
Abstract
Recently, we published self-reported data concerning the perceived effects of the menstrual cycle and hormonal contraceptives on the training and performance of 1086 female athletes participating in 57 sports. However, studies comparing differences between sports with large sample sizes are lacking. The aim of this ancillary study was to compare the impact of the menstrual cycle and hormonal contraceptives on training and performance between the three largest sports in the cohort, that is, football, handball, and orienteering, as well as the knowledge and support provided to the female athletes engaged in these sports. The results are from a web-based questionnaire completed by 312 football players, 243 handball players, and 93 orienteers. A total of 54% of the orienteers planned their training based on the menstrual cycle, which was a higher proportion compared to football (45%) and handball (29%) players (p < 0.05). Fewer football players believed that the menstrual cycle had an impact on their performance during training and competition compared to the two other sports. A high proportion of the athletes used hormonal contraceptives in all three sports, but a lower proportion of the orienteers (40%) used hormonal contraceptives compared to football (76%) and handball players (66%) (p < 0.05). Football and handball players received overall more support than orienteers, and the support was mostly provided by a physiotherapist and/or a strength and conditioner coach besides the main coach. These findings demonstrate that the perceived influence of the menstrual cycle and hormonal contraceptives on training and performance differs between endurance athletes in orienteering compared to team-sport athletes in football and handball.
Introduction
The influence of the menstrual cycle (MC) and hormonal contraceptives (HCs) on athletic performance are currently widely debated in the athletic community. Although an increasing number of researchers are addressing these questions, definitive answers are still lacking.1–3 A recent meta-analysis 1 concluded that there is a trivial reduction in muscle strength and aerobic performance during the early follicular phase (menses) of the MC compared to the mid-cycle (ovulation) and the mid-luteal phase (premenstrual). However, several knowledge gaps regarding the impact of female hormones on physical performance during the MC still exist,1,4,5 and no general guidelines are yet available.
Despite weak evidence regarding the physiological impact of female hormones on athletic performance, several studies have shown that athletes perceive that the MC influences their training and performance,6–12 particularly due to symptoms such as menstrual-related pain (dysmenorrhea) and premenstrual symptoms (PMSs). Perceptual responses such as motivation, competitiveness, and mood also seem to vary between the MC phases, with favorable responses in the late follicular to ovulatory phase and more negative responses in the late luteal phase and during menses. 13 Female athletes have also been shown to use HCs to a greater extent than the general population in the Nordic countries, 14 even though the effect of different HCs on physical performance is not fully understood. 2 Besides birth control, HCs are often used by female athletes as treatment for dysmenorrhea, menorrhagia, and amenorrhea, as well as to postpone or omit menstrual bleeding.2,10 This may explain why this group uses HCs to a greater extent than the general population.
We have recently published two studies based on self-reported data from 1086 athletes in 57 different sports.10,15 In these studies, the perceived impact of the MC and HCs on physical performance as well as offered support and knowledge were presented.10,15 However, it was beyond the scope of these studies to compare the results of the different sports included. Football, handball, and orienteering were the three most common sports in our cohort.10,15 Football and handball are characterized by intermittent work with the ability to quickly change direction and master cutting, agility, and pivoting maneuvers, whereas orienteering is an endurance sport performed in rough terrain with high cognitive elements. Because of these different demands, it is reasonable to suggest that the MC and use of HCs could impact training and performance differently. Although the perceived impact of the MC and HCs are explored in many previous studies,8,16,17 so far none has directly compared sports with large sample sizes.
The aim of this ancillary study was to compare female football players, handball players, and orienteers with respect to the perceived impact of their MC and usage of HCs on their training and performance, as well as to examine the perceived knowledge possessed by and support provided to these athletes. We hypothesized that in this context the perceptions of the participants in the individual endurance sport of orienteering differ from those involved in the team sports of football and handball.
Materials and methods
Study population and ethics
Active female members of the Swedish or Norwegian Sports Federation, at least 18 years of age, were recruited via social media and emails to professional sports clubs, as previously described. The athletes were given written information about the study before providing their consent to complete the questionnaire. Of the 1086 athletes in 57 different sports, 648 female athletes were engaged in the three most represented sports (i.e. football, handball, and orienteering). For demographic data see Table 1. Of those, 33% (n = 214) were elite athletes (i.e. athletes participating in the Olympic games, World or European championships, or in other international competitions, national championships, or the highest national league) and 77% (n = 434) were sub-elite athletes (i.e. athletes participating in the second highest national league or district competitions).
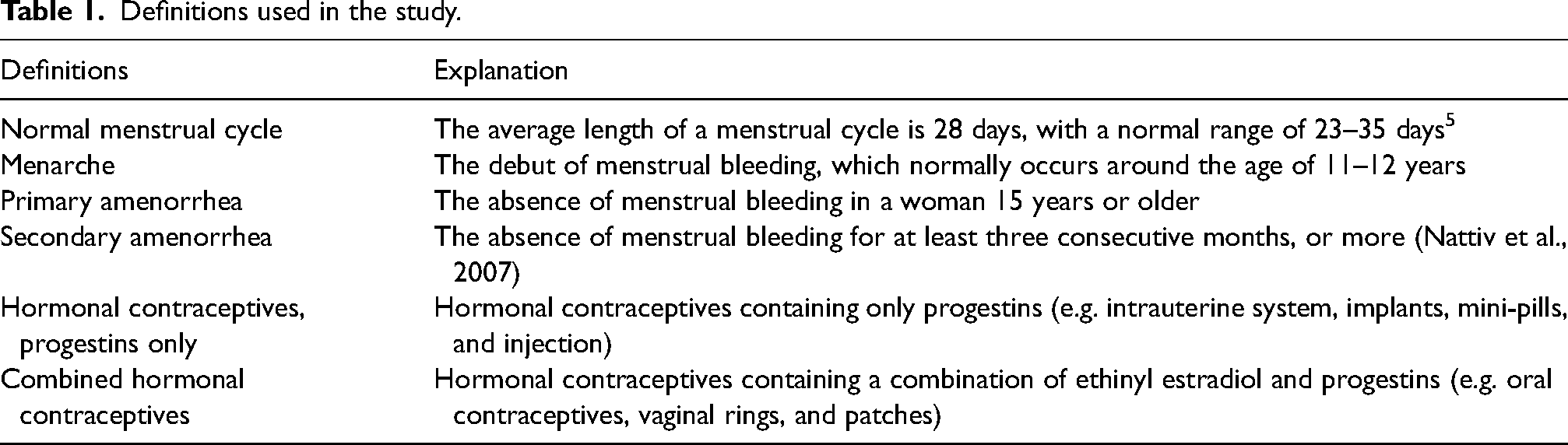
Definitions used in the study.
