
Abstract
Objective
To examine the state of cervical screening and prevention in Central Asian states, specifically Kazakhstan.
Results
In the five Central Asian countries that were formerly part of the Soviet Union (Kazakhstan, Kyrgyzstan, Tajikistan, Turkmenistan, and Uzbekistan), cervical cancer incidence and mortality rates are far higher than those in most Western and high-income nations, and are increasing. Cervical cancer screening is available in all five countries, but is mainly opportunistic. Only Kazakhstan has a structured cytological screening program, from which screening coverage analysis is possible.
Conclusion
Despite significant decreases in cervical cancer incidence and mortality in developed countries, the problem is still of great concern in these Central Asian countries and is attributed to poorly organized screening and the absence of vaccination programs.
Introduction
More than 80% of deaths due to cervical cancer (CC) occur in low- and middle-income countries. 1 In many low-income countries, there are no organized CC screening programs, and only opportunistic screening is conducted. The most common screening method is cytology, though in some high-income countries human papillomavirus (HPV) DNA testing is now used, either as primary screening or in addition to cytology screening. In low-resource settings, visual inspection with acetic acid is an option for CC screening. The most recent European Guidelines and the World Health Organization now recommend HPV testing as the primary CC screening tool. 2 HPV genotyping may be suitable and worth employing as a primary HPV screening for low- and middle-income countries who have not previously had CC screening programs. 2 Data from recent years show that HPV vaccination is very effective in preventing infection and disease related to specific HPV genotypes. 3 Data from developed countries, including Australia, Canada, USA, and Sweden, demonstrate vaccine effectiveness and show a decrease in prevalence in targeted types following HPV vaccination. 1 In developing countries, however, there are many challenges in implementing vaccination, including financial limitations. 3
Kazakhstan is one of the five Central Asian (CA) countries (which also include Kyrgyzstan, Tajikistan, Turkmenistan, and Uzbekistan) that achieved independence in 1991. 4 The collapse of the Soviet Union led Kazakhstan and these other republics into economic recession. The healthcare systems in these republics have undergone many decades of profound revolutions, as a result of which the rate and quality of healthcare progress varies between the countries. 4
Discussion
The combined population of CA countries in 2018 was around 70 million, half of whom were female. More than 25 million women in CA countries were aged over 15, and so were potentially infected by HPV. 1 The overall CC incidence in CA countries was 4555 cases (crude rate 12.5) and mortality was 2369 cases (crude rate 12.3). 1 There is considerable diversity in the incidence rates of CC in CA republics. CC incidence ranges from 5.7 per 100,000 women in Tajikistan to 19.9 per 100,000 in Kyrgyzstan, and the mortality rates range from 3.2 per 100,000 women in Tajikistan to 10.9 per 100,000 in Kyrgyzstan (Table 1). 1 These rates are much higher than those in high-income countries such as America, and Western and Northern Europe. In the United States and Canada, CC incidence is 6.5 and 5.7 per 100,000 women, respectively, and mortality rates are 1.9 and 3.1 per 100,000 women, respectively. In Switzerland, CC incidence is 3.8 and mortality is 1.1 per 100,000 women, and in Finland incidence is 4.7 and mortality is 0.9 per 100,000 women. 1
Cervical cancer screening and HPV vaccination in Kazakhstan and Central Asia.
