
Abstract
The Female Athlete Triad (Triad) and the more encompassing Relative Energy Deficiency in Sport (RED-S) are disorders caused by low energy availability (LEA). LEA is a state of insufficient energy intake by an athlete relative to their energy expenditure. Persistent LEA results in the deleterious consequences to health and performance that comprise RED-S. With respect to both the Triad and RED-S, researchers have called for more education of those involved with sport, particularly coaches, to help reduce the incidence of these disorders. Recent studies have shown that as few as 15% of coaches are aware of the Triad, with up to 89% unable to identify even one of its symptoms. RED-S is a more recently established concept such that coach knowledge regarding it has only begun to be assessed, but the results of these initial studies indicate similar trends as for the Triad. In this review, we synthesize research findings from 1986 to 2021 that pertains to LEA and RED-S, which coaches should know so they can better guide their athletes.
Keywords
Introduction
Since 1992, the term Female Athlete Triad (Triad) has been used to describe the combination of amenorrhea, osteoporosis, and disordered eating1,2. In the years following, the Triad has been studied extensively and recently has been redefined to better represent the scope of the disorder. As of 2007, the Triad is described as a disorder that features menstrual dysfunction, altered bone health, and low energy availability (LEA) with or without an eating disorder 3 . Low energy availability refers to the state of insufficient energy intake by an individual relative to their energy expenditure 4 .
Cohorts other than elite and competitive female athletes, such as males, recreational athletes and exercisers (using the terminology of McKinney et al. 5 ), can also present with Triad related-symptoms4,6–35. In 2014, the International Olympic Committee produced a consensus statement suggesting that a new term be adopted that encompasses the full scope of this symptomology36–38. The new term, Relative Energy Deficiency in Sport (RED-S), expands on the previous Triad framework by including males, recreational athletes, and exercisers as populations that are susceptible to the LEA-related symptoms. RED-S also includes a range of adverse health and performance outcomes that stem from an LEA state in addition to the already established menstrual irregularities and impaired bone health seen in the Triad framework. While debate persists on adoption of the new term, proponents of both its Triad and RED-S agree that both disorders stem from LEA 39 .
Recent studies indicate a high prevalence of LEA in athletes; however, the challenge of measuring LEA in free-living athletes implies that current estimates are spuriously low 27,40–43. Similarly, due to its wide range of outcomes, which will be described further in a later section, RED-S is thought to be more prevalent than is currently reported 44 . Given their adverse impact on health and performance, efforts are underway to better understand and prevent these disorders. A lack of coach knowledge regarding these disorders and their damaging consequences is thought to contribute to their prevalence. Several studies have assessed the knowledge of coaches regarding the Triad, including its signs and symptoms and its detrimental consequences to athlete health and performance45–54. Some of these studies reported that fewer than one-quarter of coaches are aware of the Triad50,52. Furthermore, coach knowledge varies by region, gender, and sport-type45,47,49,53,54. Studies investigating coach knowledge of RED-S are only just beginning to emerge, but they report similar trends as those of the Triad 55 . The high prevalence of the Triad and RED-S coupled with the lack of coach knowledge regarding these disorders has motivated researchers to call for more education regarding LEA and its damaging consequences43,56.
In this review, we synthesized evidence from peer-reviewed studies published between 1986 and 2021 that we believe is essential for coaches to know so they can better guide their athletes and prevent LEA. Because it is generally accepted that the Triad represents three specific symptoms of RED-S, we henceforth refer primarily to RED-S, except when referring to studies that were specific to the Triad. This review aims to provide coaches with the scientific basis underlying the concepts of LEA disorders. Specifically, we provide an overview of RED-S, discuss its performance and health outcomes, describe nutritional guidelines to help prevent LEA, and propose strategies for monitoring and supporting athletes at risk of LEA.
The female athlete triad and relative energy deficiency in sport: diagnosis, mechanism, and prevalence
Originally, the diagnosis of the Triad required the athlete to present with the three following conditions: disordered eating, absent menstruation (amenorrhea), and osteoporotic bones. Nowadays, a female presenting with low energy availability, hormone dysfunction, or low bone mineral density, either alone or in combination, is considered to be at risk of the consequences of the Triad
57
. Furthermore, athletes are considered to exist on a continuum that spans from optimal to pathological health and sub-optimal performance (Figure 1)
58