The study was approved by the Swedish Ethical Review Board (Dnr 2020-00418).
Questionnaire
A questionnaire was developed to collect demographic data, information about menstrual history, perception of the impact of the MC and HCs on athletic performance, and access to support in this context within the athletic community, as previously described.10,15 A pilot study involving 124 female athletes (median age 20 (IQR 19–24 years), median body mass index (BMI) 22.2 (IQR 21.2–23.5)), were performed to test face and content validity of the questionnaire. After the participants had filled out the questionnaire, a group discussion was conducted where the participants had the opportunity to point out ambiguities in the form and overlapping questions. Minor modifications of the questions were made after the group discussion and face as well as content validity was determined as satisfactory.
Definitions used in the study are presented in Table 1.
Data analysis
Categorical variables are expressed as frequencies and percentages (%) and continuous variables as means and standard deviations (SD). For data that was not normally distributed median and interquartile range (IQR) was used. Differences between the elite athletes in the different sports, with respect to knowledge concerning menstrual-related issues in an athletic context were tested with chi-square tests, while analogous differences between different age groups were examined using one-way ANOVA. Effect sizes for continuous data are expressed as partial eta squared as η2 and for chi-square tests as w indices. The level of statistical significance was set at ≤ 0.05. All analyses were performed utilizing Microsoft Excel (Microsoft Corporation, Redmond; WA, USA) and IBM Statistical Package for the Social Sciences (Version 27.0, SPSS Inc., Chicago, IL, USA).
Results
Demographic data of the athletes, divided into the three different sports is presented in Table 2. The orienteers were older and had a significantly lower BMI (21.3 kg/m2) compared to the football (22.8 kg/m2) and handball players (23.5 kg/m2) (p < 0.001, η2 = 0.05), whereas the handball players reported the highest training volumes. The proportion of orienteers competing at the elite level (81%, n = 76) was higher compared to the football and handball players (22%, n = 68 and 29%, n = 70, p < 0.001, w = 0.43).
Descriptive demographic data for the athletes (n = 648) divided into football, handball, and orienteering.
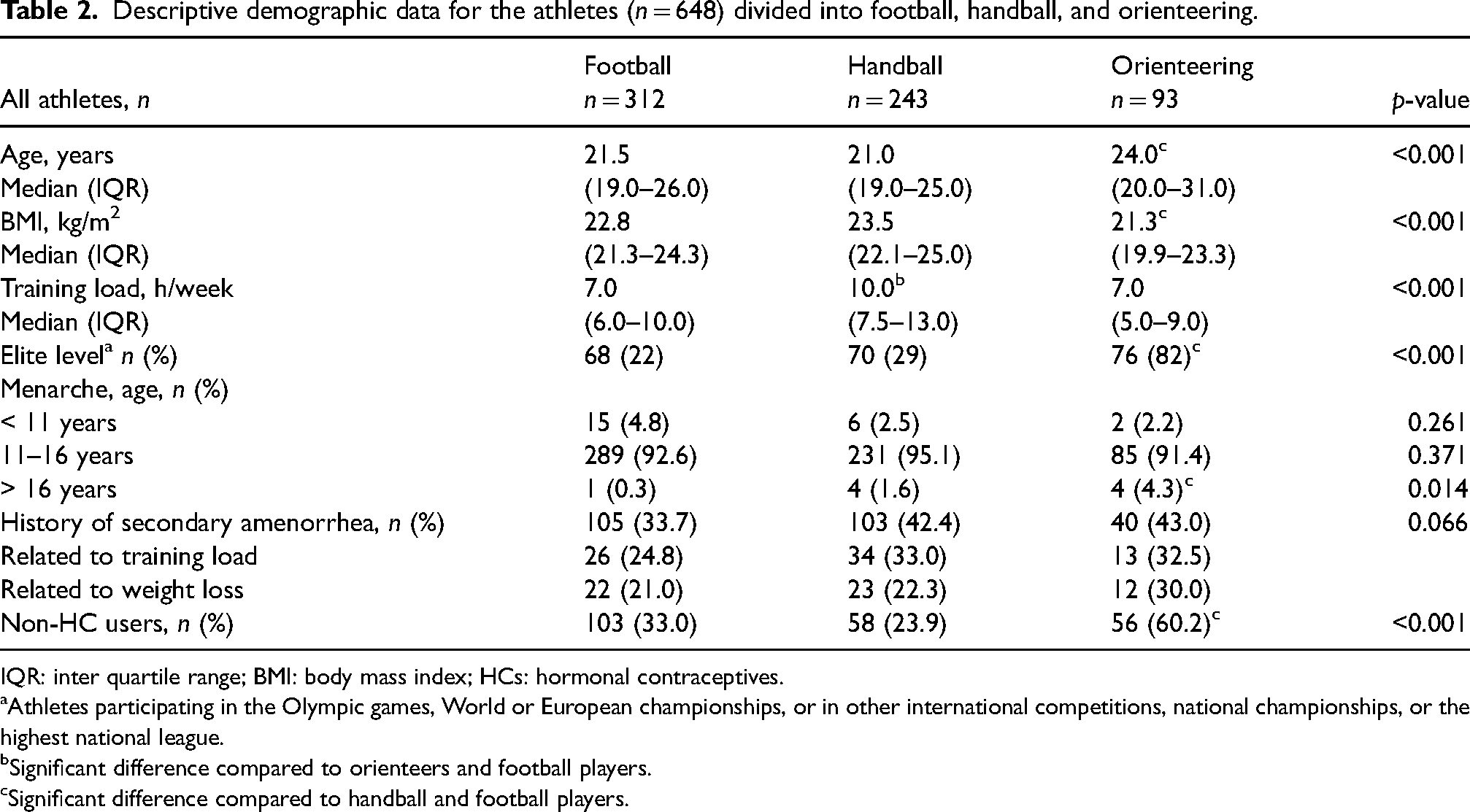
IQR: inter quartile range; BMI: body mass index; HCs: hormonal contraceptives.
Athletes participating in the Olympic games, World or European championships, or in other international competitions, national championships, or the highest national league.
Significant difference compared to orienteers and football players.
