
Abstract
Objectives
To determine which groups of women would be most likely to take part in self-sampling for cervical screening, and what they perceive as the key barriers and benefits to self-sampling.
Methods
A random sample of 3000 women aged 18–69 in Victoria, Australia, were asked questions about “taking their own Pap test” in a telephone survey about cervical screening; 2526 answered the questions about self-sampling. The terminology “Pap test” was used in questions, due to the very low understanding of HPV and its link to cervical cancer.
Results
One-third of women (34.0%) indicated they would prefer to self-sample, 57.2% would not and 8.7% were unsure. Preference for self-sampling was significantly stronger among women who had not had a Pap test for more than three years (64.8%, p < .001) or who had never had one (62.1%, p < .001), compared with those up-to-date (27.0%). Convenience was a key benefit (37.8%), as was less embarrassment (31.5%). For those who did not want to self-sample or were unsure, key factors included professionals being more skilled (53.4% and 28.2% respectively), and doubts about being able to do it properly (28.9% and 23.6%).
Conclusions
Self-sampling was most popular among women who needed to have a Pap test, and could potentially reach some women who are not participating appropriately in cervical screening. Key barriers to participation could be addressed by providing information about the test being for HPV, and being easier to do properly than a Pap test.
Introduction
Australia’s National Cervical Screening Program (NCSP) began more than 20 years ago, and has led to substantial decreases in age-adjusted cervical cancer incidence (13.3 per 100,000 in 1991 to 6.7 in 2009) and mortality (4.0 per 100,000 in 1991 to 1.9 in 2009). 1 The National Human Papilloma Virus (HPV) Vaccination Program, which commenced in 2007, will contribute to further declines in incidence and mortality over time. 1 However, receiving the HPV vaccine does not preclude the need for regular cervical screening. Current Australian guidelines state that all women aged 18 to 69 who have ever been sexually active should participate in cervical screening every two years, regardless of vaccination status. 2 Women are not invited into the NCSP and the woman, or her health care provider, must initiate cervical screening.
The main factor limiting the effectiveness of screening programmes is low participation, or failure to participate frequently enough. In the Australian state of Victoria, 50% of women diagnosed with invasive or micro-invasive cervical cancer in 2011 had no known screening history, and a further 28% had not been screened for at least two and a half years prior to their diagnosis. 3 In Victoria, strategies to encourage initiating and maintaining appropriate cervical screening have included mass media advertising and reminder letters for women with overdue Pap tests.4,5 Nonetheless, just 60% of women in the target age range (20–69) had been screened at the recommended two year interval in 2011–2012. 3
A variety of socio-demographic factors affect participation in cervical screening. Aboriginal and Torres Strait Islander women have three times the cervical cancer incidence of non-Indigenous Australian women, which is believed to be related to reduced participation in screening, although definitive figures on Indigenous screening participation are not currently collected. 6 It has also been suggested that women from Asian and middle-Eastern backgrounds are less likely to be screened than Australian-born women. 7 In Victoria, the incidence of invasive cervical cancer is inversely related to socio-economic status, as is participation in screening. 4
As well as socio-demographic factors, individual barriers to cervical screening include emotional issues such as embarrassment, or fear of pain and discomfort associated with having a Pap test, and practical issues such as difficulty in finding either the time to have the test or an appropriate doctor. An English study found that practical barriers were the biggest issue women needed to overcome; other studies have placed more importance on the emotional barriers.8–10
A possible solution to some of these barriers may be HPV self-sampling, in which a woman collects her own sample from the vagina using a swab, brush or a lavage-like device, to test for the presence of HPV DNA. HPV DNA testing, whether self-collected or collected by a physician, is more sensitive than current cervical cytology. A review including eight North American and European studies found HPV DNA testing to be substantially more sensitive in detecting CIN2 + than cytology (96.1% versus 53%) but less specific (90.7% versus 96.3%). 11
Randomized controlled trials12–21 found participation in cervical screening to be significantly higher if women were sent an HPV self-sampling kit rather than an invitation letter for a Pap test, though participation rates in self-sampling arms of the trials varied widely between countries. Studies have also shown self-sampling to be generally acceptable to women, athough uncertainty about performing the sampling correctly, or confidence in the physician’s procedure, was a concern observed across cultural, religious, and ethnic groups.22–25
In Australia, self-sample tests are not publically available (this may change with the renewal of the cervical screening programme 26 ), and it is unlikely that there is currently any public awareness that self-sampling is even possible for cervical screening. This provides a unique opportunity to explore support for self-sampling among Victorian women when they are made aware of the possibility. If self-sampling is introduced, this understanding will help with the development of appropriate communication strategies to address any barriers. This study used a population survey to determine the potential level of participation in self-sampling, and the demographic groups most likely to participate. It also aimed to identify women’s reasons for preferring either self-sampling or conventional Pap test screening.
