
Abstract
Objective:
Although cervical cancer could be prevented through medical screening, it remains one of the top causes of cancer-related morbidity and mortality all over the world. A number of factors may contribute to cervical cancer screening behaviour of women. The aim of this study was to investigate factors related to cervical cancer screening behaviour of women in Kazakhstan.
Methods:
This was a cross-sectional survey-based study with a total of 1189 participants. Women attending gynaecological clinics aged between 18 and 70 years were administered paper-based questionnaires about their awareness of cervical cancer, the associated risk factors, and cervical cancer screening. Student t test or Wilcoxon rank-sum test and chi-square test or Fisher’s exact test, where appropriate, were used to determine associations with categorical independent variables.
Results:
The mean age of participants was 36.5 ± 10.1 years. Less than half (45.7%) of the participants had been screened for cervical cancer. The key factors related to the cervical cancer screening behaviour of women in this study included age, having a larger number of children, regular menstrual function, awareness of Pap smear test, and free screening programme for cervical cancer, and the causal association of human papillomavirus with cervical cancer.
Conclusion:
This study revealed several significant factors predicting screening behaviour in Kazakhstani women. To improve the rate of screening, there is a need to increase public knowledge and awareness of cervical cancer and opportunities for the free screening programme in the female population of Kazakhstan.
Introduction
Cervical cancer (CC) was the fourth most common cancer in women during the last decade.1,2 According to the World Health Organization (WHO) report, approximately 570,000 cases of CC and 311,000 deaths from the disease occurred in 2018.1,2 CC is listed in the top three cancers affecting women younger than 45 years in 146 countries. 2 The estimated age-standardized incidence of CC in 2018 varied widely among countries, with rates ranging from less than 2 to 75 per 100,000 women, depending on the countries’ income. 2 Kazakhstan exhibits a high CC incidence rate in women of all ages, and it has risen significantly to 18.2 per 100,000 women.3,4 The age-standardized incidence and mortality were 15.7 and 7.5 per 100,000 women, respectively (estimates for 2018). 3 About 1729 new CC cases are diagnosed annually in Kazakhstan, and CC ranks as the second leading cause of cancer and cancer-related death in women.3,5
In view of this, CC screening (CCS) programmes that contribute to the reduction of incidence and mortality rates play an important role in the prevention of this disease.6,7 CCS strategies differ between countries. 7 Organized CCS programmes are found to be more effective with high participation at regular intervals with equal access and high-quality standards for diagnosis, and are thus potentially more efficient than random screening. 7 Developed countries with comprehensive cancer screening programmes have recorded sustained declines in CC incidence and mortality, while many developing countries continue to show increases in incidence and mortality rates.8,7 The Kazakhstani national screening programme has undergone significant positive changes over the past 12 years since it was implemented in 2008. 4 Initially, based on conventional Papanicolaou testing (Pap smear), screenings were performed every 5 years in the target group of women aged 30–60 years. 4 From December 2017, the screening interval was reduced to 4 years, and the age of the target group was extended to 70 years.4,5 However, despite these efforts, the CCS coverage decreased from 72.9% in 2008 to 45.9% in 2016, 9 and the high CC incidence and mortality rates in Kazakhstan reveal that the screening programme does not work effectively.
There are many socio-cultural and clinical factors and barriers affecting CCS and its effectiveness.10,11 Issues associated with CCS include disease ignorance and cultural issues related to gynaecologic screening, late reporting, economic factors, domestic gender power relations, education, alternative sources of reproductive health knowledge, and poor/unequal healthcare coverage.8,10,11 To our knowledge, there are no available published data describing factors related to the utilization of CCS service in Kazakhstan.
In light of the high incidence and mortality rates from CC in Kazakhstan and an inefficient CCS programme with low coverage, there is a need to identify factors associated with the screening programme’s effectiveness. The aim of this study was to investigate factors related to the CCS behaviour of women in Kazakhstan.
