
Abstract
Background:
The intensive care unit (ICU) may be described as a ‘deliriogenic’ environment. Critically ill patients diagnosed with delirium are at increased risk of long-term cognitive impairment and hospital mortality. Best practice guidelines recommend early mobilisation interventions to manage and prevent delirium in ICUs. However, evidence evaluating the impact and role of early mobilisation upon delirium in ICUs from the patient perspective is lacking. The aim of this study was to understand the experience of early mobilisation from the perspective of patients diagnosed with delirium in the ICU.
Methods:
This qualitative study adopted a phenomenological approach. One focus group including three participants and seven semi-structured one-to-one interviews were conducted with patients previously diagnosed with delirium in the ICU. Data were analysed using Braun and Clarke’s thematic analysis. Face validity of findings was reviewed by a public representative on the research team.
Results:
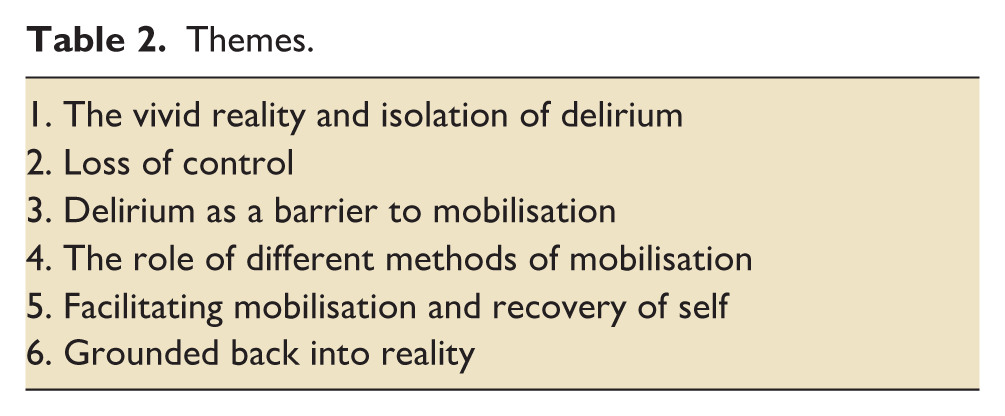
Six main themes were identified: (1). The vivid reality and isolation of delirium, (2). Loss of control, (3). Delirium as a barrier to mobilisation, (4). The role of different methods of mobilisation (5). Facilitating mobilisation and recovery of self, and (6). Grounded back into reality.
Conclusion:
This qualitative study demonstrated the impact and role of mobilisation interventions going beyond the patients’ physical recovery from critical illness. These findings support current best practice recommendations for the implementation of early mobilisation interventions in ICUs.
Introduction
Delirium is defined as an acute and fluctuating disturbance in attention, cognition, altered levels of consciousness from near coma to severe agitation, and at times, psychotic episodes.1,2 The pathophysiology of delirium is unclear but modifiable factors (e.g. immobility, pain) and unmodifiable factors (e.g. age, co-morbidities) are known predispositions for the development of delirium. 3 Delirium affects 30%—50% of patients in intensive care units (ICUs) and over 80% of patients requiring invasive mechanical ventilation.4,5 Evidence demonstrates that delirium is associated with an increased risk of long-term cognitive impairment, cumulative health care costs and is an independent predictor of mortality.4–6 The James Lind Alliance (JLA) top 10 research priorities for ICU identified jointly by clinicians, patients and carers included the: ‘identifying, monitoring and the management of delirium’ and ‘the optimal timing and methods of rehabilitation during critical illness’. 7 Best practice guidelines recommend early mobilisation within a bundle of care to prevent and manage delirium in the ICU.8,9 However, the guidelines are based upon preliminary data.10,11 Moreover, implementation of early mobilisation interventions remains infrequent.12,13 This may be due to heterogeneity and poor reporting of research regarding prescription (e.g. timing, type of activity).12,14 Current guidelines describe mobilisation ‘as a type of intervention within rehabilitation that facilitates the movement of patients and expends energy with a goal of improving patient outcomes’. 8
We recently reported the findings of a mixed-methods systematic review exploring the barriers to, and facilitators of, early mobilisation in critically ill patients diagnosed with delirium. 15 Findings highlighted that delirium was the most common staff reported barrier. The main facilitator was positive patient outcomes of early mobilisation. The studies included in the systematic review comprised staff reported perspectives. Understanding the patient experience may contribute towards improving implementation of early mobilisation interventions which this study aims to explore.
