
Abstract
Background:
The relationship between women’s empowerment and modern contraception utilization is well documented; however, they focused on all reproductive-aged women and lacked dimensions of empowerment. Research focusing only on women who have no desire for more children is scarce. Understanding the use of modern contraceptives and their relationship to women’s empowerment in this demographic is critical for reducing unwanted pregnancies, abortions, and fertility rates.
Objective:
This study aimed to investigate the relationship between women’s empowerment and the use of modern contraception among South Asian women who have no desire to have more children.
Design:
A cross-sectional study design utilizing Demographic and Health Survey data from 2015 to 2022 across five South Asian countries was employed.
Methods:
This investigation examined aggregated data from 42,573 currently married, fecund, non-sterilized, non-pregnant South Asian (Afghanistan, Bangladesh, India, Nepal, and Pakistan) women aged 15–49 who had no desire for additional children. The survey-based women’s empowerment composite index was employed to assess empowerment. A multilevel mixed-effects logistic regression analysis was utilized to explore the relationship of interest.
Results:
The prevalence of modern contraception usage among South Asian women without a desire for more children stands at 45.8%, with Pakistan exhibiting the lowest rate at 31.8% and Bangladesh the highest at 67.8%. In South Asia, high empowerment among women regarding attitudes toward violence (adjusted odds ratio: 1.17; 95% confidence interval: 1.08–1.25), social independence (adjusted odds ratio: 1.22; 95% confidence interval: 1.13–1.33), and decision-making (adjusted odds ratio: 1.11; 95% confidence interval: 1.01–1.23) is associated with a greater likelihood to utilize modern contraception compared to their less empowered counterparts. A comparable pattern of correlation appeared in specific countries, with few exceptions.
Conclusions:
The degree of women’s empowerment shows a positive correlation with the use of modern contraception in patriarchal and conservative South Asian contexts, a circumstance, that is, pertinent in developing nations with various cultures. Family planning initiatives in South Asia should focus on integrating women’s empowerment.
Plain language summary
Women’s empowerment and universal access to sexual and reproductive health are central to the Sustainable Development Goals. Prior evidence indicates a positive connection between women’s empowerment and the use of modern contraception; however, those studies used limited aspects of empowerment and focused on all women aged 15 to 49 years. This study assessed such a relationship among South Asian women who have no desire for additional children, who are expected to be more likely to utilize modern contraception to avoid pregnancy.
The researchers employed a newly developed empowerment index derived from demographic health survey data to evaluate its correlation with modern contraceptive use among women without a desire for additional children in five South Asian countries.
The researcher found that fewer than 50% of South Asian women without a desire for more children utilize modern contraception (45.8%). In an aggregated sample from South Asia, women exhibiting high empowerment in the domains of attitudes towards violence (the degree to which they reject domestic violence), social independence (encompassing access to information, education, and the age of marriage and first childbirth), and decision-making (pertaining to significant household decisions) were more inclined to utilize modern contraception. The researcher noted that various domains of empowerment correlated with the utilization of modern contraception differentially among countries.
This study delineated various empowerment dimensions across South Asian countries to inform future initiatives aimed at increasing modern contraceptive utilization. Increasing resources for education, creating gender-sensitive curriculum, and effectively utilizing mass media could boost women’s empowerment and the use of modern contraceptives in conservative patriarchal South Asian countries.
Keywords
Introduction
Recent estimates indicate that between 2015 and 2019, there were 121.0 million unintended pregnancies, which are defined as pregnancies that are either unwanted or mistimed, translating to a global rate of 64 unintended pregnancies/1000 women aged 15–49 years. 1 Data indicate that the incidence of unintended pregnancy has decreased globally, 2 with enhanced access to and utilization of contraceptive methods likely playing a significant role in these developments. Despite advancements, around 214 million women of reproductive age in developing regions are not using a modern contraceptive method, even though they wish to prevent pregnancy. 3 Additionally, the prevalence rate of modern contraceptive use among married women in low- and middle-income countries (LMICs) has remained unchanged at ~53% over the past two decades. 4 In the South Asian region, it is reported that one in every five pregnancies is unintended, 5 while the usage of modern contraceptives stands at 42%. 6 Furthermore, various challenges in advancing family planning and contraceptive use, particularly in LMICs, have resulted in a slow global increase in modern contraceptive prevalence rates. The progress in addressing the need for family planning has been inconsistent across different nations. Consequently, LMICs face significant challenges in attaining universal access to sexual and reproductive health care services, as outlined in the sustainable development goals (SDGs).7,8
The utilization of contraception is essential to reproductive health, and women’s right to access these methods has enduring effects on the health of mothers, children, and the broader community.9,10 The utilization of modern contraceptives can mitigate the adverse health consequences linked to early childbearing, low birth spacing, and elevated fertility rates. 11 The use of modern contraception correlates with decreased mother and newborn mortality by preventing unwanted and adolescent pregnancies and aids in the spacing, timing, and limiting of births. 12 Research indicates that access to contraception empowers women and fosters gender equity 13 while also enhancing women’s paid employment and yielding various benefits for society and the economy.14,15 This advantage is partly due to the fact that postponing childbearing enables women to pursue education and acquire work experience. 15 Access to modern contraception also serves as a technique to mitigate expenses for health systems and households by lowering healthcare costs related to maternal and child health. 16