. Males can likewise show the signs and symptoms of Triad, with the exception of irregular menstrual patterns11,24,26. Accordingly, the International Olympic Committee and other sport governing bodies have suggested the adoption of the more inclusive term, RED-S37,38. RED-S is defined as
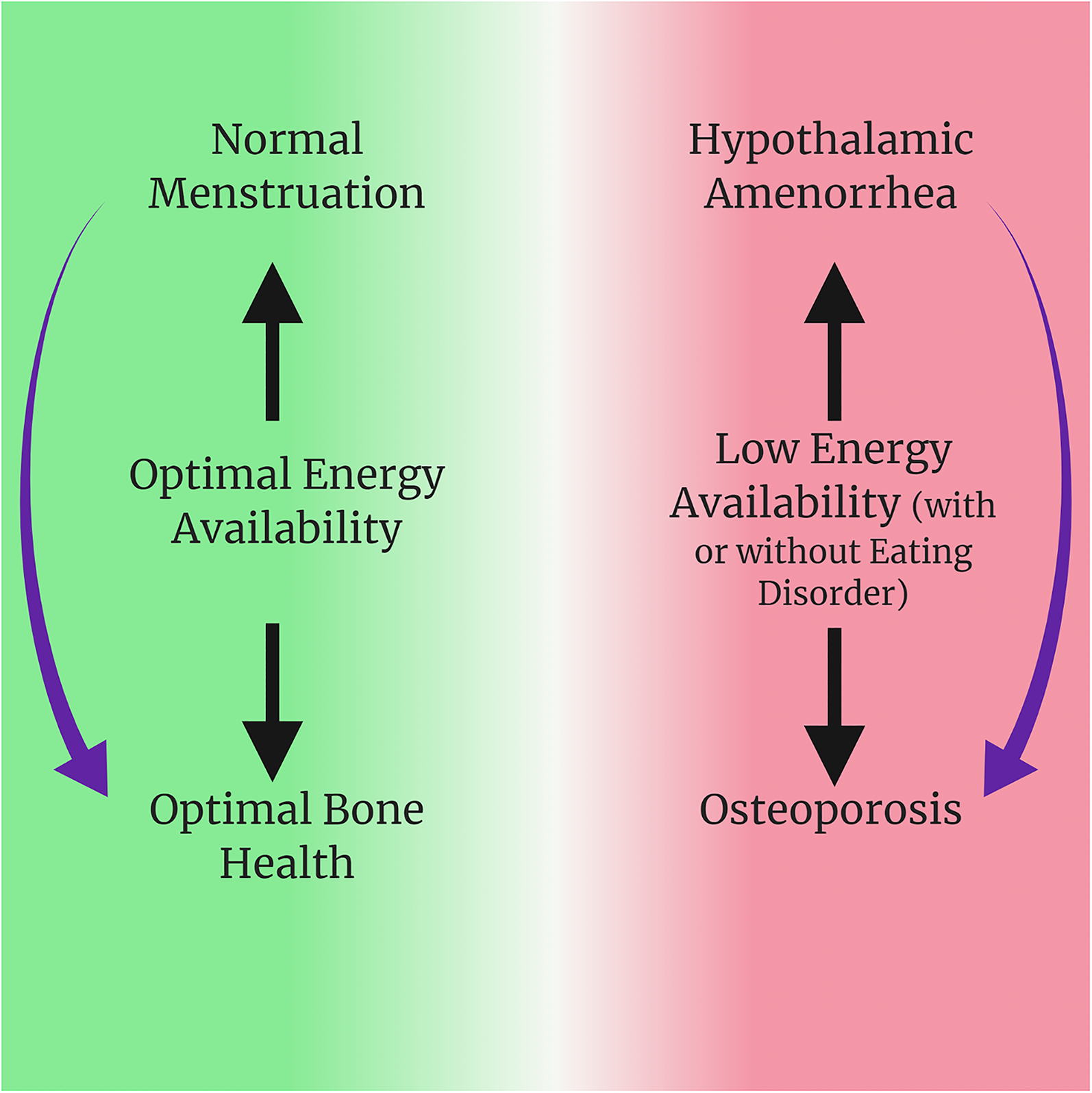
The signs of the female athlete triad exist on a continuum from healthy to pathological, as demonstrated by the green to red transition, and they are causally associated in the manner indicated by the arrows.
Several challenges hinder the diagnosis of RED-S. The first challenge is the spectrum of dysfunctions that can present and that different individuals exhibit different subsets of dysfunctions (discussed in more detail below). The second challenge is that assessment depends in part on questionnaires and food records completed by the individual. Noncompliance or inaccurate responses provided by the individual can impair accurate assessment24,27,63,65. The third challenge is that RED-S-specific questionnaires continue to be developed and validated. Questionnaires currently used for diagnosing RED-S were adapted from those used for diagnosing clinical eating disorders. Since then, several questionnaires have been developed, such as the Low Energy Availability in Females Questionnaire and the Female Athlete Screening Tool6,60,64. While these questionnaires were useful for diagnosis of RED-S in females, questionnaires for males are just beginning to emerge. For example, the Androgen Deficiency in the Aging Male Questionnaire and the Exercise Dependence Scale have been found to aid the diagnosis of RED-S in males59,66. Recent studies have shown that using a multipronged approach involving questionnaires, DXA scan, and energy intake assessment have proven useful in diagnosing the Triad and RED-S6,59,64,66. Additional studies will be needed to validate RED-S diagnostic procedures more comprehensively.
LEA is the underlying mechanism that causes RED-S 39 . Energy availability is the energy remaining for physiological function once energy expended during exercise has been taken into account 67 . It is calculated using the following equation: Energy Availability = Energy Intake – Exercise Energy Expenditure 38,39,67, with each term in the equation expressed in units of kilocalories per kilogram of fat-free mass. Those with energy availabilities of less than 30 kcal per kilogram of fat free mass are at risk of LEA41,55,68–70. It has been suggested that males can tolerate lower energy availabilities based on the higher energy needed by the female reproductive system, but limited evidence exists to support this contention68,69,71–77. Additionally, a rigorously defined threshold does not yet exist because energy availability is difficult to measure in free-living individuals27,39,56,63. LEA is further classified as advertent or inadvertent. Advertent LEA refers to the conscious and deliberate restriction of energy intake or increase in energy expenditure. Inadvertent LEA refers to the unwitting and unintentional failure to consume sufficient energy 38 .
Because of the difficulties in diagnosing LEA and RED-S, estimating the prevalence of these conditions within athletic populations is challenging. Estimates are based on inferences from surrogate measures, such as the prevalence of injuries, physiological dysfunction (i.e. amenorrhea or oligomenorrhea), and physical and behavioural signs, which are commonly associated with LEA. These challenges notwithstanding, the prevalence of LEA and RED-S are likely to be higher than is reported 78 . More than a quarter of athletes are at a moderate to high risk of LEA27,42,79–81, while up to 79% of athletes in certain cohorts may have RED-S34,82–93. Those competing in so-called “lean sports”, in which a higher power-to-body-mass ratio is thought to benefit athletic performance34,36,94, are at higher risk. Such sports include athletics (track and field), combat sports (e.g. wrestling and judo), cycling, gymnastics, rowing, synchronized swimming, and triathlon. One study estimated that in a cohort of female athletes, 56% of gymnasts, 49% of cross-country runners, and 43% of swimmers were at a moderate to high risk of LEA 79 . In a sample of collegiate distance runners, 45% of males and 41% of females were estimated to have energy availabilities lower than 30 kcal/kg fat-free mass 76 . However, the risk of LEA extends to athletes who might not be stereotypically thought of as high risk. For example, 31% of sprinters at a Canadian university presented with LEA at pre-season testing and 54% presented with at least one LEA symptom at post-season testing 42 . For the Triad, Heikura et al. estimated that 34%, 26%, and 6% of 39 female athletes presented with one, two, or three symptoms of the Triad, respectively 27 . Observational evidence indicates a relationship between LEA risk and its consequences. For example, cross-country runners in the moderate-risk category for LEA were twice as likely to sustain a bony stress injury, and those in the high-risk category were four times as likely to sustain bony stress injuries 79 . These results emphasize the need for all coaches to be knowledgeable about LEA and RED-S and be vigilant in monitoring their athletes for its presence, even coaches in sports not traditionally considered to be within the “lean sport” category.