A recent systematic review of qualitative studies explored the needs and perceptions of early mobilisation for critically ill patients. 16 Findings described that patients’ physical and psychological needs across their journey of critical illness are complex and multi-faceted. However, only one included study reported the experience of a patient diagnosed with delirium in the ICU. Therefore, our study addresses this by building upon these findings with a specific focus on the experience of patients diagnosed with delirium in the ICU.
A qualitative study carried out across two hospitals in Sweden and published in 2025 explored patients’ experiences of early mobilisation in the ICU. 17 Three themes were described including: (1). Starting the struggle to regain independence and normal life; (2). Interaction with healthcare professionals and (3). Early mobilisation in a chaotic, confused context without control. Interestingly, one participant reported that early mobilisation relieved their confusion and facilitated their recovery back into reality. Another participant reported that they perceived healthcare professionals to be frightening which they related to their confused mental state. However, whether early mobilisation impacted patients’ delirium was not directly explored. Thus, the aim of this qualitative study was to understand the experience of early mobilisation in patients diagnosed with delirium in ICUs across the United Kingdom (UK).
Methods
The protocol for this study was prospectively published. 18 The consolidated criteria for reporting qualitative research were followed. 19 A phenomenological approach guided the exploration of ICU patients’ perspectives of early mobilisation in the ICU to address the aim of this study.
Prior to data collection and recruitment, a pilot focus group was carried out via Microsoft Teams, with support of four patient and public involvement (PPI) representatives using a co-produced interview script. Following amendments (e.g. Zoom selected to replace Microsoft Teams), the pilot was repeated. All amendments were approved by St. George’s University Ethics Committee (Supplemental file).
Setting and participants
Due to the COVID-19 social distancing guidelines and participants’ clinical vulnerability, interviews were conducted using Zoom, the online platform, within 1 year of hospital discharge. A convenience sample of participants was recruited between March 2021 and August 2021 via social media platforms and attendance of virtual public support groups in Scotland and England. Participants emailed their interest to the corresponding author (JB). Mental capacity to consent was assessed in the potential participants ability to understand, recall and summarise the information provided to them about the research. Consent was re-checked prior to commencing each interview. All participants demonstrated capacity to consent. Following written consent, semi-structured interviews were carried out to allow for flexibility and expansion of answers. The interview questions were co-produced with a patient and public involvement advisory group (PAG) and a PPI representative (RG) on the research team (Supplemental file). Full details of the PPI conducted for this study have been published elsewhere. 18
Data collection
Data collection commenced between June 2021 and August 2021. Initially the focus group method was used and included three participants. Following the first focus group, the method of data collection was discussed with the focus group moderators, research team and PAG. The decision was made that a one-to-one interview method would be more suitable than a group interview method to allow time for an in-depth exploration of all participants experiences. Moreover, time from ICU discharge varied between participants. Therefore, the one-to-one interview method was agreed upon to minimise potential distress that participants recently discharged from the ICU, may experience in a group setting. Semi-structured one-to-one interviews with seven participants were subsequently carried out. A researcher and respiratory physiotherapist (JB) with training in qualitative methods, conducted all interviews. A researcher (GM) and a PPI representative (RG) on the research team were present to observe the focus group and two separate one-to-one interviews.
Interviews were audio-recorded and simultaneously transcribed using Zoom transcription software with consent and permission of participants. The researcher (JB) completed field notes and checked transcripts for accuracy alongside the recordings. Member check approval was carried out following each interview to check for accuracy for example, where transcribed data was unclear. Transcripts were anonymised following member check approval.
Data analysis
The researcher (JB) used Microsoft Excel to complete the data coding and thematic analysis. The six stages of thematic analysis described by Braun and Clarke were followed; namely: familiarisation, generating initial codes, searching for themes, reviewing themes, defining, and naming themes and producing the report. 20
Several steps were taken to demonstrate trustworthiness and rigour. Participants verified the transcribed data for accuracy; two members of the research team (GM, RG) independently cross-checked the process and results of the initial analysis. The final themes were separately verified by two individual members of the research team (GM, RG) and members of the PAG with experience of delirium in the ICU.
