
Abstract
Objectives
It has been hypothesized that, in England, the rise in incidence of cervical cancer and the fall in screening coverage might be attributable in part to the effect of migration of Eastern European born women. We explored the attitudes and behaviours of these women towards cervical cancer prevention strategies.
Methods
A mixed methods study using quantitative surveys and in-depth semi-structured qualitative interviews was conducted between April 2015 and December 2016.
Results
In total, 331 surveys and 46 interviews were completed. Native English women had greater knowledge that a smear test is a screening test for pre-cancerous cervical cells (90% vs. 71% p≤0.01), whereas migrant Eastern European women believed that it was conducted as part of a full gynaecological examination (46% vs. 21% p≤0.01) and that the screen interval was annual (18% vs. 4% p≤0.01). Distrust of the English healthcare system resulted in some Eastern European women returning to their country of birth for screening. Poor awareness of cervical cancer prior to migration and lack of information at registration with a general practitioner in England were associated with failure to participate in screening.
Conclusions
The views and attitudes expressed by the migrant Eastern European women in this study suggest that they are not fully participating in cervical screening in England. Targeted education at the point of contact with healthcare services in England is needed to increase cervical screening participation among these women.
Keywords
Introduction
Cervical cancer is largely a preventable disease, but the incidence in the UK has increased by 5% in the last decade. 1 This has coincided with a gradual but steady fall in screening coverage rates in England, particularly amongst women aged 25–29. 2 It has been hypothesized that the migration of women from Eastern European countries to the UK may be partly responsible for this rise in cervical cancer incidence. 3 Across Europe, the highest incidence of cervical cancer is reported in Central and Eastern European countries. 4 Data from North West London found that migrant Eastern European women accounted for 28.2% of all new diagnoses of cervical cancer, and that significantly more Eastern European women had not previously been screened in the UK prior to their diagnosis, compared with UK-born women (90% vs. 52.6%). 5 In the Wessex region in England, 25% (n = 66) of the Eastern European women in a survey reported that they do not attend cervical screening appointments in the UK. 6 This pattern of behaviour has also been noted in other Western European countries. A study in Spain found that migrant Eastern European women had a 62% reduced odds of having cervical screening compared with the native population. 7
There has been a significant increase in the migrant Eastern European population to the UK, 8 and recent data have shown that 73% of the European Union, 81% of Bulgarian and 77% of Romanian citizens living in the UK are aged between 16 and 49. 9 Whilst the cervical screening behaviours of non-white ethnic groups have been extensively explored,10–12 there are limited data available on white ethnic minorities, such as the migrant Eastern European population, 13 and their individual needs may go unrecognized as they are often aggregated in the general “white ethnic group” category.
This study aimed to determine the cervical screening behaviours of migrant Eastern European women in England, and explore their knowledge of and attitudes towards the National Health Service Cervical Screening Programme, human papilloma virus (HPV), and the HPV vaccine.
Methods
A mixed methods approach was adopted, using a questionnaire survey and semi-structured qualitative interviews. Data were collected between April 2015 and December 2016. Eligible women were those who fell within the English cervical screening age (25–65) from two population groups: the study group, of migrant Eastern European (from the 2004/2007 EU accession countries), and the comparison group, native English Caucasian.
The Questionnaire Survey, developed following an extensive literature review, aimed to explore existing screening behaviours, and identify the level of knowledge and awareness of cervical cancer, cervical screening, HPV and the HPV vaccine, in the two populations, using an anonymous, paper-based, self-administered tool. Where possible, pre-validated questions were used. 14 An independent transcription company translated the questionnaire into the languages of the 10 Eastern European countries (Bulgaria, Czech Republic, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, Slovakia, Slovenia) and members of The European Federation of Colposcopy verified the translation accuracy. The final questionnaire consisted of 33 items. Data were collected from two settings, secondary care colposcopy clinics, and community groups. Secondary care (colposcopy clinics from three sites in the Midlands; University Hospitals Leicester, Northampton General Hospital and University Hospitals of North Midlands) participants were given a study pack at clinic reception, and asked to complete the survey prior to their consultation. For the community group setting, a snowballing approach 15 was utilized to identify local migrant Eastern European community groups. Consent was implied on completion of the survey. Participants were asked to self-volunteer at the end of the survey (by leaving their contact details) to be involved in the interview stage of the study. The surveys were pre-coded and a dataset was created using the statistics programme, Statistical Package for Social Sciences (SPSS), IL, USA, version 22. All reported p-values were assessed using two-sided tests and statistical significance was taken as a cut-off of p < 0.05. Each question was analysed individually to account for missing responses.