Methods
Participants and Procedures
A telephone survey of Victorian women was commissioned by the Centre for Behavioural Research in Cancer in October and November 2012. The sample was generated using exchange-based random digit dialling, and trained female interviewers contacted 10,873 households asking to speak to the youngest woman aged between 18 and 69. In 4454 households an eligible participant was identified and an interview was obtained in 67.4% of these households; 3000 women completed the survey and 1454 did not. 27 Up to nine attempts were made to reach each selected number. The sample consisted of women who could complete the interview in English, and was stratified by metropolitan Melbourne and regional Victoria according to the population distribution. 28
Women were asked: “A new way of taking a Pap test is for women to take their own sample. They would do this at home and then mail the sample. If this method was available, would you prefer to do this, instead of going to a health professional for a Pap test?” Responses were classified as yes, no, and unsure. Although the test is not actually a “Pap test”, understanding of HPV in general, and HPV testing specifically, is poor, so asking women about doing an HPV test themselves would not provide any valuable information. Women were then asked the reasons for their response, and these were coded into categories by the authors, and any discrepancies discussed until concordance was reached.
Ethical approval was provided by the Cancer Council Victoria Human Research Ethics committee.
Statistical analysis
All data were weighted according to the age distribution of metropolitan Melbourne and country Victoria using Australian Bureau of Statistics (ABS) 2011 figures, 28 to ensure that the data were representative of Victorian women. Respondents’ age was aggregated into three categories (18–29, 30–49 and 50–69). 28