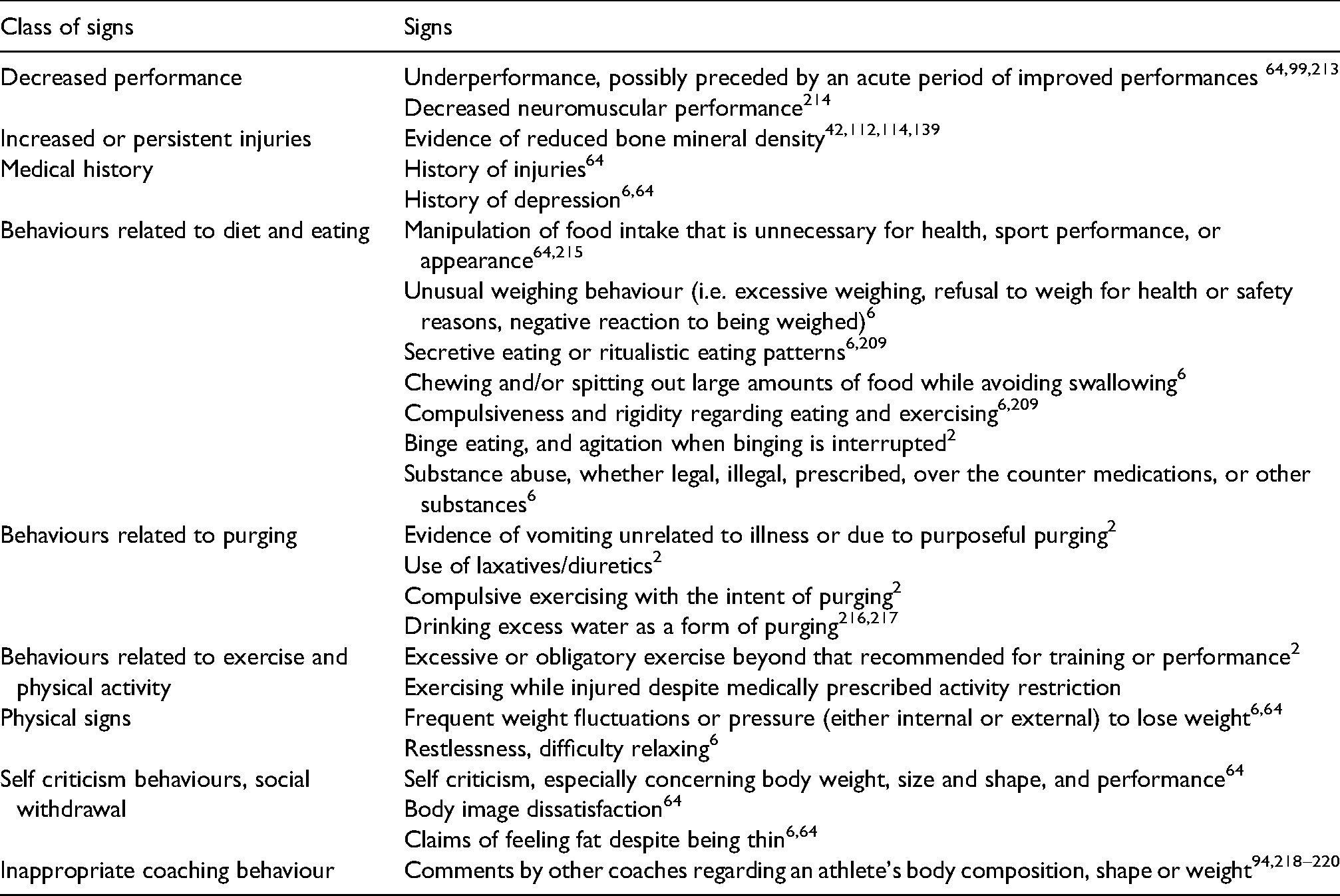
Common signs of RED-S.
Performance and health impairments of LEA and RED-S
The key to an athlete's development is the quality and quantity of training coupled with their ability to adapt to the training. Coaches must understand the intricate interrelationship between these factors and performance. Coaches understandably tend to focus on the training load part of the equation: Achieving ever greater training loads is important for improving athletic performance, especially for athletes with prolonged training histories 95 . Furthermore, training loads are relatively “easy to see.” Coaches observe athletes training and commonly collect objective data through portable measurement devices such as heart-rate monitors and GPS wristwatches. Higher training loads are implicitly assumed to represent better training.
Despite the perceived benefits to performance from higher training loads, they will only benefit performance if the athlete is capable of physiologically adapting to them. The adaptability of the athlete is much more challenging to assess, with indirect measures such as resting heart rate, athlete perceptions, and heart-rate variability commonly used in practice 96 . Proper nutrition, sleep, stress management, and recovery modalities such as massage are prescribed to maintain or enhance an athlete's adaptability 96 . However, determining whether the optimal balance of training load and recovery enhancement has been achieved is challenging. Additionally, the coaches’ abilities to observe athletes are generally limited to the sporting environment. If the athlete participates in other sports or activities, then these training loads will accumulate unseen, thus challenging the coach's ability to accurately monitor training loads. Currently, studies regarding monitoring training loads have been limited to single-sport situations, and there is currently no perfected practice for monitoring multisport athletes who interact with multiple coaching staffs.
