
Abstract
Background
Critically ill children presenting to district general hospitals (DGH) are admitted to adult intensive care units (AICUs) for stabilisation prior to transfer to paediatric intensive care units (PICUs). Current training in PICU for adult intensive care physicians is only three months. This single centre retrospective case series examines the case mix of children presenting to a DGH AICU and a multidisciplinary survey assesses confidence and previous experience, highlighting continued training needs for DGH AICU staff.
Methods
all paediatric admissions to AICU and paediatric retrievals were reviewed over a 6-year period (2014-2019). Cases were identified from the Electronic Patient Record (EPR) and from data provided by the regional paediatric retrieval service. A questionnaire survey was sent to AICU doctors and nurses to assess confidence and competence in paediatric critical care.
Results
Between 2014-2019, 284 children were managed by AICU. In total 35% of cases were <1 y, 48% of cases were <2 y and 64% of cases were <5 y, and 166/284 (58%) children were retrieved. Retrieval reduced with increasing age (OR 0.49 [0.40-0.60], p < 0.0001). The survey had an 82% response rate, and highlighted that only 13% of AICU nurses and 50% of doctors had received prior PICU training.
Conclusion
At least one critically unwell child presents to the AICU each week. Assessment, stabilisation and management of critically unwell children are vital skills for DGH AICU staff, but confidence and competence are lacking. Formalised strategies are required to develop and maintain paediatric competencies for AICU doctors and nurses.
Keywords
Introduction
Since publication of the ‘Framework for the Future’ document by the Department of Health in 1997, paediatric intensive care unit (PICU) services have been centralised, so that critically ill patients aged less than 16 years are cared for in dedicated PICUs, and those 16 years and over in adult intensive care units (AICUs). 1 This centralisation of paediatric intensive care has been facilitated by specialist PICU retrieval services which provide acute care management advice and transport for critically ill children to a tertiary PICU. 2 However, critically ill children who present to district general hospitals (DGHs) are still likely to be admitted to AICUs for resuscitation, initial treatment and stabilisation until they are retrieved.3,4 The General Medical Council (GMC) of the United Kingdom officially approved paediatric intensive care medicine as a recognised subspecialty of intensive care medicine only in 2018, and while there is a mandatory three month block of paediatric intensive care medicine in the Stage 2 of intensive care medicine training, the Paediatric Intensive Care Society (PICS) guidelines further highlight the need for continuing professional development (CPD) for doctors. 5 Intercollegiate quality standards stipulate that consultants caring for critically unwell children should have up to date advanced paediatric resuscitation and life support competencies in addition to regular CPD related to the management and care for critically ill or critically injured child. In addition all staff in the multidisciplinary team providing bedside care for critically ill children should have and retain competencies in the management of critically unwell children; training and development plans should be in place detailing how competencies are achieved and maintained, through e-Learning, departmental or hospital wide training or other forms of CPD. 5 , 6
On review of the literature, an assessment of the experience, confidence, and competences in paediatrics of staff working within a DGH AICU remained an area for further study. The purposes of this study are twofold. First, this is a retrospective case series in which we review all paediatric admissions to Gloucestershire Hospitals NHS Foundation Trust AICUs over a six-year period to quantify admission frequency, age, case-mix and the level of intervention performed. Second, a multi-disciplinary team survey aims to assess staff experience, confidence and competence in paediatric critical care; a novel but important research area required to help identify and direct future training requirements to develop and maintain paediatric competencies for AICU doctors and nurses.
Methods
Study site and population
This study took place in Gloucestershire Hospitals NHS Foundation Trust. Department of Critical Care (DCC) comprises of two AICUs across two sites, totalling 18 Level 3 mixed surgical and medical intensive care beds, with over 1,700 admissions each year. In the 2018/19 financial year 24,209 children (≤16 years) attended Emergency Department (ED) and 2,415 underwent a general anaesthetic across our foundation trust. Paediatric patients can be referred to AICU from Emergency Department (ED), paediatric ward including Paediatric HDU (Paeds HDU), Operating Theatres (OT), Post Anaesthesia Care Unit (PACU), Neonatal Intensive Care (NICU).
Study design
Review of paediatric admissions
We used our electronic record keeping software, Medicus, as well as data on children transferred from our institution by the regional retrieval service (Wales & West Acute Transport for Children Service [WATCh]) to identify all children (aged <18 years) admitted to adult ICU or retrieved in the 6-year period between January 2014 to December 2019.
Survey
An electronic questionnaire was sent to all intensive care doctors (Consultants, Higher, Intermediate and Junior Specialty Trainees as well as Foundation doctors rotating through AICU) and critical care nurses (band 6 and band 7). Additional paper surveys were collected to increase response rate. The questionnaire was directed at asking about previous training experience in paediatrics/paediatric critical care and confidence in the assessment and management of critically ill children (see supplementary S1 File).
Statistics
Data were put onto a database in Microsoft Excel (Redmond, WA, US). Statistical analyses were performed using StataCorp 2017 (Stata Statistical Software 15. College Station, TX: StataCorp LLC). Chi-squared tests were used to assess the relationships between proportions. To examine linear relationships, departure from linear trend likelihood ratio test and chi-squared test for trends were performed.
Ethics
The study details were entered into the NHS Health Research Authority online decision tool and NHS REC approval was not required. 7 Consent for the questionnaire survey was assumed upon completion and submission of the questionnaire responses.