Significant difference compared to handball and football players.
Most of the athletes (93%, n = 605) experienced menarche within normal age range. Among the orienteers, a significantly higher proportion reported menarche at an age > 16 years, compared to the football and handball players (4%, n = 4 vs. 0.5%, n = 1 and 2%, n = 4, p = 0.014, w = 0.11). History of secondary amenorrhea tended to be less frequent among the football players compared to the handball players and the orienteers (34%, n = 105 vs. 42%, n = 103 and 43%, n = 40, p = 0.066, w = 0.09).
The orienteers were a significantly higher proportion of non-HC users compared to the football players and handball players (60%, n = 56 vs. 33%, n = 103 and 24%, n = 58, p < 0.001, w = 0.25).
Impact of the MC (non-HC users)
Demographic data and menstrual-related symptoms in the non-HC users are presented in Table 3.
Descriptive demographic data and MC-related symptoms in numbers (percentage) for the athletes not using hormonal contraceptives (non-HC users), n = 217, divided into football, handball, and orienteering.
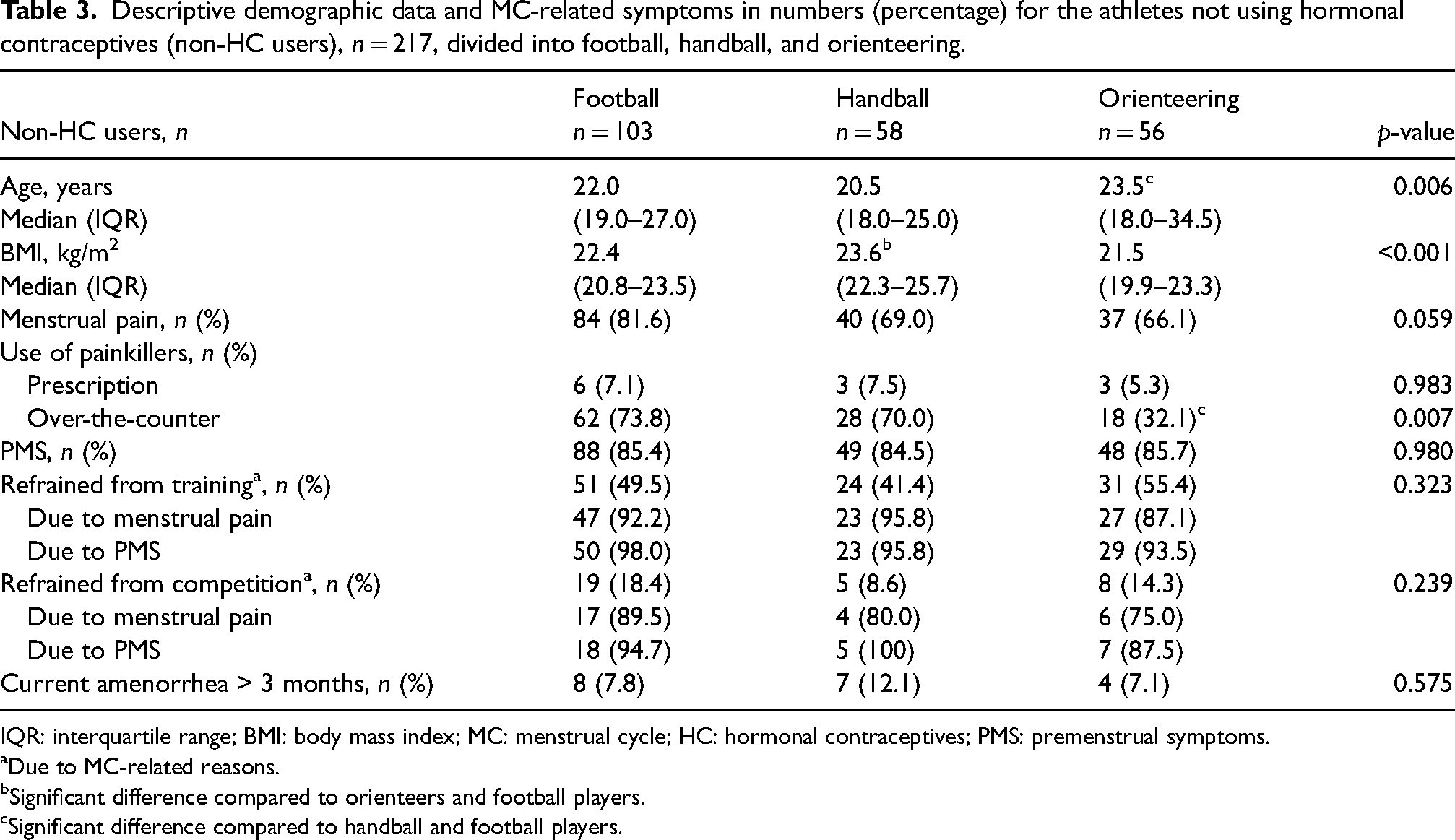
IQR: interquartile range; BMI: body mass index; MC: menstrual cycle; HC: hormonal contraceptives; PMS: premenstrual symptoms.
Due to MC-related reasons.
Significant difference compared to orienteers and football players.
Significant difference compared to handball and football players.
The football players tended to report menstrual-related pain to a higher extent compared to the handball players and orienteers (82%, n = 84 vs. 69%, n = 40 and 66%, n = 37, p = 0.059, w = 0.16). On the other hand, orienteers (32%, n = 18) used over-the-counter painkillers to a significantly less extent compared to the football and handball players (74%, n = 62 and 70%, n = 28, p = 0.007, w = 0.25). Most of the athletes (85%, n = 551) experienced PMS but without any difference between groups.
Overall, there were no significant differences between the sports that refrained from training or competition due to MC-related symptoms (Table 3). However, most of the athletes, regardless of sport, reported that they believed that their MC had some or even a considerable impact on their performance during training and competition (Figure 1A and B). The football players believed to a significantly lesser extent that their MC had an impact on the training compared to the handball players and the orienteers (86%, n = 88 vs. 94%, n = 55 and 96%, n = 54, p = 0.034, w = 0.18) (Figure 1A). The proportion of the orienteers (54%, n = 30) who planned their training to some or to a considerable extent based on their MC was significantly higher than in the case of the football (45%, n = 46) and handball players (29%, n = 17, p = 0.043, w = 0.17) (Figure 1C).
