
Abstract
Recent nursing shortages have been particularly felt in specialist areas, like Critical Care, which require higher staffing quotas; leading to increased recruitment of Newly Qualified Nurses in an area once reserved for the more experienced. This qualitative systematic review aimed to explore the experiences of Newly Qualified Nurses working in Critical Care, as their first job post-registration. A systematic search was undertaken between December 2017 and May 2018, yielding eight studies for inclusion in this review. Eligibility criteria included a qualitative design; Newly Qualified Nurses with less than two years post-registration experience, working in adult Intensive Care Units. Data were extracted and synthesised using the Thematic Synthesis approach. Five main themes emerged from the data: Intensive Care Unit Readiness; An Emotional Spectrum; Developing Relationships; The Journey to Self-Satisfaction and Intensive Care Unit Commitment. Conclusions are that an undergraduate placement in Critical Care should be facilitated where possible, consistent mentorship enhances Newly Qualified Nurse satisfaction, peer support is an important coping mechanism and opportunities for socialisation should be facilitated.
Introduction
This review examines the experiences of Newly Qualified Nurses (NQNs) working in Critical Care, an environment traditionally reserved for experienced nurses, due to the complexity of patients and specialist skills required. 1 Recent decline in the nursing workforce has been acutely felt in specialist areas, including Critical Care, with higher staffing requirements. 2 This has led to increased recruitment of NQNs in Critical Care, a phenomenon still relatively unexplored.1,3
Evidence on the experiences of NQNs transitioning from student to registered nurse in the ward setting is widely available. O’Shea and Kelly's 4 study describes NQNs experiencing significant stress, some describing physiological disturbances, including insomnia and weight loss. Rudman and Gustavsson 5 found that 50% of NQNs had experienced burnout, a psychological syndrome of exhaustion and disillusionment, due to job-related stress. 6 Kramer's 7 1974 seminal work recognised that stress may be particularly prominent amongst NQNs due to ‘Reality Shock’, where the realities of working as a qualified nurse are vastly different to expectations developed during nursing education. Confirmed by Higgins et al.’s 8 review exploring the experiences of NQNs in the UK, which found that NQNs undergo a period of role change, made particularly stressful as they encounter uncontrollable and overwhelming events; far removed from the idealised care taught in training.
O'Shea and Kelly 4 also reveal that NQNs perceive a clinical skills deficit upon qualification. Although adequately prepared for routine skills, such as dressings or suture removal, they lacked specialist skills, such as passing a nasogastric tube or suctioning. Patterson et al.'s 9 study based in the Emergency Department (ED) reflects these challenges, observing that the breadth of skills required for working in specialist areas and the rapid pace can be overwhelming for NQNs. Although set outside Critical Care, these studies allude to the challenges that NQNs face in a specialist area.
Farnell and Dawson 10 explored the perceptions of experienced registered nurses, transitioning from the ward into Critical Care. Participants identified comparisons between transitioning from student to registered nurse; they were surprised by the knowledge required to look after the critically ill, often feeling overwhelmed. King and Macleod Clark 11 explored the development of intuition skills in Critical Care, featuring nurses with varied experience. Those least experienced exhibited greater anxiety, lacking both confidence and critical thinking skills. These studies of experienced nurses cast doubt upon the suitability of this environment for NQNs. Parker et al. 12 describe the first 12–24 months post qualification as the most vulnerable time for NQNs, during which they decide whether to commit to the profession. Hence the case for increasing understanding about the NQNs experiences in Critical Care, in order to provide optimal support, ultimately to maintain patient safety, but also to reduce attrition.
Terminology surrounding Critical Care remains unstandardized; therefore, throughout this review, the terms ‘Critical Care’ and ‘Intensive Care’ are used interchangeably to describe areas solely dedicated to providing closer observation or support for single or multiple failing organ systems. 13 It does not cover other specialities such as ED or Theatres, which may also intermittently provide organ support.
Methods
Aims and objectives
This review aims to explore the experiences of NQNs beginning their career in Critical Care, with the following objectives:
Identify the experiences of NQNs working in Critical Care, as their first job post-registration. Discuss the unique challenges faced by NQNs working in Critical Care. Make recommendations to enhance support for NQNs beginning their career in Critical Care.
These informed the final review question ‘What are the experiences of Newly Qualified Nurses beginning their career in Critical Care?’ This was broken down into facets using the population, exposure, outcome framework, later underpinning the search strategy. 14
Protocol and design
A review protocol was developed including elements of the Joanna Briggs Institute (JBI) Reviewer's Manual, 14 arguably the most established for synthesising qualitative data; alongside principles from The Cochrane Collaboration Handbook 15 and supplementary guidance from The Cochrane Qualitative and Implementation Methods Group. 16 The protocol was not externally registered. Ethical approval was not required for this review, as it had been sought by the primary researcher in all original studies.
Eligibility criteria
Eligibility criteria.
