
Abstract
Background:
Emergency contraception (EC) can prevent up to 95% of unplanned pregnancies if used correctly. Despite efforts to enhance its accessibility, cost and cultural stigmas persist as formidable barriers.
Objective:
This study assessed the knowledge and practices of EC use and determined the associated factors among the female undergraduate students of Northern Uganda.
Design:
This was a descriptive, institutional-based cross-sectional study conducted among the female undergraduate students of Lira University in Northern Uganda.
Methods:
Data were collected from 328 female undergraduates who were surveyed using self-administered questionnaires after obtaining informed consent from them. Data were analyzed using Statistical Package for Social Sciences (SPSS) and presented as frequencies and percentages, and binary and multiple logistic regressions were used to determine the association between the outcome variable and the independent variables. Results were presented as odds ratios with 95% confidence intervals, and associations were considered statistically significant at p ⩽ 0.05.
Results:
The response proportion was 328/334 (98%). Majority of the participants were 18–23 years old (233/328; 71.0%), had a consistent sexual partner (221/328; 67.4%), and unmarried (206/328; 62.8%). Almost all the participants (315/328; 96%) had heard about EC, where 150/328 (45.7%) learned about EC from health professionals and 135/328 (41.2%) learned about EC from family members and friends. The most well-known brand of EC was Postinor-2 (Levonorgestrel), as reported by 130/328(39.6%) participants. Of the study participants, 200/328 (61.0%) were knowledgeable about the correct timing of EC. Regarding practices of EC use, 214/328 (65.2%) used EC, of whom 122/214 (57.0%) acquired EC from the pharmacy, and most of the participants who had used EC used Postinor-2 (92/214; 43.0%). Of those who used EC, 175/214 (81.8%) used it to prevent unplanned pregnancy, and 182/214 (85.0%) participants used it with the correct timing. The factors that were associated with EC use were being a student who was studying at the Faculty of Health Sciences (adjusted odds ratio (AOR): 4.27, CI: 1.61, 10.09, p ⩽ 0.003) and the absence of a consistent current sexual partner (AOR: 8.63, CI: 4.49, 16.59, p ⩽ 0.00).
Conclusion:
Participants showed good EC knowledge and usage, but gaps persist. Factors like being a student who was studying at the Faculty of Health Sciences, and lack of a consistent current sexual partner correlated with EC use. Consistent education efforts are needed to address knowledge gaps, focusing on diverse EC forms, reliable information, and affordability.
Registration:
Not applicable.
Plain language summary
Keywords
Introduction
Emergency contraception (EC) refers to methods of contraception that can be used to prevent pregnancy after sexual intercourse. 1 EC can prevent over 95% of pregnancies when taken within the recommended time interval after sexual intercourse depending on the type of EC used and can be effective in the prevention of unplanned pregnancies.1,2 Over 100 million acts of sexual intercourse take place in the world each day resulting in around 3 million conceptions of which 50% are unplanned and 25% of those are unwanted. 3 An unplanned pregnancy refers to a pregnancy that occurs when conception happens despite not being actively desired or intended at the time of conception. 4 Unplanned pregnancies may not have been part of immediate life plans but they may not necessarily be unwanted since some unplanned pregnancies can be welcomed and accepted once they occur. 5 On the other hand, unwanted pregnancy refers to a situation where the person who becomes pregnant did not desire or intend to become pregnant at all and these pregnancies typically involve feelings of; distress, reluctance, or a clear decision to not proceed with the pregnancy leading to considerations of options like; abortion, adoption, or carrying to term with subsequent plans for adoption. 5
A study published in 2022 found that the prevalence of unplanned pregnancy in sub-Saharan Africa was 33.9%, with 11.2% being unwanted and 22.1% being unplanned. 6 In Uganda, the prevalence of unplanned pregnancy is even higher at 46% as was found in the 2021 Performance Monitoring for Action-PMA Uganda project, a Phase 2 cross-sectional survey from Makerere University School of Public Health. 7
According to the World Health Organization (WHO), EC can be used in the following situations: unprotected intercourse, possible contraceptive failure, incorrect use of contraceptives, and sexual assault for victims without contraception coverage.1,4 EC methods include copper-bearing intrauterine devices (IUDs), LNG (levonorgestrel) IUDs, and emergency contraceptive pills (ECPs).1,8 A copper-bearing IUD is the most effective form of EC available. 9 The ECP regimens recommended by the WHO are ulipristal acetate, levonorgestrel, or combined oral contraceptives (COCs) consisting ethinyl oestradiol plus levonorgestrel. 8 According to the WHO, EC can be used by all women of reproductive age, and this can be beneficial in preventing unplanned pregnancies and their associated complications.1,4
Previous studies have found that unplanned pregnancies pose a great challenge to the reproductive health of young adults in developing countries like Uganda where some young women with unplanned pregnancies may choose to abort.5,10 Because of the strict abortion laws in Uganda that do not legalize abortion for everyone but only in exceptional cases, 11 many young women perform unsafe abortion, which poses a great risk of morbidity and mortality.10,12 The Ministry of Health of Uganda and development partners introduced EC in Uganda and made it available through government and private health facilities, as well as through pharmacies and drug shops.13,14 This means EC in Uganda can be bought without a prescription and without an age limit. Despite the efforts to make EC accessible, this commodity is very expensive when acquired from private pharmacies and drug shops such that many Ugandans cannot afford to buy it; meanwhile, in public health facilities where EC is free, many who go to access EC report face stigmatization from health workers and a vast array of questions which tend to make them shy away from accessing EC from these health facilities; the stigmatization also occur in private health facilities. 15 As anecdotally evidenced in Uganda, many women have resorted to the use of Aspirin as EC because it is cheaper and are thereby impeded from the remedial benefits of using EC. 16