Country-disaggregated data from South Asian countries reveal notable disparities in the use of modern contraceptives, rates of unintended pregnancies, and fertility rates, both across and within countries.5,17 Commonly identified obstacles to the use of modern contraceptives among South Asian women encompass cultural norms, insufficient knowledge of methods, apprehension regarding side effects, and religious limitations.18,19 Nonetheless, the varied religious and geopolitical landscape among South Asian countries necessitates a detailed analysis of the disparities in the use of modern contraception among women who have no desire to have more children across these nations. Despite the diversity, all these countries exhibit a comparable development status and sociocultural environment regarding the prevailing conservatism surrounding sexual and reproductive health issues. In South Asian countries, the interactions between spouses and the status of women within family or societal frameworks can greatly impact reproductive decision-making. Gender equality, especially among spouses, is a vital element in defining this authority and arises from the increased decision-making capacity of women, known as empowerment.20,21 In low- and middle-income nations, the promotion of gender equality and women’s empowerment has become a vital component of social programs, recognized as both fundamentally important and indispensable for economic growth and development. 22 Evidence suggests that increased women’s empowerment can improve household efficiency, enhance family welfare, encourage contraceptive usage, and decrease unwanted fertility.22–25
A substantial corpus of literature has been developed that examines women’s empowerment across various dimensions and evaluates its correlation with the utilization of modern contraceptives. For instance, the use of modern contraceptives has been linked to involvement in household decision-making,23,26–29 economic decision-making, 30 tolerance of domestic violence,28,31,32 freedom of movement,23,33 and possession of assets such as land, mobile phones, and bank accounts. 34 Nonetheless, these studies offer a limited perspective on women’s empowerment for comprehending this relationship. This study seeks to investigate the relationship between women’s empowerment and the use of modern contraception among women who have no desire to have more children, employing the validated survey-based women’s empowerment (SWPER)35,36 index to inform the empirical analysis. Women’s empowerment is challenging to quantify due to its ambiguous and complex nature. Empowerment is multifaceted and can manifest across various levels. 37 Nonetheless, the significance of specific dimensions or levels remains a subject of debate. The empowerment module of the Demographic and Health Survey (DHS) has proposed various indices in developing countries that encompass inquiries regarding women’s involvement in household decision-making, attitudes toward domestic violence, control over financial resources, employment status and income type, as well as personal ownership of land or property.23,26–34 The subjective weighting and tailoring of these indexes to specific nations or small groups of nations limits their comparability with other countries. 35 Furthermore, Akseer et al. 38 employed various indices to assess the empowerment of women in Islamic nations. Numerous additional group-level measures, such as the Gender Gap Index, 39 the Gender Development Index, and the Gender Inequality Index, 40 have been suggested at the national level. These indicators do not allow for subnational analysis or subgroup comparisons. Ewerling et al. developed the SWPER index, utilizing individual-level DHS data from 34 African countries, to effectively encapsulate the multifaceted and intricate nature of women’s empowerment, facilitating comparability across nations and temporal contexts. 35 SWPER Global has recently been developed and validated in 62 LMICs, including Bangladesh. 36 The SWPER index was developed with a standardized set of questions from the DHS data and subsequently tested against the established Gender Development Index.
The SWPER index has been used to study its relationship with modern contraception worldwide,41,42 including South Asian countries.26,43,44 Nevertheless, the results of these investigations exhibit a lack of consistency. A study conducted in African nations, specifically Nigeria and Zambia, revealed that within the three domains of the SWPER, the domain concerning attitudes toward violence was linked to the use of modern contraception. 42 Conversely, research in Bangladesh indicated that only the decision-making domain was associated with the utilization of modern contraception. 26 Nevertheless, an alternative study conducted in Bangladesh indicated that all three domains of the SWPER index were correlated with contraception use, albeit with reduced odds. 43 Another study in India indicated that women exhibiting more permissive views toward domestic abuse and possessing lower degrees of social independence demonstrated a greater demand for family planning fulfilled by modern contraceptive methods. 44 The existing comprehension of the interplay between women’s empowerment and the utilization of contraception is still lacking in completeness. Furthermore, while all the studies have acknowledged the significance of women’s empowerment in the adoption of modern contraceptive methods, none has examined these relationships among women who do not intend to bear another child, a demographic for whom such insights are vital in preventing unwanted pregnancies and fulfilling reproductive goals. Consequently, examining the relationship between women’s empowerment and the use of modern contraceptives, especially among those who desire to have no additional children, is significant for comprehending future trends in contraceptive use and fertility patterns.