For the semi-structured qualitative interviews, participants from the survey who left contact details were given the choice of face-to-face one-to-one interviews, or a focus group session. Participants were interviewed until data saturation was reached. To ensure standardization and consistency, HP conducted all the interviews. An interpreter, if required, was available for the interviews with the Eastern European women. Participants decided on the meeting place based on convenience, either in a meeting room at the hospital or in the community at a location of their choice. The aim of these sessions was to obtain a detailed understanding of the thought processes behind particular screening behaviours and choices. The same topic schedule was utilized for the one-to-one interviews and the focus group session. The interviews were audio recorded and transcribed verbatim. Inductive framework analysis was used, with the aid of NVivo software to analyse the data. Two reviewers (HP, SS) reviewed the initial two transcripts independently and agreed on an extensive list of codes. HP reviewed the remaining transcripts to which the codes were applied. 16
Ethical approval for the study was obtained from the London Bromley research ethics committee (15/LO/0249).
Results
Questionnaire data
Of 400 questionnaires distributed to the three participating sites and in the community setting, 331 (249 from native English women and 82 from Eastern European migrant women) were completed, a response rate of 83%. The socio-demographic characteristics of the participants are described in Table 1. Knowledge of the English cervical screening programme was lower in the Eastern European migrant group, with 71% aware that a smear test was a screening test for pre-cancerous cervical cells, compared with 90% in the native English group, p≤0.01 (Table 2). A significantly greater proportion of Eastern European women believed that a smear test was part of a full gynaecological examination (46% vs. 21%, p≤0.01) and that the screen interval was one yearly (18% vs. 4%, p≤0.01). Just over half (55%[n = 40]) of the Eastern European women reported to have smears in England only. The remainder either had all their smears in their country of birth, or had smears in both their country of birth and England (Table 3). Overall, only 68% (221/324) of the women stated that they had previously heard of the HPV virus. Native English women were more likely to have heard of HPV than Eastern European women (73%[n = 179] vs. 53%[n = 42], p≤0.01). A detailed breakdown of specific HPV knowledge is presented in Supplemental Data 1. Multivariate analysis using linear regression for the whole cohort showed that none of the socio-demographic factors were significant for knowledge of the purpose of cervical smears. Higher educational attainment remained significant for all three HPV knowledge categories (general, testing and vaccine). Lower age persisted to show a significant association with HPV vaccine knowledge (Table 4)
Socio-demographic characteristics.
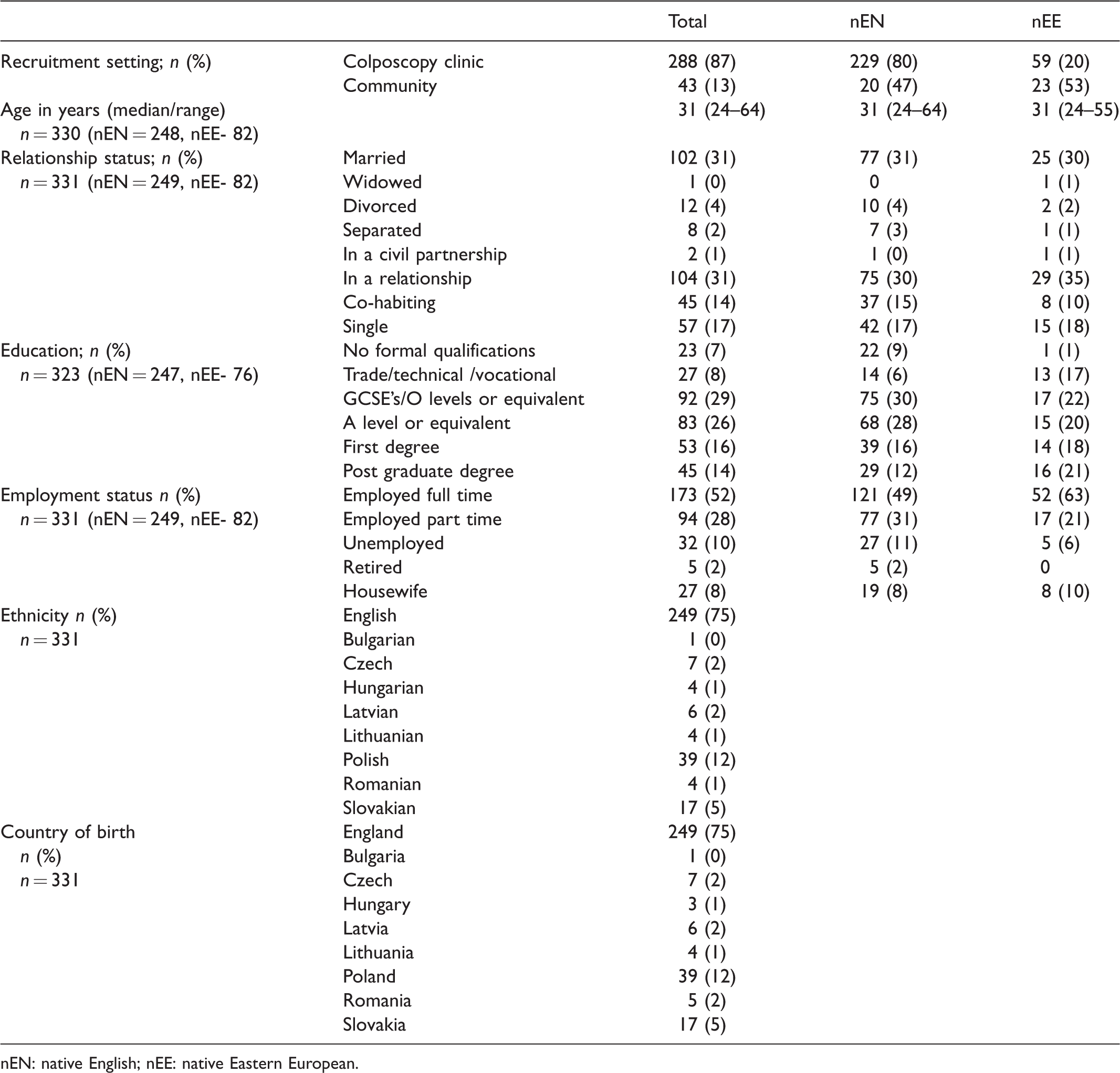
nEN: native English; nEE: native Eastern European.
Cervical screening behaviours and knowledge.
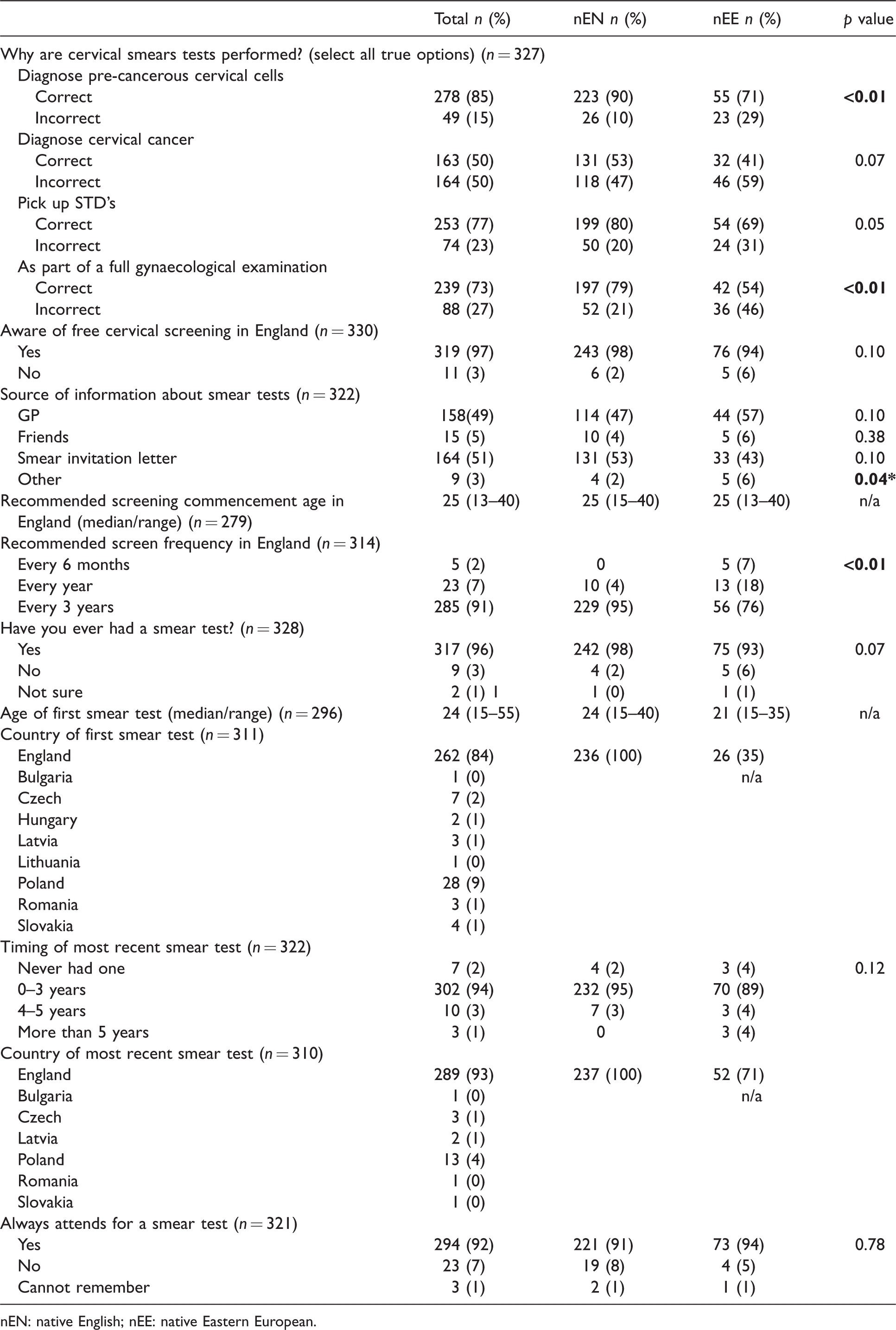
nEN: native English; nEE: native Eastern European.