Methods
Study participants
A cross-sectional survey-based study was conducted between 25 May 2019 and February 2020. Women attending gynaecological clinics aged between 18 and 70 years who agreed to participate were included in our study. Women were recruited using a convenience sampling method. Patients visiting these gynaecological clinics were offered to participate in this study. Women were selected from cities from five different regions of Kazakhstan: Nur-Sultan (central), Almaty (southern), Aktobe (western), Pavlodar (northern), and Oskemen (eastern).
In Kazakhstan, free screening for CC is available for women aged between 30 and 70 years. 5 However, women facing gynaecological problems might visit gynaecological clinics to carry out screening at an earlier age. Thus, the age range for women participating in this study was set to be between 18 and 70 years.
Study instrument
Data were collected using two questionnaires. First, a paper-based questionnaire was filled out by doctors from the gynaecological clinics. The questionnaire consisted of 30 items and included questions about socio-demographic characteristics, lifestyle characteristics, and the medical history of gynaecological diseases of the participants.
The second questionnaire was adapted from previous studies12,13 and was filled out by the participants. The patient questionnaire consisted of 25 items: socio-demographic characteristics of the patients, awareness of CC and the associated risk factors, awareness of screening for CC, whether the patient had gone through screening for CC, awareness of human papillomavirus (HPV), and awareness of risks of HPV (supplemental materials are available online). The survey was conducted in Kazakh and Russian languages depending on the preferences of the participants. The STROBE guidelines for cross-sectional studies were followed.
Study variables
Independent variables were socio-economic as indicated by income (average monthly salary for June 2020 was 196,922 tenge (US$471) according to the Ministry of the national economy of the Republic of Kazakhstan 14 – ⩽100,000 tenge (⩽US$241.54), 101,000–200,000 tenge, and >200,000 tenge; education level – high school or less, vocational level, and university level) and demographic characteristics (age; ethnicity – Kazakh and non-Kazakh (Russian and other ethnicities); body mass index (BMI); and city of residence) of the participants. Also, information on marital status (in a relationship – married, in a committed relationship; single – single, widowed, and divorced), family (number of children, history of abortion, and age when started sex life), and lifestyle (smoking status and alcohol consumption) characteristics of participants was collected. Gynaecological health (menstrual function, history of gynaecological surgery, and history of sexually transmitted diseases (STD)), medical factors (having an oncological disease and family history of oncological disease), and awareness of the participants about CC and HPV (awareness of CC, Pap smear test, recommended frequency for oncocytology (Pap smear) test, meaning of an abnormal Pap smear result, availability of free screening programme for CC (Pap smear test) in Kazakhstan, and awareness of causal association of HPV with CC) were included in the survey.
Outcome variable for this study was whether the patient had been screened for CC. Screened respondents were women who responded ‘yes’ to the question ‘Have you ever undergone screening for CC (Pap smear test) in the past?’ while not screened were those who answered ‘No, I didn’t use any screening program’.
Ethical considerations
This study design and the content of the questionnaires were approved by the Nazarbayev University Institutional Research Ethics Committee (NU IREC), protocol number 146/4042019, date of approval: 23 April 2019. Verbal informed consent was received from all participants and recorded on their record. Verbal consent was obtained for a number of reasons, outlined below, and approved by the NU IREC. Verbal consent was prioritized as Kazakhstan is a post-Soviet country where many people are not comfortable with signing documents that are similar to a contract. Moreover, the general population tends to have low trust towards interviews and researchers. All patients were assigned with the personal code, and no personal information (personal identifiers) was made available to the investigators at any time before, during, or after the study. The verbal consent used for this study included all the necessary components of informed consent. All the information about the study and participants rights was stated both orally and on the information letter provided to the participants.
Data analysis
Data was analysed using STATA 16. 15 Data analysis consisted of descriptive statistics including frequencies and mean scores for the demographic variables, and was presented as mean (SD) or median (range) for continuous variables, and as frequency and percentage for categorical variables. To determine associations with continuous independent variables, Student t test or Wilcoxon rank-sum test was used, whereas chi-square test or Fisher’s exact test, where appropriate, was used to determine associations with categorical independent variables. Using univariate and multivariable logistic regression models, crude odds ratio (COR) and adjusted odds ratio (AOR) with corresponding confidence intervals were calculated in regression analysis. The model was built using a backward approach, until all statistically significant variables were left in the model. A significance value of 0.05 was used as an indication of association between variables.