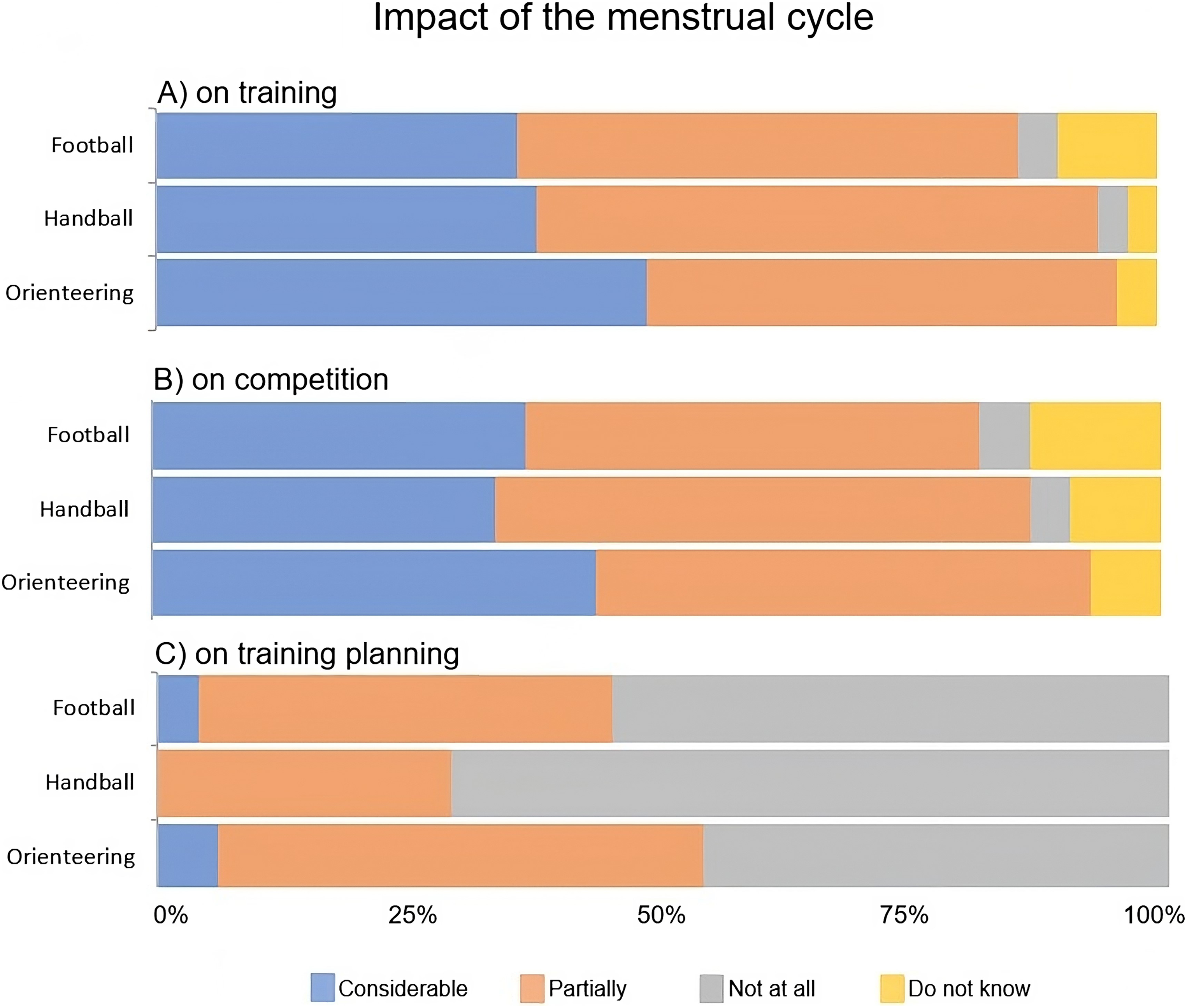
Athletes’ perception of the impact of the MC on performance, is divided into football, handball, and orienteering. (A) MC has an impact on training, (B) MC has an impact on competitive performance, and (C) plan the training according to the MC. Percentage of athletes (non-HC users), n = 217.
The influence of HCs users
The use of HCs was lower among the orienteers (40%, n = 37), compared to the handball (66%, n = 209) and football players (76%, n = 185, p < 0.001, w = 0.25). The football players reported side effects of their HCs to a greater extent than the handball players and the orienteers (47%, n = 41 vs. 37%, n = 68 and 38%, n = 14, p < 0.001, w = 0.19). It was less common among HC users to refrain from training and competition (41%, n = 178 and 12%, n = 52) due to menstrual-related issues compared to non-HC users (49%, n = 106 and 15%, n = 32), without any difference between sports. Reasons for refraining from training and competition are shown in Table 4.
Descriptive demographic data and HC-related symptoms in numbers (percentage) for the athletes using hormonal contraceptives (HC users), n = 431, divided into football, handball, and orienteering.