The 2011 Socio-economic Index For Areas (SEIFA), a composite measure of the relative socioeconomic disadvantage in a particular geographic area, as determined by postcode, was also applied to the dataset. 29 Respondents were classified into tertiles (low, middle, high) according to their SEIFA score.
Descriptive statistics were used to describe the data, and chi-square tests were used to explore the relationship between demographic characteristics. A p-value of less than 0.05 was deemed statistically significant, and 95% confidence intervals are reported where appropriate. Multivariate logistic regression was performed to examine the relationship between self-sampling preference and socio-demographic characteristics. Binary categories of “prefer to self-sample” and “all other responses” (no and unsure) were created. Outcomes were compared across age, location of residence, Socio-economic status (SES), and time since last Pap test, adjusting for covariates. The regression model did not include language spoken at home, and treated those who had not been screened for more than three years as one group, due to the small cell sizes. Adjusted odds ratios with 95% confidence intervals are reported. Analysis was conducted using SPSS (version 20.0). 30
Results
Socio-demographic characteristics of the respondents (n = 2625).
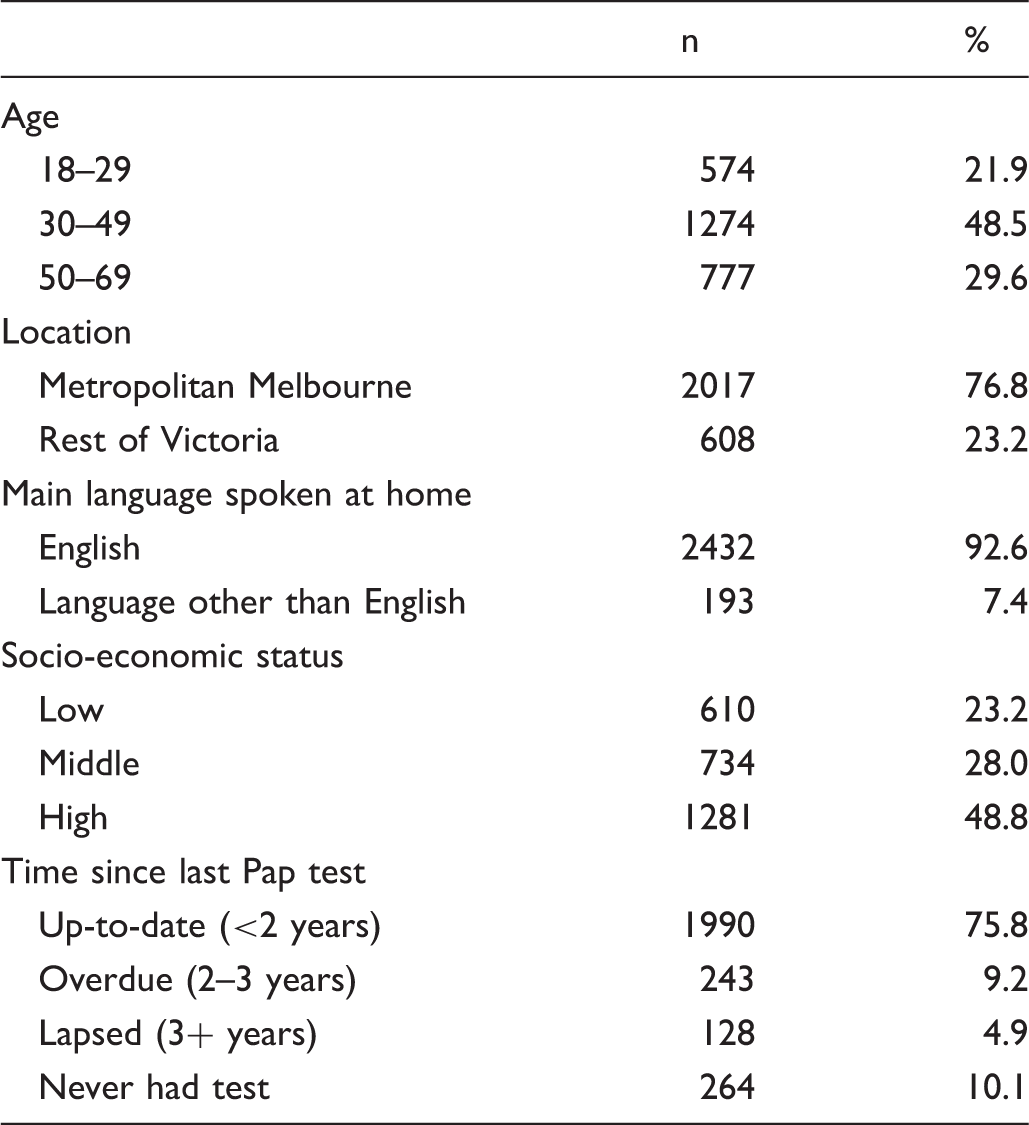
Age was significantly associated with time since last Pap test. Women aged 18–29 were less likely to be up-to-date with screening (51.7%) than women aged 30–49 (82.3%) or 50–59 (83.1%) (χ2(6) = 850.7, p < 0.01). Location and SES were not significantly associated with time since last Pap test.
