
Abstract
Objectives:
Women who sell sex have a high prevalence of human papilloma virus, which may cause cervical cancer. The objective of this review was to collate findings on prevalence, associated factors, screening, service provision and utilization of services in relation to human papilloma virus and cervical cancer among women who sell sex in Eastern and Southern Africa.
Methods:
A scoping review methodology was employed. Inclusion criteria were as follows: (1) empirical papers, (2) of studies conducted in Eastern and Southern Africa, (3) published in the last 10 years, and (4) addressing women who sell sex in relation to (5) human papilloma virus and cervical cancer. A thorough search of a range of databases surfaced 66 papers. Both authors applied inclusion and exclusion criteria, resulting in 14 papers being reviewed.
Results:
The reported prevalence of high-risk human papillomavirus virus varied between 23.6% and 70.5%. HIV sero-positivity, other sexually transmitted infections and Epstein-Barr virus were associated with human papilloma virus and high-grade cervical lesions. High-risk human papilloma virus was associated with women who reported younger age at first intercourse, non-barrier contraceptive use, and no history of condom use. For screening, there was overall agreement between physician- and self-collected samples. Contradictory results were found for visual inspection with acetic acid. Screening services utilization was associated with provider’s recommendation, history of sexually transmitted infections, frequency of facility visit and history of vaginal examination. A diagonal programme led to an increase in screening, attributed to the targeted services.
Conclusions:
Context is important in planning cervical cancer services. There is a need for enhanced sexually transmitted infections and viral management within cervical cancer prevention. Women who sell sex should be empowered in self-collection of stored-dry specimens, especially in resource-constrained regions. Cervical cancer screening services should be honed to the needs of women who sell sex.
Introduction
It is estimated that 85% of the mortality from cervical cancer currently occurs in low- and middle-income countries (LMIC). 1 In sub-Saharan Africa, specifically, cervical cancer is a leading cause of cancer death among women. 2 In 2012, about 60,000 deaths from cervical cancer were estimated to have occurred. 3 The high incidence of, and mortality arising from, cervical cancer in this region may be explained by low awareness, advanced stage at presentation, and low national capacity in prevention, screening, diagnostic, and treatment options.1,4
Globally, women who sell sex (WSS) have a high prevalence of human papilloma virus (HPV) infection of high-risk types owing to high HPV exposure.5,6 This, together with the cervical cancer prevention and service challenges in LMIC, puts WSS in Africa in a precarious position. A review of clinical and non-clinical facility-based sexual and reproductive health (SRH) services for WSS in Africa revealed that most interventions were localized and small-scale, operated with little coordination nationally or regionally, had scanty government support, and narrowly addressed HIV prevention, counselling and testing, and sexually transmitted infections (STIs). Broader SRH needs such as cervical cancer screening were generally ignored. 7
The need for HPV and cervical cancer prevention campaigns to be tailored to WSS is increasingly recognized. 6 For this to occur, knowledge of the prevalence, associated factors, and current services is needed. The aim of this study is to review studies conducted on cervical cancer and WSS in the Eastern and Southern African (ESA) region.
Methodology
The scoping review methodology 8 was used in this project. The research aims of the review were to identify the following issues in relation to HPV and cervical cancer in WSS in Eastern and Southern Africa: prevalence, associated factors, screening, service provision and utilization of services. The following electronic databases were searched: Academic Search Premier; Health Source: Nursing/Academic Edition; Medline; PsyArticles; PsyINFO; SocIndex; Sabinet; Web of Science; PubMed; and Google scholar. The key word search for studies was: Female sex workers (Note of terminology: most public health publications use the term ‘female sex workers’. In this paper, we prefer the person-first approach, using women who sell sex; this is in line with other authors (Crankshaw et al. 9 ) OR sex workers AND cervical cancer OR HPV AND (list of countries (Angola OR Botswana OR Burundi OR Comoros OR Democratic Republic of Congo OR Eritrea OR Eswatini OR Swaziland OR Ethiopia OR Kenya OR Lesotho OR Madagascar OR Malawi OR Mauritius OR Mozambique OR Namibia OR Rwanda OR Seychelles OR South Africa OR South Sudan OR Tanzania OR Uganda OR Zambia OR Zimbabwe)) OR Eastern Africa OR Southern Africa. The search was restricted to the last 10 years (2010–2020, plus the first 3 months of 2021) to ensure that the information is current. No language restriction was placed on the search, in case there were relevant papers in another language (most likely French or Portuguese). The search, however, only surfaced papers written in English.