Results
Participant characteristics
In total, 1189 women participated in the study. A summary of the socio-economic and demographic characteristics of the study participants is provided in Table 1. The mean age of the participants was 36.5 ± 10.1 years, with the majority of patients (37.5%) aged between 26 and 35 years. The mean BMI of women was 24.2 ± 4.7. Approximately three quarters (77.0%) of women were of Kazakh ethnicity. The number of women recruited from the five cities (namely Nur-Sultan, Almaty, Pavlodar, Aktobe, and Oskemen) was almost the same. Less than half of the participants (40.8%) were from cities with a population of more than one million. Almost half of the participants (45.4%) had obtained a university degree, and almost 50% of the women have reported their family income to be less than or equal to 100,000 tenge per month (~US$300). Only a few women reported tobacco smoking or drinking alcohol, which was 5.1% and 0.3%, respectively.
Demographic and socio-economic characteristics of study participants (N = 1189).

BMI: body mass index.
The majority of women were married (79.8%) and had one or more children (82%). About half (49.5%) of the participating women had no abortions in the past. The mean age at which the women started their sexual life was 20.5 ± 2.9 (Table 2).
Marital, family, and lifestyle characteristics of study participants.

The vast majority (94.1%) of women had regular menstrual cycles and 76.7% had no gynaecological surgery. Only a small number of women reported having a history of STDs (5.7%), oncological diseases (0.5%), and a family history of oncological diseases (2.6%) (Table 3).
Gynaecological, health, and medical characteristics of study participants.

STD: sexually transmitted disease.
Awareness and knowledge of CC and HPV
The majority of the participants (60%) were aware of the causes of CC. More than half of the participants (53.1%) knew about the Pap smear test and 47.4% were aware of the meaning of Pap smear results. However, only 14.4% of the women knew the recommended frequency for the Pap test. More than half of the participants (58.5%) were aware of a free screening programme for CC. Three quarters of the participants (74.3%) were not aware that HPV infection was the major cause of CC (Table 4).
Awareness and knowledge of CC and factors associated with CCS utilization among study participants.
