous studies reported that in case of staff shortage or heavy workload at night shifts, nurses might ignore patient rights, ethical principles, and PR complications and resort to PR to ensure patient safety. 36
We also found that while using PR, nurses may experience great emotional distress and negative feelings such as guilt, sorrow, and suffering. PR-related emotional distress can negatively affect nurses' emotional stability 19 and health and gradually cause them mental problems such as sleeplessness, headache, anxiety, fatigue, and ultimately result in long absences from work and job burnout. 24
Study findings also revealed that the compulsion to ignore patient rights and ethical principles for the sake of patient safety could cause nurses moral conflict. Protecting patients against injuries are among the most important professional roles of nurses. 30 On the other hand, PR use to ensure patient safety can negatively affect patients' freedom, welfare, and well-being and violate the principles of ethical practice. 37 The necessity to balance between professional roles and ethical practice can cause moral distress for nurses. Similarly, a study showed that balancing between patient safety through PR use and patients' freedom through not using PR can place nurses in difficult ethical situations.33,38
The other finding of the present study was nurses' inability to find an appropriate alternative for PR due to staff shortage, equipment shortage, and lack of knowledge. The findings of a study reported that 52% of nurses were unaware of PR alternatives. 39 Other studies also showed that PR alternatives are not accessible to nurses.38,40
Study limitations
Due to the sensitivity of PR use, our participants might have avoided sharing some aspects of their experiences. Of course, we attempted to manage this limitation by establishing a trustful relationship with them.
Conclusion
This study suggests that critical care nurses face different organizational, ethical, and emotional challenges in using PR. Healthcare managers and authorities can reduce these challenges through developing standard evidence-based guidelines for PR use, equipping hospital wards with standard PR equipment, implementing PR-related in-service continuing education programs, supervising nurses' PR practice, and empowering them for finding and using PR alternatives. Nurses can also reduce these challenges through careful patient assessment, considering different PR alternatives, and consulting with colleagues.
Footnotes
Acknowledgments
This article was extracted from the PhD Dissertation of the first author. We would like to thank the Research Administration of Iran University of Medical Sciences, Tehran, Iran, for financially supporting the dissertation as well as all participating nurses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.