Results
During the six-year period (2014–2019), 284 critically unwell children were managed by the AICU and admitted or retrieved by regional retrieval service from Gloucestershire Royal Hospital. This represents between 35–60 referrals a year from our institution to WATCh service (Figure 1). Between 24–41 children were admitted to the Department of Critical Care (DCC) each year and between 6–22 children transferred to a tertiary PICU: this included 8 time critical transfers and 166 retrievals. Paediatric patients were admitted to AICU from the Emergency Department, Paediatric ward including Paediatric HDU, Operating Theatres, Post Anaesthesia Care Unit (Recovery) and Neonatal Intensive Care Unit.
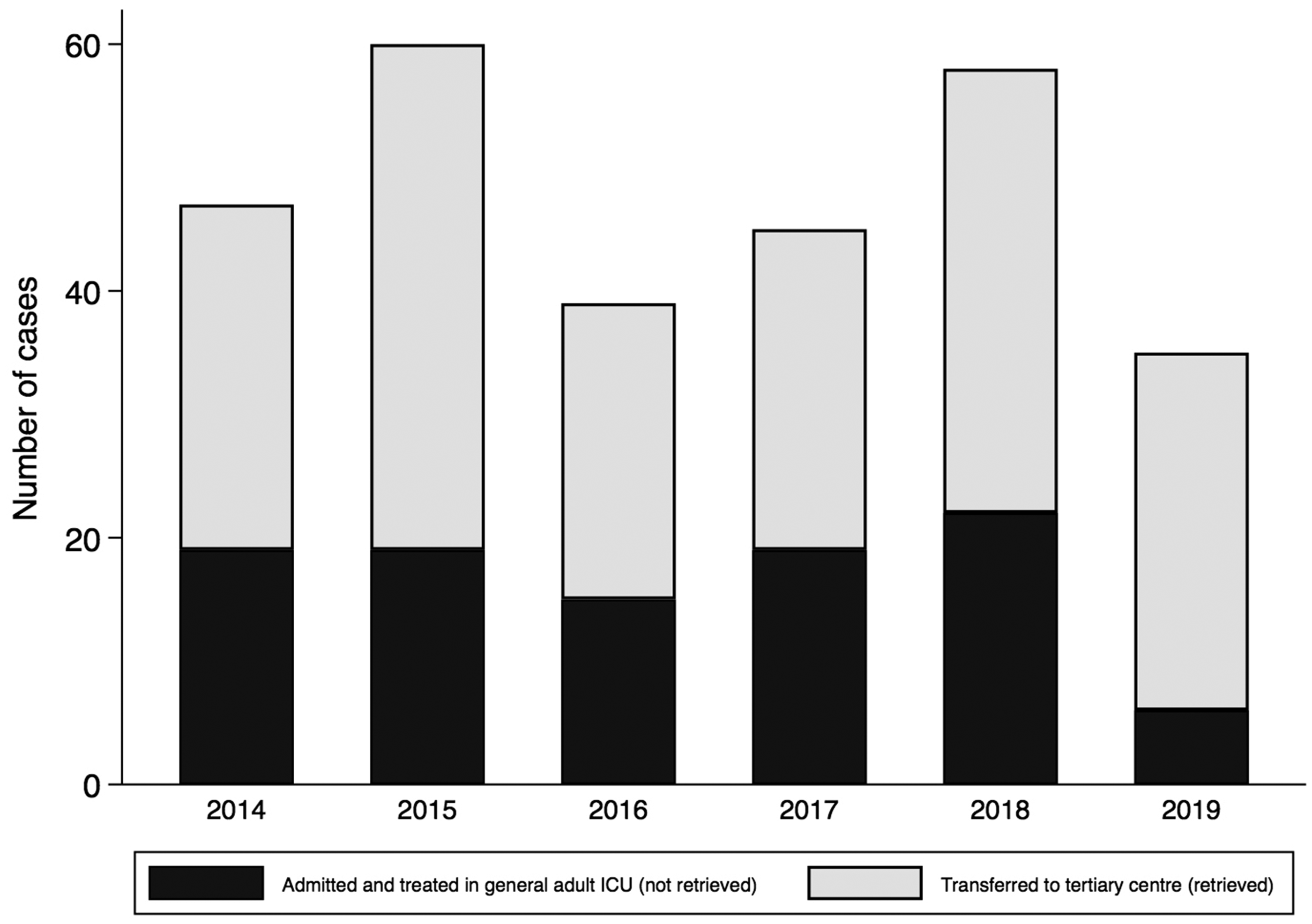
Number of critically unwell children managed by the department of critical care each year. Stratified by the number of admissions and the number transferred by WATCh.
In total, 35% of cases were <1 y, 48% of cases were <2 y and 64% of cases were <5 y (Figure 2). The five most common paediatric presentations requiring intensive care input were respiratory (31%) and neurological conditions (22%), cardio-pulmonary arrest (8%), sepsis (7%) and trauma (7%) (Figure 3). The type of presentation varied by age (p < 0.0001; Table 1).