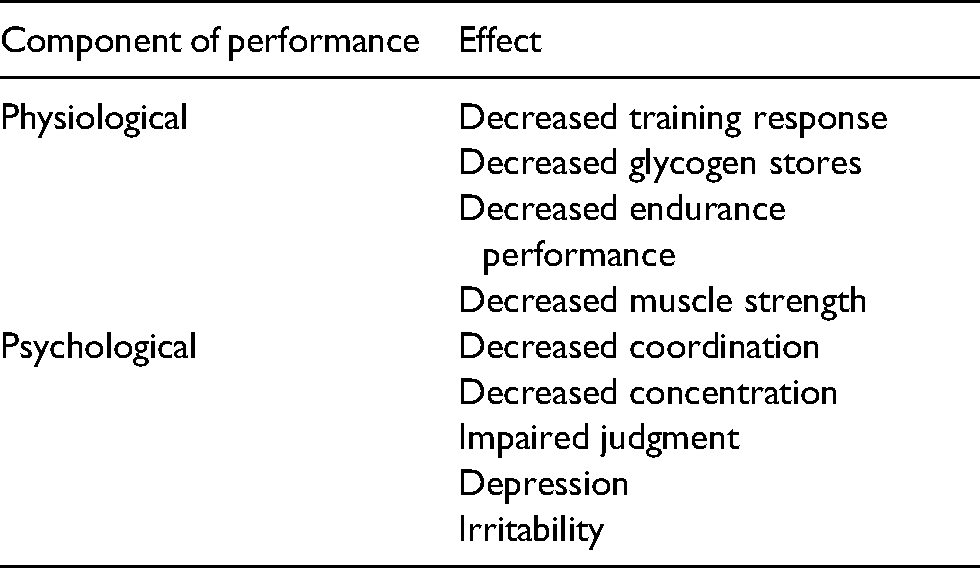
LEA limits performance by compromising the body's ability to adapt to a given training load. Table 1 lists some of the physiological and psychological performance components of LEA that present in individuals with RED-S. The list is neither exhaustive nor universal; other performance outcomes may be caused by LEA, while not all those with RED-S may experience all the listed impairments. Generally, more severe LEA and its consequences can cause lost training days due to injury or illness, and lost training days compromise performance 97 . Overall, coaches must internalize these basic considerations: proper training loads combined with adequate nutrition are two critical and inseparable factors for achieving peak athletic performance.
Beyond performance, coaches should adhere to the ethical principle that they “strive to preserve the present and future health and well-being of athletes” 101 . RED-S can have significant and potentially long-term irreversible health consequences for athletes (Figure 2). These health effects centre on three areas: hormone and metabolic function, bone health, and cognitive ability and mental health.
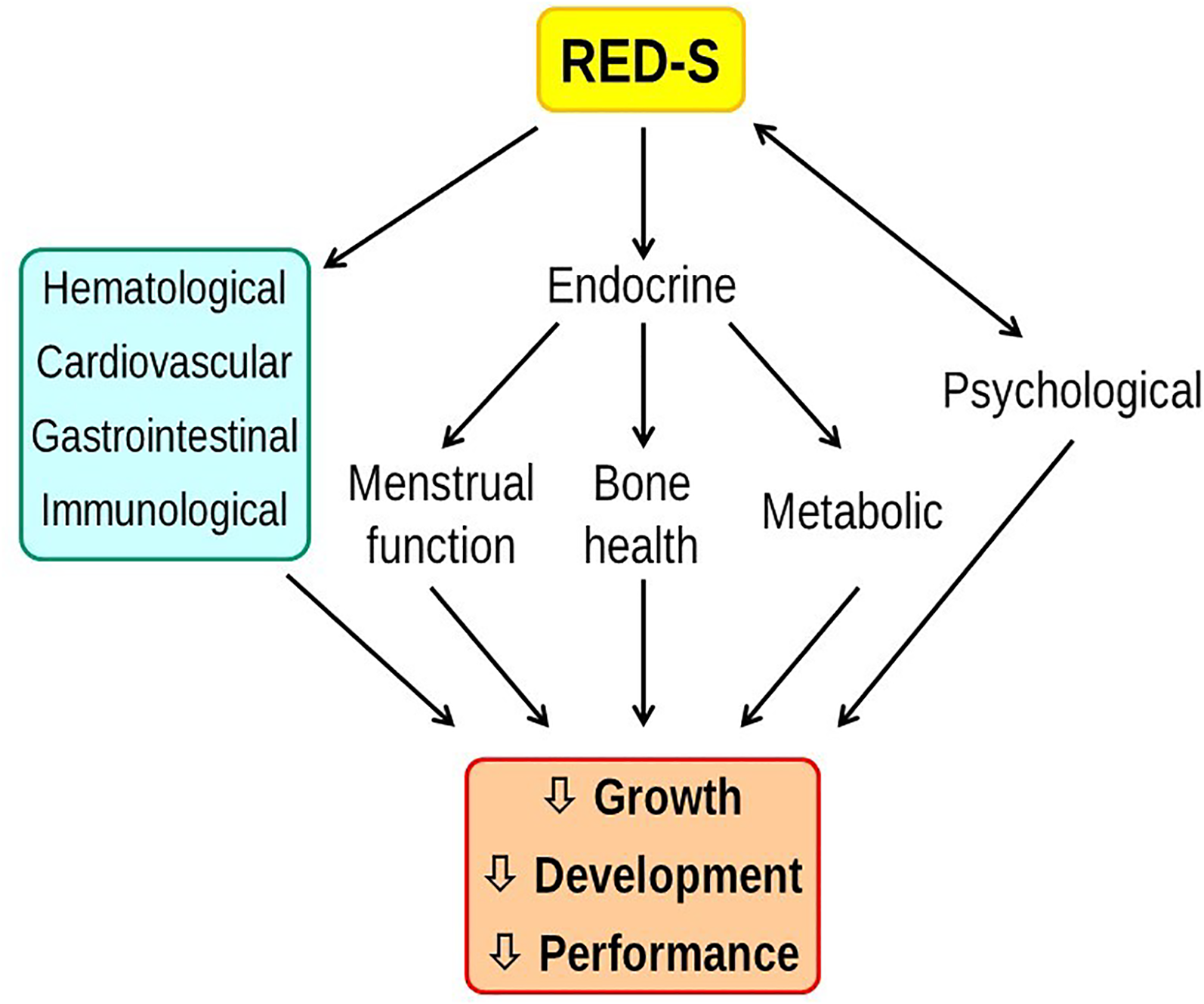
Relative energy deficiency impairs the physiological functions that support athlete growth and development, health, and performance.
Hormonal and metabolic function
Hormones are chemical messengers that help control virtually all bodily functions, including metabolism, muscle and bone mass and function, and cognitive functioning. Hormone physiology is complex, and their effects are not easily understood by those without specialized training in physiology. At minimum, coaches should know that hormone dysfunction is a hallmark of LEA disorders15,16,21,24,25,102–106. For those that seek more detail, we describe below dysfunctions with selected hormones, including estrogen, testosterone, leptin, insulin growth factor-1 (IGF-1), growth hormone, cortisol, thyroid hormone, and insulin.