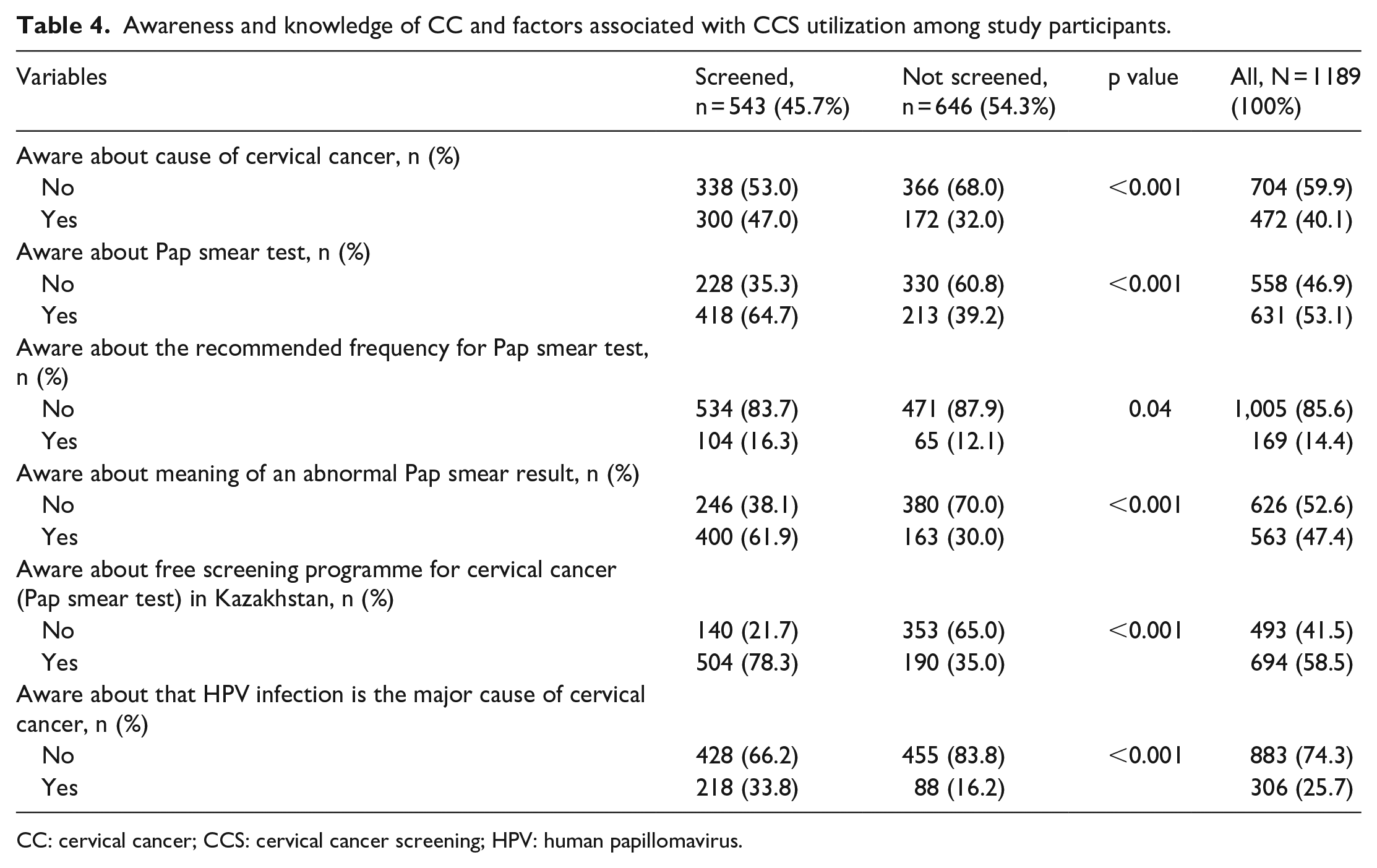
CC: cervical cancer; CCS: cervical cancer screening; HPV: human papillomavirus.
Patients who had been screened previously (N = 543) indicated their sources of information on free CCS. Gynaecologists (75%) and general practitioners (40.1%) were the main sources that had provided information about screening to the participants. Nurses and other health professionals had a lower contribution to such information for patients, which were 10.1% and 4.6%, respectively. Not only medical specialists but also television (5.3%) and the Internet (12.7%) became the sources of CC to the women as well. Educational events, magazines, friends, and peers were also sources of information about screening, but only for a few participating women.
Less than half of the participant women (45.7%) did not have screening for various reasons. The most prevalent barrier (42.3%) to screening was the fact that women were not aware of screening for CC. The second most common barrier was that many women (32.7%) considered themselves to be healthy and therefore did not seek screening.
Bivariable analysis
More than half (54.3%) of the participants had not been screened for CC. Younger Kazakh women aged 18–25 years were statistically significantly less likely to attend screening for CC. In addition, BMI, city where they lived, family income, number of children, history of previous abortions, and menstrual function were statistically significantly associated with obtaining screening for CC (Table 2).
Awareness of the cause of CC, Pap smear test, meaning of an abnormal oncocytology, availability of free screening test, causal association of HPV with CC, and knowledge about HPV as the major cause of CC were found to be statistically significantly associated factors for screening behaviour of the participating women (Table 3).
Multivariable analysis
Multivariable logistic regression modelling showed that older age, having a larger number of children, regular menstrual function, awareness of Pap smear test, free screening programme for CC, and causal association of HPV with CC were found to be independently associated factors with screening behaviour. The odds of being screened for CC were 4.27 times higher for women who knew about the free screening programme for CC (Table 5).