South Asian countries have entrenched patriarchal structures. Patriarchal norms in this region appear in various forms, including son preference, regressive gender norms, diminished women’s empowerment, and a kinship system favoring males. 45 Moreover, in South Asian religious contexts, patriarchal norms interlace with many religious traditions, creating power dynamics and gender relations while profoundly impacting women’s autonomy and agency. Patriarchal norms, in their various dimensions, may constrain women’s choices and opportunities,46,47 including their roles in domestic spheres, access to education, employment, financial services, and participation in civil society and political institutions, resulting in detrimental demographic outcomes, such as increased fertility rates and decreased contraceptive use.48,49 Such restrictions may undermine women’s control over their reproductive choices. Understanding the elements that support women’s ability to control their reproductive health is crucial as South Asians strive toward the SDG of ensuring universal access to family planning, contraception, and reproductive health. The inconsistent findings regarding the relationship between women’s empowerment and contraceptive use, coupled with the broad spectrum of women’s empowerment, highlight the necessity for additional research to evaluate these relationships in conservative South Asian countries. This study aims to investigate the correlation between women’s empowerment and the use of contemporary contraception among reproductive-aged South Asian women who have no desire for more children, employing both pooled and disaggregated analyses. The research hypotheses assert that enhanced women’s empowerment is associated with a greater use of modern contraception. This study’s findings will furnish evidence to guide decision-makers and stakeholders in family planning to enhance women’s access to sexual and reproductive health services, particularly modern contraceptives, in South Asia.
Methods
Data sources
This cross-sectional investigation utilized the latest nationally representative standard DHS data from five South Asian nations: Afghanistan, Bangladesh, India, Nepal, and Pakistan. The survey designs employed by the DHS incorporate a stratified multistage sampling approach, dividing each country into administrative regions. Primary sampling units (PSUs) are selected based on probability proportional to population size, employing the latest census data available. In the second stage of sampling, every house within a PSU is listed according to the most recent population census, and ~30 households/PSU are selected at random for an interview. Every individual within the sampled households is listed and has an equal chance of being selected. The approach utilized by the DHS has been documented elsewhere. 50 Participants with missing data for women’s empowerment, contraceptive use, or control variables are excluded using a listwise approach. While listwise deletion, or complete case analysis, remains the predominant method for addressing missing data, some scholars argue that this approach may lead to bias in parameter estimation. Nonetheless, should the assumption of missing completely at random hold true, employing listwise deletion is recognized to yield unbiased estimates and conservative outcomes. In instances where the data do not adhere to the assumption of being missing completely at random, employing listwise deletion could introduce bias into the parameter estimates. 51 Nonetheless, in instances where a sufficiently large sample exists, where power is not an issue, and the assumption of data being missing completely at random holds true, employing listwise deletion could be a reasonable approach. 52 Nonetheless, the sensitivity analysis demonstrated that the results were consistent regardless of whether multiple imputation or listwise deletion was applied to address the missing data. This investigation examined aggregated data from 42,573 currently married, fecund, non-sterilized, non-pregnant South Asian women aged 15–49 who were living with their husbands and had at least one child. Table 1 presents the sample sizes designated by country. The article was prepared using the STROBE guidelines as a framework (Supplement Table 1). 53
Selection of study sample.

Note. DHS: Demographic and Health Survey.
Outcome variable
Current use of modern contraception among women with no desire for additional children is the outcome of interest. We focused on women who have no desire for children, as we anticipate that they are more likely to use contraceptives to prevent conception. Understanding the use of modern contraceptives and their relationship to women’s empowerment is critical for reducing unwanted pregnancies, abortions, and fertility rates. The DHS consistently framed the inquiry about the desire for an additional child to women aged 15–49, and if they did indeed want another child, they were asked to specify their preferred timeframe for childbirth, with the following response options: (i) wants within 2 years; (ii) wants after 2 or more years; (iii) wants uncertain timing; (iv) undecided; (v) wants no more; (vi) sterilized (respondent or partner); (vii) declared infecundity. This study includes solely response option (v), representing women with no desire for additional children. Undecided responses, along with the rest of the response options, were excluded from the study, as previous research indicated that women who were undecided shared characteristics with those desiring additional children and did not demonstrate a clear intention to cease childbearing. 54
The use of modern contraceptives among women with no desire for additional children was determined via a question that inquired about the sorts of contraceptive methods employed by respondents during the survey, with response options being “no method,” “folkloric method,” “traditional method,” and “modern method.” Modern contraceptive methods encompass male and female sterilization, intrauterine devices/postpartum intrauterine devices (IUD/PPIUD), injectables, implants, contraceptive pills, and the lactational amenorrhea method. It also includes emergency contraception, female and male condoms, the standard day method, diaphragms, and foam/jelly, along with country-specific modern methods and other modern contraceptive methods (including cervical caps, contraceptive sponges, and others) mentioned by respondents. Periodic abstinence, including the rhythm and calendar methods, withdrawal (coitus interruptus), and effective country-specific traditional methods were classified as traditional methods. Locally described methods, such as herbs and massage, which have unproven effectiveness, 55 were classified as folkloric methods. Women utilizing modern methods were designated a code of 1, whereas those not using any methods or relying on traditional or folkloric methods were designated a code of 0. We concentrated on the utilization of modern contraceptive methods among women who have no desire for additional children, as these methods demonstrate greater efficacy in avoiding pregnancy compared to traditional or folk methods. 55
Exposure variable
The measurement of women’s empowerment was conducted using the SWPER Global, which serves as an individual-level indicator for women aged 15–49 who are married or in a union. 36 Details of the SWPER indicator and its validity can be found elsewhere. 36 Principal component analyses of 14 DHS questions covering three areas of women’s empowerment are used to derive the SWPER: (a) attitudes toward violence, specifically the extent to which women reject domestic violence; (b) social independence, which pertains to access to information, education, and the age at marriage and first birth; and (c) decision-making, which involves making decisions regarding significant household matters. The scores were standardized, where positive values reflect above-average empowerment and negative values denote below-average empowerment. A value of zero signifies that the woman exhibits an average degree of empowerment compared to the cohort of LMICs used to construct the index.35,36 We employed the recommended cut-off points defined by the authors, 36 which categorize global scores into tertiles. The SWPER domain was categorized into low, medium, or high levels of empowerment based on the proposed threshold values.