Estrogen and testosterone are important for reproductive functioning and for bone health and metabolic regulation107–109. Therefore, disruptions in these hormones can have widespread detrimental consequences including enhanced injury risk. Estrogen levels in females and testosterone levels in males are lower in those with LEA compared to those who have adequate EA14,27,68,106. The hormone leptin regulates reproductive function via stimulation of gonadotropin-releasing hormone 110 . Leptin is secreted by adipocytes (fat cells) and its levels are proportional to fat mass 111 . Athletes with LEA exhibit decreased leptin levels68,74,112,113 and attendant disruption of reproductive function due to decreased gonadotropin-releasing hormone stimulation 68 .
Growth hormone is required for muscle and bone anabolism (anabolism connotes “assembly” or “building up”, as opposed to catabolism, which connotes “breaking down”). Growth hormone acts via IGF-1, which also acts to regulate growth hormone secretion 77 . Athletes experiencing LEA exhibit elevated growth hormone levels but reduced circulating IGF-1, suggesting that resistance within this pathway has developed during LEA25,68,114,115. The overall effect of these changes is decreased muscle synthesis, bone anabolism, growth, and repair.
Cortisol is primarily a catabolic hormone25,116 that acts to promote energy supply, in part through muscle protein breakdown and lipolysis (breakdown of fats). Those experiencing LEA exhibit elevated levels of cortisol, which promotes a catabolic state that can restrict muscle glycogen stores, promote proteolysis of muscle tissue and promote resorption of bone tissues25,77,116, thus increasing risk of injury and illness.
Thyroid hormone controls energy expenditure to ensure sufficient energy for growth and reproduction25,117. It is intimately tied to the reproductive hormones estrogen and testosterone. Thyroid deficiency generally leads to an energy preservation state, in which energy normally reserved for growth and reproduction is reduced and diverted to more vital functions 117 . As such, athletes in LEA states have reduced thyroid hormone levels25,68,77,115,118. These deficiencies result in decreased growth and reproductive function, which is evident when considering the amenorrheic athlete 119 . In this instance, the decrease in thyroid hormone results in a dysregulation of the intricate relationship between thyroid hormone and estrogen production, ultimately resulting in reproductive system impairments77,117.
Insulin is also an anabolic hormone: it activates glucose uptake, glycogen synthesis, protein synthesis, and inhibits protein degradation25,116,120,121. Circulating glucose is the primary source of energy in the body; blood glucose is tightly regulated by insulin and its counteracting hormone, glucagon. By promoting glucose uptake into cells, insulin works to decrease blood glucose. Insulin levels tend to be decreased in those with LEA68,74. Athletes with LEA have lower energy stores and thus a driving force exists to sustain blood glucose levels by producing and secreting less insulin 25 . Reduced insulin levels are detrimental because it allows for accelerated breakdown of proteins to sustain blood glucose and may result in reduced protein synthesis121,122. The increased breakdown of muscle may increase the risk of injury and reduce strength and performance. If the athlete is injured, the decrease in protein synthesis may potentially prolong recovery and the time taken to return to sport36,123–126.
A notable consequence of LEA is that the resting metabolic rate (RMR) tends to decrease 25 . The RMR is the energy expended per unit time by the body while in the resting state and results from processes that maintain vital bodily functions such as breathing, cardiac functioning, growth and repair, etc. In LEA, RMR is reduced such that less energy is utilized by the reproductive, growth and repair systems, and energy is conserved for functions necessary for survival127,128. LEA is associated with increased percentage body fat and muscle breakdown43,129. The relative gain in fat may seem paradoxical and the mechanisms remain poorly understood, but it has been reproducibly observed and also occurs in those with anorexia nervosa130–134. Coaches must understand the effects of LEA on metabolic rate and body composition, which underscores that simplistically restricting energy intake as a mechanism for losing weight or body fat is likely to be counterproductive.
Bone health
Peak bone accrual typically occurs between the ages of 18 and 22; however, some studies indicate further accrual into the third decade of life135–137. Athletes who have LEA tend to have altered bone density and geometry due to their inability to produce sufficient levels of regulatory hormones and for those hormones to act appropriately on their targets112,114,138–140. These hormones can act either directly (i.e. IGF-1, leptin, and triiodothyronine) or indirectly (i.e. estrogen, testosterone) on bone metabolism. In some cases of LEA, particularly those involving intentional restricted caloric intake, athletes may not get sufficient calcium and vitamin D, both of which are essential to generating new bone85,141,142 As a result, 12–45% of athletes with LEA tend to have lower bone mineral density, between one and two standard deviations below the population average38,114,139,143,144. Depending on the duration of their LEA, athletes may also present with altered bone geometry compared to their healthy peers, particularly decreased trabecular area in weight-bearing bones such as the pelvis 38,139,140. The lower bone density and weakened structure can lead to increased risk of bony stress injuries that in turn can lead to stress fractures, which results from imbalanced bone resorption and bone formation79,114,145. Such scenarios are especially problematic for female athletes because they tend to be at higher risk of developing bony stress injuries compared to their male counterparts due to anatomical and hormonal differences146–149. Athletes sustaining these injuries lose training time. Additionally, recurrent bony stress injury history is predictive of future bone-related injuries150–154.
Cognitive ability and mental health
Those with LEA exhibit decreased cognitive ability, decreased attention, and higher risk of anxiety 34 . A survey of 1000 participants admitted to a Boston hospital with sport-related injuries found that those classified as having LEA were 4.3-times more likely to report impaired judgment, 1.6-times more likely to report feeling uncoordinated, and twice as likely to report problems concentrating 81 . In addition, those experiencing iron deficiency as a result of poor nutrition habits associated with RED-S were more likely to present with cognitive impairments, depression, and anxiety due to hypothyroid-like states seen with LEA 155 .
Nutritional practices to help prevent LEA and RED-S
The most effective approach to mitigate the adverse performance and health consequences of RED-S is through proper nutrition. Many academic and sport organizations, including the International Olympic Committee, recommend that coaches educate themselves about proper nutrition. We further emphasize that athletes and their parents should also be educated in sports nutrition. A detailed review of sport nutrition is beyond the scope of this review, but we direct the reader to the following credible and readily available scientific references:
American College of Sports Medicine, Academy of Nutrition and Dietetics, and Dieticians of Canada joint position stand on Nutrition and Athletic Performance (2016)
156
International Society for Sport Nutrition Exercise & Sports Nutrition Review Update: Research & Recommendations (2018)
157
Coaches working with youth athletes are further referred to review articles focused on youth athletes (cf. refs 158,159). Drawing upon these sources, we discuss below some general principles for ensuring sufficient nutrition for athletes.