Bivariable and multivariable logistic regression modelling to determine factors associated with cervical cancer screening service utilization.

COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; HPV: human papillomavirus.
Discussion
To our knowledge, this is the first study to explore the CCS behaviour among Kazakhstani women. The findings of this study revealed about half of the participants (45.7%) had actually been screened for CC. Although the percentage of the women screened for CC in this study was not lower than that in most of the other middle-income countries, the numbers do not meet the goals set by the Ministry of Health of the Republic of Kazakhstan, which is to cover at least 70% of the target population. According to the national screening programme of Kazakhstan, every 4 years, each woman aged 30–70 years should attend the free screening for CC. 5
The prevalence of women attending screening for CC (45.7%) is higher in Kazakhstan if compared with other middle-income countries. A study conducted in Jordan revealed that only 31% of women were screened for CC. 16 And a study conducted among Chinese women revealed that only 21% of women were screened for CC. 17 There have been certain barriers to having CCS for the participants of our study who were not screened for CC (54%). The major barriers were the participants’ unawareness of the free CCS (42.3%) programme and the fact that participants considered themselves either healthy or too young to go for screening (32.7%). This is comparable to many other countries,18,19 although there can be many other reasons why there is such a low prevalence of screening for CC globally.
In regard to knowledge and awareness of participants about CC risks and screening, the majority of participants were not aware of the CC causes (59.9%), about the recommended frequency for Pap smear test (85.6%), and about the meaning of abnormal cytology (52.6%). However, a majority of our participants were informed of the Pap smear test (53.1%), the free screening programme for CC (58.5%), and HPV as a major cause of CC (74.3%). Therefore, we can conclude, although not complete, participants of our study had a good understanding of CC and CCS. The major sources of information for CCS were gynaecologists (75.0%) and general practitioners (40.1%). This shows the importance of healthcare workers in informing people about CC and screening opportunities, which is in line with the results of a similar study conducted in Jordan, where the lack of recommendations from the health professionals was found to be the most prevalent barrier in screening for CC. 20
Overall, the knowledge of CC and CCS in many developing countries is low. Knowledge, attitudes, and practices (KAP) study on CC prevention in Cambodia revealed that 46% of women were aware of the causes of CC, but only 2% were aware that HPV infection was a risk factor for CC. 19 Similar results were also found in the study among Saudi women, whereby 70% of women had previous knowledge of CC, but had very low awareness that HPV was the main risk factor for CC (3.2%). 21 A study conducted in Ethiopia revealed only 30% of the participants had knowledge of CC. In comparison, our study showed that 40.1% of women attending gynaecological clinics in Kazakhstan were aware of CC and 25.7% were aware of the HPV infection as a risk factor for CC.
One of the interesting findings of this study was the association between the regular menstrual cycle and the positive screening behaviour of women. This finding appears contradictory as most women with irregular menstrual cycles or women with complications would most likely see their gynaecologists and carry out their CCS. However, this contradictory finding can be explained by the ‘healthy volunteer bias’ phenomenon. 22 Those who are healthy were more likely to be screened – ‘healthy volunteer effect’ – as people who practice preventive therapies, usually tend to adhere to more healthy behaviours like a cancer screen. 23 Nevertheless, this is certainly an interesting finding and deserves further future investigation.
Although attending college or university showed a higher likelihood of undergoing screening in other studies,24,25 our study showed no association between education and the likelihood of a woman to undergo screening. This trend can be attributed to the fact that there is easy access to education in Kazakhstan. The majority of participants (85.1%) had achieved education either at the vocational level or at the university level. Only a few women (14.1%) had either high school education or less. Education in Kazakhstan is affordable for the majority of the population due to the lower fees and a large number of state grants and scholarships awarded to students annually.