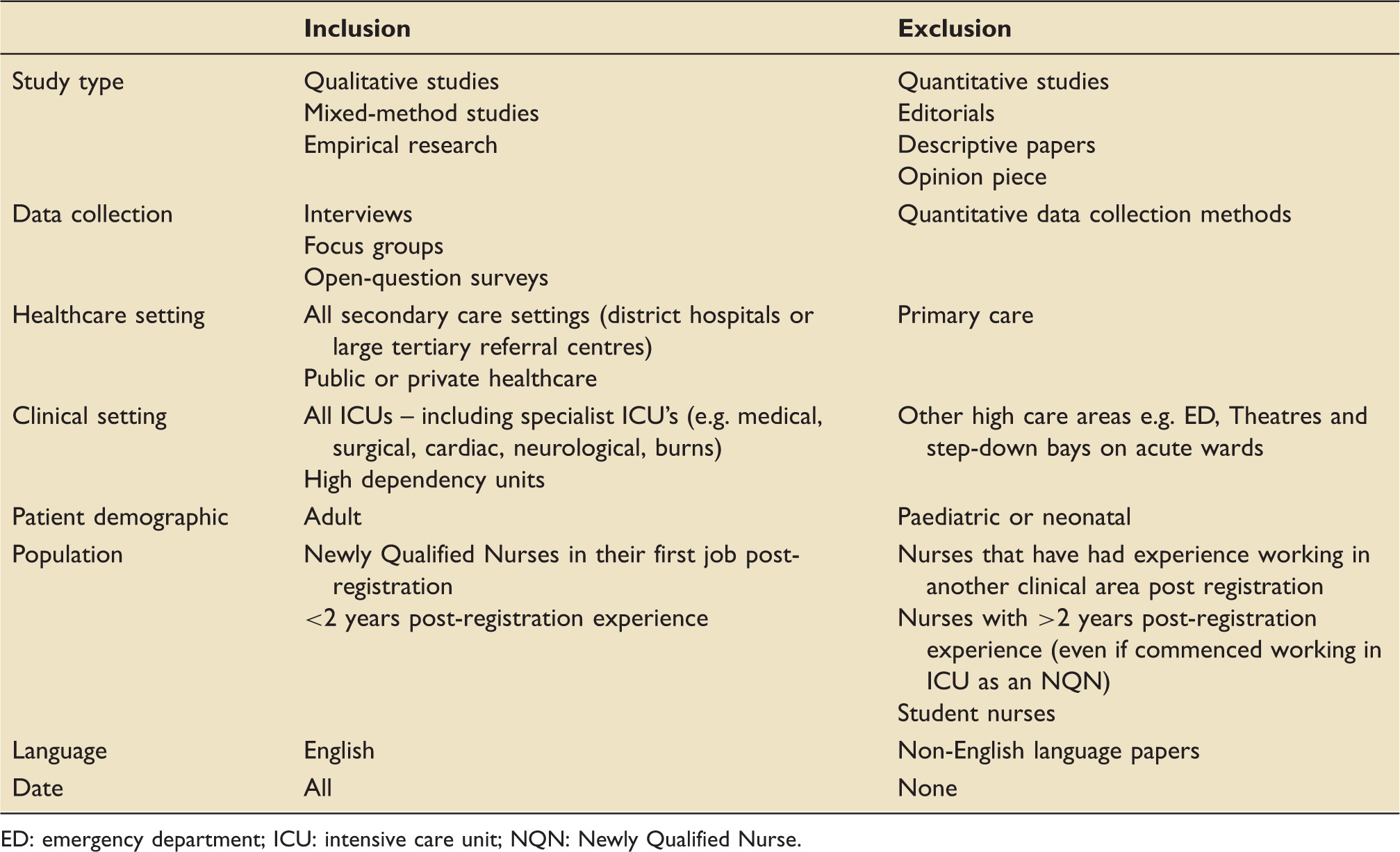
ED: emergency department; ICU: intensive care unit; NQN: Newly Qualified Nurse.
Search strategy
Search strategy.