First, athletes must obtain sufficient total energy (Calories) from food. Energy requirements depend on sex, body mass, biological age, and energy expenditure from training and competing. Pubescent and pre-pubescent children have greater energy requirements due to the increased energy need to support growth. The accepted daily energy requirement for female athletes aged 11 to 18 is approximately 2200 kcal, while that for males of the same age range is 2500–3000 kcal156,158. Following puberty, the energy needs of a person will show a minor increase, primarily due to the increase in body mass160–162. These energy needs are generally maintained through early adulthood until approximately 40-years of age, at which point they steadily decrease to 2000–2500 kcal in the elderly years158,160–162. Daily energy needs vary considerably across individuals and depend proportionally on body mass and physical activity levels158,160,161. We therefore emphasize that the cited numbers serve as a general guide only and that those performing higher levels of activity will have correspondingly higher energy needs.
Second, athletes must obtain sufficient macronutrients, i.e., carbohydrate, fat, and protein. Athletes are advised to consume 5–12 g of carbohydrate per kilogram body mass per day, depending on the nature of their training activities141,163. Those training at moderate-to-high intensities for 1–3 h per day should consume closer to 5–8 g per kilogram body mass, whereas those training at moderate-to-high intensities 4–5 h per day should consume closer to 9–12 g per kilogram body mass164–166.
Athletes may consume inadequate carbohydrate for several reasons. First, carbohydrate-restricted diets are popular for weight loss76,167. Second, athletes may restrict carbohydrate as a stimulus to promote enhanced fat oxidation and endurance. While some studies show that low-carbohydrate diets can spare glycogen and enhance fat oxidation, these adaptations fail to improve performance 141 . In fact, performance often decreases due to impaired ability to use carbohydrate as a fuel, which is necessary for exercise at higher intensities. Third, some athletes may inadvertently limit their carbohydrate intake by avoiding certain foods due to gastrointestinal distress168,169. Such impairments to carbohydrate intake can lead to lower quality training and negatively impact bone mineral density by potentially increasing concentrations of molecules associated with bone resorption141,170,171.
Protein is essential for muscle repair and other anabolic processes. Athletes should consume 1.2–1.7 g of protein per kilogram body mass per day141,163. If an athlete is injured, it is recommended that the athlete consumes 1.2–1.5-times more protein than usual124,126,163,172 because doing so can help accelerate recovery and prevent muscle breakdown due to inactivity 126 . In general, athletes consume close to the recommended protein requirements; however, in the case of those who follow restricted diets (e.g. vegan, gluten free), athletes may not obtain enough141,173,174.
Fat intake is important because lipid molecules are critical components of cells and they contribute to numerous aspects of physiology including the immune response, absorption of fat-soluble vitamins (A, D, and E), and hormone regulation 17 . It is therefore suggested that fat intake be approximately 15–30% of daily total caloric intake141,163. Generally, eating a well-balanced diet will result in sufficient fat intake 156 . However, fat intake may be inadequate in those who consume inadequate total energy or who follow restrictive diets141,173,174.
Third, athletes must obtain adequate micronutrients such as minerals and vitamins. While there are many micronutrients, we focus on the following three minerals: Calcium, phosphorus, and iron. Calcium and phosphorous are critically important for bone formation because bone material consists of the compound calcium phosphate. During puberty, when the rate of bone accrual is heightened, both minerals are needed in higher amounts. Athletes should consume higher amounts of calcium because transient periods of minor bone loss followed by bone growth occur in response to physical activity57,139,175,176. Additionally, calcium is important for nervous system functioning and muscle activation 177 .
Iron is an essential mineral involved in hemoglobin synthesis, thyroid metabolism, and energy production178–181 Those deficient in iron typically exhibit extreme fatigue, decreased aerobic performance, and impaired immune functioning178,181. Iron deficiency is common in athletes, particularly those competing in endurance sports. Prevalence rates range from zero to 17% in males and 24–42% in females. However, some studies report that up to 65% of males and 86% of females present with deficient iron levels181–183.
Vitamin D is critical to bone formation due to its integral role in calcium absorption. Without it, sufficient calcium cannot be absorbed to maintain proper bone health. Vitamin D is also important to maintaining nervous system and muscular functioning141,163. Athletes living and training in certain geographic regions, specifically in areas above 40° North, may get insufficient sunlight141,184. Sunlight is a major factor for Vitamin D synthesis, such that supplementation may be required for those who get insufficient exposure to sunlight141,184. Furthermore, it has been shown that Vitamin D deficiency is more prevalent in the winter and spring seasons compared to summer and fall 184 . Food sources rich in Vitamin D include fortified dairy products, egg products, and fatty fishes 141 .
National food guidelines provide practical recommendations for consuming sufficient nutrition. For example, national nutrition guidelines commonly emphasize eating plenty of fruits and vegetables, choosing whole grain foods, and eating sufficient protein 185 . In addition, it is recommended to limit the consumption of processed foods in favour of home-cooked meals 185 . Food that is less processed contains more vitamins and minerals for a given number of calories 186 . Moreover, including a broad variety of foods within the diet is recommended 156 . An idea to promote variety in meals is to make the meal as colourful as possible 187 . Implementing this rule of thumb associates with healthier food choices and decreased consumption of sugary foods 187 . Consuming diverse foods maximizes the chances of consuming sufficient micronutrients and antioxidants 156 . Proper hydration is important because dehydration can impair performance and recovery from training188–190. Water is the recommended drink of choice; consuming sugary drinks and alcohol should be limited because of their deleterious effects on performance in the short term and health in the long term 163 .