Multivariable logistic regression of preference for self-sampling (n = 2625).
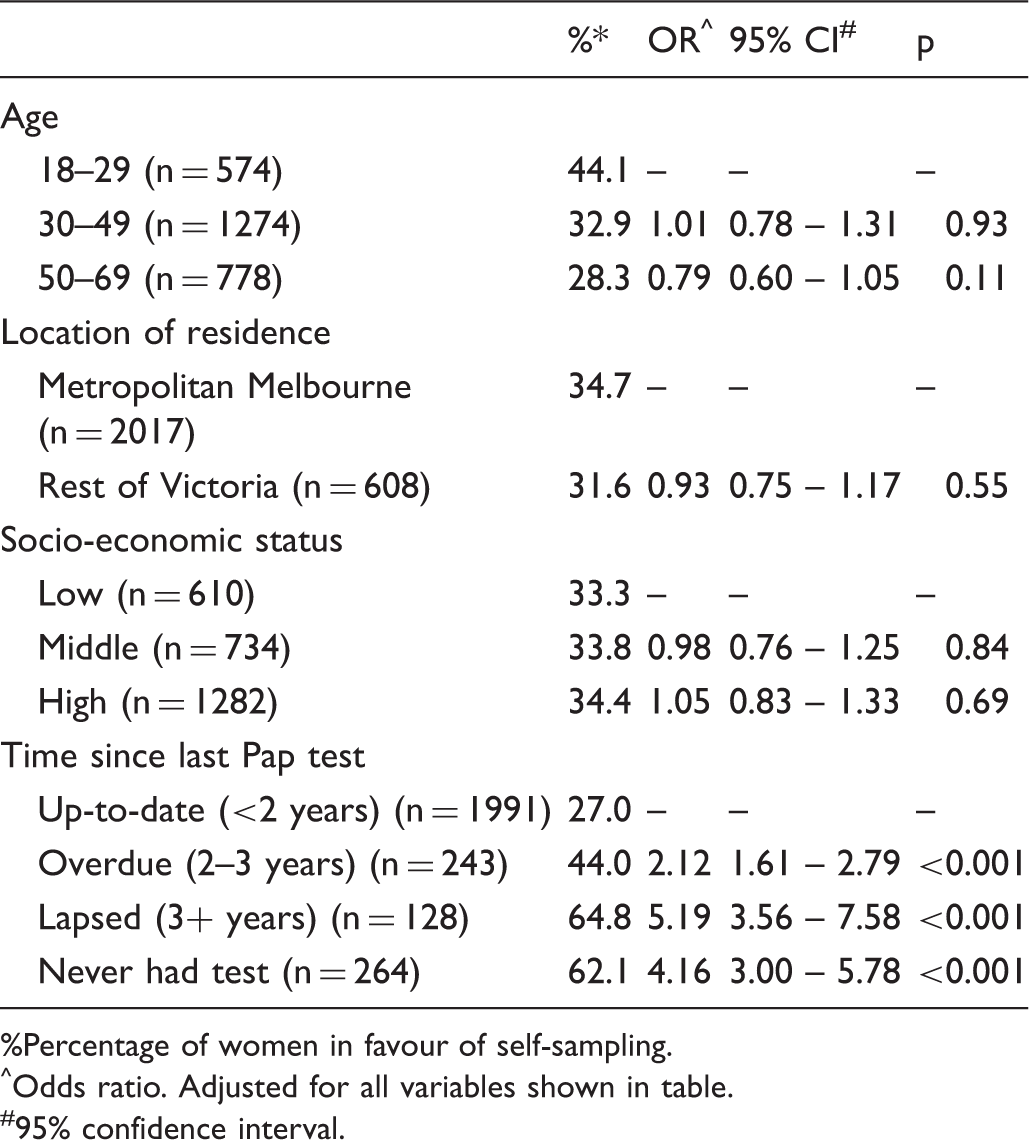
Percentage of women in favour of self-sampling.
Odds ratio. Adjusted for all variables shown in table.
95% confidence interval.
Multivariate analysis adjusting for time since last Pap test, age, location, and SES found that only time since last Pap test was a significant factor in self-sampling preference. Compared with women whose Pap test was up-to-date, those overdue for a test were 2.12 times more likely to prefer self-sampling, women who had lapsed in their screening were 5.19 times more likely, and those who had never had a Pap test were 4.16 times more likely to prefer self-sampling.
Top four reasons given for self-sampling preference.
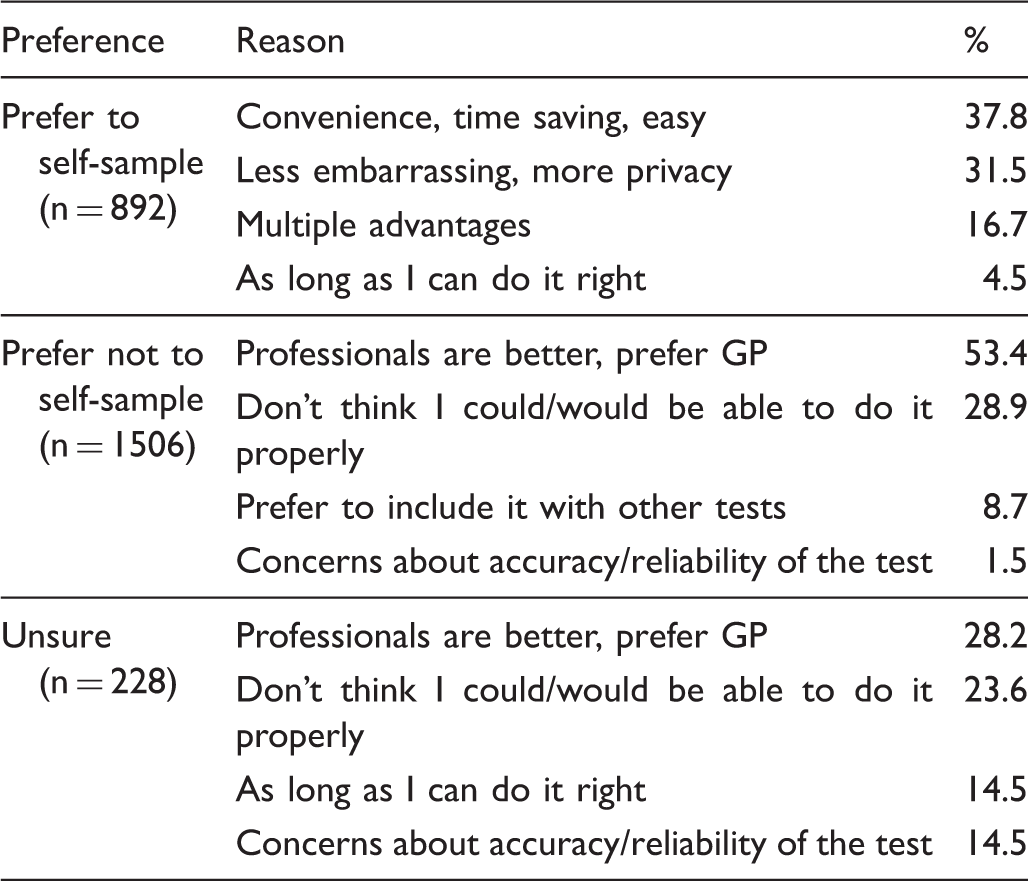
Among women who would prefer to self-sample, the most common reasons were that it would be convenient, time saving or easy (37.8%), and that it would be less embarrassing and afford more privacy than a standard Pap test (31.5%). For women who preferred not to self-sample, over half considered that health professionals are better equipped to accurately perform the test (53.4%), with many women worried about being able to do the test properly on their own (28.9%). Among women who were unsure about self-sampling, some responses indicated they were not likely to do it, with health professionals being better (28.2%) and women not being able to do the test properly themselves (23.6%) being key responses for this group as well, but others possibly could be swayed if they thought they could do it properly (14.5%) and were convinced the test was reliable and accurate (14.5%).