Cervical screening behaviours and knowledge of cervical cancer prevention in their country of birth for the Eastern European migrant women.
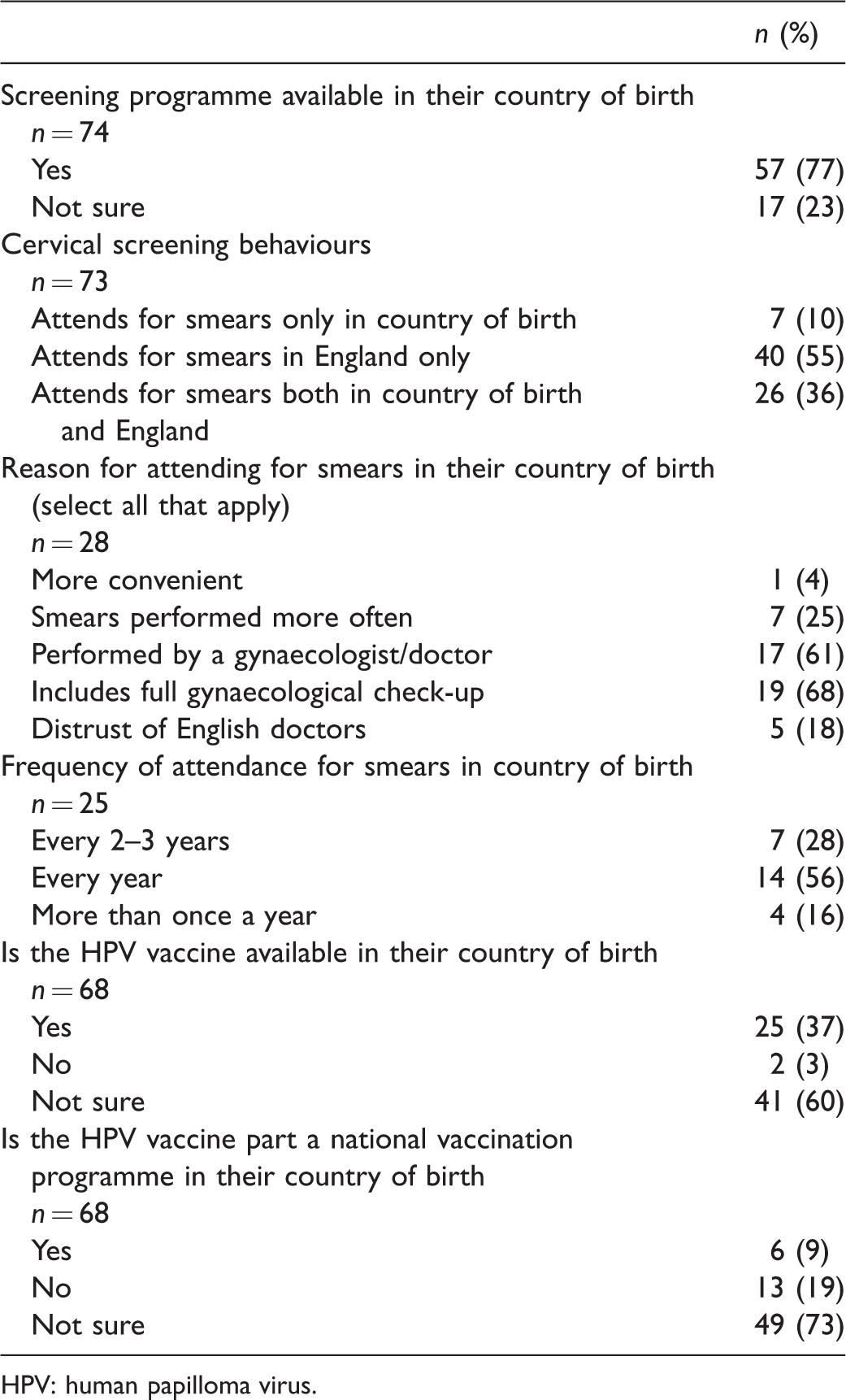
HPV: human papilloma virus.