Several studies have explored awareness and perceptions of EC in various regions. Most participants were familiar with EC in a study conducted in Nigeria, another study conducted in Ghana, and another study conducted in Democratic Republic of Congo.17 –19 However, among university students in Nigeria, only 37.9% reported awareness of EC, and among adolescent girls, 52.8% had heard of it.20,21 Perceptions of EC’s purpose also varied across contexts. While a study in India found a significant proportion of the participants believed EC was used wrongly with the intention of causing abortion, only 4.6% of the college students in the same setting held the same view.22,23 Sources of information about EC also differed with family and friends being the most common sources in Ghana, whereas the internet was the leading source in India.22,24
Regarding access and use, a study in Bangladesh and another study in India reported that over half of participants believed EC should be prescription based.22,25 On the other hand, a study in Ethiopia and another study in Nigeria showed varying levels of EC use, ranging from one-quarter to two-thirds of participants. The morning-after pill was the most commonly used method in most studies although a few participants in different settings used COCs, progestin-only pills or progestogen-only pills (POPs), or IUDs.17,26 Furthermore, knowledge about EC was found to be a strong predictor of its use. 26
While global studies provide insight into EC awareness and usage, Uganda has higher rates of unwanted pregnancies than other sub-Saharan African (SSA) countries. 7 In addition, there exists differences in how EC is accessed in Uganda and in other SSA countries, and the cost one need to meet to acquire and use them also varies. 27 Due to the limited research focused on EC use among the female undergraduates in Uganda, it was imperative to understand their knowledge and perceptions since this can be used in developing targeted interventions to reduce unplanned pregnancies and prevent associated risk of school dropout or unsafe abortion. 12 This study assessed the knowledge and practices of EC use and associated factors among female undergraduate students at Lira University.
Methods
Study design
This was a descriptive cross-sectional survey study conducted among the female undergraduates aged 18–49 attending Lira University during the 2022–2023 academic year. Despite the fact that the benefits of EC are more relevant for younger individuals, including women up to 49 years old allowed us to understand the broader implications of EC use across different age groups. When preparing this manuscript, Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) study guidelines for reporting observational studies was used as a guide. 28
Setting
This study was conducted at Lira University located in Northern Uganda during the 2022–2023 academic year, and data were collected from January 10 to 17, 2023. Uganda had a total of 21 chartered universities as of 2023, 10 of which were private and 11 public. 29 All public universities in Uganda have a similar administrative structure and admit students from all parts of Uganda; thus, the student populations can be comparable. Lira University is one of the 11 public universities in Uganda 30 ; it is located in Ayere Cell, Barapwo Ward, Lira City West, Lira City, Northern Uganda, and covers a total land area of 621 acres (251.3 hectares). The university had an average of 1500 undergraduate students as of the academic year 2022–2023, out of which 600 students were female and 900 were male. The students of Lira University, just as the other 10 public universities in Uganda, come from different parts of the country and are highly representative of a typical university population in Uganda, despite the fact that some universities have higher enrollments than others depending on their years of existence. Though Lira University has not been in existence for long, it is already fully established just like other public universities in Uganda.
Participants
Target population
Undergraduate female students at Lira University were recruited to take part in this study. The researchers have chosen undergraduate students because the majority of students at Lira University are undergraduates, which is more representative of the university population; besides, the majority of younger population who may most benefit from emergency contraceptives are undergraduate students. Additionally, the few cases of unintended pregnancies anecdotally identified within Lira University setting were among the undergraduate students. Lira University is one of the 11 public universities in Uganda, and at the time this study was conducted, Lira University had 4 academic faculties with a total undergraduate population of 1500. The faculties were medicine, health sciences, management sciences, and education. The Faculty of Health Sciences had the greatest number of students, followed by the Faculty of Medicine. The Faculty of Management Sciences and the Faculty of Education had the least enrollment at the time of the study. An additional 170 students were enrolled in graduate programs at the time of the study, but these students were not included in the study.
Inclusion and exclusion criteria
Inclusion criteria
Female undergraduate students at Lira University aged 18–49.
Exclusion criteria
Females with fertility issues, those who reached menopause, and those who had never had sexual intercourse were excluded from this study to minimize bias. This is because these category of people do not need to prevent pregnancy, and so they do not need to use modern contraceptive methods such as EC. Therefore, they were not considered suitable participants for this study.