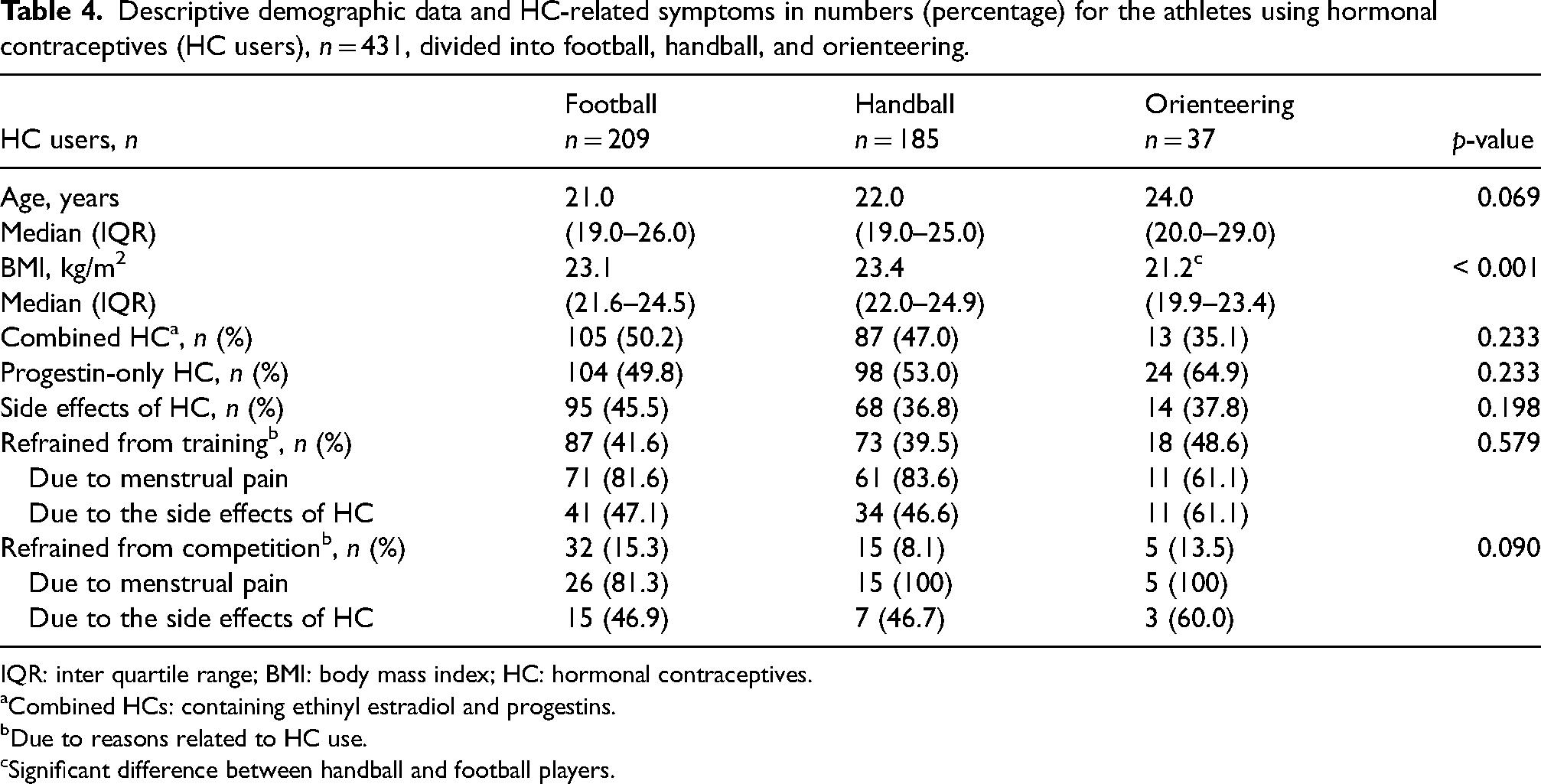
IQR: inter quartile range; BMI: body mass index; HC: hormonal contraceptives.
Combined HCs: containing ethinyl estradiol and progestins.
Due to reasons related to HC use.
Significant difference between handball and football players.
Most of the athletes, regardless of sports, believed to some or even a high extent that their HCs impacted their training and competitive performance, but there were no significant differences between sports (Figure 2A and B). The HC users (35%, n = 151) reported planning their training with respect to HC use to a lesser extent compared to the non-HC users (43%, n = 93, p = 0.052, w = 0.08). Among the HC users, there were no differences between sport groups in training planning related to their HC use (p = 0.317, w = 0.07) (Figure 2C).
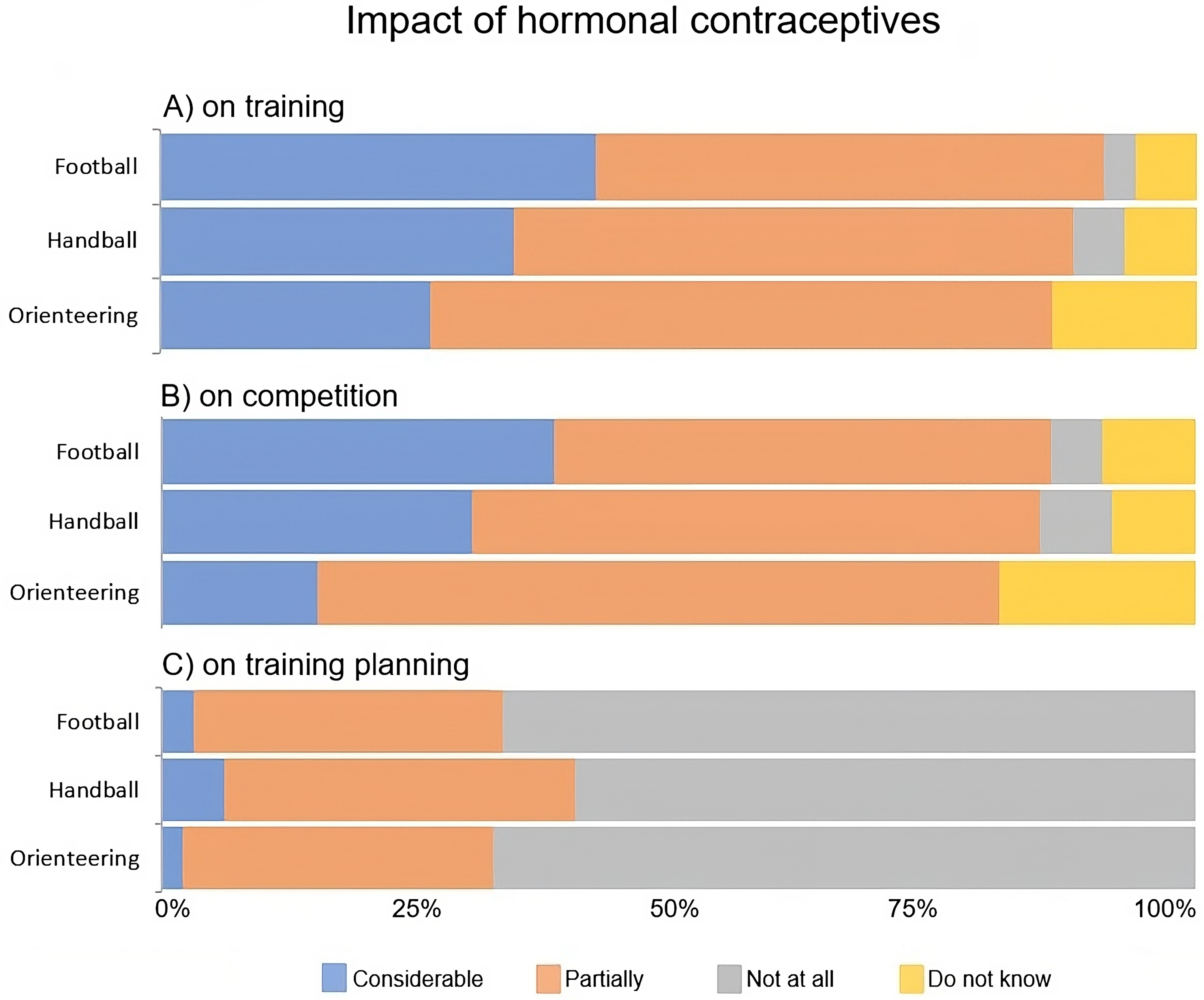
Athletes’ perception of the impact of the use of hormonal contraceptives (HCs) on performance, is divided into football, handball, and orienteering. (A) HC use has an impact on their training, (B) HC use has an impact on their competitive performance, and (C) plan the training according to the use of HCs. Percentage of athletes (HC users), n = 431.