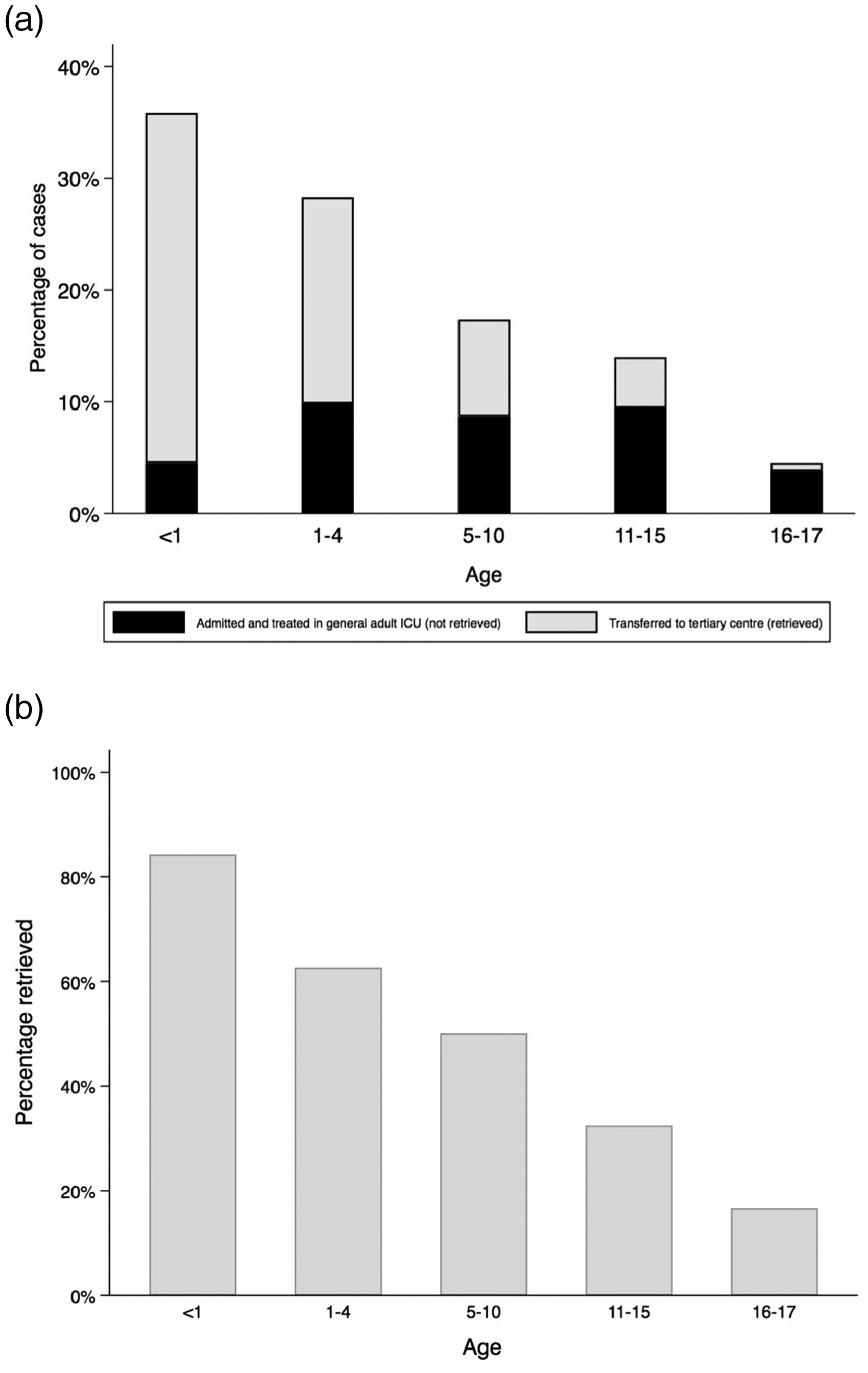
Age distribution of admissions/retrievals. a) Bars represent the percentage breakdown for each age-group from this six-year cohort, and shows the proportion of children who were retrieved to a tertiary centre (in grey) and the proportion of children who treated in the AICU. b) Bars represent the percentage of children from each age-group who were retrieved to a tertiary centre, showing that older ages were less likely to be retrieved than younger ages (OR 0.49, 95%CI 0.40-0.60, p < 0.0001).
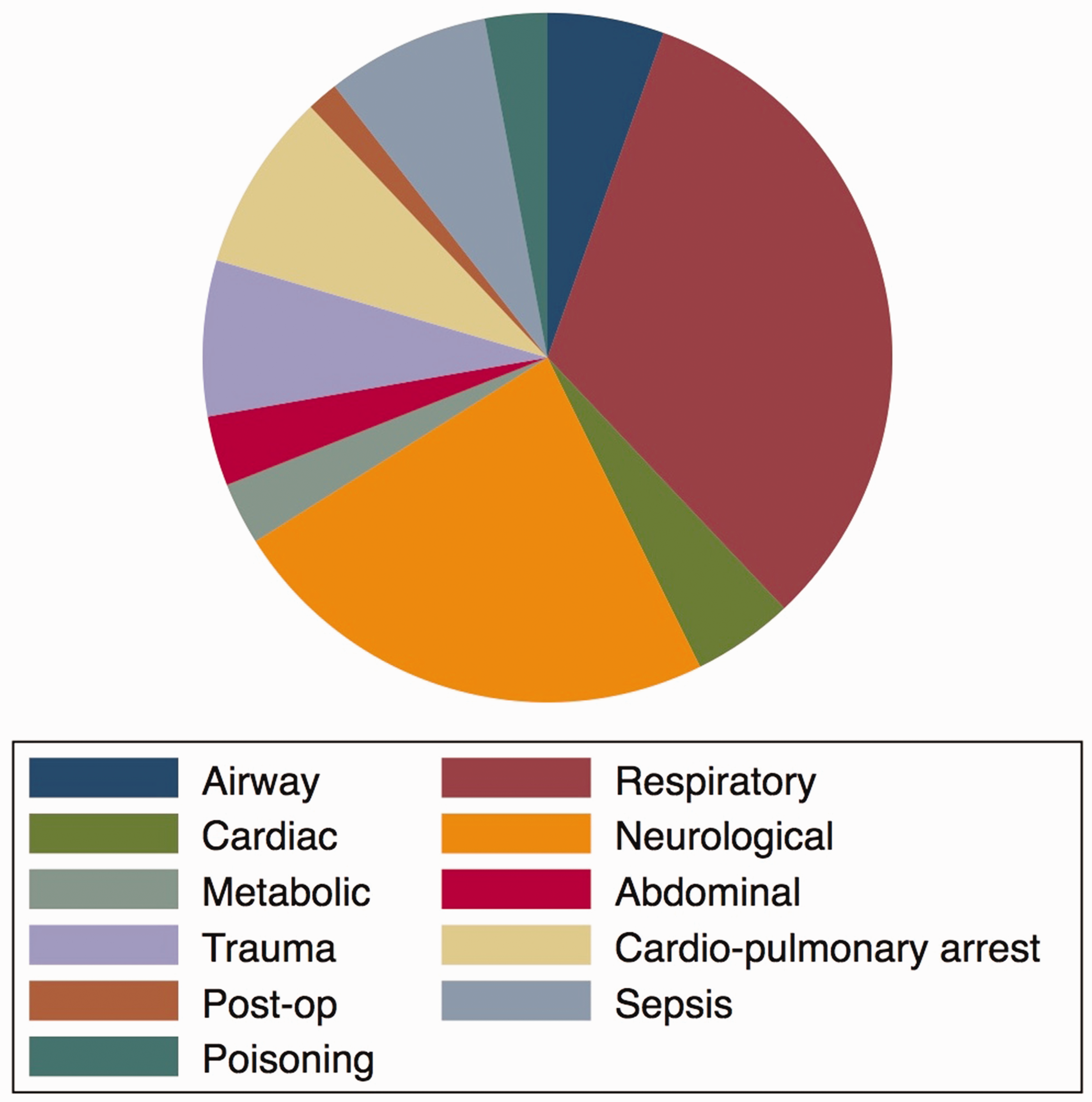
Primary reason for referral to the AICU (categorised by system).
Distribution of presentation by age.
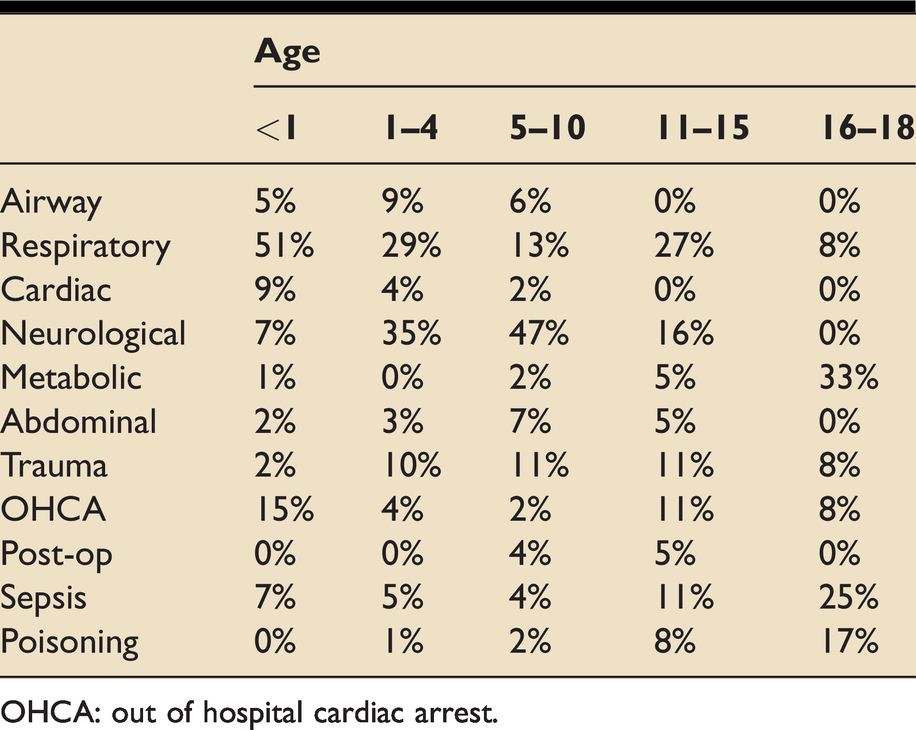
OHCA: out of hospital cardiac arrest.
Retrieval and outcome
There were 166/284 (58.5%) critically unwell children who were retrieved by WATCh. There were 63% children who were retrieved after the child had been admitted to the AICU for initial management and stabilisation, and 37% were retrieved from paediatric high dependency unit or ED (p = 0.04). Older ages were less likely to be retrieved than younger ages (OR 0.49, 95%CI 0.40–0.60, p < 0.0001; Figure 2), where 16.7% of 16–17 y were retrieved, and 87.4% of children <1 y were retrieved. In addition, retrieval rates differed according to the presentation of the illness (p < 0.0001; Figure 4). Children presenting with airway, respiratory and cardiac problems were the most likely to be transferred to a tertiary centre, whereas children with poisoning or metabolic issues and post-op patients were the least likely to be transferred.