Multivariate analysis models for the associations between socio-demographic factors and knowledge of cervical cancerprevention.
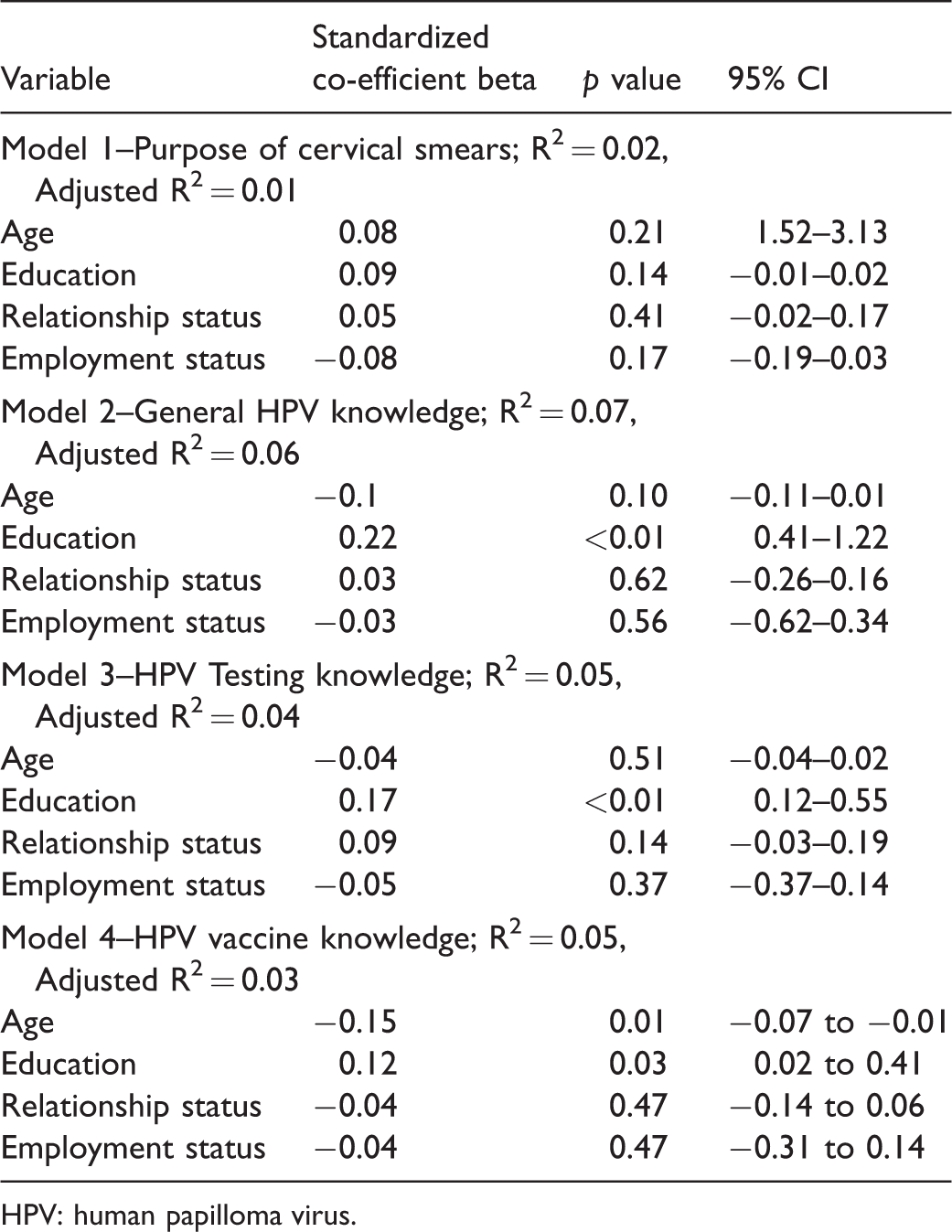
HPV: human papilloma virus.