Support provided to the athlete
A significantly larger proportion of the football and handball players (97%, n = 304 and 98%, n = 237) reported to have a main coach, than the orienteers (44%, n = 41, p < 0.001, w = 0.62). Having a female coach was significantly more common among the football players (16%, n = 49) compared to the handball players and the orienteers (9%, n = 21 and 3%, n = 3, p = 0.001, w = 0.15). Overall, the handball and football players (84%, n = 207 and 75%, n = 234) received significantly more overall support (e.g. physiotherapist, physician, gynaecologist, dietician, mental coach, strength and conditioner coach) than the orienteers (41%, n = 38, p < 0.001, w = 0.33). Figure 3 displays the support offered in the different sports, respectively.
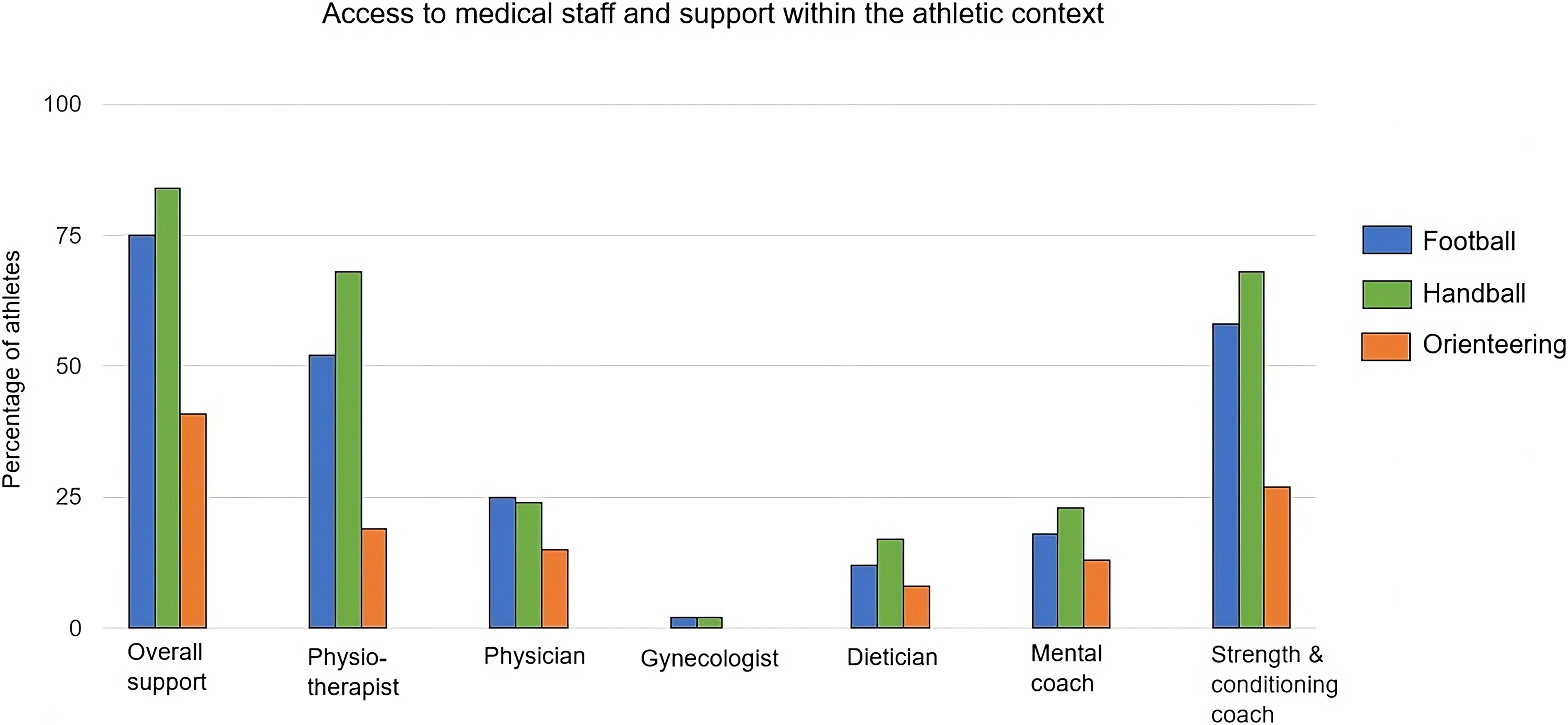
Access to medical staff and support, percentage of athletes in football, handball, and orienteering. All athletes, n = 648.
Knowledge concerning menstrual-related issues in an athletic context
The level of knowledge perceived by the athletes, divided into the different types of sports is displayed in Table 5. Most athletes regardless of sport perceived their own knowledge about menstrual-related issues in an athlete context as fair or even good/very good. For all sports, athletes whose main coach was a woman were aware of these issues to a greater extent (very good or good) than those who had a male main coach (34% vs. 2%, p < 0.001, w = 0.42).
The sex of the main coach and perceived level of knowledge about menstrual-related issues in an athletic context, divided into sports (football, handball, and orienteering), n = 648.