The initial search produced 66 papers. After duplicates were removed, the two authors went through the papers independently, determining whether the identified studies were relevant to the research aims. Inclusion criteria were that the papers should (1) be empirical papers, (2) specifically address WSS in relation to (3) HPV or cervical cancer, and (4) be conducted in ESA countries. All papers that did not meet the inclusion criteria were excluded (theoretical or review papers; not about WSS; not focussed on HPV or cervical cancer; conducted outside ESA countries). Each author’s assessments were compared. Where there were differences, these were resolved through discussion. The papers were quality checked through use of the mixed-methods appraisal tool (MMAT). No studies were discarded following this assessment. The result was 14 papers. Figure 1 is a flowchart of the literature search process. These papers were analysed by both authors using the research objectives as a template. As all journal articles used in this review are in the public domain, no ethics clearance was sought or needed.

PRISMA diagram.
Results
Table 1 provides a summary of the studies contained in this review.
Summary of studies.
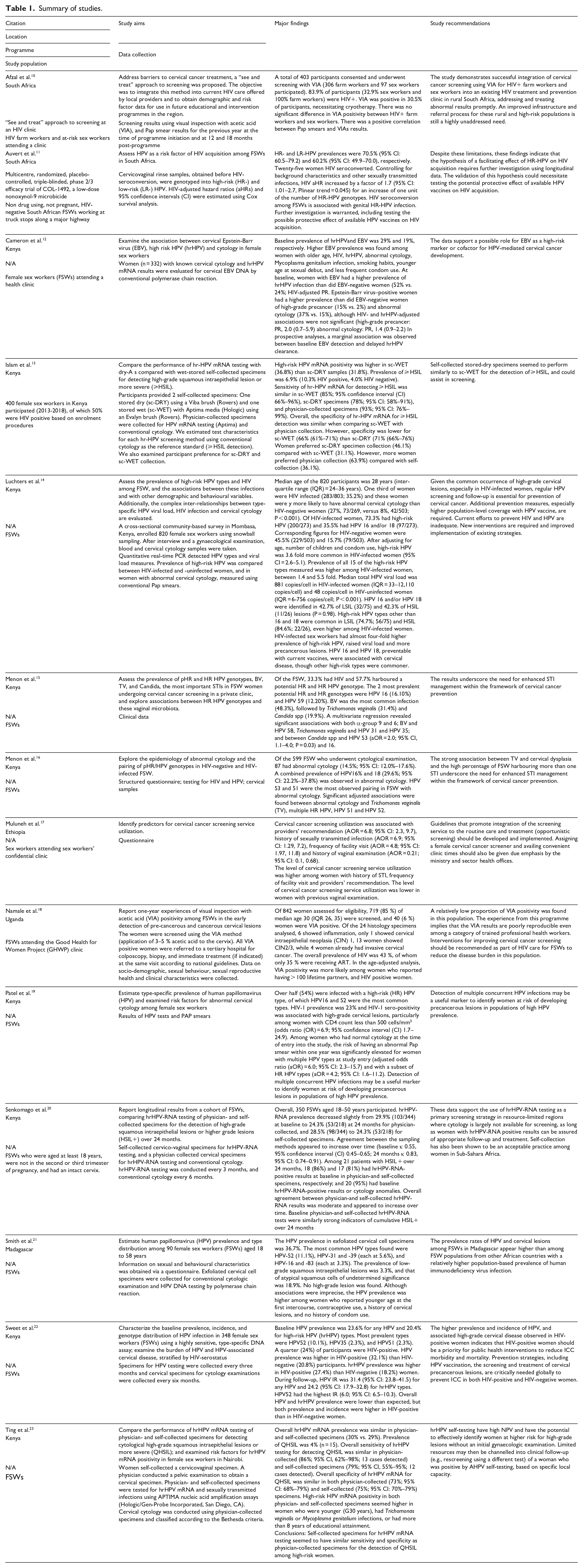
Four studies – two conducted in Kenya, one in Madagascar, and one in South Africa – measured the prevalence of HPV among samples of WSS. Patel et al. 19 found that 54% of respondents in Nairobi, Kenya, were infected with a high-risk HPV (hrHPV), with HPV-16 and 52 being the most common. Sweet et al’.s 22 study, also conducted in Nairobi, found a lower prevalence of 23.6% for any HPV and 20.4% for hrHPV. In follow-up, however, the incident rate was 31.4% for any HPV and 24.2% for hrHPV. In a Madagascar study, 21 the HPV prevalence was 36.7% (HPV-52: 11.1%; HPV-31 and 39: each at 5.6%; and HPV-16 and 83: each at 3.3%). In the South African study, 11 high-risk and low-risk HPV prevalences were much higher at 70.5% and 60.2%, respectively.