Interview data
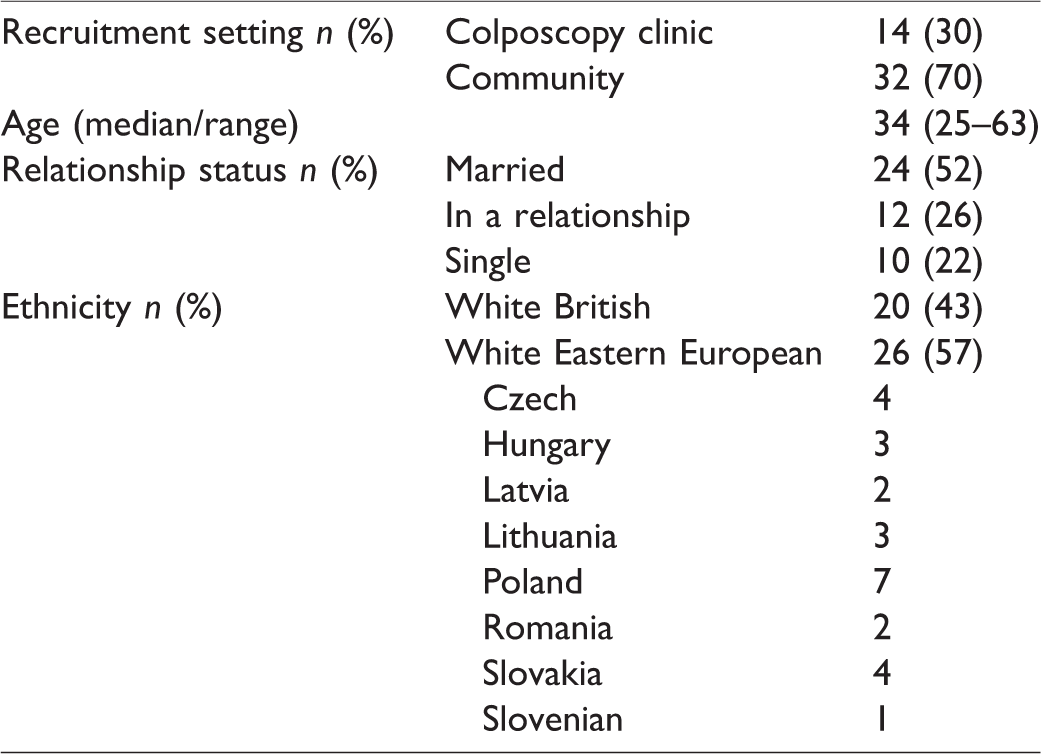
In addition to 40 one-to-one semi-structured interviews (20 with Native English women and 20 with Eastern European migrant women), one focus group was conducted, with six women from Czech and Slovakian backgrounds. The analyses of the interviews and the focus group have been performed together as there was only one focus group, and the same interview schedule was utilized for both. Details of the participant characteristics are displayed in Table 5. From the 14 theme categories and 45 codes (see Supplemental Data 2), a summary of the key themes and findings are described below. Details in the parentheses following the quotes represent the participant's identification number and recruitment setting (PC = Community, PH = Colposcopy clinic, FG = Focus group), age (in years) and ethnicity. Additional supporting quotes are provided in Supplemental Data 3.
Participant characteristics for qualitative interviews.
Perceptions of the English healthcare system
The Eastern European women had often delayed registration with the general practitioner (GP) on migration, for reasons including that they were not “unwell” or because they were able to self-medicate. They held largely negative views about GPs in England, and felt that their concerns were not taken seriously and that often their symptoms would be dismissed. In comparison, in their countries of birth they had direct access to specialist care, and found it frustrating that in England the GP acted as a gatekeeper. Several women in the migrant group reported that “it’s much easier to book a ticket and go back to one of those countries, pay privately, and at least they do something” (PH1, 35, Lithuanian).