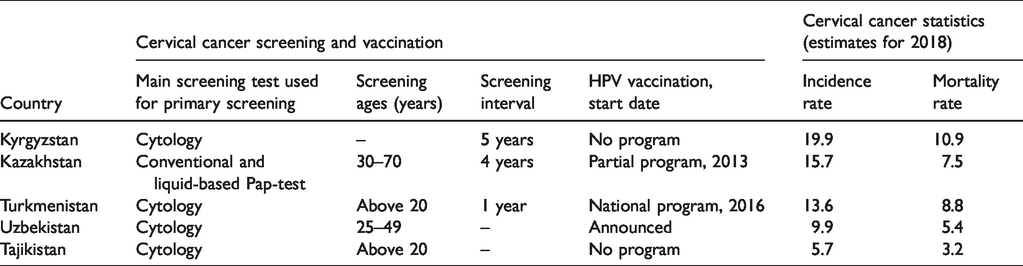
CC screening is currently available in all CA countries, but it is mainly opportunistic with no active process of invitation. It is characterized by cytology testing using Romanowsky staining, with generally low or unreported coverage (Table 1).1,5 In Kazakhstan, up to 2005, CC screening using Romanowsky staining was mainly opportunistic.5,6 Since 2005, cytological CC screening has been conducted under governmental auspices, initially covering women aged 30–34, and from 2006–2007 covering women aged 18–49. 6 Among CA countries, CC screening coverage data analysis is accessible only for Kazakhstan. The available resources clearly show that, within the nine-year period 2008–2016, coverage decreased by 27%, from 72.9% in 2008 to 45.9% in 2016, with the highest coverage in 2012. 7 In 2017, the CC screening algorithm in Kazakhstan was changed by the Ministry of Health (order#995, see Table 1). In general, the CC screening program in Kazakhstan is improving and expected to contribute to the reduction of the CC incidence and mortality.
Among the CA countries, Kyrgyzstan exhibits the highest CC incidence and mortality rates.1,8 There was no CC screening program in Kyrgyzstan till 2013.5,8 Cytological CC screening has now been introduced, 1 but we have been unable to identify whether there is a government program that regulates age groups covered by the screening (Table 1). Tajikistan had no CC screening program until the end of 2009, when a national program on preventive maintenance, diagnostics, and treatment of malignant neoplasia was established. This program is undergoing extension planned from 2010 through 2015.5,8 In Turkmenistan, a national CC screening program was introduced in 2007, and annual cervical cytological tests and colposcopy were initiated in 2010 (Table 1). In Uzbekistan, opportunistic screening with low coverage was originally in place in different regions. In 2010, organized cytology screening using Papanicolaou tests was initiated in the most populous part of the country, 5 with 25,000 women aged 25–49 offered follow-up for abnormal cytology and treatment.
HPV vaccination coverage in Kazakhstan and the other CA countries is poor. Only Turkmenistan has implemented a national vaccination program in 2016. 1 In Kazakhstan, a pilot vaccination program was started in 2013, but was not followed by full implementation as it did not receive support on the state level. There is also a lack of governmental HPV testing programs in CA countries. 5 HPV testing is available on a self-payment basis, which is mostly accessible only in large cities.
To address the high CC incidence and mortality rates, there is an obvious need for efficient organized screening systems and quality-controlled cytology services. A better CC screening infrastructure is present in Kazakhstan compared with the other CA countries; however, the lowest incidence and mortality rates are reported in Uzbekistan and Tajikistan, 1 which does not correlate with the screening and vaccination program development. Another problem with CC screening in Kazakhstan and CA countries relates to the guidelines routinely used for the management of patients with abnormal cervical cytology. Currently, the specialists dealing with screening are utilizing different international guidelines. The guidelines of the American Cancer Society and the American Society for Colposcopy and Cervical Pathology, which are found to be effective all over the world, have not been adopted by the health policymakers in Kazakhstan. 9
Although there are multiple risk factors involved, the increasing trend of CC in developing countries can be attributed mainly to poorly organized screening and lack of vaccination programs. 10 Despite the significant progress in the decrease in CC incidence and mortality in developed countries, the problem is still of great concern in low- and middle-income countries.
Conclusion
Despite definite progress achieved, CC remains an important healthcare issue in Kazakhstan and the other CA countries. While effective screening policies and vaccination would have reduced the CC rates across screening ages in CA countries (as seen in developed European and American countries), CC incidence and mortality rates in CA countries are increasing, as a result of poorly organized screening programs and the lack of HPV vaccination. It is necessary to establish national screening and vaccination programs in Kazakhstan and the republics of Central Asia to help to reduce CC mortality.
Footnotes
Authors’ contribution
CKC and GA compiled analyzed and reviewed data and prepared the manuscript. TU, BI, AB, and KK contributed information related to epidemiology and screening programs. AA provided intellectual input to contribute towards manuscript preparation and edited the manuscript. All authors reviewed and approved the final manuscript.
Acknowledgements
The authors acknowledge the Nazarbayev University School of Medicine for the support that enabled completion of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.