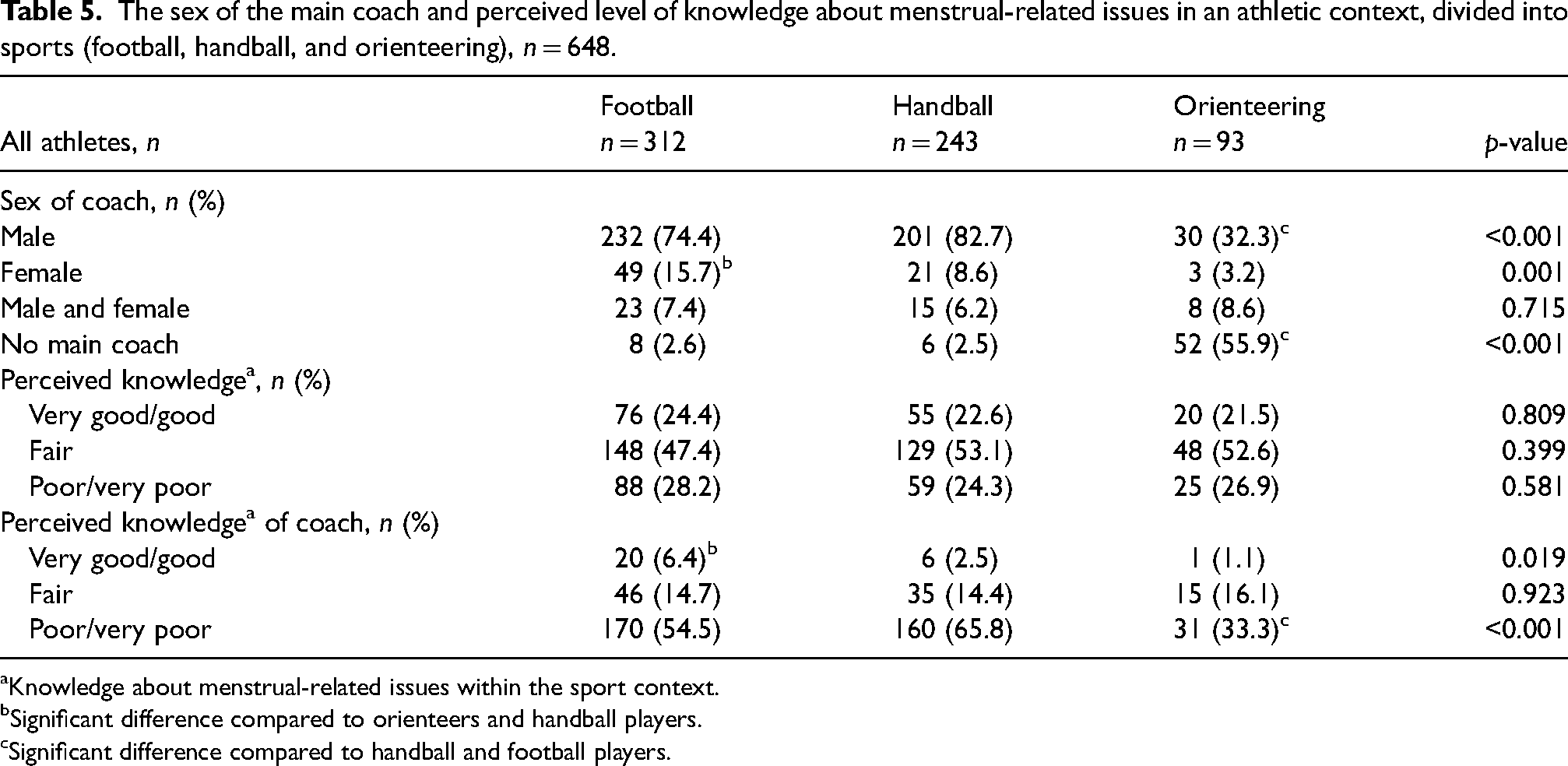
Knowledge about menstrual-related issues within the sport context.
Significant difference compared to orienteers and handball players.
Significant difference compared to handball and football players.
Acquisition of knowledge
Most of the athletes acquired their knowledge concerning MC-related issues in an athletic context on their own, with no differences between sports (Figure 4). With respect to those who had acquired such knowledge within the athletic community itself, the largest proportion was among orienteers (22%, n = 20), as compared to 5% (n = 16) and 4% (n = 10) among the football and handball players, respectively (p < 0.001, w = 0.25).
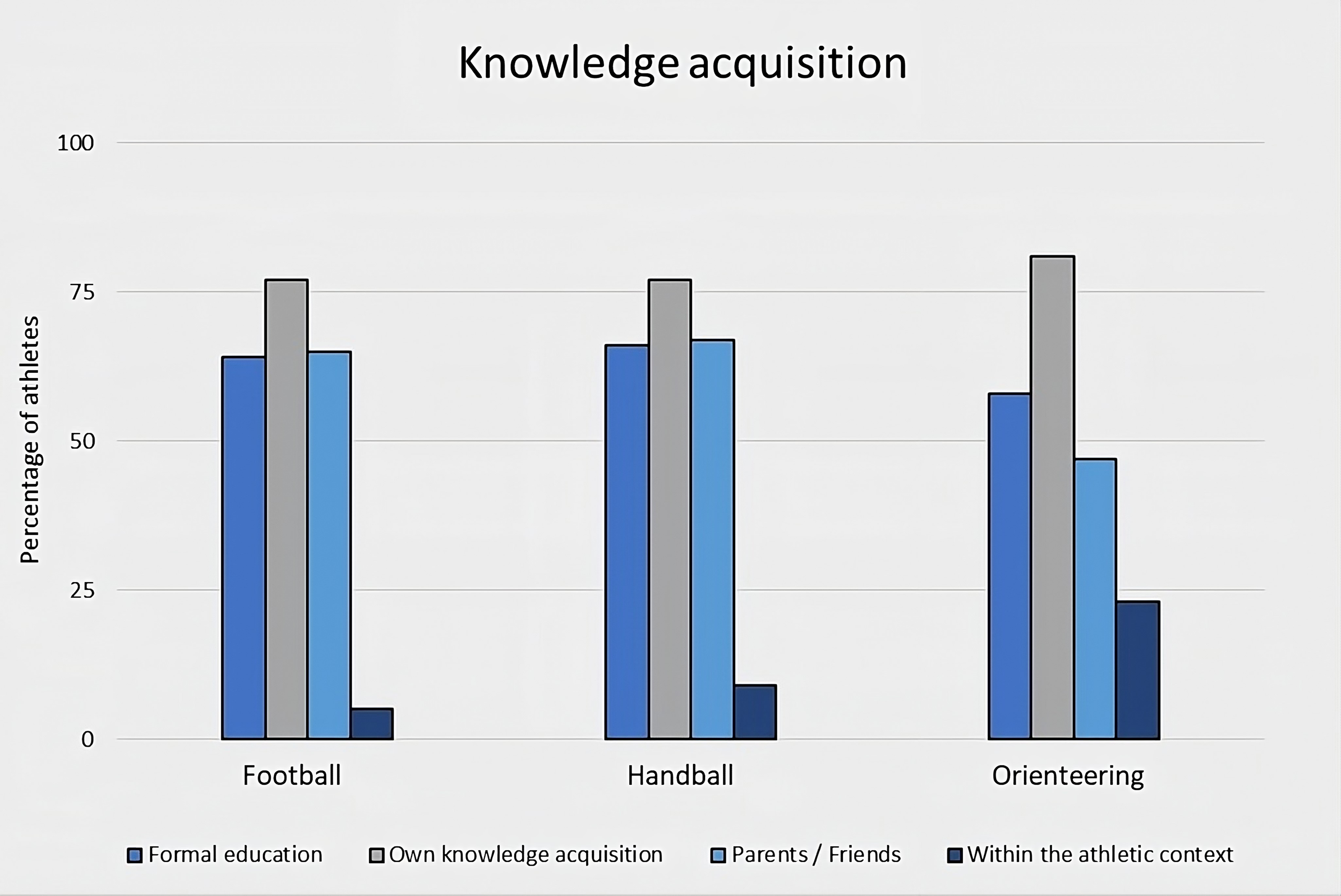
Knowledge acquisition about menstrual-related issues within the athletic context in football, handball, and orienteering. All athletes, n = 648.