Understanding of cervical cancer, screening and HPV
Knowledge of cervical cancer was poor in both groups of women. Many believed that cervical cancer was hereditary; some were aware that it could be asymptomatic. The Eastern European women used this fact to justify the need for more frequent smear tests and having a specialist review. Also, cervical cancer, there aren’t really many symptoms, so it’s hard to realize, find out unless you go to the doctor that you have cervical cancer. So, it’s peace of mind if you go once a year that some specialist looked at you, rather than go every three years. (FG, Czech/Slovak) … when I moved here I didn't have any information about it and even in GP practice they didn't, like in the walk-in clinic they didn't even suggest me anything like that, so it’s like there isn't any information and there isn't any education about it either. (PC1, 34, Latvian)
Cervical screening behaviours
The Eastern European women, overall, had commenced cervical screening from age 18 as part of an annual gynaecological review, compared with the native English women, who started between the ages of 20 and 25. Migrant women had mainly had their initial smear in their country of birth, and subsequent screens in England and/or in their country of birth, or had not participated in any screening in either country. On the whole, the Eastern European-born women had a heightened desire to protect themselves, which resulted in them having more frequent smears in their country of birth. It was felt that over three years it was possible to develop cancer, without necessarily being aware of it or having any specific symptoms. This fear related back to their deficient knowledge of cervical cancer development, with many of them not aware whether it was a rapidly progressing disease. Some of the women believed that it was due to cost implications that more frequent smears were not routinely performed. Although this was not true for all participants, Eastern European-born women used the smear in their home country as a “double check” mechanism, as they trusted their own doctors more. “I know it’s going to sound a little bit harsh but I trust more, like, Polish … if I’ve done the test here and if I’ve done it in Poland at least I double check if you know what I mean” (PC14,29,Polish).
Motivators
The main motivators for participation with cervical screening were shared amongst the two groups of women. These included the fear of getting cancer and the desire to preserve good health and having adequate knowledge to appreciate the benefit of screening in the prevention of cervical cancer; some women believed that it was part of a sexual health check. The latter belief was more prevalent in the Eastern European group, who largely believed that cervical screening and a “routine” gynaecological review were synonymous. Throughout the interviews, the Eastern European women used the terms cervical screening and gynaecological examination interchangeably. “…I started to have sexual intercourse and I thought that it would be good to do the whole… gynaecological review” (PC5,34, Polish).
Barriers
Shared barriers among the two groups included being asymptomatic, no knowledge of cervical screening, and feeling embarrassed. Barriers to cervical screening specific to the Eastern European group included language, which served as an obstacle to initially registering with the GP, understanding the screening invitation letter, booking an appointment and making travel arrangements to attend. Prioritization of tasks on migration, such as sourcing employment and finding accommodation and schooling for their children, further precluded screening participation. The person performing the smear test was of great importance to the majority of the migrant women; they were not comfortable that, in England, practice nurses perform the majority of cervical smears. They believed that smear tests should only be performed by a specialist (gynaecologist). “The gynaecologists, so, you know, there is more studying involved. I don’t want to sort of underestimate or underrate the nurses here, but it’s more comfort, it being done by a doctor” (FG, Czech/Slovak).
Increasing the uptake of screening
Language was perceived to be the main barrier to screening for Eastern European Women. Suggestions were made to produce information in their native languages. Targeting advertisements at specialized supermarkets, community centres, or recruitment centres was thought to increase awareness and hence participation. “Yes, maybe like some, like when you have like Polish shop or Polish restaurant, maybe just to leave some leaflets or something” (PC14,29,Polish). The women disclosed that many Eastern European women could live in isolation when they first arrive in England, and therefore it might be difficult to reach them. The provision of education, for example, simply taking the time to explain what the purpose of a smear test is and the important role it plays in the prevention of cervical cancer, was believed to be a key factor. The participants believed that many Eastern European women would not have this knowledge on migration.
Discussion
This mixed methods study shows that the barriers preventing Eastern European migrant women from participating in cervical screening in England were not exclusive to this group, and that some barriers were shared with native English women and women from other cultural backgrounds.17,18 The cervical screening behaviours of the Eastern European migrant women were specifically influenced by the manner in which they accessed healthcare services, and their trust in healthcare/healthcare professionals in England.
The incidence of cervical cancer has been predicted to rise by 43% 19 in the UK between 2014 and 2035, and the findings of this study suggest that the migrant Eastern European population may contribute to this rise. The views and attitudes expressed by the Eastern European migrant women in this study suggest that they are not fully participating in cervical screening in England, supporting the findings from previous work in Birmingham that the majority of Eastern European migrant women had not attended screening prior to their cervical cancer diagnosis. 20 Because the uptake of cervical screening in their countries of birth is suboptimal, 21 there is also the potential that many of these women will not have been screened prior to migration. For example, the largest Eastern European population in England is from Poland, 22 where screening uptake is only 25%.21,23,24
This study indicates that there are two groups of migrant Eastern European women who are not attending for cervical screening in England: those who have some knowledge but do not trust the English healthcare system fully, and those who have no awareness of screening, either in England or their country of birth. Targeted education to increase awareness of cervical screening in both these groups is imperative, but it will be difficult to identify the latter group, as they might not present to healthcare services in England.