Control variables
The development of the SWPER involved a comprehensive consideration of various socio-demographic variables; therefore, six variables were controlled for in this study, which included current age (15–24, 25–34, and 35–49 years), the number of living children (1, 2, and ⩾3), the perceived ideal number of children (0–2, 3–4, and ⩾5), and current working status (yes or no), as well as contextual-level variables like wealth index (poorest, poorer, middle, richer, and richest) and place of residence (urban or rural). The selection of these variables was informed by their impact on the utilization of modern contraception as indicated in previous studies,24–27,56,57 as well as their presence in the DHS dataset.
Statistical analysis
In the case of pooled datasets, we undertook the process of denormalizing the sampling weight and subsequently established a new population-level weight by dividing the sampling weight by the denormalized weight. A unique cluster variable was constructed by integrating country and cluster numbers. The population-level weight and distinct cluster were utilized to compute the pooled estimates. At the outset, we utilized a weighted descriptive analysis to evaluate the distribution of the respondents’ background characteristics. Chi-square tests were employed to evaluate proportional disparities in the utilization of modern contraception, taking into account various domains of women’s empowerment and additional variables. The svy command in Stata 14 was utilized to tackle a complex survey design and enhance the generalizability of the findings. Given the hierarchical nature of the DHS data, sophisticated models—specifically multilevel mixed-effect logistic regression analysis—were employed to investigate the correlation between women’s empowerment and the use of modern contraception among women who express no desire for further children. The results derived from fixed effects are to be understood as odds ratios (ORs), supplemented by a 95% confidence interval (CI). The assessment of random effects was conducted through the application of the intraclass correlation, median OR, and proportional change in variance. We developed four unique nested models tailored specifically for South Asia and its individual nations. At the outset, we constructed a model devoid of any predictors, containing solely the outcome variable. We subsequently integrated individual-level characteristics into Model I and contextual-level variables into Model II. The final model (Model III) encompassed all factors at both the individual and contextual levels. The model’s goodness of fit was evaluated using the log-likelihood ratio (LLR) and the Akaike Information Criterion (AIC) in comparison to previous models. The best-fit model was identified as the one with the highest LLR value and the lowest AIC values. 58 The concluding model (Model III) for South Asia and its respective countries was presented in this study, as it exhibited the highest LLR and the lowest AIC value (Supplement Tables 2–7). Before conducting the multivariable analysis, an assessment of multicollinearity among the variables was carried out through the variance inflation factor (VIF). All variables exhibited low VIF values (<3), indicating a lack of multicollinearity. 59 All statistical analyses were conducted using STATA (version 14.0; StataCorp, LP, College Station, TX), and descriptive analyses were assessed employing two-sided tests. All statistical inferences were performed at a significance threshold of 0.05.
Results
Table 2 outlines the demographic characteristics of South Asian women who have no desire to have more children. Among respondents in South Asia, 50.2% who expressed no desire for additional children were aged 25–34. Approximately 55.0% of women had three or more living children, whereas 58.3% of respondents indicated a preferred ideal number of children between 0 and 2. During the survey period, ~27.1% of women were working, while the majority, 65.1%, resided in rural areas. The percentages of women’s empowerment in various domains in South Asia are presented in Figure 1. About 35.5% of South Asian women reported high levels of empowerment regarding attitudes toward violence, while 21.2% indicated high empowerment in social independence and 59.8% in decision-making. The prevalence of modern contraception use among South Asian women who have no desire for additional children was 45.8% (Figure 2). The highest prevalence was noted in Bangladeshi women (67.8%), whereas the lowest was recorded in Pakistani women (31.8%).
Sociodemographic characteristics of women with no desire for additional children in South Asia (n = 42,573).

Note. CI: confidence interval.
In estimating percentages, the complex survey design and sampling weights were taken into account. Percentages may not total 100.0 because of rounding.

Women’s empowerment in South Asia assessed by the SWPER index.

The prevalence of modern contraception uses among South Asian women.
Table 3 presents the percentage of women using modern contraception, categorized by various domains of women’s empowerment and other sociodemographic variables in South Asia (pooled) and particular countries. In comparison to lowly empowered women, the prevalence of using modern contraceptives was higher among highly empowered women concerning the attitude toward violence (38.3% versus 56.0%; p < 0.001), social independence (41.6% versus 54.3%), and the decision-making (40.6% versus 46.7%; p < 0.001) domains. However, use of modern contraception among women with no desire for additional children was higher among highly empowered women compared to their lowly empowered counterparts in the attitude toward violence domain in Bangladesh (67.3% versus 72.9%; p < 0.001), India (36.1% versus 49.7%; p < 0.001), and Pakistan (30.6% versus 41.2%; p < 0.001). Regarding the social independence domain, the prevalence of modern contraception use was higher among highly empowered women than among less empowered women in all the countries. The prevalence of using modern contraception was also found to be higher among highly empowered women in relation to decision-making in all the countries except Pakistan.