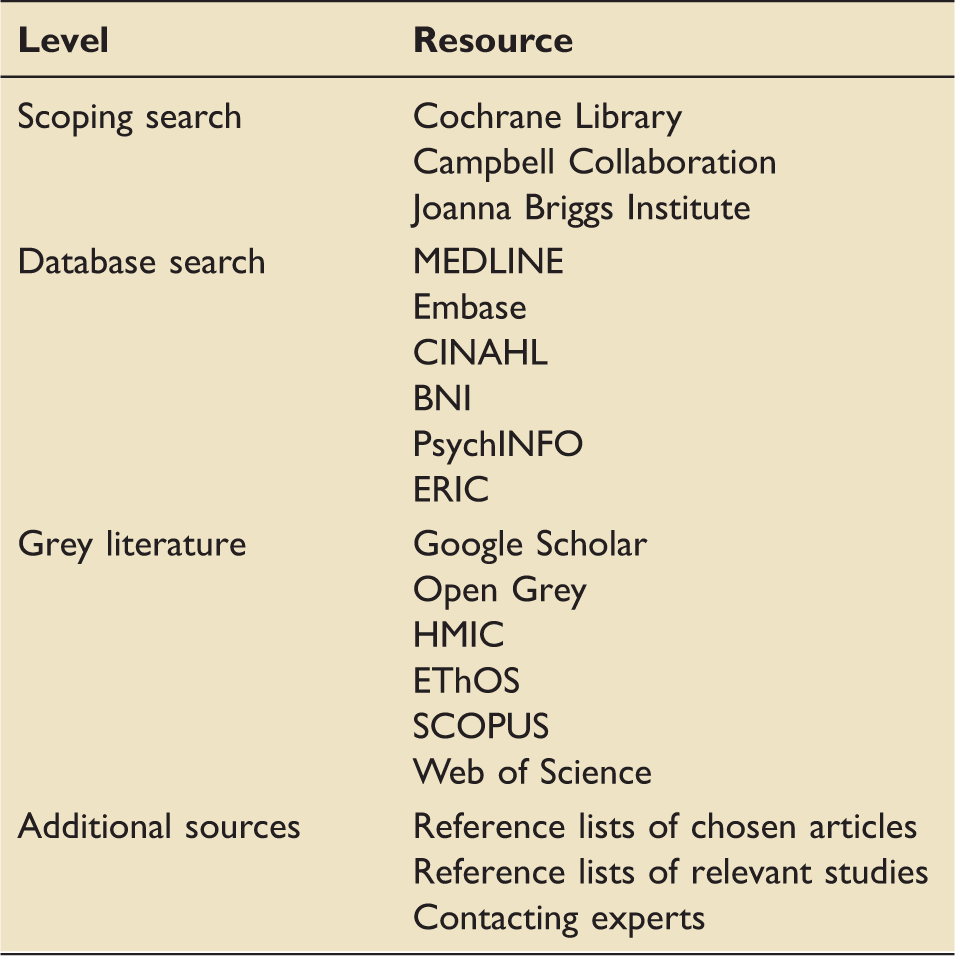
The initial search was undertaken between December 2017 and March 2018. The searches were saved and run again on each database immediately prior to data extraction in May 2018 to identify the emergence of new papers. An example search using MEDLINE can be viewed in Supplementary material online.
Critical appraisal
JBI critical appraisal checklist for qualitative research. 20
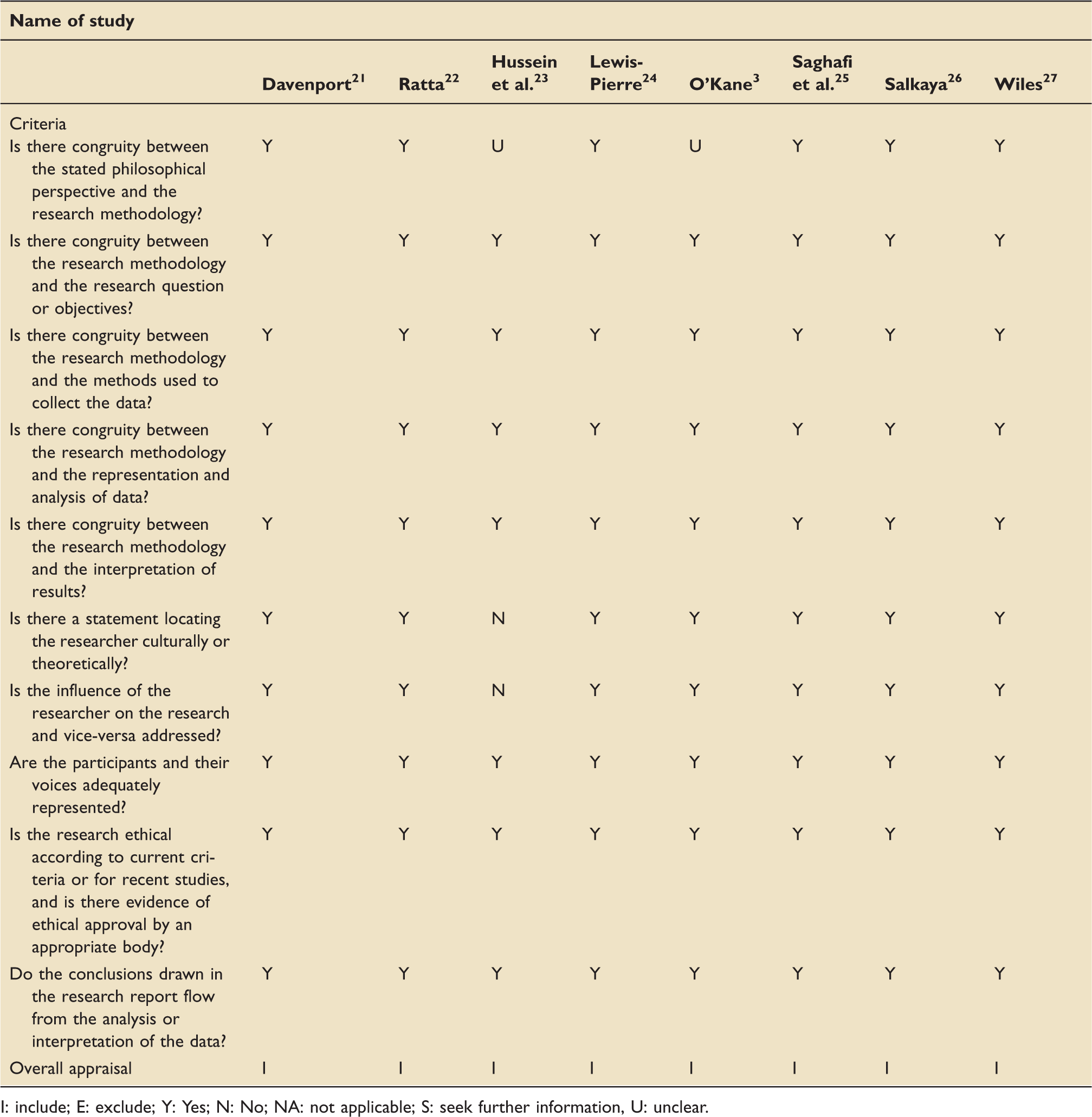
I: include; E: exclude; Y: Yes; N: No; NA: not applicable; S: seek further information, U: unclear.
Data extraction and synthesis
Data were synthesised using the three-stage ‘Thematic Synthesis’ 28 method chosen for its interpretative approach, well-suited to exploring the lived experience. 