
Abstract
Background:
Modern contraceptive use is vital for women’s reproductive autonomy and maternal-child health, yet recent nationally representative studies on its determinants among married women in Lesotho are limited.
Objective:
This study addresses these gaps using the latest Lesotho Demographic and Health Survey to provide updated evidence on prevalence and determinants.
Design:
A cross-sectional study using nationally representative survey data.
Methods:
The 2023–2024 Lesotho Demographic and Health Survey data were used for analysis. A weighted sample of 3102 married women of reproductive age from 400 enumeration areas across 10 districts was included in the analysis. A multilevel mixed-effects binary logistic regression model was employed to identify individual- and community-level factors associated with modern contraceptive use. Significant factors were determined using odds ratios with 95% confidence intervals and a p value of <0.05.
Results:
Modern contraceptive use was reported by 65.6% of married women. Women aged 35–49 were less likely to use modern contraceptives than younger women (adjusted odds ratio (AOR) = 0.65, 95% CI: 0.43–0.98). Women with primary (AOR = 4.5, 95% CI: 1.9–10.4), secondary (AOR = 5.6, 95% CI: 2.4–13.1), or higher education (AOR = 6.1, 95% CI: 2.3–16.5), as well as those whose husbands had higher education (AOR = 1.8, 95% CI: 1.02–3.2), were more likely to use modern contraceptives. Employed women (AOR = 1.4, 95% CI: 1.07–1.5), joint decision-making with husbands (AOR = 1.45, 95% CI: 1.13–1.7), and knowledge of modern contraceptives (AOR = 1.8, 95% CI: 1.09–3.7) were also associated with higher use. Women with one to two living children (AOR = 9.7, 95% CI: 6.3–14.9) and those with three or more children (AOR = 16.4, 95% CI: 9.0–29.9) were more likely to use modern contraceptives. At the community level, women in all other districts had lower odds of use than those in Butha-Buthe.
Conclusion:
Current modern contraceptive use among married women was moderately high. Key predictors included women’s and husbands’ education, employment, parity, joint decision-making, and contraceptive knowledge, while older women and certain districts had lower odds. These findings highlight the need for targeted interventions to enhance education, economic empowerment, spousal communication, and equitable access.
Introduction
Modern contraceptive use refers to the current use of medically approved methods to prevent pregnancy. These include short-acting methods (e.g., pills, condoms, and injectables), long-acting reversible methods (e.g., implants, intrauterine devices (IUDs)), and permanent methods (e.g., sterilization).1,2
Family planning programs play a significant role in decreasing maternal and neonatal mortality through contraceptive use—both by lowering the number of unintended pregnancies and the burden associated with high-risk pregnancies. 3 Modern contraceptive use improves mother’s and child’s health by enabling better birth spacing and reducing unintended pregnancies, which in turn lowers risks associated with maternal morbidity and infant mortality.4,5 In developing countries, addressing postpartum contraceptive use remains a major challenge since most women give birth at home.6 –8 Globally, in 2021, 1.1 billion women of reproductive age (15–49 years) needed family planning; 874 million were using modern contraception, while 164 million still lacked access to it. 9 Modern contraceptive use varied widely across Africa, reflecting regional disparities in access, policy, and cultural norms.10,11 The overall prevalence in Africa was 26%, with country-level estimates ranging from as low as 6% in Guinea to as high as 62% in Zimbabwe. 12 In sub-Saharan Africa, usage rates ranged from 18.4% 13 to 29.6%,14,15 highlighting persistent gaps in coverage across the region. East Africa reported a higher prevalence of 45.7%, 16 while West Africa lagged behind at 16.6%, 17 indicating significant sub-regional differences. In Ethiopia, modern contraceptive use has shown some variation, with estimates ranging from 28%18,19 to 37%, 20 suggesting a gradual but inconsistent uptake over time. Progress in some countries has been attributed to targeted policy interventions, as evidenced by Sierra Leone, where modern contraceptive use increased from 6.7% in 2008 to 20.9% in 2019, largely due to strong government commitment, including the introduction of the Free Health Care Initiative in 2010. 