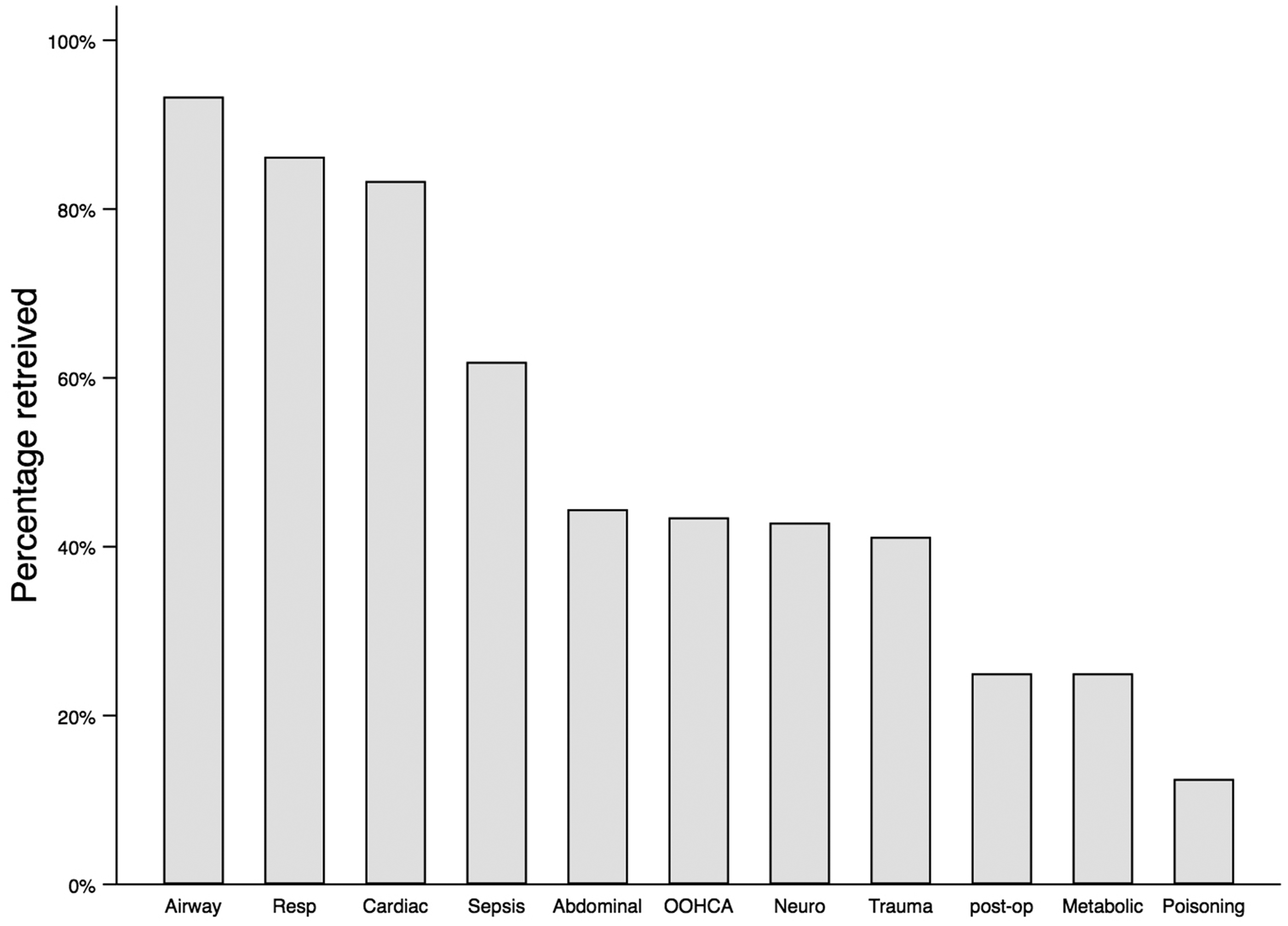
Bars represent the percentage of children retrieved according to their initial presentation. Statistical analysis using the Chi-squared test demonstrated that retrieval differed significantly according to the presentation (p < 0.0001).
In the study population, 19/284 (7%) unfortunately died. Death most commonly occurred following from cardiopulmonary arrest (12/19), then by sepsis (3/12), neurological (2/12), respiratory (1/12) and airway (1/12) problems.
Skills and support
In total 193/284 (68%) were intubated and 26/284 (9%) required vasopressors or inotropes. There were 86/284 (30%) of children who required arterial cannulation and 39/284 (14%) who required central venous access.
Questionnaire survey
The response rate for the questionnaire survey was 61/74 (82%). The breakdown of respondents by role was as follows: Band 6 nurse 23/61 (37.7%); Band 7/7+ nurse 8/61 (13.1%); Foundation doctor 2/61 (3.2%), Core trainee (anaesthetics, medicine or acute care common stem trainee) 5/61 (8.2%); Specialist registrar (anaesthetics or intensive care medicine) 7/61 (11.5%); consultant 16/61 (26.2%). Of all respondents, only 19/61 (31%) had received prior experience or training in PICU (Figure 5); 15/16 (94%) of consultants and 4/31 (13%) of nurses. Staff confidence was highest in the management of paediatric physiology, and lowest in the ongoing disease management for critically ill children (Figure 6; see supplementary table (S1 Table), which shows confidence levels with a breakdown for each staff group). Only 33/61 (55%) respondents were APLS/EPLS providers and 58/61 (95%) requested additional training in the management of critically ill children.