29 In stage 1, the original studies were imported into NVivo 11 Pro 30 and coded line by line. All text labelled ‘findings’ or ‘results’ was considered, but only direct participant quotes were coded to avoid including the primary reviewer's interpretations and potential researcher bias. In stage 2, codes were organised into related subject areas and assigned a descriptive theme. Stage 3 involved grouping the descriptive themes into analytical themes based upon similarities and allocating a more abstract concept heading.
Results
Search yield
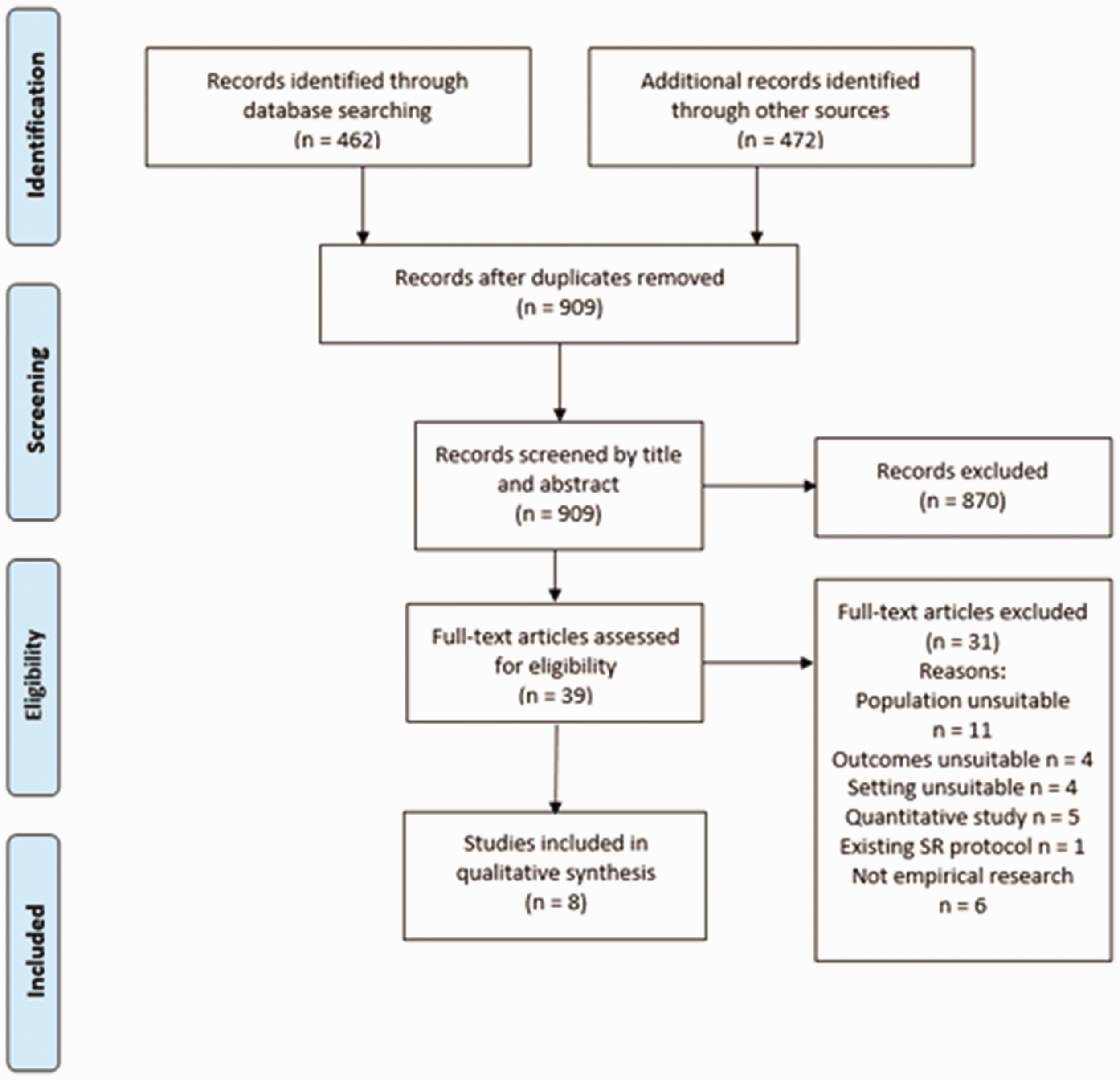
The search identified 909 studies following removal of duplicates. Once screened by title and abstract, 39 studies were screened by full text against the eligibility criteria, leaving eight studies for inclusion in the review (Figure 1).