Distribution of modern contraceptive use among women with no desire for additional children by women’s empowerment and other variables in South Asia and by country.
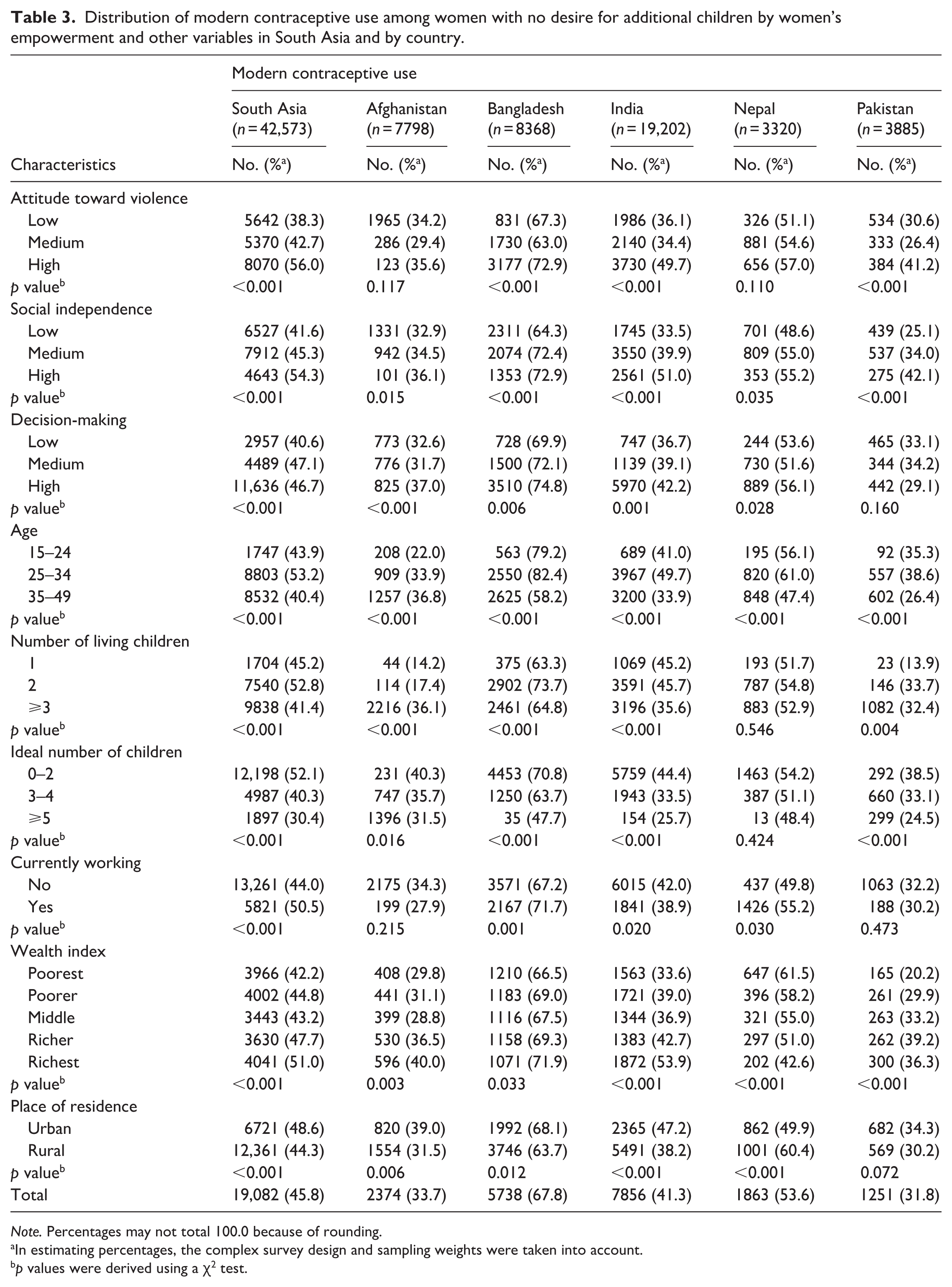
Note. Percentages may not total 100.0 because of rounding.
In estimating percentages, the complex survey design and sampling weights were taken into account.
p values were derived using a ꭓ2 test.
Table 4 presents the outcomes of a multilevel logistic regression analysis examining the correlation between women’s empowerment and the utilization of modern contraception in South Asia (pooled) and specific countries. After adjusting for other sociodemographic factors, the odds of utilizing modern contraception were high among women who exhibited higher empowerment in relation to attitudes toward violence (adjusted OR (AOR): 1.17; 95% CI: 1.08–1.25) compared to those with low empowerment in South Asia. High empowerment in this domain among women in Bangladesh and India was also associated with a higher likelihood of using modern contraception. The likelihood of utilizing modern contraceptives among women with medium (AOR 1.19; 95% CI: 1.13–1.23) and high (AOR 1.22; 95% CI: 1.13–1.33) empowerment levels in relation to social independence was greater than that of low-empowered women in South Asia. All countries, with the exception of Nepal, demonstrated similar outcomes regarding high social independence in contrast to low social independence. Our findings indicate that women exhibiting high levels of empowerment in decision-making are more inclined to use modern contraceptive methods (AOR: 1.11; 95% CI: 1.01–1.23) when compared to those with lower empowerment in South Asia. In Afghanistan, Bangladesh, India, and Nepal, a higher propensity to utilize modern contraceptives was noted among women with high empowerment levels compared to those with low empowerment levels.