Fourth, athletes should eat the right foods at the right time. Effective timing ensures not only that an athlete is properly fueled for workouts and competition, but also recovers efficiently from the workloads. For pre-training or pre-competition nutrition, athletes should consume approximately 1–4 g of carbohydrates per kilogram body mass (normally around 200 g of carbohydrates), about 10–30 g of protein (depending on whether the exercise is more endurance focused or power/resistance focused), and limited fat to avoid gastrointestinal distress141,163. Meals should be consumed one to four hours prior to training or competition, with the time proportional to the size of the meal 165 . Post-training, athletes should consume about 60–120 g of carbohydrate within 30 min of exercise to promote glycogen replenishment141,163. In addition, it is proposed an “anabolic window” exists up to 48 h after exercise, during which protein intake is likely most effective in enhancing muscle protein synthesis and impairing muscle breakdown. It has therefore been recommended that athletes consume 20–30 g of protein sometime between one hour before training to one hour after training156,163,191,192. While this consumption of protein in close proximity to training is encouraged by the American College of Sports Medicine and the International Society of Sports Nutrition156,157, evidence exists that total protein intake over 24-h periods may be more influential than the timing of protein intake to enhancing muscle protein synthesis193,194.
Throughout a competitive season, training loads are commonly periodized in order to maximize sport adaptation195,196. Phases generally include preparatory, pre-competition and competition phases, which vary in training load durations and intensities. Likewise, the nutritional demands of each of these phases will vary with the demands of the training sessions. As such, it has been suggested that nutrition periodization may be crucial in some sporting environments to help maximize adaptation165,197–200. Macro-periodization refers to month-to-month nutritional strategies, whereas micro-periodization refers to within-day or week nutrition. Due to complexities of various training programs, no single optimal strategy can be prescribed. However, some suggested strategies that may be relevant over a wide range of sports include reducing the amount of fibrous foods within 1–2 h of training sessions to avoid gut disturbances, prioritizing appropriate carbohydrate and protein intake immediately following sessions, and incorporating snacks throughout a 24-h period to avoid the depletion of energy stores.199,200
Finally, coaches must understand that body composition management should be undertaken only for elite-level athletes using scientifically sound approaches assisted by qualified professionals 94 (Figure 3). Indeed, losing weight is neither easy to achieve nor necessarily beneficial because of the compensation in resting metabolic rate, the detrimental effects of reduced carbohydrate on performance, and the loss of muscle mass. Hence, any attempt to lose weight must be informed by these consequences, and evidence-based guidelines are available for doing so 201 . For example, adequate protein intake is essential to support protein synthesis and maintenance of muscle mass. Indeed, for those in a slight energy deficit, increasing protein intake helps preserve muscle mass123,197,202,203. In addition, the frequency of protein consumption should increase 201,203,204. By spreading protein intake throughout the day, it is thought that a sufficient pool of protein and amino acids will be available to support protein synthesis201,203,205,206.
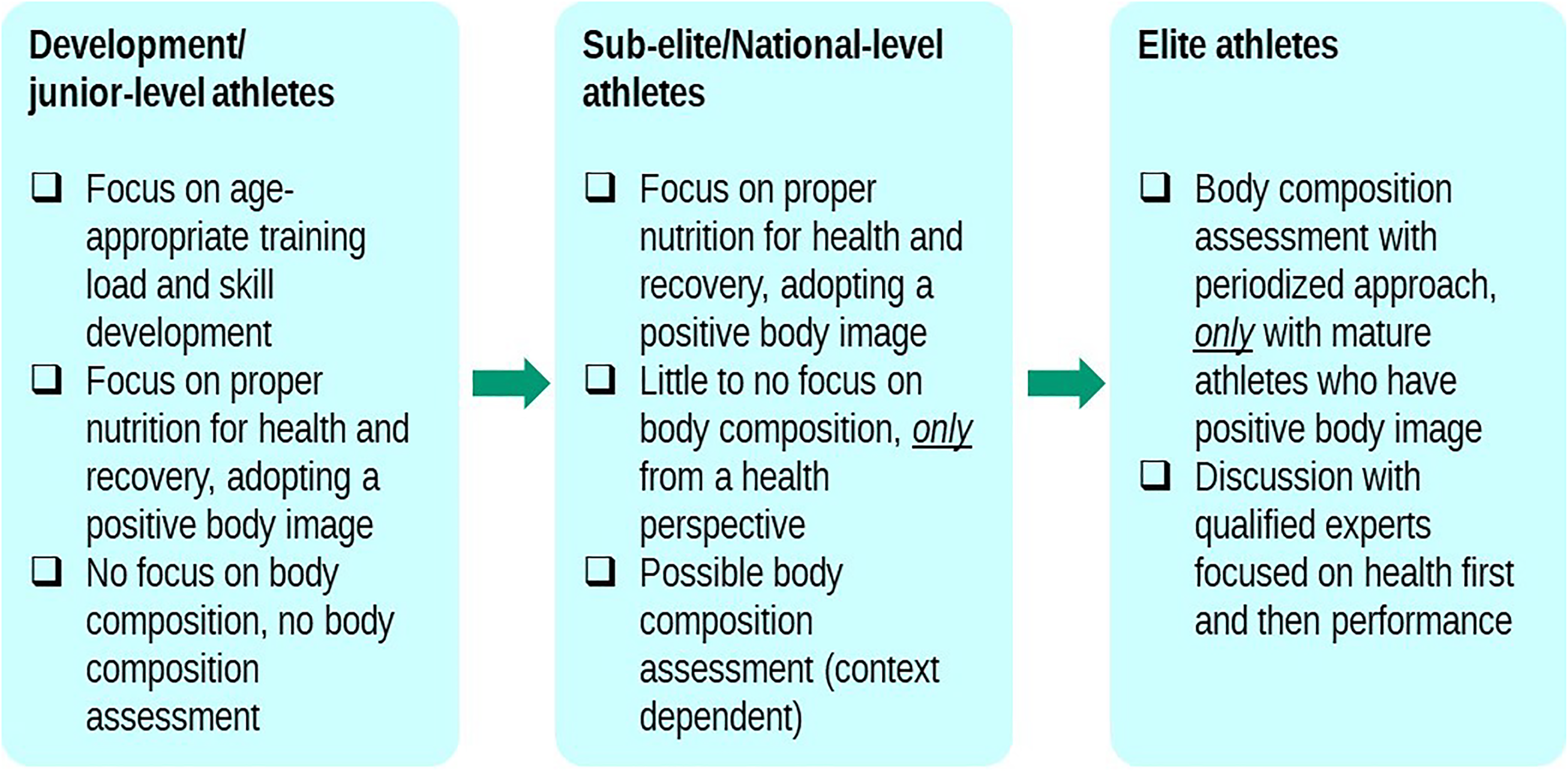
Guidelines for nutrition and body composition across the stages of athlete development. Adapted from Ackerman (2020) 206 .