Study recruitment
Data were collected by five researchers who were all team members of this study and had received training on both ethical issues in research and the data collection tool. The data were collected for 7 days consecutively from January 10 to 17, 2023. Data were collected from each faculty at a time, and the recruitment of participants from one faculty was completed before the team began collecting data from another faculty. Data were collected during school hours when the students were on campus whereby each of the researchers approached a potential participant on a one-on-one basis, introduced him or herself and explained the purpose, benefits, and eligibility for participating in the study while also answering any questions. If found to be eligible, the students were invited to participate in the study, after which signed informed consent was obtained from those who accepted.
Data collection procedure
Permission to collect data was obtained from the dean of students of Lira University. After the recruitment of the participants into the study, they were then given a paper-based self-administered questionnaire with 30 min to complete, which was then collected immediately by the researcher. All students who consented to participate in the study took no more than 10 min filling out the questionnaires. Those who declined to participate in the study and those who were not eligible to participate were not recruited, and those who declined to participate were recorded as nonresponse. Each of the participants was given an incentive of 5000 Ugandan shillings to compensate for the time spent filling out the questionnaire, this amount of money is small (about 1.32 US dollars) and therefore not persuasive. The researchers approached a total of 336 participants, only 4 of whom were not eligible for inclusion into the study, 4 of them declined to participate in the study since they said they did not have time at that moment, then 328 of them were enrolled into the study with no dropout; hence, the final sample size was 328 participants.
Variables
Independent variables
The independent variables in this study were sociodemographic factors such as age, area of study, year of study, religion, marital status, place of residence, and minimum upkeep pocket money at any particular time. This is because we suspected that these factors may affect the ability of an individual to access or use EC; this has been demonstrated in other studies.26,31 Knowledge of EC use was also one of the independent variables, and it included aspects such as hearing about EC, source of information about EC, types of drugs or commodities used as EC, knowledge about when to use EC, and the time interval to use EC after having unprotected sexual intercourse. Another component of the independent variables was practices of EC use such as where the person acquired EC from, the types of drugs or commodities used as EC, the circumstance under which the person used EC, and the timing of use of the EC with respect to when the person had unprotected sexual intercourse. Factors associated with EC use were also independent variables.
Dependent variable/outcome variable
The dependent variable in this study was EC use, which we suspected as being associated with a variety of factors that were determined following data analysis.
Data sources
The data were collected using a data collection tool, which was developed following the review of previous literature on EC.18 –20 The data collection tool had three sections of sociodemographic information, knowledge on EC use, and practices of EC use. A self-administered, paper-based data collection tool was used. Under the knowledge on EC use, there were several key questions with options for the participants to choose from, and some of the options were incorrect to test whether the study participants were knowledgeable about EC. For instance, the question was asked about the knowledge on the types of EC: Aspirin tablet was included among the options to check whether the participants actually knew aspirin is not a method of EC, but the rest of the options were correct methods of EC. Regarding the correct timing of the use of EC, there was only one correct option, that is, before the end of 72 h following unprotected sexual intercourse. Many options were given to test whether the participant actually knew the correct timing of use of EC. Regarding knowledge on the indication for the use of EC, many options were provided, of which the incorrect options were as follows: after conception of unplanned pregnancy, to terminate a pregnancy/for abortion, to prevent STI/STDs, used as a routine birth control method. That meant a participant who choose the wrong methods did not know when to use EC. For the access of EC in Uganda, they could be accessed either through prescription or over the counter; so, the researchers wanted to know whether the study participants were aware of those facts.
Bias
To ensure reliability of this study, the data collection tool was pretested using 10% of the sample size (34 participants) from Lira University, who were not included in the sample. The participants who were chosen in the pretest met the inclusion criteria for participation in the study. The questionnaire was then modified based on the pretest results.
During data collection, females with fertility issues, menopause, and never had sexual intercourse were excluded from this study to minimize bias. This is because these category of people do not need to prevent pregnancy, and so they do not need to use modern contraceptive methods such as EC; therefore, they were not considered suitable participants for this study.
In this study, we accounted for potential nonresponse bias during the sample size calculation, where we adjusted our sample size to 334 participants based on an anticipated nonresponse rate of 10%. We then achieved a high response rate of 98%, which suggests that our sample is likely representative of the target population. This high level of participation helped mitigate concerns regarding nonresponse bias, so our results are most likely representative of the study population.
Study size
The desired sample size was 334, which was determined using the Leslie Kish formula of sample size calculation (1965), with a 95% confidence interval (CI). The Z value was 0.5 and Z 2 (1−α) = 1.96.
Formula:

where n was the sample size, α was the level of significance, Z 2 (1 − α) = 1.96 was the Z-score corresponding to the degree of confidence, P = 27.1% was the estimated prevalence of EC use among the undergraduate students, D was the margin of error or the desired precision, and P (1 − P) was the variance (PQ).
Sampling approach
Proportionate sampling was used in this study, 32 where equal proportions of participants were chosen at random from each of the four academic faculties.
Quantitative variables
The study collected various quantitative measurements related to ECEC use, including demographic characteristics, knowledge of EC, and reported practices. Frequencies and percentages were calculated for these measurements to provide a comprehensive overview of the study participants. Statistical Package for Social Sciences (SPSS) version 23.0 was used to aid data analysis.