Results
Thirteen participants were recruited in total. On verifying eligibility at the time of interview, three participants were excluded (ICU discharge > 1 year). Therefore, 10 consenting participants who had been discharged from the ICU within 1 year and had experienced delirium were included. ICU length of stay ranged from 7 to 21 days. One participant was admitted to the ICU on three occasions within 1 year (Table 1). Four participants identified as male and six as female. Participants’ ages ranged between 40 and 73 years. The resolution of delirium was self-reported by participants. Delirium had resolved for seven participants; one was unsure and one reported partial resolution that is, occurred less than before. Delirium had not resolved for one participant. Ongoing delirium was reported to occur mostly in the evening. Most participants (n = 9) were of white British ethnicity.
Participant characteristics.
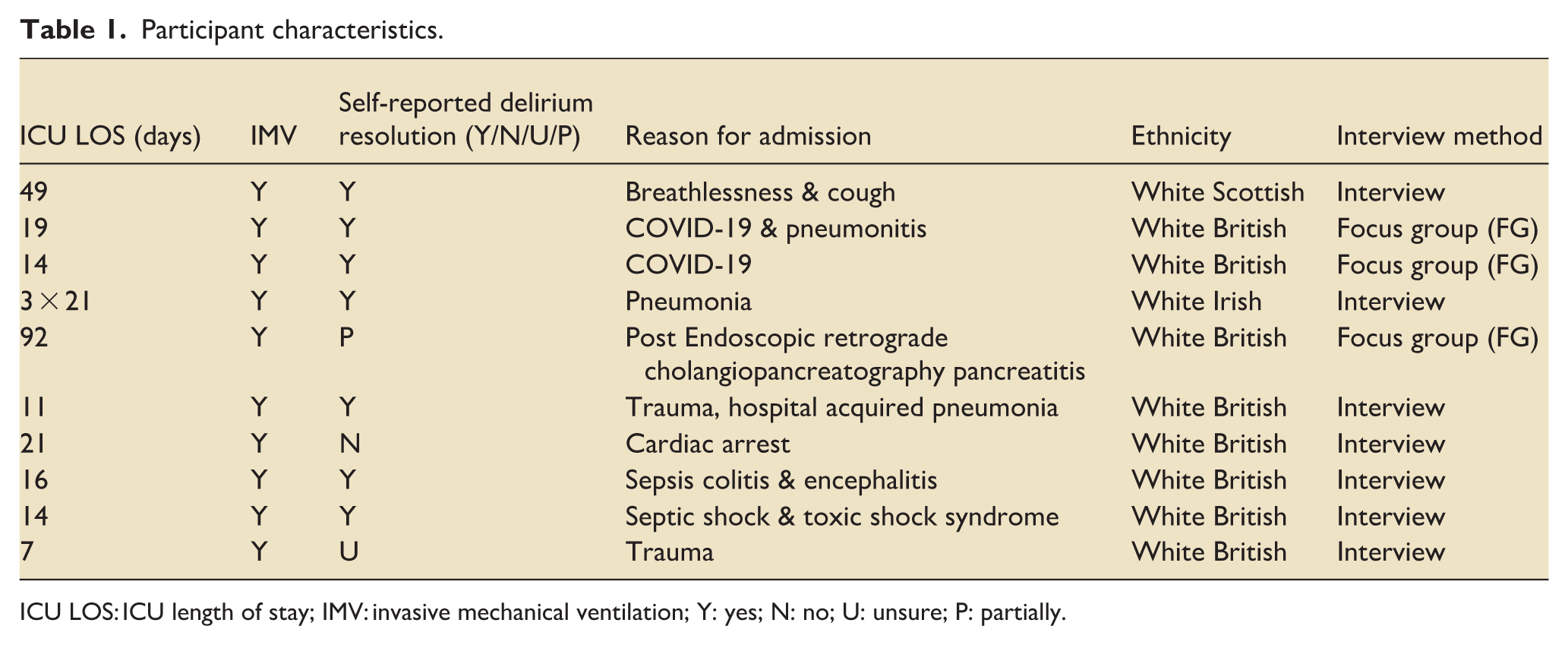
ICU LOS: ICU length of stay; IMV: invasive mechanical ventilation; Y: yes; N: no; U: unsure; P: partially.