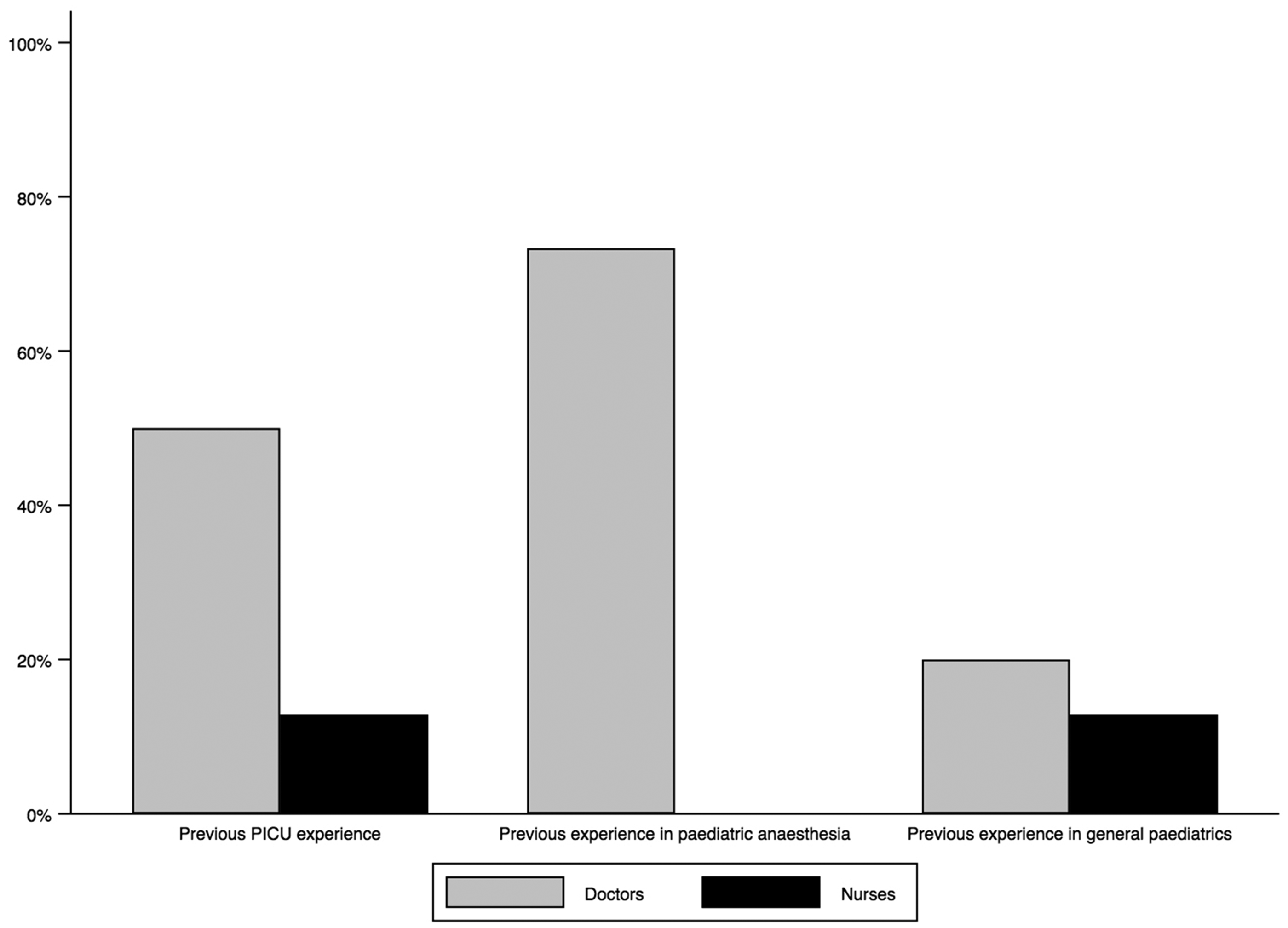
Percentage of nurses and doctors with previous paediatric experience.
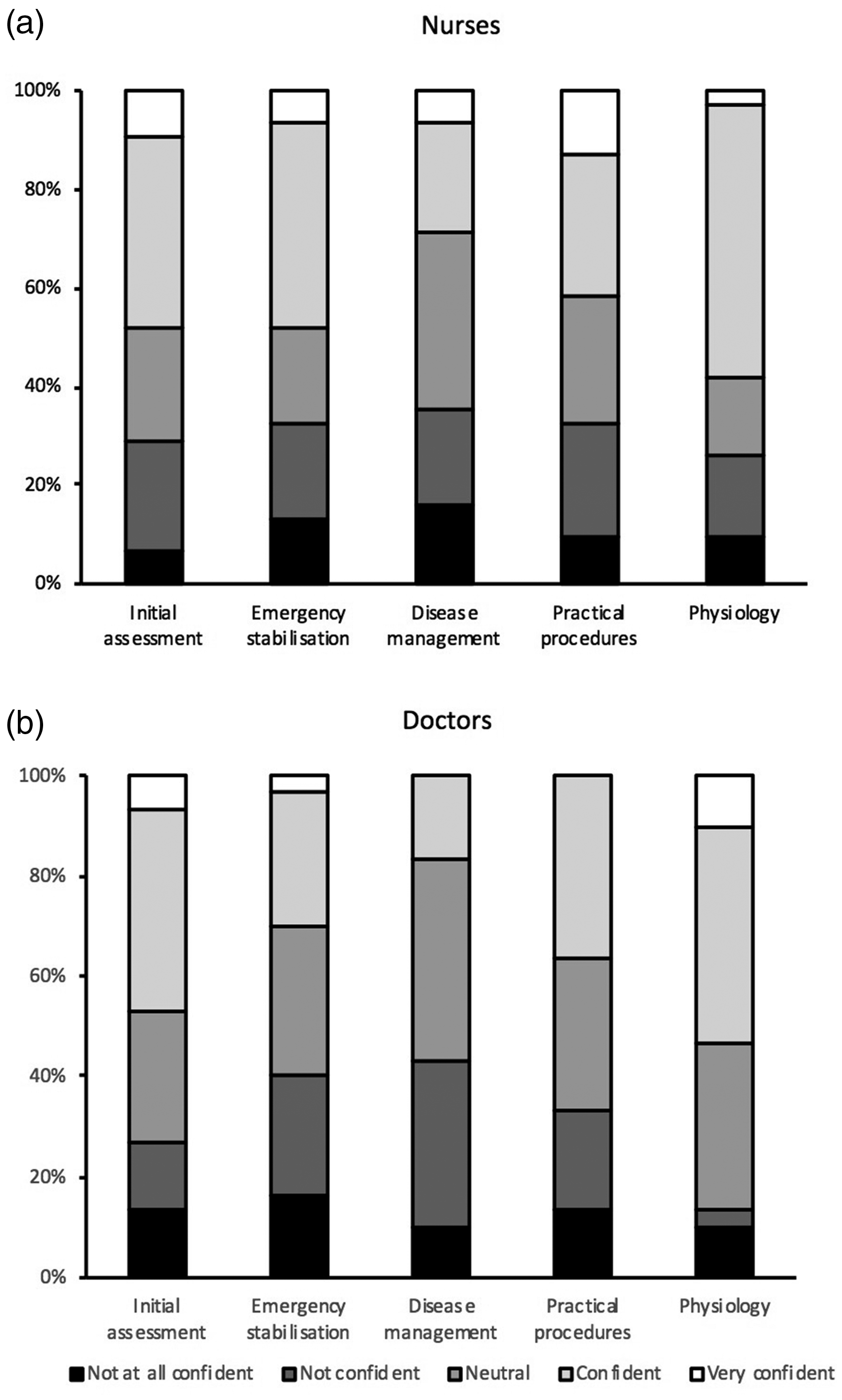
Survey responses of confidence ratings from nursing staff (a) and doctors (b) in different domains of paediatric management.
Discussion
In this single centre case series we describe the age distribution, mode of presentation and level of intervention required for paediatric critical care admission to AICU in a DGH. In addition, this is the first study to assess confidence of AICU staff in the assessment and management of critically unwell children. Over the six-year period, 284 children were managed by the AICU, of whom 58.5% were transferred or retrieved. The number of critically unwell children presenting to AICU in this DGH averaged three-four a month, meaning the AICU team is contacted for advice or to a review an unwell child at least on weekly basis as children present to ED, paediatric ward or undergo a general anaesthetic. The age distribution was heavily skewed towards very young children, with 35% of admissions less than one year of age, 48% less than two years of age, and nearly two thirds less than five; a finding similar to another DGH where 44% of paediatric admissions to the AICU were less than three years old. 3 Respiratory and neurological presentations were the most common in this study, which is reflected in findings elsewhere. 2 In our study, 8% of patients were coded as presenting with out-of-hospital cardio-pulmonary arrests (OHCA), which likely reflects a range of leading causes including sudden infant death syndrome (SIDS; ‘cot/crib death’), respiratory arrest, choking, trauma and sepsis. 6 The mortality rate of 7% of critically unwell children is similar to findings published in a previous survey (of 8%). 8