21 In Zambia, a 12% usage rate among adolescent girls was reported, 22 highlighting age-related disparities in access and uptake. At the district level in South Africa, a notably high 84% of women were using contraceptive methods, 23 underscoring the potential impact of localized health strategies. A study conducted in Lesotho among teenagers revealed that nearly one-third reported using contraceptives, with injectable and condoms being the most commonly preferred methods. While 64.5% of respondents understood that contraception prevents pregnancy, only 20% were aware that barrier methods, such as condoms, can also prevent HIV and other sexually transmitted infections (STIs). 24 This highlights important gaps in comprehensive knowledge about the diverse benefits and limitations of different contraceptive methods among adolescents. Although the reported usage rate suggests some level of access and acceptance, the limited understanding of broader sexual and reproductive health implications points to the need for enhanced education and targeted interventions to improve awareness and informed decision-making among young people in Lesotho. Empowering women increases the demand for and satisfaction with family planning.25,26 Women involved in joint contraceptive decision-making with their spouses demonstrated higher utilization rates. 27 Women exposed to media—such as radio, television, or newspapers—and aware of any contraceptive method were more likely to use modern contraceptives.14,28 Women aged 25–34 years were more likely to use modern contraceptives compared to those aged 15–24 years.12,28 Modern contraceptive use was also more common among women with three or more children. 29 Urban residence and a history of unintended pregnancy were positively associated with contraceptive use, while greater distance to a health facility showed a negative association.16,30 Women from households with more children, and those in middle- or high-income groups, were more likely to use modern contraceptive methods. 18 Studies in Lesotho showed that contraceptive use among adolescents was low due to fears of promoting promiscuity and perceptions of irresponsibility by parents and communities. Cultural and religious taboos limit open discussions about sexual health. In addition, poor access—resulting from distant facilities, lack of adolescent-friendly confidential services, and judgmental providers—further discourages use.24,31,32 In the national context of Lesotho, where elevated adolescent fertility, high HIV prevalence, and low uptake of modern contraceptives remain urgent public health concerns,33,34 implementing effective reproductive health interventions is critically important. Despite these insights, nationally representative data on modern contraceptive use and its determinants in Lesotho remain limited. This study uses the 2023–2024 Lesotho Demographic and Health Survey (LDHS) to assess the prevalence and determinants of modern contraceptive use among married women aged 15–49 years. The findings are intended to inform public health decisions, including district-level targeting, postpartum counseling, and improving access to methods such as implants and injectables. The primary objective is to estimate the prevalence of current modern contraceptive use, while the secondary objectives examine variations by sociodemographic factors (age, education, employment, and parity), behavioral factors (knowledge, decision-making), and contextual factors (district) to identify barriers and facilitators that can guide policies and interventions to improve maternal and child health in Lesotho.
Methodology
Study design and setting
This study is a secondary analysis of data from the 2023 to 2024 LDHS, a nationally representative cross-sectional survey conducted by the Ministry of Health. This was the fourth DHS conducted in the country, following previous surveys in 2004, 2009, and 2014. Lesotho is divided into ten districts—Butha-Buthe, Leribe, Berea, Maseru, Mafeteng, Mohale’s Hoek, Quthing, Qacha’s Nek, Mokhotlong, and Thaba-Tseka—which encompass urban, peri-urban, and rural areas. Data collection took place from November 27, 2023 to February 29, 2024.
Reporting guideline: This study follows the STROBE guidelines for cross-sectional studies, 35 with the completed checklist provided as a Supplemental File 1.
Inclusion and exclusion criteria
Inclusion criteria: The analytic sample included married or union women aged 15–49 years (v501 = 1 or 2) from the Lesotho DHS 2023–2024 who had complete, non-missing data on current contraceptive use, as captured by variables v312 (current method) and v313 (method type). The final reported sample comprised n = 3149 (weighted n = 3102).
Exclusion criteria: Women were excluded from the analysis if they met any of the following criteria: they were never married, divorced, separated, or widowed—based on variable v501 with values 0 (never in union), 3 (widowed), 4 (divorced), or 5 (not living together); or if they had missing responses for contraceptive use variables.