Statistical analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 23.0. At the univariate level, descriptive statistics, such as frequencies and percentages were employed to summarize the data. Binary logistic regression was conducted to determine significant factors at the bivariate level. For the multivariate analysis, multiple logistic regression was utilized to identify factors independently associated with EC use among the study participants, employing a 95% confidence interval (CI) and a significance level of p ⩽ 0.05.
In this study, factors significant at the bivariate level were treated as covariates. Additionally, missing data were minimal and reported as such, as they were not expected to significantly impact the overall findings.
Results
Descriptive data
Sociodemographic characteristics of the study participants
The study team recruited 328 participants who were all undergraduate female students of Lira University, and the response proportion was 328/334 (98%). A majority of the study participant were in the age bracket of 18–23 years old (233/328; 71.0%), unmarried (206/328; 62.8%), had a consistent current sexual partner (221/328; 67.4%), and reported typically having at least 25,000 Ugandan shillings of pocket money at any particular time (270/328; 82.3%). This amount is equivalent to about 6.55 U.S. dollars, 27 which although it is a small amount of money is just enough for one to purchase EC if the need arises. This means that to some extent a majority of the study participants could afford to buy EC if needed, since the average cost of EC in Uganda at the time of the study was 3.3 U.S. dollars. However, this point does not put into consideration the participants’ other basic needs, which could prevent them from using the pocket money to purchase EC. Half of the study participants were students who study at the Faculty of Health Sciences of Lira University (166/328; 50.6%), a third of the participants were in their second year of study at Lira University (125/328; 38.1%), and 133/328 (40.5%) of the participants were Anglican by religion. When asked about their residence, it was found that more than half, 185/328 (56.6%), of the participants resided in hostels with friends around Lira University (Table 1).
Sociodemographic characteristics of the study participants (n = 328).

The term sexual partner used in this study refers to opposite sex partner not the same-sex partner as EC will have no benefit to same-sex partners. Faculty of Health Sciences used in this study included the department Nursing and Midwifery, and the Department of Public Health. EC: emergency contraception.
Outcome data and main results
EC use and knowledge among the study participants
More than half (214/328; 65.2%) of the study participants reported they had used EC (Table 2). Almost all the study participants reported they had heard of EC (315/328; 96%), and a majority of them reported they had learned about EC from health professionals (150/328; 45.7%), and family members and friends (135/328; 41.2%). The most well-known type/brand of EC among the female undergraduate students of Lira University was Postinor-2 or morning-after pills (130/328; 39.6%). Meanwhile, 101/328 (30.8%) of the study participants knew of progestogen-only pills (POP), 104/328 (31.7%) of the participants knew of COCs, and only 38/328 (11.6%) of the participants knew of IUDs as a method of EC. More than half of the study participants (200/328; 61.0%) were knowledgeable about the correct timing of EC use. When the participants were asked about when EC can be used, they responded as follows: More than half said EC is used after rape or forced sex (180/328; 54.9%), almost two-thirds said EC is used when a condom breaks during sex (197/328; 60.1%), less than one-third said EC is used after missing a daily birth control pill (72/328; 22.0%), and 56/328 participants (17.1%) said EC is used for abortion. Only 124/328 participants (37.8%) said that EC should be accessed via prescription only. Six participants did not answer the question on EC use, but these missing data were small and negligible since it may not affect the overall outcome of the result, so it was reported as missing (Table 2).