Multilevel logistic regression results of the relationship between women’s empowerment and modern contraceptive use among women with no desire for additional children in South Asia.

Note. AOR: adjusted odds ratio; 95% CI: 95% confidence interval.
Model was adjusted for age, number of living children, ideal number of children, current working status, wealth index, place of residence, and individual country.
Models were adjusted for age, number of living children, ideal number of children, current working status, wealth index, place of residence.
Discussion
This study sought to better understand the relationship between women’s empowerment and the use of modern contraceptives among reproductive-aged women in South Asia who have no desire to have more children. The findings indicate that 45.8% of women in South Asia who expressed no desire for additional children utilized modern contraceptive methods. This figure aligns closely with the global average of 49% among women of reproductive age. 6 Our findings indicate that women who exhibit strong empowerment in their attitudes toward violence, social independence, and decision-making are more likely to utilize modern contraception. The results of this analysis were consistent with expectations, highlighting the importance of understanding the connection between women’s empowerment and the use of modern contraceptives for the advancement of family planning initiatives in South Asia.
This study indicates that while the prevalence of modern contraception usage in South Asia surpasses that observed among women in sub-Saharan Africa who have no desire to have children, 56 it remains significantly lower compared to that of women in Eastern and Southeastern Asia, Australia and New Zealand, Latin America and the Caribbean, as well as Europe and Northern America. 60 This finding suggests that the integration of modern contraceptives for fertility regulation continues to pose challenges for women in South Asia. The limited accessibility to family planning services, the lack of availability, and the costs associated with existing methods are reported to be the principal reasons for the underutilization of modern contraception in South Asian countries. 61 It is remarkable that Bangladesh’s adoption of modern contraceptive methods substantially surpasses that of its South Asian counterparts. Throughout the last three decades, Bangladesh’s family planning initiative has made remarkable progress, attributed to unwavering political commitment, creative program strategies, partnerships between governmental and non-governmental organizations (NGOs), a strong information, education, and communication campaign, a diverse methodological approach, and the dedication of personnel at the grassroots level. 62
The evidence we gathered substantiates the study’s hypothesis that a greater degree of women’s empowerment correlates with a heightened probability of utilizing modern contraception among reproductive-aged women in South Asia who have no desire to have more children. We found that exhibiting a high degree of empowerment in the domains of attitudes toward violence, social independence, and decision-making demonstrated a greater propensity to adopt modern contraceptive methods, thereby supporting earlier research.23–25,56 The findings underscored the essential role of women’s empowerment in shaping the use of modern contraceptives within South Asian contexts.
The concept of empowerment plays a vital role in fostering individual agency and manifests in diverse ways, such as motivation, negotiation, contemplation, and the ability to set and pursue personal goals and choices. 63 Empowering women has the potential to catalyze significant changes in gender dynamics and the societal norms governing women’s behavior both within the home and in the wider community. 64 These modifications necessitate parallel adjustments in male conduct toward females, encompassing choices related to reproduction and the use of contraceptives. In South Asian contexts, family dynamics and gender expectations often impose restrictions on women’s independence, their capacity to make decisions, and their freedom of movement in multiple domains. The enduring impact of male supremacy and control profoundly shapes gender dynamics, as husbands often assume the prerogative to dictate the timing and quantity of offspring their wives should have, while women tend to avoid conversations about fertility and reproductive regulations with their spouses, driven by a legitimate fear of potential violence.65,66 In these contexts, the findings of this study carry substantial implications for forthcoming reproductive trends, underscoring that the empowerment of women is an essential factor shaping their reproductive behavior.
The correlation between women’s empowerment and the use of modern contraception varies across countries. This study revealed that higher empowerment about attitudes toward violence was correlated with the utilization of modern contraception in Bangladesh and India, but not in the other three countries. The attitude of women toward violence is frequently influenced by entrenched gender norms and ideas inside patriarchal power systems that endorse male supremacy and facilitate the reduction of women’s rights. 67 Pakistan and Afghanistan are sometimes regarded as identical nations due to their profound historical connections, cultural similarities, analogous socioeconomic structures, and shared religious and ethnocultural identities. 68 The infringement of women’s rights has been a pervasive and enduring practice in both countries, entrenched in patriarchal norms as well as patriarchal interpretations and practices of Islam that subordinate women in socio-cultural interactions, resulting in an inequitable dynamic that diminishes women’s autonomy and authority over vital decisions regarding their health and lives. These may influence women’s reproductive decisions and the use of modern contraception. Nepal, a South Asian nation abundant in culture and natural beauty, is among the least developed countries globally. The predominantly Hindu culture has historically defined itself through a hierarchical caste structure, which frequently delineates women’s roles as homemakers and legitimizes violence against them. 69 In numerous Nepali households, women’s reproductive choices are constrained by patriarchal norms and diminished negotiating power, corroborating data from South Asia that male supremacy in fertility decisions obstructs the adoption of family planning.70,71 In Nepal, the phenomenon of spouses residing away from home has become prevalent due to extensive male migration. 72 The elevated prevalence of male migration may exacerbate the complexities surrounding modern contraceptive utilization, as women frequently postpone adoption until their husbands’ return, thus forgoing options for consistent protection. In addition, an examination of the Nepal DHS reveals that various ethnic groups encounter numerous obstacles in obtaining family planning services, primarily due to factors such as illiteracy, poverty, and reduced status in society.73,74
Higher empowerment concerning social independence was correlated with increased likelihood of utilizing modern contraception in Afghanistan, Bangladesh, India, and Pakistan. Given the parameters outlined for this domain, it is expected that women who are well-informed and have not interrupted their schooling or jobs owing to early life events such as marriage or childbirth are more inclined to use modern contraception. Nonetheless, we failed to observe a significant relationship in Nepal. A subsequent DHS study in Nepal revealed that education, a crucial factor in social independence, was not correlated with the utilization of modern contraception, with lower probabilities observed among more educated women. 72 In Nepalese society, a husband’s influence significantly impacts a woman’s decision to utilize contraceptives; even educated women who want to use contraceptive methods often refrain due to their husband’s opposition to family planning. 75 This finding may elucidate the absence of a correlation between high empowerment for social independence and the utilization of modern contraception among women with no desire for additional children.