PRISMA flow diagram.
31
Study characteristics
Included studies were based in England, 3 Australia23,25,26 and The United States.21,22,24,27 Three were multi-centre21,22,27 and five were single-centre studies.3,23–26 Studies occurred in tertiary referral centres3,21,24,25, and smaller district or private hospitals.21,22,26 Dates ranged from 2000 to 2017. Data collection included interviews, focus groups and open-question surveys. The studies totalled 118 participants. A full summary of included studies can be viewed in Supplementary material online.
Findings
Five analytical themes emerged from the data: ICU Readiness; An Emotional Spectrum; Developing Relationships; The Journey to Self-Satisfaction and ICU Commitment. Participant quotes have been allocated pseudonyms by the original researcher.
ICU readiness
‘ICU Readiness’ encompasses how prepared NQNs felt to work in Critical Care; including preparation by undergraduate education, structure of orientation, supernumerary time and challenges faced during early days.
In five studies, participants felt that undergraduate training had left them inadequately prepared for the environment.3,21,24,26,27 Common complaints were that undergraduate training provided little exposure to critically ill patients, medications required or equipment used.24,26 Consequently, some felt disadvantaged by not having an undergraduate placement in ICU.24,26 I learned medications in the nursing schools but the discussions did not include all the ICU medications such as beta-blockers and analgesics. (G4: 94)
24
If I've [sic] done a ICU placement during university I probably would have known what to expect. (Catherine: 45)
26
[During supernumerary] You don't have the skills or competencies, you couldn't really help. So you can't really be visible as part of the team. You can't really contribute on the same level. (Participant 7: 47)
3
An emotional spectrum
In all studies, participants described a range of emotions, fluctuating between positive and negative, depending on individual circumstances and events. Excitement was the most frequently discussed positive emotion, discussed in two studies.21,26 One NQN described the ‘adrenaline rush’ when trying to ‘save a life’.
21
Others were excited by the environment itself, perceiving it to be more ‘fun’ than in other areas (the ward), particularly when busy.
26
There is an excitement. It's that rush. I always like the excitement. It's the idea of trying to save them and doing all this stuff on the spur of the moment. (Susan: 126)
21
I think there's actually pressure that on you and how do I put it [pause] so yes, I'm scared at a point that you would do something wrong and that would harm the patient. (Sue: 39)
26
A patient (HDU) clinically deteriorated and [I] felt very uncomfortable, useless, dumb as I did not know what to do and the team took over (Participant 4.15)
23
The charge nurse got a bunch of us new grads to practice chest compressions. That was pretty exciting … I haven't found my place in a code [cardiac arrest] yet. I hate to say this but I'm not real good at them … I get nervous and my hands start shaking. (Kelly: 193)
21
Developing relationships
Developing relationships with service users, colleagues and peers was an important aspect of the NQNs' transition into Critical Care.
Family interactions featured in six studies.21,22,24–27 Forming bonds with families often bolstered the NQNs confidence.
21
Others lacked confidence around families, for fear of saying the wrong thing.