Prevalence and knowledge on EC use among the study participants (n = 328).
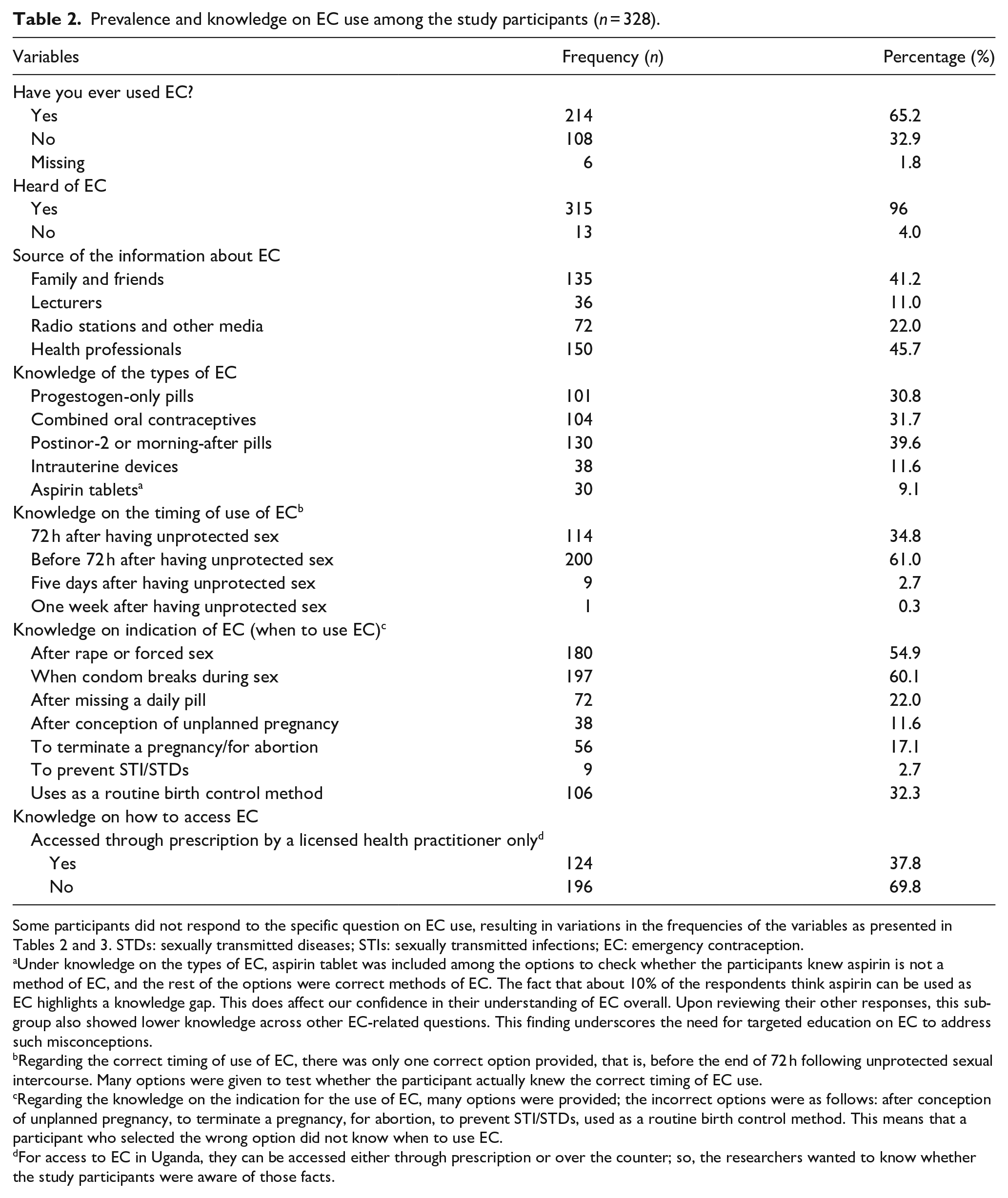
Some participants did not respond to the specific question on EC use, resulting in variations in the frequencies of the variables as presented in Tables 2 and 3. STDs: sexually transmitted diseases; STIs: sexually transmitted infections; EC: emergency contraception.
Under knowledge on the types of EC, aspirin tablet was included among the options to check whether the participants knew aspirin is not a method of EC, and the rest of the options were correct methods of EC. The fact that about 10% of the respondents think aspirin can be used as EC highlights a knowledge gap. This does affect our confidence in their understanding of EC overall. Upon reviewing their other responses, this subgroup also showed lower knowledge across other EC-related questions. This finding underscores the need for targeted education on EC to address such misconceptions.
Regarding the correct timing of use of EC, there was only one correct option provided, that is, before the end of 72 h following unprotected sexual intercourse. Many options were given to test whether the participant actually knew the correct timing of EC use.
Regarding the knowledge on the indication for the use of EC, many options were provided; the incorrect options were as follows: after conception of unplanned pregnancy, to terminate a pregnancy, for abortion, to prevent STI/STDs, used as a routine birth control method. This means that a participant who selected the wrong option did not know when to use EC.
For access to EC in Uganda, they can be accessed either through prescription or over the counter; so, the researchers wanted to know whether the study participants were aware of those facts.
Practices of EC use among the study participants
About two-thirds of the study participants reported they had used EC (214/328; 65.2%). More than half of those who had used EC purchased from the pharmacy (122/214; 57.0%). Meanwhile, 11/214 participants (5.1%) acquired EC from the university hospital for free, 82/214 participants (38.3%) purchased it from a local drug shop, and 20/214 participants (9.3%) acquired it from a government health facility for free. When asked about the type of EC they used, more than two-fifths of the participants reported using Postinor-2 or morning-after pills (92/214; 43.0%). Meanwhile, 53/214 participants (24.8%) used COCs, 54/214 participants (25.2%) used POP, and only 12/214 participants (5.6%) used IUDs. The majority of the study participants used EC to prevent unplanned pregnancy (175/214; 81.8%). Furthermore, some participants used EC after forced sex (18/214; 8.9%) or when a condom broke during sex (31/214; 14.5%). More than three-quarters of those who used EC used it with the correct timing (182/214; 85.0%) (Table 3).
Practices of EC use among the study participants (n = 328).

Some participants did not respond to specific questions on EC use, resulting in variations in the frequencies of the variables as shown in Tables 2 and 3. COC: combined oral contraceptives; POP: progestogen-only pill; IUD: intrauterine device.
The correct timing for using EC is within/before 72 h following unprotected sexual intercourse.