Our data revealed that high levels of empowerment in decision-making among women correlated with the use of modern contraceptives across all South Asian nations studied with the exception of Pakistan. In conservative environments such as Pakistan, women are often not the only determinants of their reproductive choices. Significant emphasis is placed on the involvement of males, specifically spouses, in fertility decision-making. Nonetheless, other individuals, such as mothers-in-law, also influence these decisions. 76 Consequently, factors such as household composition and size, the joint family system, and the husband’s attributes may influence a woman’s contraceptive use and her ability to exercise reproductive rights. The insignificant results in Pakistan may stem from the predominance of joint decision-making led by the spouse. 77 In support of this, a study conducted in Pakistan by MacQuarrie and Aziz 29 indicated that the utilization of modern contraceptives is hindered when husbands are the principal decision-makers about contraceptive choices. The husband’s decision-making significantly restricts the utilization of injectables, IUDs, tablets, and other contemporary treatments. These procedures typically necessitate a consultation with a healthcare provider, highlighting the “gatekeeper” function that males may assume in accessing healthcare. 29 Furthermore, the gender disparity in Pakistan exceeds that of other South Asian nations. The “Global Gender Gap Report 2025” indicates that Pakistan ranks last among South Asian nations and globally, occupying the 148th position; however, Afghanistan was excluded from this report.
The variability in the relationship between various aspects of women’s empowerment and the utilization of modern contraception among women with no desire for children across different South Asian countries can also be elucidated by the positive correlation observed among the distinct dimensions of the SWPER index, whereby an enhancement in one aspect of empowerment corresponds with an elevation in the others. For example, women with higher levels of education were more inclined to engage in decision-making processes 78 and rejected the justification of domestic violence 79 compared to their less educated counterparts. Women engaged in household decision-making are also less inclined to justify wife beating under any circumstances. 80 Our analysis revealed that Bangladesh and India stand out as the two countries exhibiting a greater proportion of women experiencing high levels of empowerment across various domains, a phenomenon, that is, also linked to the higher utilization of modern contraception.
The differences in the relationship between women’s empowerment and the utilization of modern contraception among women in South Asian nations may also be elucidated through the lens of religious beliefs. South Asian conservatives advocate a stringent and fundamentalist interpretation of religion and culture that fosters male dominance, expecting women to confine themselves to domestic roles and refrain from participating in external economic activity. 81 Research indicates that regarding women’s roles in society, Islam exhibits a level of patriarchy comparable to that of other major world religions, particularly Hinduism and Christianity. 82 Although Hinduism and Islam are the largest religions in South Asia, both exhibit patriarchal structures; nevertheless, their perspectives on family planning differ significantly. Muslims contend that their laws prohibit family planning, while Hindus are typically more amenable to it. 83 The low levels of empowerment, coupled with a conservative Muslim societal framework, may contribute to a lower use of contraception in Afghanistan and Pakistan. Although the population of Bangladesh predominantly adheres to similar religious beliefs as those in Afghanistan and Pakistan, this similarity has little influence on the empowerment of women or the utilization of contraception. The differences may stem from Bangladesh’s historical context as a non-conservative Muslim society, 84 coupled with various governmental initiatives designed to promote women’s rights, such as free education for girls and efforts to mitigate gender inequalities in labor force participation, education, and earnings, along with productive collaborations with NGOs in targeted areas of women’s development. The populations of India and Nepal largely share a common religious framework, Hinduism, which allows for the use of all forms of contraception. 85 Consequently, in the patriarchal Hindu societies of India and Nepal, the adoption of modern contraception surpasses that observed in other orthodox Muslim countries within South Asia, such as Afghanistan and Pakistan. Nevertheless, due to the exclusion of religion from the DHS dataset (as seen with Pakistan), we were unable to incorporate religious factors into our analysis to examine their influence on the utilization of modern contraception in this study. Future research is recommended to evaluate how patriarchal norms and religious beliefs across various South Asian nations may differentially influence empowerment and contraceptive practices.