The focus group (lasting 110 min) comprised three patient participants. One-to-one interviews were conducted with seven participants (ranging from 48 to 108 min). After this point no new data were added. Six main themes were identified: (1). The vivid reality and isolation of delirium, (2). Loss of control, (3). Delirium as a barrier to mobilisation, (4). The role of different methods of mobilisation, (5). Facilitating mobilisation and recovery of self, and (6). Grounded back into reality (Table 2). Immobility was a prominent theme negatively associated with participants’ experience and intensity of delirium.
Themes.
We now highlight each theme in more detail below:
The vivid reality and isolation of delirium
The experience of delirium impacted participants’ perceptions of the ICU. All participants described their experience of delirium as real. This was because of the vivid detail in which they had ‘lived’ delirium.
“It [delirium] has that texture of reality, whereas a dream doesn’t. . . a dream is.. different.” [FG participant no.3]. “When you’re in delirium. . . . . .there’s nothing to discuss. Whatever’s going on in your mind is absolute reality.” [FG participant no.4].
Participants expressed this was because of the ‘intricacy’ and at times the perceived accuracy of the detail experienced. This led to experiences of ‘lived’ fear because of the difficulty distinguishing between what was real and illusory. Participants described resultant spiralling negative thoughts, paranoia, and feelings of being tortured.
“. . .I had to do as they said and then they’d let me go. . .I thought I was in a coffin being kept alive by a tube. . . .” [participant no.10].
Most participants described negative experiences of delirium except two participants who described a ‘good delirium’. Interestingly, they reported that it was the uncertainty about the authenticity of reality that led to feelings of loss of control and loneliness.
“I was having good dreams, which were far too vivid for me, not to believe they were actually happening” [participant no.2] . . . “because I don’t know whether it [delirium] was [real] or not, that was frightening”. [participant no.9].
Participants reported that delirium in the ICU was more intense and continuous than on the inpatient wards. They described the experience of delirium after the ICU was episodic. However, one described it as episodes of delirium on the ICU. Another described their experience as a series of deliriums.
“The ICU experience was with 99% delirium with little bits of reality. . . that proportion started to change when I went onto the acute wards.” [FG participant no.3].
Loss of control
The loss of mobility appeared closely related to the theme of loss of control. Participants described immobility as frightening, feeling stuck, trapped, and frustrated. This resulted in a sense of loss of self. This participant explained: “. . .when you have a normal nightmare, you can get yourself up out of bed. . . When you can’t move yourself. . .You can’t escape it [delirium]. . .I know that I was distressed by my body. . .I felt it was all fading away around me. And I think it was part of me feeling, am I here, am I not here? Am I dead? I even thought that you know, sort of lost, who you are. . .” [participant no.13].
One participant expressed the shame they felt at losing themselves in the experience of delirium.
“. . .the thoughts or the visions . . .and the feelings I was experiencing was so opposite to the me of normal. . . they were quite violent. . . racist. . .aggressive. . . the opposite of who I am.” [participant no.11].
Moreover, participants perceived the care they received whilst being immobile as negative and scary things being done to them. Through the experience of delirium this was described as a kind of torture due to the inability to decide for themselves, communicate, move or understand what was real.
“I just thought these people were, were torturing me” [Participant no.12]. “I had to do as they said and then they’d let me go. I felt like I was being held against my will. I felt like I wasn’t in control, I couldn’t do anything but lay there. I was just there. . . I could even be dead.” [participant no.10].
Delirium as a barrier to mobilisation
Most participants felt the approach to mobilisation was focussed towards improving their physical function. Moreover, they expressed they felt their delirious state meant mobilisation was not prioritised.
“I would say it [delirium and physical activity] was [managed as] two separate things.” [participant no.6].
This led to some participants feeling frustrated with their experience of the care they received.
“No, I had [mobilisation] in ICU, but they’ve written in there [ICU diary] that they couldn’t do a lot because I was so disorientated. . . there must be ways of working with people who are having that experience.” [participant no.11].
Similarly, participants reported delirium was a barrier to their physical progression compared to other patients on the inpatient wards post ICU.