Our retrospective analysis has some limitations. A proportion of referrals to intensive care were not counted/analysed if the patient was not admitted to AICU or not retrieved by regional paediatric retrieval service. This means that time critical transfers and children who had received AICU team input (including procedures) but had been managed on the paediatric HDU, ED, PACU, paediatric ward or NICU in our hospital and not retrieved by WATCh were not included in this analysis. This means that our sample most likely reflects an under-representation of the true AICU involvement in the assessment and management of unwell children. However, there were very few missing data points, and so the findings represent an accurate picture of the paediatric admissions to this DGH AICU. As this is a single centre study, findings are not generalizable to other units. Our results are comparative to a previous single-centre AICU study in the South West, UK, noting similar age distributions at admission to the AICU. 3 The South West Audit of Critically Ill Children from 2001–2020 estimated 30–35% of admissions to DGHs over this time were transferred to PICUs. 9 This is lower than the 58.9% retrieved from our study, but highlights the importance of competencies for ongoing disease management in addition to acute stabilisation.
This analysis shows that only a small proportion of children become critically unwell and require admission to an AICU. In the 2018/19 financial year there were 24,209 paediatric ED attendances of whom 2,415 underwent a general anaesthetic, yet less than 60 children were admitted to AICU and/or retrieved by retrieval service. As expected, and demonstrated in other studies, younger and sicker children are more likely to be retrieved to specialised centres (regional PICU). 10 This is most likely due to the centralised nature of PICUs, predicted ‘short ICU stay’ by clinician for certain conditions (such as febrile convulsion) and more familiarity in managing older children who presented with conditions was commonly seen in the adult population, such as overdoses, trauma, and metabolic/diabetic emergencies. The finding that children presenting with these conditions are both older and more likely to be managed in the adult ICU, rather than exposing them to the risk of transfer, is therefore unsurprising.