Factors associated with EC use among the study participants
Statistical analysis at bivariate level showed that eight factors were associated with EC use and that only two factors were associated with EC use at the multivariate level of analysis. At binary logistic regression, the factors that were statistically significant at p ⩽ 0.05 were the following: age of the participants (p ⩽ 0.038), area of study (p ⩽ 0.05), absence of a consistent current sexual partner (p ⩽ 0.00), marital status (p ⩽ 0.000), use of EC due to forced sex or rape (p ⩽ 0.00), use of EC when a condom broke during sexual intercourse (p ⩽ 0.00), and use of EC for the prevention of unplanned pregnancy (p ⩽ 0.00). At multivariate logistic regression, only two factors were found to be independently statistically significant at p ⩽ 0.05. These factors were as follows: area of study (i.e., students who study at the Faculty of Health Sciences; adjusted odds ratio (AOR): 4.27, CI: 1.61, 10.09, p ⩽ 0.003), and the absence of a consistent current sexual partner (AOR: 8.63, CI: 4.49, 16.59, p ⩽ 0.00). These factors are further discussed in the Results section (Table 4).
Bivariate and multivariate analyses of factors associated with EC use among the study participants (n = 328).

p-Values have been included for both bivariate analysis (first p-value at binary logistic regression) and multiple logistic regression (second p-value with the AOR). The term sexual partner used in this study means opposite sex partner since EC has no benefit for same-sax partners. CI: confidence interval; COR: crude odds ratio; AOR: adjusted odds ratio; p-value: level of significance.
The thinking behind the term absence of a consistent current sexual partners is that one may not be sure whether she will have sex with anyone, so she may not want to use the routine short-term (3 months) or long term (3–10 years) modern contraceptive methods. But in case she has chances to get a sexual partner at random and has unprotected sexual intercourse, then she will have to take EC to prevent her from getting pregnant. All the factors included in the above Table 4 are significant at bivariate level of analysis.
p ⩽ 0.05.
Discussion
This study aimed to assess the knowledge and practices of EC among female undergraduate students in Northern Uganda and identify the factors associated with its use. EC can prevent up to 95% of unplanned pregnancies when used correctly but remains underutilized due to barriers such as cost, accessibility, and cultural stigma.1,2 By exploring the awareness and use of EC, as well as the factors influencing these behaviors, this study offers valuable insights into the reproductive health practices of university students. The findings can inform the development of more effective educational interventions, promote EC access, and empower students to make informed reproductive health decisions.
Nearly all participants in this study reported having heard of EC, suggesting widespread awareness among female undergraduate students at Lira University. This finding aligns with studies in Nigeria, Ghana, and the Democratic Republic of Congo, where most participants were aware of EC.17 –19 However, the result contrasts with studies in Nigeria, which found that only 37.9% of university students were aware of EC, 20 and among adolescent girls in Nigeria, where 52.8% were aware. 21 Discrepancies in these findings could be attributed to varying cultural norms. Some societies, particularly those with taboo views on sexuality, may be less open to discussing or acknowledging modern contraceptives, depriving their populations of knowledge about EC. 33 Furthermore, public health education efforts vary by context, with some countries focusing resources on interventions with immediate, measurable impacts, potentially leaving gaps in EC awareness. 34 Additionally, religious beliefs, such as those in Catholic-majority regions, may influence the acceptance of modern contraceptives, including EC. 35 These differences highlight the need for context-specific studies to inform interventions aimed at improving knowledge and usage of EC.
Most participants reported having at least 25,000 Ugandan shillings (approximately 6.55 US dollars) as pocket money, which is sufficient to purchase EC, as the average cost in Uganda during the study period was around 3.3 US dollars. 36 However, this amount might not account for other essential needs, which could prevent students from spending their pocket money on EC. While this study did not focus extensively on cost as a barrier to access, recent studies on EC often overlook cost-related accessibility issues.12,37,38 To increase EC usage among university students, EC should be made available at no or reduced cost.
In this study, about one of the six participants had the misconception that EC can be used for abortion. The word abortion has been conceptualized in this study as termination of pregnancy before viability but after 72 h following unprotected sexual intercourse when pregnancy has been diagnostically confirmed. 39 The result of this study is consistent with those of other studies, which showed misconceptions about EC as used for abortion in different settings like India.22,23,40 The misconception could have stemmed from the possible misinformation that women of reproductive age receive from family members and friends who they consult regarding the use of EC. 41 Information about EC that circulates within the community is highly influenced by beliefs and cultural factors, which are not always supported by scientific evidence. 42 Continuous efforts should be made to educate the public about the reliable sources of information about modern contraceptives.