“I think, because I had the delirium maybe I wasn’t moved or didn’t have as much [mobilisation on the ward] as maybe I would have done if I didn’t have delirium.” [participant no.11].
One participant described how they felt their experience of mobilisation was specifically offered to address their delirium in the ICU.
“I think it [mobilisation] helped me on ICU, I think it was part of the delirium management on ICU . . .but I don’t think I had any delirium management. . . on the step-down wards.” [participant no.13].
Interestingly, participants expressed that the timing of mobilisation during their ICU admission may have influenced their recovery from delirium and their experience in the ICU.
“If they did start the process of the physical activity early in the [ICU], I don’t think it would’ve [made delirium worse]. I think it would have helped. I really do.” [participant no.12].
The role of different methods of mobilisation
Participants described their experience of feeling grounded during functional activities for example, sitting on the edge of the bed and standing.
“. . .when they. . .stand ya up it’s like your feet are hitting the floor. So, it’s like grounding.” [participant no.9].
However, one participant reported that abstract activities such as being hoisted into a chair was, “. . .sort of an out of body experience . . . a few times I was heaved up in the hoist. It’s scary scary.” [FG participant no. 4].
In-bed activities for example, assisted passive limb movements, were reported to provide relief and distraction from the physical discomfort of immobility and the intensity of delirium. However, participants felt frustrated with the infrequency of both in-bed and out-of-bed activities. They expressed feelings of being stuck, unsafe and the need for mental focus.
“I don’t feel that the in-bed exercises were that much. I felt I needed more. . . felt quite trapped really in bed. I couldn’t move myself. I think I became distressed. I think that must have impacted on the delirium.” [participant no.13]. “. . .maybe. . .physical [activity] with my hands. . . I’d have been able to do it. That would have been something that I could have started at the early stages. I can guarantee that would have exhausted me. And it would have took my focus off . . . who’s of these are trying to kill me. . . and I would’ve slept a bit better.” [participant no.12].
Facilitating mobilisation and recovery of self
Referring to their patient diaries (completed by ICU staff) and recall, participants described that mobilisation was a co-ordinated effort in physiotherapy and nursing care. Some participants explained that physiotherapists completed initial assessments and less frequent but longer mobilisation sessions. Whereas others experienced more frequent but shorter episodes of mobilisation with the ICU nursing staff. However, this differed between participants.
“I’d say it was the nurses more with everything. . . . . . . .I suppose I saw the physio twice maybe in my remembering. . .” [participant no.10]. “The longest periods of contact were with the physios, and I knew. . .they were going to help me get out of hospital, get on my feet.” [FG participant no.4].
Factors described to improve mobilisation whilst experiencing delirium included staff availability, kind communication and reassurance. These helped participants to feel safe and overcome the fear experienced from delirium and their acute realisation of their new self.
“I felt safe, and they kept reassuring me I was safe. I can recall that on ICU. . .” [participant no.13].
Participants described how the inclusion of relatives and goal setting empowered their personal drive, sense of control and identity.
“When I first saw my wife. . .I realised that this wasn’t my life that I wasn’t a professional patient.” [FG participant no. 3]. “. . .obviously when you’re in that situation the targets will be very small, but progression is improvement, and. . .that’s invaluable for moving forward with your mind process as well.” [participant no.12].
Grounded back into reality
All participants expressed that mobilisation was important for both their physical and mental functioning. They explained that this was because it brought relief from delirium and facilitated their recovery (in mind and body).
“So, in a way for me it’s like a necessity. . . as much as you need the oxygen ..you also need to be able to move and being moved is part of that treatment, regardless of delirium. . . . [health professionals] definitely need more help, because it [immobility] just cannot be helping with recovery because it [delirium] is so traumatic. . . . I wish that there was more time to move people. . .” [participant no.13]. “No, I think it [mobilisation] prevents it [delirium]. . .I think if you’re focusing on something all the time and not moving, you tend to overthink things.” [participant no.6].
All participants described how their initial experience of mobilisation in the ICU ‘broke’ their delirium.
“. . . .my first experience of being mobilised . . .brought me back into reality. I credit that as a very strong moment for me. That got me out of complete delirium and delusion.” [participant no.13].