Sample design and selection
The 2023–24 LDHS employed a two-stage stratified sampling design across 29 strata, defined by residence (urban, peri-urban, and rural) within each of the 10 districts, except Butha-Buthe (which has no peri-urban stratum). In the first stage, enumeration areas (EAs) served as the primary sampling units. A total of 400 EAs were selected using probability proportional to size. Large EAs were segmented, and one segment was randomly chosen, forming the survey cluster. In the second stage, 25 households were systematically selected from each cluster without replacement. Sampling weights, calculated to adjust for differential probabilities of selection and nonresponse, were applied to ensure representativeness at the national and domain (stratum) levels. Of the 400 clusters, 131 were urban, 45 peri-urban, and 224 rural. From the 10,000 households sampled (3275 urban, 1125 peri-urban, and 5600 rural), a total of 6413 women aged 15–49 years were successfully interviewed: 2396 urban, 735 peri-urban, and 3282 rural. 36 The final reported sample comprised 3149 married women, corresponding to a weighted sample of 3102 (Figure 1). All analyses incorporated the stratification, clustering, and survey weights as specified in the DHS design to produce valid population-level estimates and standard errors. Further details on sample design and selection are available in the LDHS report (https://www.dhsprogram.com/pubs/pdf/FR391/FR391.pdf).
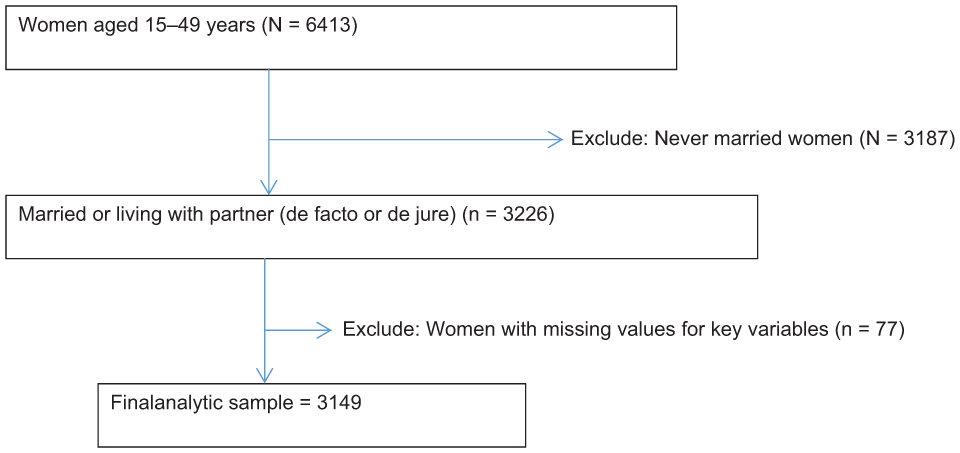
Selection procedure of married women (DHS analysis).
Data sources
The data were accessed from the DHS website (https://www.dhsprogram.com/data/dataset_admin/index.cfm) after registering and obtaining approval. Independent and dependent variables were extracted from the DHS codebook for the women’s record (IR file). The DHS collected data on whether currently married women aged 15–49 years had used modern contraceptives in the 2 weeks preceding the survey. Information was obtained through direct interviews with these women.
Definition
Currently married refers to women who reported being formally married or living with a partner as if married at the time of the survey. 37
Current modern contraceptive use was defined as the current use of any scientifically approved method to prevent pregnancy among women aged 15–49 years in union. The 2023–2024 Lesotho DHS classifies modern methods as female and male sterilization, pills, IUDs, injectables, implants, condoms, emergency contraception, and vaginal barrier methods (e.g., diaphragms and spermicides), coded under DHS variables v312 (current method) and v313 (method type).
Media exposure, in DHS data, is coded as yes if an individual reads a newspaper, listens to the radio, or watches television at least once a week; otherwise, it is coded as no.
Urban refers to areas characterized by high population density, built environment, and infrastructure that support nonagricultural economic activities, services, and social institutions. 38
Peri-urban areas are transitional zones between urban and rural settings, located near cities and characterized by rapid population growth, informal settlements, and mixed land use.39,40
Study variable
Dependent variable
The outcome of interest in this study was the current use of modern contraceptives among women aged 15–49 years. Modern contraceptive utilization is categorized as “1” for those who used at least one of the following methods: short-acting methods (oral contraceptive pills, injectables, male condoms, female condoms, and emergency contraceptive pills), long-acting reversible contraceptives (implants and IUDs), and permanent methods (male and female sterilization)1,2,41; otherwise, it was categorized as 0.