When asked for the source of their knowledge about EC, most of the participants reported that they learned about modern contraceptives from healthcare professionals. The result of this study is not consistent with that of a study conducted in Ghana, which found that the primary source of information among the study participants was family members and friends. 24 Similarly, a study in India (Davis et al., 22 ) and a study in Syria ( 43 ) found that the primary source of information about EC utilized by the study participants was the internet and social media. The difference in the result of these study could be due to the fact that majority of our study participants were students from the Faculty of Health Sciences who may be more knowledgeable about the best source of information about EC compared with the general population. On the other hand, the findings in India and Syria may be due to the differing ability of the study participants in these distinct contexts to possess a smartphone and access the internet, and participants in India and Syria may have had a better access to the internet than the participants from Uganda and Ghana. 44
When asked about the EC they knew, most of the participants in this study reported that they were aware of Postinor-2, while about 3 in 10 reported that they were aware of POP and COCs. Although IUD is the most effective form of EC, 22 our study found that very few participants (11.6%) knew about it in this context. The result of this study is consistent with that of another study conducted in South Asia, which also found that very few study participants (6.3%) were aware of the IUD as an EC, 38 and another study conducted in Uganda found that IUD was not well known as an EC method. 45 This may be due to a lack of public education and healthcare focus on IUD compared with the more commonly discussed EC methods in both settings.46,47 On the other hand, IUD is not approved by FDA (Food and Drug Authority) to be used as an EC though the WHO recognizes and recommends it as the most effective modern contraceptive method that can be used as an EC; this could also be one of the reasons why countries are reluctant and educating the public on the use of IUD as an EC.48,57 Addressing this gap through country-specific targeted public health campaigns and training of healthcare providers to promote IUD as an EC option could significantly improve awareness and uptake.
Furthermore, more than half of the study participants were knowledgeable about the correct timing of EC. This implies that more than half of the study participants know how to use EC, and this would be very instrumental in preventing unplanned pregnancies among them. The result of this study is similar to that of a study conducted among the college students in India, which also found that majority of the study participants were knowledgeable about the correct timing of EC. 22 The result of this study is inconsistent with that of a study in Bangladesh, which found that more than half of the study participants did not know the correct timing of EC, 25 and that of a study in Ethiopia, which also found that few of the participants were aware of the correct timing of EC. 49 The difference in the results of these studies could be due to the possible variations in study population category, and the level and quality of public education interventions in the different settings. Despite the fact that more than half of the participants in this study were aware of the correct timing of EC, this result still shows that there is a significant knowledge gap about the use of EC among the female university students.
A few participants believed that EC should be accessed only through prescription, consistent with another study. 50 Limiting access to EC via prescription could restrict availability for those in need. However, studies in Bangladesh and India found that many participants preferred prescription-based access.22,25 The differences may be due to variations in community engagement strategies and the sources of EC-related information. A community-centered approach could better inform the public about how to access EC.
When asked about the use of EC, about two-thirds of the study participants reported they had used EC. The result of this study is consistent with that of another study among college students in Dire Dawa City in Eastern Ethiopia, which found that about two-thirds of the participants had used EC. 26 However, the result of this study is not consistent with that of a study among university students in Santa Maria, Brazil in South America, and a study in Ethiopia, both of which found that about half of the study participants had used EC.31,51 The result of this study is not consistent with that of a study in Nigeria, a study in Ethiopia, and other studies in other African contexts, which all showed different results where they found that a quarter of the study participants had used EC.21,49,50,52 Furthermore, the level of EC use varied across different contexts as evidenced by various studies.2,12,37,53,54 The differences in the level of EC use could be due to differences in the level of knowledge about EC, 26 varying levels of acceptance and access issues, and different attitudes toward EC, which are often shaped by cultural factors and beliefs. Innovative, context-specific strategies should be designed to address the barriers to EC use among the women of reproductive age in the different contexts.
Regarding the type of EC used, most participants reported using Postinor-2 or morning-after pills. This finding aligns with a study in Nigeria, which also identified morning-after pills as the most commonly used EC, 17 and a similar study in Ethiopia. 49 This suggests that participants are more familiar with levonorgestrel-based EC. While Postinor-2 is less expensive, its cost-effectiveness can vary depending on the socioeconomic status of those accessing it. The widespread use of Postinor-2 is likely due to its easy accessibility and availability, making it a preferred option over other EC methods.
More than three-quarters of those who used EC used it with the correct timing, that is to say, within the first 72 h following unprotected sexual intercourse. The result of this study is consistent with that of another study in Ethiopia, which also found that most of the study participants used EC with the correct timing. 55 This implies that most of the university students are maximizing the potential of EC in such contexts. However, in cases where IUD is used as an emergency contraceptive, its effectiveness is guaranteed even up to 5 days following an unprotected sexual intercourse. 8 In our study, IUD was not commonly known as an EC or used by the participants; thus, the time reference used was perfectly fitting this study but may not fully apply to all the methods of EC used in other settings.
When asked about the reason for using EC, half of the participants reported that they used EC to prevent unplanned pregnancy, a few reported having used EC because a condom broke during sexual intercourse, very few reported having used EC after forced sex and also very few reported they used EC with the intention of terminating pregnancy. In this study, the statement of using EC to prevent unplanned pregnancy means that the participant had unprotected sexual intercourse intentionally knowing she would take EC, but when the condom broke or after forced sex, it was not in her plan to take EC but since she did not want to get pregnant, she had to conditionally take it. Then for those who used EC with the intention of terminating unplanned pregnancy, this was not a correct use of EC since EC does not terminate pregnancy. 19 EC, particularly levonorgestrel (LNG), primarily functions by delaying ovulation, thus preventing pregnancy. 8 It is important to note that LNG does not terminate an established pregnancy and is ineffective once medical definitions of pregnancy have commenced, particularly after fertilization.8,56 We suggest that some participants may have an unmet contraceptive need where, in this context, they do not expect a pregnancy and do not want to use any contraception at all, so if they have a pregnancy, they may want to terminate the pregnancy, for example, with EC as supported by this study. The result of our study was similar to that of a study conducted in Ghana 54 and other studies conducted in other contexts like Nigeria 57 and Ethiopia. 58 Context-specific studies should be conducted to determine the unmet need for family planning and the essence of the unmet need so as to guide targeted intervention to meet the unmet need.