24
As a new graduate, we are unsure of how to talk and communicate … Especially when their loved one is critically ill and not doing well, I don't know what to say. (G7: 92)
24
I held his hand and I talked to him by his first name. He's confused at times and I'm trying to make sure he knows where he is and who he is because he doesn't always know that … The patient's comfort, that he sleeps good when I'm there, is important and I'm proud of that. (Carmen: 164)
21
I felt like I had a different preceptor [mentor] every day … They never asked me what I felt comfortable doing. I had such a conflict about techniques. One would say you should really do it this way. Another would want me to do the same thing another way. I was so overwhelmed. (Karen: 158)
21
There were a lot of other GNPs [graduate nurse programme] starting with me or around about the same time as me … you have people to relate to, you can understand … . (Ashton: 48)
26
The journey to self-satisfaction
This theme encompassed the NQNs’ development of critical thinking skills and ability to self-reflect. Critical thinking skills were discussed in five studies.21,22,24,25,27 NQNs began to observe trends and treatment patterns, therefore anticipating interventions. Some had the confidence to make recommendations to the doctor.21,22 They began to trust their instincts and as their confidence grew, they advocated for their patients if they ‘felt that something wasn't right’. 27
In four studies, participants were reflective, describing scenarios they had learnt from.21,22,25,27 Often critical of their own practice, they questioned what they could have done better, without appreciating other contributing factors.21,27 I was so busy and so overwhelmed that night. It was such a pain to have an isolation patient. I felt like my other two patients didn't get my attention. When she died, I felt like I could have done something different … I could have been a little bit more compassionate. I beat myself up for that. (Carmen: 194)
21
I have had a couple of patients that have said … ‘you are a really good nurse keep going this way, don't change, make sure you stay in nursing so that other people have the same experience that I have’; and you come out and you feel really good; and you think like wow … I really made a difference to someone … . (Rose: 24)
25
ICU commitment
This theme explores NQNs preconceptions of ICU and their current position having now worked there.
In three studies, NQNs were motivated to work in ICU by a ‘dream’ or ‘calling’.3,21,26 One attempted to get their ‘foot in the door’ by gaining experience as a Healthcare Assistant.
21
Some NQNs perceived that a lower nurse–patient ratio would give them more time to look after their patients.
3
I felt that I could do a better job here (ICU) than on an understaffed ward. I feel that on a ward, if there isn't enough staff, I couldn't give the standard of care which is not only acceptable to the patient but to me and the reason I went into nursing. (Participant 4: 48)
3
For someone with absolutely no past nursing experience who from undergraduate go out and do GNP [graduate nurse programme] placement, ICU should not be the first placement. I think you should integrate all your basic nursing skills first … . (Carmen: 54)
26
I know that a lot of the senior staff sort of want their GNPs to have a placement on the ward first. But, I don't personally think it's necessary. I think we have those experiences through the undergraduate program. (Ashton: 56)
26
Discussion
The initial aim of this review was to explore the experiences of NQNs beginning their career in Critical Care. The subsequent themes have been illustrated using a conceptual framework shown in Figure 2.
The Newly Qualified Nurses' journey in Critical Care.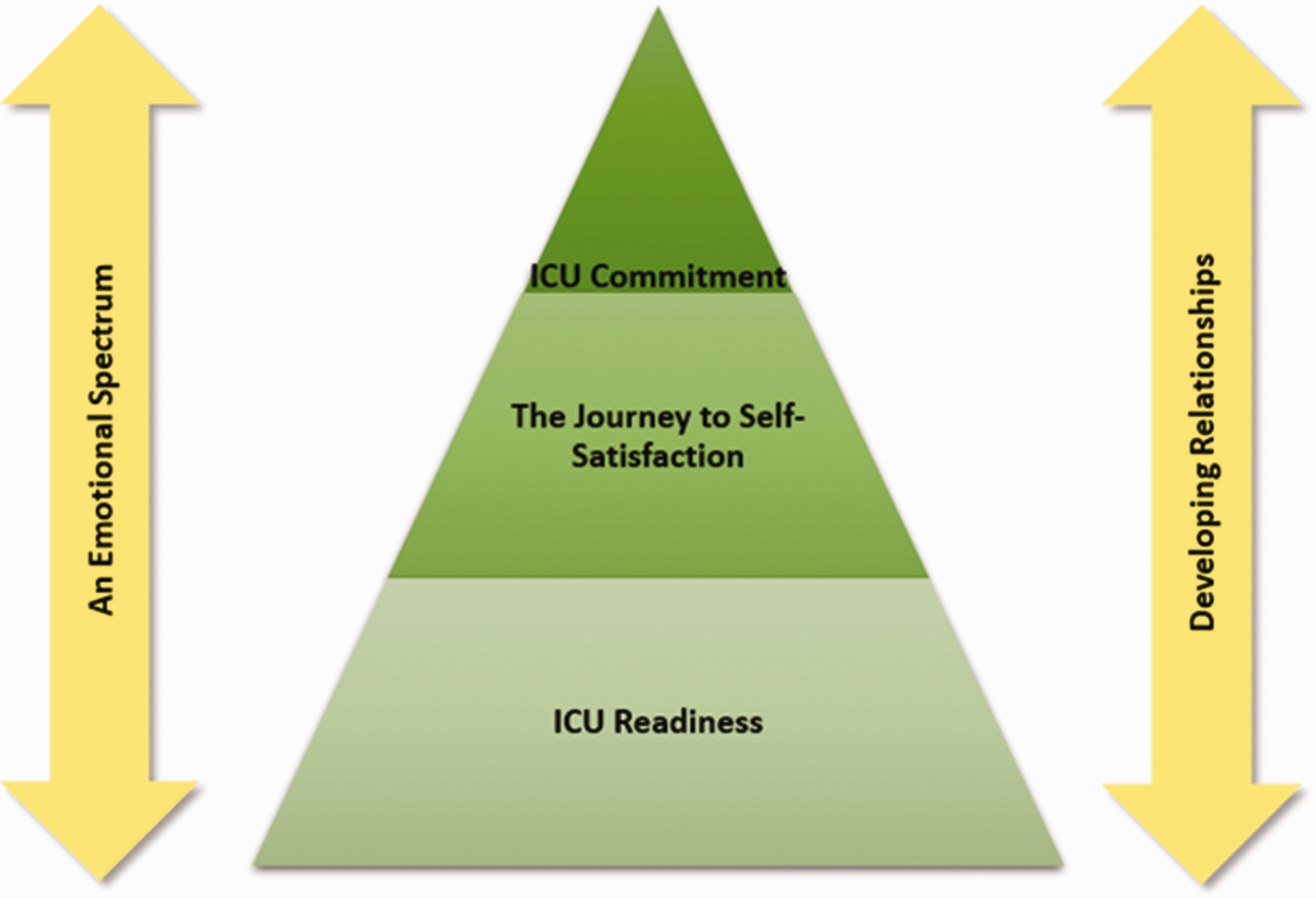