Monitoring athletes for risk of LEA
To help athletes avoid the pitfalls of RED-S, coaches should be aware of the signs and symptoms indicating those at risk of LEA. Because RED-S can affect multiple organ systems, many signs and symptoms can manifest, which can make detection challenging. One particularly prevalent sign of RED-S is that of decreased performance. Some athletes may initially experience a temporary period of improved performance prior to a prolonged period of underperformance. The degree of performance hindrance can range from minor to severe. Other noteworthy signs include injury and illness. Athletes with LEA are at higher risk of sustaining stress fractures and muscle strains, and report illnesses more frequently compared to their peers64,79,207.
Aspects of an athlete's medical history may associate with a higher risk of RED-S. A plethora of behavioural changes can accompany LEA. Behaviours regarding feeding and diet, exercise and physical activity, and self criticism are especially common (Table 2)6,25,38,42,64,98,208,209. The behaviours exhibited by those with RED-S may be similar to those exhibited by those with disordered eating63,81,210,211. Other signs include social withdrawal and depression6,64,212.
Importantly, athletes are likely to exhibit a unique subset of the possible signs3,38. For example, Athlete A may present with irregular menstruation, evidence of disordered eating, and have a long history of musculoskeletal injuries. Athlete B may present with minor social withdrawal, feelings of fatigue, and rigidity in their routine. For this reason, coaches should be attentive to their athletes and maintain effective communication, so that some of these patterns can be more readily identified. If an athlete begins to show some of these signs and symptoms, then coaches should immediately take steps to address and manage the problem. The next section describes management strategies for at-risk athletes.
Supporting athletes at risk of LEA
Even if preventive measures are instituted, some athletes may still be at risk for LEA, such that coaches may find themselves having to support an athlete with RED-S. The first step the coach should take in supporting an athlete at risk is to document the signs and symptoms that they have observed. The next step is to speak with the athlete (and their parents if a youth) stating that their observations are consistent with the athlete being at risk of having RED-S. The coach should then encourage the athlete to consult with a sports medicine physician, who are the healthcare professionals with specialized training needed to manage these disorders. The physician can then assess the athlete and propose an appropriate plan of action based on the athlete's needs.
There are several key points to emphasize in supporting at-risk athletes:
The earlier the plan of action is implemented, the sooner the athlete may be able to return to form, and the lower the risk of long-term impacts on physical and mental health36,43. The coach should communicate with the athlete in a manner that preserves their dignity. These conversations are personal and should be conducted privately away from other athletes101,221. Coaches should respect the athlete's autonomy; it is their choice to seek medical attention. Coaches can merely encourage the athlete to seek medical attention
101
. Coaches must respect their scope of practice; they are not medical professionals, and they cannot diagnose illnesses, injuries, or disorders
222
.
For athletes with LEA, effective coach-athlete (and, if appropriate, coach-parent) communication is imperative. The communication style and methods employed by the coach can have negative or positive effects. Negative coach commentary regarding the athlete's performance, body composition, or attitude may propel the athlete to adopt pathological habits to attempt to reduce the negative commentary94,218–220,223. In contrast, positive commentary used to support an athlete can assist them to avoid pathological behaviours224. Indeed, it appears that carefully considered word choices and appropriate conflict resolution methods are beneficial for supporting athletes. Coach communication can be difficult to navigate, and coaches often use a mix of positive and negative strategies224. However, strategies for positive coach-athlete/parent communication have been proposed, such as encouraging open dialogue, not dismissing or denying athlete concerns, and encouraging the athlete to seek medical advice particularly relating to weight issues and mental health94,219,223,224
After an athlete has sought medical advice, the coach can support the athlete in adhering to the recovery plan. In particular, the coach should adhere to medically recommended activity restrictions as part of the return-to-sport protocol when the athlete has returned to training. In doing so, the coach assists the athlete to avoid relapse, injury, or other problems that would further set the athlete back.
The International Olympic Committee has recently released a clinical assessment tool and a return-to-sport model that practitioners may use to aid in the athlete's return to training and competing. In this model, the athlete is stratified into one of three risk levels
98
:
Low risk: the athlete has an appropriate physique that is managed without undue stress or unhealthy diet or training strategies. Moderate risk: the athlete may have prolonged or severe low-energy availability marked by low BMI, low bone mineral density, abnormal menstruation, or a disordered eating pattern; and High risk: the athlete is diagnosed with eating disorders or other serious medical conditions (psychological or physiological) relating to low energy availability.
High-risk athletes may be encouraged to abstain from training and competition until they progress into a moderate- or low-risk category38,98. Even within the moderate category, training and competitions restrictions may be imposed, with return to sport requiring clearance by a physician.
The management of an athlete at risk of RED-S should include a multidisciplinary healthcare approach6,37,38,57,211. The coach may work with the overseeing physician or allied health professionals to develop an appropriate return-to-sport plan. In addition, the athlete may face stressors from within the sport context or external to it that may trigger relapse. The coach is well positioned to help minimize stressors from within the sport, such as the pressure to perform and relationships with teammates and team personnel 6 . Coaches should encourage safe return and discourage premature sport or competition participation.
Coaches should understand the critical role they play in the athlete's recovery process. Athletes tend to follow their coaches’ advice more so than that from parents or physicians4,31. This degree of influence is important for athlete development but can be detrimental if coaches provide advice and influence that conflicts with that of the overseeing physician. It is the coach's primary responsibility to protect the health of the athlete and to help the athlete adhere to the recovery program prescribed by the physician.
Conclusion
All athletes are at risk of LEA, particularly those who compete in sports that benefit from a high power-to-weight ratio. Although injury and illness are more common outcomes of LEA, the potential long-term damages to physiological development incurred from unfavourable metabolism and altered hormone profiles are particularly concerning. Coaches are uniquely positioned to help prevent athletes from entering LEA states, because they prescribe athlete training loads and observe and communicate with athletes in the daily training environment. Similarly, coaches play a crucial role in supporting athletes with LEA disorders back to health. However, coaches can only fulfill these prevention and support roles if they are well educated with regards to LEA and RED-S and are mindful of their influence on athlete behaviour. The information provided within this review should help coaches to play integral roles in reducing RED-S incidence.