This study found that participants who were students and who study at the Faculty of Health Sciences were 4.27 times more likely to use EC than their counterparts while participants who did not have a consistent current sexual partner were 8.63 times more likely to use EC than those who had consistent current sexual partners. This implies that health science students are more knowledgeable about EC than their counterparts and those who do not have a consistent current sexual partner may prefer to use EC because they may not want to become pregnant after having sex with any random sexual partner whom they may not know very well. This implies that EC should be made easily accessible in a setting with high numbers of women of reproductive age without a consistent current sexual partner to prevent unwanted pregnancies among them. The result of this study is similar to those of some studies in Ethiopia, which also found that women who were unmarried, single, or without a consistent current sexual partner were more likely to use EC.26,31 The result of this study is not consistent with that of another study conducted in Ethiopia, which found that participants aged 20–24 were 2.02 times more likely to use EC than their counterparts, and other factors associated with EC use included urban residence, being knowledgeable on EC, and having a favorable attitude toward EC. 31 Similarly, some other studies in Ethiopia also found varying results where they found that having knowledge about EC, forced sex, unprotected sex, and fear of discontinuing school were associated with EC use.12,26 The differences in the results of these studies could be due to the differences in the key characteristics of study population like the age groups, student status and level, economic activity and class, and the differences in the nature of the variables measured by the data collection tools and how they were structured. While the majority of respondents viewed EC as an emergency option, there appears to be a subset who may use EC in different contexts, specifically individuals with inconsistent current sexual partners. They may rely on EC as a rarely used but planned option due to the sporadic nature of their sexual activity. This suggests that for some, EC functions as a supplementary contraceptive measure rather than strictly as an emergency response. This finding needs further exploration into how sexual activity patterns shape contraceptive choices. The factors associated with EC use should be contextually explored, and barriers should be subsequently addressed in order to realize maximum utilization of modern contraceptives and reduce the proportion of unplanned pregnancies and the associated consequences like unsafe abortion.
Limitations
The limitation of this study was that it was conducted among university students, so the results may not be generalizable to the entire population of women of reproductive age with dissimilar characteristics; however, the results of this study can be generalizable to the women of reproductive age with similar characteristics. Furthermore, the sample consists solely of female students, which may limit the ability to generalize the results to the entire university population; hence, the study is only generalizable to the female university students and women of reproductive age with similar characteristics and context as our study participants.
Additional predictive factors that may play a role in the use of EC that have not been explored in this study include cultural beliefs, norms and values, the complexity of the protocol to be followed to access EC from the public health facilities, and the judgmental nature of EC providers in public and private health facilities. Most African cultures consider sex to be a taboo for those not officially married, the expectation is that anyone who is not married should not have sex and that anyone who is married should give birth to many children, hence there is no need for EC. 33 This can hinder access to EC for those who may need it as one may prefer to use EC without the knowledge of others. In the Ugandan setting, young people who have gone to public health facilities and even some private health facilities and drug shops to access EC often complain of how they are welcomed with judgmental and stigmatizing attitude, perceived as criminals for using ECs that discourages them from going back to the health facilities to access ECs. 15 These judgmental and stigmatizing attitudes exhibited by health workers, which stem from their personal values and beliefs, prevent potential EC users from accessing EC. 24 The judgmental and stigmatizing attitudes of the health workers negatively affect the accessibility of EC from these facilities because most potential EC users are discouraged. 15 Finally, the data collection tool used did not provide a time frame reference for the practices of EC use, so some participants who might have used EC long time ago might have not remembered every information around their use of EC.
Conclusion
Most study participants were aware of EC, with healthcare professionals being the most important primary source of information, while family members and friends being the second most preferred source of information by the participants. Postinor-2 was the most commonly used EC method by the study participants. More than half of the participants demonstrated knowledge about the correct timing for EC, and two-thirds reported using EC, primarily Postinor-2, with a majority using it appropriately.
Participants utilized EC to prevent unplanned pregnancies due to circumstances such as condom failure or instances of forced sex. Factors associated with EC use included being a student at the Faculty of Health Sciences and lacking a consistent current sexual partner.
To enhance access to EC, services should be made available at user-friendly locations for university students. Additionally, ongoing education is essential to inform students about the various forms of EC, their indications, sources of information, and the advantages and disadvantages associated with each method. Future research should also explore how the presence or absence of a consistent sexual partner influences the choice of EC method.
Footnotes
Acknowledgements
We would like to acknowledge all the participants who accepted to participate in this study and Josephine Akullu, a staff at Lira University who also offered support to the research team during data collection. Pre-Publication Support Service (PREPSS) supported the development of this manuscript by providing the authors training, as well as prepublication peer-review and copy editing. This research was funded with support from Center for International Reproductive Health Training at University of Michigan (CIRHT-UM).