The base of the pyramid represents a strong foundation for building ICU readiness, achieved through undergraduate education, addressing knowledge deficits and inexperience, supernumerary time and the ICU orientation process. The journey to self-satisfaction is a large section at the centre of the pyramid, representing a significant period of self-reflection and developing critical thinking skills. ICU commitment is a slender portion at the top, where the NQN accepts themselves as an ‘ICU nurse’ and expresses a desire to stay. This is a fragile state, and the double-headed arrows flanking the pyramid represent how the NQN may take steps backwards. Having experienced a spectrum of emotions to get to this stage, revisiting negative emotions at the top of the pyramid may cause the NQN to regress. Relationships are equally fragile, positive relationships may strengthen ICU commitment, but confrontations may cause the NQN to question their resolve. However, some NQNs may never reach the top of the pyramid, becoming trapped in the orientation phase, struggling to developing ICU readiness or never completing the journey to self-satisfaction. At this point, they may seek an alternative career path.
Those findings with direct practice implications will now be discussed further. Despite the inclusion of international studies, it is beyond the scope of this review and the author's expertise to critique the domestic health policy of other countries. Consequently, the discussion of findings takes place within a UK context, but the findings may have relevance in other healthcare systems, and the reader may assess their transferability.
Preparation by undergraduate education
Preparation by undergraduate education for working in Critical Care was a key component of ‘ICU Readiness’. NQNs who had not experienced an undergraduate placement in ICU felt disadvantaged now that they were employed as a registered nurse. The Nursing and Midwifery Council (NMC) 32 takes a generalist view on the range of undergraduate placement experiences that should be provided, recommending that ‘training take place in hospitals, other health institutions and in the community’, likely recognising the challenges of finding suitable practice placements. Some of these challenges include the provision of mentors; multiple cohorts of students per year causing peaks and troughs in student activity in practice; factors affecting local services, for instance local rules regarding student placement, ward closures, fluctuating staff, beds and altering clinical priorities as well as wider political and economic influences. 33
Consistent mentorship
Mentor interactions were an important aspect of ‘Developing Relationships’. NQNs expressed particular dissatisfaction in having multiple mentors. Some felt unable to practice new skills, having to prove themselves to each new mentor. Evans et al. 34 found that NQNs valued working the same shift patterns as their mentors. Chenery-Morris's 35 study supports this, with NQNs describing being ‘pushed from pillar to post’, as detrimental to their development. However, some learners felt that it was beneficial to work with other people in order to observe a range of practices. In reality, the availability of experienced staff, mentor workload and willingness to accept the role presents barriers to achieving continuity in mentorship, 36 alongside day-to-day challenges of staffing levels and patient acuity.
The Guidelines for the Provision of Intensive Care Services (GPICS) 13 previously advocated that all newly appointed registered nurses, new to Critical Care, be allocated a mentor with a recognised mentorship qualification and that the learner spend a minimum of 40% of their time with ‘their mentor/assessor/practice educator and/or delegated appropriate other.’ GPICS Edition 2 37 no longer makes recommendations upon nursing mentorship provision; instead, simply advocating that all staff newly appointed to Critical Care receive a supernumerary period to ‘enable achievement of basic specialist competence’. This leaves it to individual units to determine their own model for supporting new staff.