Overall, the football players (43%, n = 133) and the orienteers (42%, n = 39) agreed to a greater extent (p = 0.167, w = 0.07) than the handball players (35%, n = 85) that discussion of MC related issues within the sports community is taboo.
Discussion
Our present findings reveal significant differences between the perceived influence of the MC and HCs on performance, as well as the associated knowledge and support provided to athletes participating in football, handball, and orienteering. More than half of the orienteers planned their training based on the MC, whereas relatively fewer football and handball players did so. The use of HCs was common among all female athletes, but to a lesser extent among orienteers compared to football and handball players. In addition, relatively more orienteers used progestin-only HCs compared to the other two sports. Football and handball players received more support compared to the orienteers, primarily from a physiotherapist and strength and conditioning coach in addition to the main coach.
Menstrual-related pain and PMS were common in all three sports, even if the football players tended to experience pain more often than the handball players and the orienteers. Most athletes deal with their menstrual-related pain with over-the-counter painkillers. However, the orienteers used significantly less painkillers than the football and handball players. Although menstrual-related symptoms were common in all sports, orienteers planned their training based on their MC to a higher extent compared to football and handball players. That might be explained by a greater opportunity for an athlete in an individual sport to schedule their own training than athletes in team sports. Furthermore, the football players believed to a lesser extent that their MC had an impact on the training compared to the other athlete groups. In a previous study, 8 only 7% of elite endurance athletes reported that they considered the MC when planning their training.
Use of HCs is common (40%–70%) among female athletes,6,8–10,12,18 and seems today to be even more common than in the general population. 14 Planning training and competition with respect to HC use, and to refrain from training and competition due to menstrual pain was less common among HC users compared to non-HC users. Furthermore, there was no difference between sports among HC users in this regard. These results indicate that HCs is efficient in alleviating MC-related symptoms.
However, the orienteers used HCs to a significantly lower extent compared to the football and handball players. There are few previous studies comparing the use of HCs in sports. Nolan et al. 12 compared rugby players and powerlifters but did not detect any difference in HC use between these sports. To investigate the reason for this difference, more in-depth interviews with the athletes need to be conducted. The orienteers also used progestins to a larger extent than the football and handball players. High use of progestins has also been reported in cross-country skiers and biathletes, 9 while others have shown combined HCs to be the most common type among female athletes in various sports.6–8 In the current study, the highest frequency of combined HCs was seen among football players. The knowledge of the response to different HCs in athletes is still sparse. 2 More studies in various sports are needed to explore the effect of HCs containing different types and doses of synthetic hormones on physical performance and well-being in female athletes.
MC and HC-related issues have been reported to be a taboo topic in the sports community8,15,19 and few female athletes discuss these matters with their coach.8,15 Female coaches are not so common in the sports community, and we have previously reported a dominance of male coaches in Norway and Sweden, especially in team sports. 15 In this study, orienteers reported to have fewer female coaches, but this could be explained by the fact that many of them had no main coach at all, which most of the football and handball players had. A greater openness to discuss menstrual-related issues has been reported if the coach is a woman.8,15,20
Besides the coach, most athletes had other support such as a strength and conditioning coach and/or medical personnel. Previous studies have reported it is more convenient for female athletes to turn to the medical team instead of the coach to discuss MC or HC-related issues.11,15 The handball players had overall most support while the orienteers had the least. Access to a physiotherapist and strength and conditioning coach were the most common professions in the medical team and might be explained by the high risk of acute injuries in team sports like football and handball.21–24 Knowledge of female health issues in relation to physical performance has been shown to vary even among medical personnel.25,26 Therefore, it is important that the support team also get sufficient knowledge through educational efforts.
Athletes’ perceived knowledge about the MC and HCs in relation to training and performance differed between sports. The orienteers perceived their knowledge to be higher compared to football and handball players. Orienteers also acquired their knowledge within an athletic context to a higher extent compared to the others. However, the orienteers were older and on a higher performance level than the football and handball players, which could explain the better knowledge. Athletes whose main coach was a woman had also more knowledge about the MC and HCs compared to athletes with a male main coach.
This is the first study comparing three sports in a large cohort exploring the influence of the MC and HCs on training and performance. Limitations such as the risk of misinterpretation of the questions or as recall bias as previously described.10,15 Despite a large material, there is a risk of limited statistical power when analysing the material divided into sub-groups.
Conclusion
In our relatively large cohort, we observed considerable differences between orienteers compared to football players and handball players with respect to their perceptions of the influence of the MC and HCs on training and performance, as well as concerning knowledge and support. Orienteers planned their training related to the MC to a larger extent than the athletes involved in the other two sports. At the same time, the football and handball players used HCs to a greater extent than the orienteers, and relatively more orienteers used progestin-only HCs. The football and handball players had a main coach and access to a support team more often than the orienteers, whereas the orienteers had more knowledge concerning female health issues, even if the knowledge in this area was generally low. These findings indicate a need for more knowledge about the influence of the MC and HCs on training and performance, as well as improved access to and organization of support systems around these issues, adapted to the requirements of the different sports.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Swedish Olympic Committé.