Most participants used the term ‘grounded’ to describe how mobilisation was felt to reduce the intensity of, or ‘break’ their delirium. This contrasted their descriptions of how immobility exacerbated their delirium.
“There was no positive [impact on delirium] of not doing anything. . . In my honest opinion there was no positive whatsoever” [participant no.12].
Furthermore, mobilisation was described as a process of realisation where they were able to dissociate between their natural state and delirium.
“. . . . It (mobilisation) made me become more aware of what was happening to my body. Whereas before whenever I was just lying in the bed not doing any exercises. . . my mind was just running rampant. . .doing its own thing, looking for something to do.” [participant no.2]. “. . .The [mobilisation] experience was the most grounding. . .It was hands-on and brought me back into my body. . .” [FG participant no.1]
Participants described their experiences of mobilisation as a journey of freedom and escape from delirium towards regaining control. However, all participants explained how difficult a journey this was due to the realisation of their loss of control and the shame experienced upon becoming aware of their new and reduced physical and mental capability. Moreover, they described limitations to mobilisation such as fear of falling, lack of staffing and the ICU environment.
“I think the two [mobilisation and delirium] are interlinked. . .It had some impact on grounding me. . .but I was so weak. . .I was so scared of falling.” [participant 11]. “The room was too small for the physiotherapists to bring in the different pieces of equipment [e.g., hoist].” [participant no.2].
The frequency and timing of their mobilisation was of a particular focus for participants. However, all participants expressed the method of mobilisation wasn’t of great importance because any form of movement facilitated recovery of ‘self’ and some freedom from delirium.
“So, if they did keep up with whatever physical activities they can do when you’re intubated, I think, that would be very important. . . if it’s done on a regular basis. . . it will eventually make the delirium go away. . .that would ground a lot of people, and the delirium perhaps won’t last as long.” [participant no.9]. “Definitely early as possible. And as much as possible. . . And not just necessarily getting them out of bed it’s like I say even doing little things with your hands.” [participant no.12].
All participants expressed that mobilisation did not adversely impact their delirium. However, one participant expressed that they felt frustration during activities because of their inability to concentrate. Moreover, participants expressed they had felt disappointment and frustration because they expected regular progressive mobilisation.
“. . .I was a bit disappointed, that. . . eh the [mobilisation] regime wasn’t a bit more intense. I was expecting more.” [participant no.2].
Discussion
The findings of this qualitative study highlight the experiences of both immobilisation and mobilisation for patients diagnosed with delirium in the ICU. Mobilisation was described to break delirium, ground participants back into reality and help integrate them back into their bodies. Participants perceived that mobilisation provided an escape from the lived ‘reality’ of fear, torture and paranoia in which they felt trapped without personal agency. These findings build upon those described by Söderberg et al where one participant reported that early mobilisation provided relief from delirium and supported their recovery back into reality. 17 Although mobilisation facilitated their journey to recovery, the realisation of their new physical and mental capabilities was described as difficult. Additionally, participants explained their recovery was frustrating at times. This was due to several barriers to mobilisation including staff availability, delirium itself, concentration difficulties and the environment design. Corner et al, similarly identified that delirium, fatigue and poor memory were limitations to rehabilitation and recovery from ICU-acquired weakness. 21 Moreover, this study provides new knowledge highlighting the experience of different methods of mobilisation. This may support the JLA research priority for intensive care to identify optimal methods of rehabilitation in ICU and importantly guide clinicians in the consideration of in-bed and out-of-bed mobilisation. 7
All participants in the present study stressed that, in their opinion, mobilisation initiated as early as possible regardless of the type of activity (e.g. in- or out-of-bed), is a necessity for their recovery from delirium. Furthermore, they expressed their sobering experiences of immobility upon delirium in the ICU resulting in feelings of loss of self, terror and torture. These findings are comparable to previous studies, where mobilisation was described by both patients and relatives in the ICU as a necessity and important to initiate as early as possible.21,22 Our study contributes further to previous research by providing a unique insight into the patient experience and perception of mobilisation specifically in facilitating their recovery from delirium in the ICU.