Awareness and knowledge about CC and CCS have been found to be one of the biggest and most important factors in our study associated with the likelihood of women to undergo screening. Women who were informed about free screening were 4.27 times more likely to attend the screening for CC in comparison with those who did not. Moreover, women who were aware of the fact that HPV infection is one of the major causes of CC were also 1.46 times more likely to attend the screening for CC in comparison with women who lacked this information. These results are in line with the findings from other studies, 17 where women who were aware of this information were more likely to participate in the screening programme. However, in our study, certain socio-economic factors, such as the level of education, salary, or city of the living, did not show significance in our statistical model. Therefore, it indicates a need for an advertisement for free screening programmes, as well as a need for an increase in the knowledge of CC among the women population throughout Kazakhstan.
Study limitations. Since the design of our study was cross-sectional, we cannot identify causal relationships between selected factors and the level of CCS. Future research is needed to identify whether some factors have effects beyond association. This study employed a convenience sampling method and self-reporting as the means to collect data. Both of these could create biases, such as underreporting or exaggeration of information provided. As well as selection bias, such as non-response bias, a bias that occurs when non-responders from a sample differ in a meaningful way from those who responded. Also, the study participants were not selected randomly but rather enrolled by convenient sampling which could be a source of selection bias. In addition, we do not have data to compare whether the study participants were similar by socio-demographic, clinical, and other important characteristics to women attending clinics outside of the study sample.
Strengths and future directions. This is the first study with a wide population reach to evaluate CCS behaviour among women in Kazakhstan. The results of the study showed that a lot fewer women in Kazakhstan screened for CC than was aimed for by the free national CCS programme. Our findings indicate that there is a need to focus on women with a younger demographic profile, as they are less likely to participate in screening. It is also clear that awareness of Pap smear tests, free CCS programmes, and knowledge of the link between HPV and CC significantly increase the odds of a woman who would undergo CCS. Healthcare providers should focus on increasing awareness regarding CC through various means, such as education by healthcare workers and Internet advertisements.
Generalizability. Despite this study including 1189 women from five different cities of the largest regions of Kazakhstan, the generalizability of the study results could be limited. The study findings might not be applicable for the rural citizens because only urban residents of gynaecological clinics were enrolled.
Conclusion
This study revealed that Kazakhstani women between the ages of 18 and 70 years who visited gynaecological clinics had higher levels of CCS (45.7%) in comparison with the other middle-income countries. This number, however, still falls short of the Kazakhstani national screening programme target of 70%. In this study, we found the key predictors of CCS uptake which include age, having a larger number of children, regular menstrual function, awareness of Pap smear test, and free screening programme for CC, and the causative association of HPV with CC. Furthermore, the study revealed the significant role of healthcare professionals including gynaecologists and general practitioners as key sources of information about CCS. Thus, they can play a critical role to improve the education of women regarding CCS in Kazakhstan.
Supplemental Material
sj-doc-1-whe-10.1177_17455065211004135 – Supplemental material for Factors associated with cervical cancer screening behaviour of women attending gynaecological clinics in Kazakhstan: A cross-sectional study
Supplemental material, sj-doc-1-whe-10.1177_17455065211004135 for Factors associated with cervical cancer screening behaviour of women attending gynaecological clinics in Kazakhstan: A cross-sectional study by Torgyn Issa, Aisha Babi, Azliyati Azizan, Raushan Alibekova, Saleem A. Khan, Alpamys Issanov, Chee Kai Chan and Gulzhanat Aimagambetova in Women’s Health
Footnotes
Acknowledgements
The authors would like to acknowledge the Nazarbayev University School of Medicine for the support that enabled completion on this review article.
Author’s contributions
T.I., A.B., and G.A. collected the surveys. T.I., A.B., C.K.C., and A.I. compiled, analysed, and reviewed the data. G.A., C.K.C., and A.A. prepared the article. S.K. and A.A. provided intellectual input to contribute towards article preparation and edited the article. All authors reviewed and approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Faculty Development Research Grant Programme 2019–2021 (Funder Project Reference: 110119FD4528, title: A molecular epidemiological study to determine the prevalence of oncogenic HPV strains for CC prevention in Kazakhstan). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the article. G.A. is a principal investigator of the project.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.