The study’s findings have profound implications for the fertility and health sectors, demonstrating that women’s empowerment acts as a catalyst for positive behaviors related to reproductive health and improves negotiation and communication regarding the use of modern contraception. It is imperative for governments to allocate additional resources to the public education system, thereby alleviating the financial strain on impoverished households and enhancing literacy and enrollment rates among women. Reducing the gender gap in education will lead to an increased participation of women in the non-agriculture sector, thereby enhancing household income. These initiatives will enhance women’s domestic agency and, hence, the utilization of modern contraception. Governments ought to emphasize the development of gender-sensitive curricula, fostering equality and combating conventional gender stereotypes. Policymakers must refine existing legal frameworks and ensure the effective implementation of legislation safeguarding women’s rights, particularly in areas such as gender-based violence, inheritance, and employment rights. Insufficient support for the advancement of women’s rights may stem from prevailing cultural values and varying interpretations of religious doctrines. Governments and civil society organizations ought to engage in dialogue with representatives of conservative groups to harmonize longstanding beliefs with contemporary notions of gender equality. Informing women and their partners about the significance of female empowerment and its lasting advantages for families can significantly enhance women’s healthcare, particularly regarding reproductive health initiatives. In this context, mass media can assume a crucial role. The authorities should leverage mass media as a conduit for disseminating precise information regarding family planning, thereby motivating couples to engage in such practices. Furthermore, family planning information is tailored to be age-appropriate, culturally sensitive, and readily accessible. In addition to traditional mass media, it is imperative that information regarding family planning be disseminated through the internet and various digital media platforms. A comprehensive strategy that involves women’s organizations, community leaders, and government agencies in a cooperative endeavor is crucial for improving awareness about women’s rights and their access to sexual and reproductive healthcare services.
Limitations
This study poses several strengths and limitations. This study examines five South Asian countries employing a standardized methodology and questionnaire, facilitating a thorough understanding of the issue through integrated findings and country-specific assessments. Moreover, utilizing a validated and standardized metric for women’s empowerment, the SWPER worldwide, 36 enabled a thorough evaluation across five countries. However, it is vital to point out several limitations. The data were obtained from a self-reported survey, making them susceptible to recall bias. The analysis conducted is observational and cross-sectional; thus, causality cannot be inferred from it. The relationship between empowerment and modern contraception use was evaluated among women who have no desire for additional children, which may limit the findings’ generalizability to all reproductive-aged women. An intrinsic limitation of the SWPER is that it is exclusively applicable to partnered or married women. The evaluation of women’s empowerment within health surveys is hindered by a restricted array of variables and omits several significant dimensions of empowerment as well as other important factors, including psychological factors, women’s ownership status, reproductive coercion, male attitudes, religious beliefs, geographic availability of services, and sexual and reproductive autonomy, among others. Additionally, the SWPER index presents a notable constraint in its scope, as it depends solely on data from the DHS and fails to consider women’s empowerment as a process.
Conclusion
This investigation contributes to the expanding corpus of research focused on elucidating the connection between the empowerment of women and the utilization of modern contraceptive methods. The results of this research suggest that the empowerment of women significantly influences the use of modern contraception. Women who hold more equitable views regarding violence against their gender, exhibit greater social independence, and actively participate in household decision-making are more inclined to utilize modern contraceptive methods compared to those who are less empowered. Promoting the utilization of modern contraception among South Asian women requires focusing on empowering individuals, cultivating equitable negotiation dynamics between partners, and facilitating regular discussions on fertility and its regulation.
Supplemental Material
sj-docx-1-whe-10.1177_17455057261432611 – Supplemental material for Empowering women can increase modern contraception use among women with no fertility intentions in South Asia
Supplemental material, sj-docx-1-whe-10.1177_17455057261432611 for Empowering women can increase modern contraception use among women with no fertility intentions in South Asia by Mahmudul Hasan Tonmoy, Raufun Hasan Arnob, Shamima Akter and Md. Mosfequr Rahman in Women's Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057261432611 – Supplemental material for Empowering women can increase modern contraception use among women with no fertility intentions in South Asia
Supplemental material, sj-docx-2-whe-10.1177_17455057261432611 for Empowering women can increase modern contraception use among women with no fertility intentions in South Asia by Mahmudul Hasan Tonmoy, Raufun Hasan Arnob, Shamima Akter and Md. Mosfequr Rahman in Women's Health
Footnotes
Acknowledgements
We express our gratitude to MEASURE DHS for granting us access to the data employed in this research. We wish to convey our sincere appreciation to all individuals and organizations from the countries encompassed in this study who contributed to the implementation of the DHS.
Ethical considerations
The surveys received approval from the ICF Institutional Review Board, and the survey protocols were reviewed and approved by the National Research Ethics Committee of the respective country; for instance, in Bangladesh, the Institutional Review Board of ICF International (reference number 2022-135) and the Bangladesh Medical Research Council (BMRC; reference number BMRC/NREC/2019-2022/156) provided approval. MEASURE DHS granted us formal authorization and raw survey data for utilization. Additional information concerning DHS data and ethical standards can be found online at ![]() .
.
Consent to participate
All participants gave verbal informed consent before taking part in the study; however, married girls ages 15–17, considered emancipated minors, also gave verbal consent. This study, being a secondary analysis of anonymized data and lacking direct interaction with participants, did not necessitate further consent from the participants.
Consent for publication
This study, being a secondary analysis of anonymized data and lacking direct interaction with participants, did not necessitate further consent from the participants.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.