Following the first trial in 2009 that found that early mobilisation was associated with reduced delirium in the ICU, limited research has been undertaken to explore the effectiveness of these interventions to manage and prevent delirium. 10 This is because the evidence to date has mainly focussed on investigating the physical recovery of critically ill patients. Two recent systematic reviews and meta-analyses investigated the impact of physical activity interventions and early mobilisation upon delirium in the ICU.14,23 The results indicated a paucity of trials exploring the effectiveness of physical activity upon delirium. Furthermore, studies investigating the management and treatment of delirium in the ICU have demonstrated considerable heterogenity. 24 This may limit implementation of the best practice guidelines into standard ICU practice.8,9 Recently, Patel et al. demonstrated that early (within 96 h of IMV) physical and occupational therapy reduced cognitive impairment at 1 year after hospital discharge. Secondary outcomes showed reduced duration (days) of delirium in the intervention group compared to usual care (0 (0–2) versus 1 day (0–3); p = 0·005). 11 These findings further support the evidence suggesting that there is a need to investigate the effectiveness of early mobilisation intervention to manage and prevent delirium in the ICU. Our study’s findings build upon the evidence to date and may may support clinician’s understanding of the role of, and approaches to, implementing early mobilisation interventions. This may facilitate clinicians’ prioritisation of early mobilisation interventions to manage and prevent delirium in the ICU.
Strengths and limitations
A strength of this study was the access to this research for potential participants from ICUs across the UK with support by the ICU steps Charity and social media platforms in the context of the COVID-19 pandemic. This helps contribute towards the depth and diversity of the data collected. However, it is noted that participation was limited to Scotland and England due to the availability of virtual support groups at the time. Although using different interview methods may limit the depth of data, data saturation (no new data) was apparent therefore, no further one-to-one interviews were added. 25 Thematic analysis of the initial focus group data allowed the exploration of the phenomenon of interest and identified potential patterns of conceptualisation. One-to-one interviews built upon these data with greater depth to further develop and conceptualise themes.
The time from ICU discharge to interview may be a limitation of this study due to variation of participants recall and cognitive recovery such as impaired memory. In this study most participants were able to confirm the timing of events with reference to their ICU patient diaries, discussion with family members/ friends, hospital visits and their discharge summaries. The perspectives and experiences highlighted in our study are limited to those of previous ICU patients diagnosed with delirium. This was because of the difficulties recruiting relatives and carers (Supplemental material). This may be due to an increased burden of care during the COVID-19 pandemic. Additionally, participant’s experiences could have been impacted by the COVID-19 pandemic, which may be important to consider when interpretating these findings. Moreover, all participants were of white ethnicity. This may be a limitation of convenience sampling. Exploring strategies to improve accessibility and inclusivity of other ethnic groups should be considered in future research to optimise transferability of findings.
Conclusion
This is the first study providing insight into patients experiences of delirium and the impact of mobilisation and immobilisation, upon their delirium in the ICU. Our findings demonstrate that critically ill patients perceive mobilisation in the ICU as a necessity for the prevention and management of delirium. Participants expressed that immobilisation exacerbated their delirium and experience of loss of self. All participants stressed the importance of initiating both in and out-of-bed mobilisation early to help provide relief from delirium and support their recovery. These findings may support ICU clinicians with further knowledge and understanding about the role of early mobilisation as a non-pharmacological treatment for the management and prevention of delirium.
Supplemental Material
sj-docx-1-inc-10.1177_17511437261416698 – Supplemental material for The impact of early physical mobilisation for the management and prevention of intensive care unit delirium: A qualitative study exploring patients’ perspectives
Supplemental material, sj-docx-1-inc-10.1177_17511437261416698 for The impact of early physical mobilisation for the management and prevention of intensive care unit delirium: A qualitative study exploring patients’ perspectives by Jacqueline Bennion, Roger Garrett, Duncan Barron, Daniel Martin and Gill Mein in Journal of the Intensive Care Society
Footnotes
Ethical considerations
St. George’s University Ethics Committee approved this study (REC No. 2021.0019).
Consent to participate
All participants gave written informed consent before data collection began.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This qualitative research is independent research supported by the National Institute for Health Research HEE/NIHR ICA Programme Pre-doctoral Clinical Academic Fellowship, Miss Jacqueline Bennion, NIHR301174. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research or the Department of Health and Social Care. The first author (JB) independently raised funding for public members involved in the research process for this study. This involved crowdfunding by completing the Wimbledon trail half marathon in October 2021.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.