Peer support
The importance of peer support from other NQNs emerged in this review. Boyle et al.'s 38 study supports this, reporting that group cohesion and developing friendships had a positive impact on clinical performance. Recently, Innes and Calleja 39 found that forming relationships with other graduates helped create a culture of support during the transition process, particularly when graduates attended an introductory education programme together.
One study in this review 26 revealed that employing NQNs in groups provided an opportunity for socialisation. Personal experience indicates that this helps new staff integrate and feel accepted as part of the team. Van Rooyen et al. 40 suggest that it may also help to develop professional identity, with positive outcomes for clinical practice. Arguably, this may also cause peaks and troughs in the workforce skill mix, placing additional pressure on mentors, frequently juggling supporting novice nurses with the demands of their workload. 41
Employment of NQNs in critical care
One study 26 directly asked NQNs if they felt that Critical Care was a suitable environment to begin their career. Responses were mixed, but ultimately participants felt that it was dependent on previous experience. Some felt their undergraduate training was sufficient, and others expressed that ICU was more suited to those who had previously worked elsewhere in healthcare. The data in this review is insufficient to pass judgement on this issue, but existing literature discusses manager's perspectives. Ihlenfeld 1 recognises that due to nursing shortages, hiring NQNs is unavoidable; therefore, a thorough recruitment process is essential, with candidates who have experienced an undergraduate placement preferable. Everhart et al. 42 agree recognising that ICU is emotionally challenging. Ideal candidates possess maturity and willingness to develop long-term relationships with patients and families; previous experience an important indicator of this. Kirwan 43 provides a junior nurses’ perspective, suggesting that with the right support, a novice can be empowered to cope in this environment. The NMC 44 states that undergraduate training should produce ‘safe and effective’ nurses at the point of registration, regardless of the environment, thus ultimately the recruitment of NQNs in ICU remains a matter for individual units. Arguably, capability is based as much on personal attributes, as on underpinning knowledge and skills; therefore, NQNs should be judged on individual merit, rather than past experience. 45
Limitations
Only one study was set in the UK, 3 which may limit transferability of the findings. However, transferability is not the primary aim of qualitative research, which seeks to understand phenomena, and it is the responsibility of the reader to contextualise the findings. 46
This work was undertaken as part of an MSc dissertation; thus, it was not possible to achieve triangulation through involving multiple researchers, due to academic constraints. Therefore, all aspects of the design, data extraction, synthesis and interpretation of findings were scrutinised by the academic supervisor regularly.
In this review, solely, the raw data (participant quotes) were synthesised to avoid including the primary reviewer's interpretations, a potential source of researcher bias. Arguably, this approach may not be representative of all the participants' views. However, four of the eight studies in this review were doctoral theses providing greater raw data than traditionally presented in published articles, and the authors of this review were satisfied that data saturation had been met through this method.
Conclusions
There is a perceived knowledge and skills deficit amongst NQNs entering Critical Care. An undergraduate placement in the area may enhance confidence in caring for the critically ill. Consistent mentorship is valued by NQNs, helping to develop supportive relationships and ensuring their skills are recognised and valued. Although mentorship provision is no longer dictated by national guidance if unit pressures permit, senior nurses coordinating the shift should aim to allocate NQNs to work with mentors consistently during the supernumerary phase and in the early days of independent working. Peer support was found to be an important coping mechanism. Although commencing employment of NQNs in groups may not always be possible, opportunities to facilitate socialisation should be provided. The data does not sufficiently address the suitability of employing NQNs in Critical Care; however, based upon existing literature, it is the author's opinion that the NQN should be judged on individual merit, rather than past experience. Instead, recommendations are provided to enhance support for NQNs transitioning in this area. This review has highlighted an overall paucity of research in this subject area; therefore, it is recommended that further studies on NQNs experience be carried out, in particular with a UK focus.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143720926794 - Supplemental material for Experiences of Newly Qualified Nurses in Critical Care: A qualitative systematic review
Supplemental material, sj-pdf-1-inc-10.1177_1751143720926794 for Experiences of Newly Qualified Nurses in Critical Care: A qualitative systematic review by Charlotte E Elias and Tina Day in Journal of the Intensive Care Society
Supplemental Material
sj-pdf-2-inc-10.1177_1751143720926794 - Supplemental material for Experiences of Newly Qualified Nurses in Critical Care: A qualitative systematic review
Supplemental material, sj-pdf-2-inc-10.1177_1751143720926794 for Experiences of Newly Qualified Nurses in Critical Care: A qualitative systematic review by Charlotte E Elias and Tina Day in Journal of the Intensive Care Society
Footnotes
Acknowledgements
The lead author would like express thanks to King's College London and in particular academic supervisor Dr Tina Day, for supporting completion of this work; to the University of Gloucestershire for their support, particularly in granting study time and to CC3N for their encouragement in publishing this work. This work was completed with King's College London, as a dissertation project for an MSc in Education for Healthcare Professionals.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.