In Kenya, Patel et al. 19 report that HIV sero-positivity was associated with high-grade cervical lesions, particularly among women with a lower CD4 count (below 500 cells/mm3). Similar associations were found in Sweet et al’.s 22 Kenyan study, with the prevalence and incidence of hrHPV being higher in HIV+ than HIV– women, and in Luchters et al. 14 Kenyan study in which HIV+ sex workers had almost four-fold higher prevalence of hrHPV, raised viral load and more precancerous lesions than HIV- WSS. Auvert et al. 11 investigated HPV as a risk factor in HIV acquisition, showing that HIV seroconversion was associated in their sample with genital high-risk HPV infection. They note a number of limitations to their study, and argue for further longitudinal studies.
Significant associations between bacterial vaginosis (BV) and HPV 58, between Candida spp and HPV 16 and 53, and between Trichomonas vaginalis (TV) and cervical dysplasia were found in two Kenyan studies by Menon et al.15,16 respectively. The authors argue that these results underscore the need for enhanced STI management within the framework of cervical cancer prevention. In Madagascar, Smith et al. 21 found higher HPV prevalence among women who reported younger age at the first intercourse, contraceptive use, a history of cervical lesions, and no history of condom use. In their Kenyan study, Cameron et al. 12 found that Epstein-Barr virus (EBV)-positive women had a higher prevalence than did EBV-negative women of high-grade pre-cancer (15% vs 2%) and abnormal cytology (37% vs 15%), suggesting a possible role for EBV as a high-risk marker or cofactor for HPV-mediated cervical cancer development.
Screening for hrHPV and cervical cancer was addressed by a number of studies. In Kenya, Islam et al. 13 compared self-collected specimens versus physician-collected specimens; within self-collected specimens, they compared one stored DRY (using a Viba brush) and one stored WET (with Aptima media using an Evalyn brush). Women in the sample preferred physician collection (63.9%) compared to self-collection (36.1%); for self-collection, they preferred DRY (46.1%) compared to WET (31.1%). The self-collected stored-dry specimens seemed to perform similarly to self-collected stored-wet specimens for the detection of high-grade squamous intraepithelial lesions (HSIL). In a follow-up study with the same cohort, Senkomago et al. 20 and Ting et al. 23 found overall agreement between physician- and self-collected hrHPV-RNA results. They argue that the results strongly support the use of hrHPV-RNA testing of self-collected specimens in resource-constrained regions where access to physicians and cytopathologists is limited.