Discussion
This study provides valuable information about the level of support self-sampling could receive from Australian women, even before they are provided with full information about the test or its benefits. Around one-third of women said that they would prefer to self-sample, with acceptance significantly higher among those who most need a test. Around two-thirds of women who had never had a Pap test, or had not had one for over three years, preferred self-sampling.
Support for self-sampling was no stronger among women who lived in regional Victoria, although they may have poorer access to medical professionals to conduct a Pap test. This may not be the case in other parts of Australia, where geographical isolation is a far greater factor. Victoria is a relatively small state, with few areas classified as remote or very remote, and the majority of women in the survey were up to date with their Pap tests, so clearly they were able to access healthcare for cervical screening if they wished.
SES is known to have an impact on cervical screening rates, with women from areas of high average SES more likely to be up to date with screening. 4 One review suggests that the most deprived women will be least likely to accept self-sampling, 31 but in our study, there was no significant difference in the preference for self-sampling by women in different SES groups. Thus, if self-sampling becomes available as part of an organized screening programme it may not address the fundamental disparity in screening currently found across socio-economic groups, but there is no indication that it will exacerbate it. A limitation of our study is that postcodes rather than individual measures were used to determine area-level SES, which may not be as accurate for all participants. A possible future strategy for distributing self-sampling kits could be to use postcodes to identify locations where both screening and SES is low, and to distribute self-sampling kits to women in those areas. Thus, the broader measure of area level SES could be the most appropriate.
The reasons provided by some women for preferring not to self-sample are less issues with self-sampling itself, but more an indication of a preference for seeing their doctor. These women like to combine their Pap test with other tests or procedures, and do not want to give up the visit to the doctor as they had more confidence in the doctor’s ability This has been shown to be an issue in other studies of women from different ethnic and cultural backgrounds.24–25
The question used in this survey was not strictly accurate, as we used the term “Pap test” rather than “HPV test”. This was deliberate, as women have little understanding of HPV or what an HPV test would involve, 32 whereas most are aware of Pap tests and what they entail. HPV tests are actually easier to perform accurately than Pap tests, as there is not the same need to sample cells from a specific part of the cervix. Some of the women who doubted their ability to self test might be persuaded to try a self-sample for HPV if they understood this, and this should be a key component of any communication with women.
The key limitation to this study was that it was conducted in English, with over 92% of respondents reporting that they spoke English at home. It does not give any information about how women from some community groups, which are believed to be under-screened, such as new migrants, might respond. Only ten women in the survey identified themselves as Aboriginal and Torres Strait Islanders, so the study was unable to shed any light on the possible uptake of self-sampling among this group. The small size of the Aboriginal and Torres Strait Islander population in Victoria, as well as the diverse number of languages spoken by migrant communities, make these groups very difficult to include in such telephone surveys.
Because intention does not necessarily predict behaviour, it remains to be seen how many women would actually participate in self-sampling if given the opportunity. Nevertheless, the study does indicate widespread support for the general concept of self-sampling, even in the absence of any communication to raise awareness of the possibility. The way in which self-sampling is presented will be crucial in gaining acceptance from women, and is an important topic for further research.
Overall, this survey indicated that self-sampling is a promising technology, which has the potential to reach women who have traditionally not engaged in Pap testing, or at least not engaged at appropriate frequency. A trial of the uptake of HPV self-sampling among under- and never-screened women currently underway in Victoria will determine actual participation rates among the most at-risk groups.
Footnotes
Funding
The study was funded by PapScreen Victoria. PapScreen is a joint Commonwealth-State funded programme delivered by Cancer Council Victoria.