The frequency of smear tests in England was an area of concern for the Eastern European women, who believed that cervical screening should be offered on an annual basis. The “prolonged” screen interval was a motivating factor for some to travel for more frequent smear tests. For the majority of these women, access to more frequent screening, even in their country of birth, would have been outside of any national programme. 25 Annual screening has not been shown to add significant protection over the three- or five-yearly screen intervals, 26 and there is a risk of overtreatment of lesions that may spontaneously regress. 27
It has been suggested that the process of migrant acculturation follows a linear path, determined by the length of residence in the migrating country. 28 In this study, the impact of length of residence in England on cervical screening behaviours was not clear, and as it only included first generation Eastern European women, future research would be needed to explore the cervical screening behaviours in second or subsequent generations. Work conducted by Jackowska et al. 13 in migrant Eastern European women in London between 2008 and 2009 found similar themes to the present study, which suggests that there has been little change in behaviours and attitudes, and also that any efforts that might have been made to engage this group with cervical screening in England have not been fully effective. “The context of reception” (the behaviours and attitudes of the receiving society) is also believed to influence the process of acculturation. 29 Our data indicate that this is where changes can be made to improve screening participation in this migrant group. Healthcare professionals in England (the receiving society) have a vital role to play. It is imperative that they understand the context in which the health beliefs of migrant Eastern European women are formed (i.e. the system and provision of healthcare in their country of origin). Individualized education on the natural history of cervical cancer and cervical screening will need to be provided to justify the differences (from their country of origin) in the provision of cervical screening services in England. It is possible that migrant Eastern European women represent a group that is inherently less likely to engage with healthcare services in the county of migration, and a study in Norway found similar problems with engaging Eastern European migrant women with healthcare and cervical screening. 30
Outreach community work and opportunistic promotion of cervical cancer prevention strategies are required, ideally when the women first make contact with healthcare services in England (primary or emergency care). The main limiting factors of adopting this strategy are those of resources and time, particularly in the emergency setting; however, it might be argued that the resource/cost implication of cervical cancer treatment is significantly greater.
This study has some limitations. A non-random consecutive sampling method was utilized to recruit participants for the questionnaire component. Due to the scale of the study and the relatively low population of Eastern European migrant women in the study area, this was the most achievable method of recruitment, and participants were recruited from a large geographical region and multiple institutions. Difficulties were experienced in identifying and engaging these participants in the community, highlighting the challenges in accessing this population for the purpose of health promotion. The majority of surveys were completed by women attending colposcopy clinics who are, by default, already engaging with cervical screening. Importantly, however, they provide an important insight into what motivated them to participate, rather than primarily focusing on the barriers. 31 Eastern European migrant women who have not joined community groups or integrated with the community were not sampled, and it could be argued that this is the group that should be targeted.
Because the participants were asked to self-volunteer for the interview component of the study, this group might represent women who are already engaging more with health promotion. Nevertheless, some of the women had not always participated in cervical screening or engaged with healthcare services in England, and this group provided an insight into what induced a change in their health behaviours and what their barriers were prior to this.
It is acknowledged that the Eastern European migrant group is very heterogeneous, and not all of the countries of interest were represented. As all populations are not the same, the findings might not be representative; however, our study has shown that many of the views and health behaviours were shared amongst women from the different Eastern European countries.
Conclusion
The cervical screening behaviours of the Eastern European migrant population to England appeared to be, in part, governed by their perception and/or level of trust overall in the English healthcare system, which prevents them from wholly accepting screening advice and/or recommendations. Pre-existing knowledge of cervical cancer and screening behaviours prior to migration also play a role. To increase uptake in this high-risk group of women, targeted education should be provided at the initial point of contact with healthcare services in England.
Supplemental Material
Supplemental Material1 - Supplemental material for Awareness of and attitudes towards cervical cancer prevention among migrant Eastern European women in England
Supplemental material, Supplemental Material1 for Awareness of and attitudes towards cervical cancer prevention among migrant Eastern European women in England by Hersha Patel, Susan M Sherman, Douglas Tincello and Esther L Moss in Journal of Medical Screening
Supplemental Material
Supplemental Material2 - Supplemental material for Awareness of and attitudes towards cervical cancer prevention among migrant Eastern European women in England
Supplemental material, Supplemental Material2 for Awareness of and attitudes towards cervical cancer prevention among migrant Eastern European women in England by Hersha Patel, Susan M Sherman, Douglas Tincello and Esther L Moss in Journal of Medical Screening
Footnotes
Acknowledgements
We acknowledge the contributions made by Mr Charles Redman as supervisor for this study, the colposcopy teams at University Hospitals of Leicester, Northampton General Hospital and University Hospitals North-Midlands for their help with recruiting women for the study. We would like to acknowledge all the women who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Leicester Hospitals Charity.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.