Afzal et al. 10 conducted a cross sectional study using visual inspection with acetic acid (VIA), with those having positive screens being offered cryotherapy. There was a positive correlation between Pap smears and VIAs results. They argue that VIA screening could be integrated in HIV treatment, thereby addressing and treating abnormal results promptly. Namale et al’.s 18 research in Uganda, however, contradicts these findings. The VIA had low sensitivity in their study, even though administered by trained health workers. They argue that the VIA is not a reproducible test and will lead to under-estimating the burden of disease.
Afzal et al. 10 note in their South African study that there are long delays in addressing abnormal Pap smears. Indeed, Namale et al. 18 note that, despite their reticence regarding VIA, the same day linkage of the VIA screen-positives to the diagnosis and treatment facility was critical. They call for careful consideration of the feasibility of the ‘screen and treat’ strategy for preventing cervical cancer recommended by the WHO for low-resource countries. Patel et al. 19 argue that detection of multiple concurrent HPV infections may be a useful marker in identifying women at risk of developing precancerous lesions, which could affect follow-up treatment.
Cervical cancer screening service utilization is addressed in an Ethiopian study. 17 Utilization was associated with provider’s recommendation, history of STI, frequency of facility visit, and history of vaginal examination. The Diagonal Interventions for Fast-Forward Health (DIFFER) programme was developed and piloted in India, Kenya, South Africa and Mozambique. It was aimed at improving targeted services for WSS and public health services, as well as cooperation between the two. An evaluation of the DIFFER intervention 24 in Mozambique showed an increase in screening in cervical cancer among WSS; this was attributed to WSS targeted outreach rather than use of public health clinics.
Discussion
The variability in prevalence of HPV among WSS reported in the studies points to the importance of context in the reproductive health of these women. The association of HPV and HIV-sero-positivity may account for some of the contextual variability.
The association of HIV sero-positivity, other STIs and EBV with HPV and high-grade cervical lesions highlights the need for enhanced STI and viral management within the framework of cervical cancer prevention. The association with non-barrier contraceptive use and no history of condom use illustrates the importance of condom distribution and programmes encouraging use among WSS and their partners.
The overall agreement between physician- and self-collected samples for HPV screening suggests that WSS should be empowered in self-collection of stored-dry specimens, especially in resource-constrained regions where access to physicians and cytopathologists is limited. Contradictory results were found for VIA. Nonetheless, the decrease in time delay between diagnosis and treatment that VIA allows means that this possibility should be explored further.
Utilization of cervical cancer screening services was associated with provider’s recommendation. Research on how and whether front-line healthcare providers refer WSS for screening could assist with improving this aspect of the reproductive health of WSS. The findings from the DIFFER programme that targeted services improved cervical cancer screening suggests that services honed to the needs of WSS are important. These kinds of approaches, including referral for, or actual, cervical cancer screening services should be integrated into routine care and treatment.
As a scoping review, this study is limited to the research questions and methods adopted by the studies included in the review. In order to allow assessment of whether the search criteria were unduly limiting, those criteria have been reported, as have the study inclusion criteria.
Conclusion
Context is important in planning cervical cancer services. There is a need for enhanced STI and viral management within cervical cancer prevention and consistent condom distribution. WSS should be empowered in self-collection of stored-dry specimens, especially in resource-constrained regions. Cervical cancer screening services should be honed to the needs of WSS.
Footnotes
Acknowledgements
We thank Richard Delate and Anna Maria Speciale for inputs on this project.
Author contributions
Catriona Ida Macleod conceptualized the project, applied inclusion and exclusion criteria to initial search papers; co-reviewed included papers; wrote the first draft of the article; finalized the article. John Hunter Reynolds performed the search; applied inclusion and exclusion criteria to initial search papers; co-reviewed included papers; contributed to writing the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is based on research supported by the South African Research Chairs initiative of the Department of Science and Technology and National Research Foundation of South Africa (grant number: 87582), and the United Nations Population Fund.