Given the steady demand of paediatric admissions to our ICU during this six-year period, this study demonstrates clearly the necessity of future intensive care consultants to be able to maintain paediatric critical care skills. A national review of paediatric admissions to AICUs found that admission numbers were not decreasing since centralisation of services, our study also found no evidence of decreasing admission rates. 11
It is vital to put in place strategies to develop or retain skills required to resuscitate, stabilise and manage children on adult ICU. The challenge will be to continue providing professional development, skills acquisition and maintenance of the whole multidisciplinary team (doctors, nurses, advanced critical care practitioners, outreach and theatre nurses, physiotherapists) in the context of pandemic. The Quality Standards for the Care of Critically Ill Children published by Paediatric Intensive Care Society (PICS) in 2015 put an emphasis on all intensivists and anaesthetists with emergency paediatric responsibilities to keep up to date competencies in advanced paediatric resuscitation and airway support. 12 A report drawn up by the Department of Health and a multidisciplinary clinical expert advisory group in 2006, commonly known as the ‘Tanner Report’, recommended that DGH staff should be appropriately prepared for managing and transferring critically unwell children. 13 These are not only required for ‘time critical’ or ‘hyper-acute’ transfers, such as neurosurgical emergencies, but also assessment, management and extended care of children in a DGH ICU. 14
Maintaining competence and confidence in paediatric critical care amongst adult ICU practitioners in DGHs will be challenging. Interventions can be targeted at an individual, team/departmental and organisational/hospital level. There is an obligation on the professional to retain or acquire skills and competencies for safe paediatric practice. This can be achieved through attendance on training courses, for example PLS, APLS and transfer courses. Involvement in quality improvement is essential for sustainable change. For example a nursing paediatric competency training booklet can be introduced to ensure individual training needs are being met. The availability of secondments to paediatric wards, tertiary paediatric theatres, PICU, NICU or retrieval teams should be facilitated to ensure breadth of training. Departmental facilitation for continuing professional development (CPD) is vital and the importance of collaborative teamwork is consistently highlighted in working party reviews. 13 Simulation is a valuable training tool due the benefit of recreating clinical experience without exposing patients to the associated risks and can be organised in a variety of clinical settings (for example, in ED, Paediatric HDU or ICU) with involvement of the multi-disciplinary team. The creation of a ‘buddy system’ for junior staff to be supported by more experienced staff can be effective and can include supervised shifts with assessment in certain challenging domains such as paediatric drug-calculation. 15 The hospital/organisation has an essential role in the provision of safe facilities and equipment, in addition to helping to facilitate sufficient time to support staff training. Study leave acquisition for paediatric skill development is vital. A safe environment for paediatric admissions must be provided, to include a specialised paediatric resus bay and HDU and appropriate equipment availability, to include paediatric emergency bags and paediatric emergency trolleys. Staff should have access to support systems to assist with the psychological aspects of dealing with potentially traumatic events in managing some critically ill children.16,17 The southwest regional Paediatric Critical Care Network organise annual ‘roadshows’ that act as outreach sessions enabling learning from cases in addition to fostering cohesive regional working relationships. Dissemination of learning, particularly to infrequent clinical situations is paramount. The quarterly case review meetings have been a long-standing invaluable tool to collaboratively reflect on cases. Key learning points from such meetings can be shared more widely via departmental monthly bulletins.
These solutions however are not infallible. As demonstrated in this study, the majority of patients were less than five years of age and critically unwell, which does not reflect the age or clinical cases anaesthetised on an elective theatre paediatric list in a DGH or tertiary centre. Furthermore, there are an increasing number of single-speciality intensive care medicine (ICM) trainees, who once awarded their Certificate of Completion of Training (CCT) will commence working in DGHs. At present ICM training incorporates a three-month Paediatric Intensive Care Medicine (PICM) rotation in stage two of training, therefore for some clinicians this may be their only post-graduate experience in paediatrics prior to CCT. 18 Maintaining skills in paediatric resuscitation may become a challenge. One model may be to rely on a core group of anaesthetic or ICU consultants who would be called upon in the case of paediatric admission to adult ICU to facilitate practical procedures and resuscitation and to work in close collaboration with paediatricians and PICU services for continued management and diagnosis.
Conclusions
Despite a growing centralisation of paediatric services within tertiary centres, maintaining and developing competency in paediatric management remains relevant for the DGH adult ICU practitioner. In this retrospective case review, 24 to 41 children were admitted to adult ICU each year, of whom half were under two years of age. The survey identified that the minority of members of staff had prior paediatric experience in PICU, and that there was a strong interest in gaining further training opportunities. For many clinicians, paediatrics may constitute only three months of pre-CCT rotations, and ongoing training integrated with tertiary centres and retrieval services may help to maintain confidence and competence in the care of children. Our recommendation is that a formalised strategy should be adopted, particularly within DGHs, to maintain and develop paediatric competencies for adult ICU consultants.
Supplemental Material
sj-pdf-1-inc-10.1177_17511437211012151 - Supplemental material for Paediatric admissions to a district general hospital adult intensive care unit over a six year period: A single centre retrospective case series, with review of practitioner confidence and competence in paediatric critical care
Supplemental material, sj-pdf-1-inc-10.1177_17511437211012151 for Paediatric admissions to a district general hospital adult intensive care unit over a six year period: A single centre retrospective case series, with review of practitioner confidence and competence in paediatric critical care by Stephen A Spencer, Joanna S Gumley and Marcin Pachucki in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-2-inc-10.1177_17511437211012151 - Supplemental material for Paediatric admissions to a district general hospital adult intensive care unit over a six year period: A single centre retrospective case series, with review of practitioner confidence and competence in paediatric critical care
Supplemental material, sj-pdf-2-inc-10.1177_17511437211012151 for Paediatric admissions to a district general hospital adult intensive care unit over a six year period: A single centre retrospective case series, with review of practitioner confidence and competence in paediatric critical care by Stephen A Spencer, Joanna S Gumley and Marcin Pachucki in Journal of the Intensive Care Society
Footnotes
Acknowledgements
Thanks to all staff for participating in the questionnaire survey. This study was not funded.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.