Independent variable
Independent variables were selected based on a review of literature examining factors linked to modern contraceptive use at individual and community levels to capture multilevel influences on behavior. Individual-level variables included age, occupation, religion, knowledge of contraceptives (yes/no), sex of the household head, number of living children and children under 5 years, educational attainment, husband’s or partner’s educational level, wealth index, media exposure, and decision-making autonomy regarding contraceptive use. These variables were chosen due to their established relevance in prior studies and their availability within the DHS dataset. Age was categorized into three groups: 15–24, 25–34, and 35–49 by merging the ranges 15–19 with 20–24, 25–29 with 30–34, and 35–39 with 40–49. Religion was classified as Christian and other (including Islam and non-Christian faiths). Occupational status was grouped into employed (any form of work) and unemployed (not working). The number of living children was categorized as none, one to two, and three or more. Similarly, the number of children under the age of 5 was grouped into none, one, and two or more. In the DHS, educational status was classified as no education, primary, secondary, or higher. The wealth index was categorized into poor (poorest and poorer), middle, and rich (richer and richest). Decision-making on contraceptive use (DHS variable v632) was categorized as “respondent alone” if the woman made the decision independently, “husband/partner alone” if the decision was made solely by the husband or partner, and “joint decision” if the decision was made collaboratively by both partners. Community-level factors included district, residence (urban, peri-urban, rural), ethnicity, distance to health facility (big problem vs not), community literacy (low vs high), community knowledge of modern contraceptives (poor vs good), community wealth index, and community media exposure (low vs high). These variables came from two sources: direct community-level data (district, residence, ethnicity, and distance) and aggregated individual-level data at the cluster level. Community-level literacy, contraceptive knowledge, and media exposure were derived from the corresponding dichotomous characteristics of individual women and categorized as low or high based on the cluster median. The wealth index was classified as low for women with a poor wealth index and high for those with a middle- or high-wealth index.
Statistical analysis
The variables in this study were extracted and analyzed from the IR dataset using STATA version 17.0 statistical software 42 . The extracted data were weighted using the sampling weight (v005) to obtain a valid statistical estimation. The data in DHS were hierarchical; as a result, multi-stage stratified cluster sampling techniques were used. A multilevel logistic regression analysis was conducted to estimate independent variables’ effects on the current modern contraception use to account for cluster effects. Variable selection was guided by a conceptual framework rather than preselection based on statistical significance. Based on the conceptual framework, the selected distal determinants included sociodemographic characteristics such as age, mother’s education, husband’s/partner’s education, occupation, religion, and wealth index. The proximal determinants, representing factors more directly influencing contraceptive use, included media exposure, knowledge of contraceptives, number of living children, number of children under 5 years, sex of the household head, and decision-making autonomy regarding contraceptive use. This categorization follows established causal frameworks in reproductive health.43,44 To ensure robustness and address potential collinearity, we also applied lasso penalized regression as a sensitivity analysis. The lasso procedure selected 12 predictors, highlighting the variables with the strongest and most independent association with the outcome. Education, age, occupation, religion, wealth, household decision-making, family composition (living children, under-five children), knowledge of contraceptives, and media exposure emerged as important predictors. By shrinking irrelevant or collinear variables to zero, LASSO improved model parsimony and addressed multicollinearity, leaving only the most informative predictors for interpretation and prediction. In this analysis, we fitted four distinct models to determine the model that best fits the data. The first model was the null model (a model without the independent variable). The null model gives the variance of the outcome variable attributed to the cluster without the independent variables (to assess the magnitude of the cluster variation in current modern contraceptive use). Model I only includes individual-level factors; Model II only includes community-level factors; and Model III includes both individual and community-level factors. Model comparison and selection were based on log-likelihood values, deviance statistics (−2LL), and the Akaike Information Criterion (AIC). The model with the lowest deviance and AIC, and the highest log-likelihood, was considered the best-fitting model for final interpretation. In the multivariable analysis, the factors associated with the current modern contraceptive use were determined using an adjusted odds ratio (AOR) with a 95% confidence interval (CI). Variations in the magnitude of current modern contraceptive use across different clusters were assessed by the intra-class correlation coefficient (ICC), proportion change in variance (PCV), and median odds ratio (MOR). ICC measures the overall variance in the extent of current modern contraceptive use that can be related to cluster differences. It was calculated as follows: ICC = Va/(Va + Vi), where Va is cluster-level variance and Vi is individual-level variance. PCV was calculated for all models using the empty model as a reference. PCV reflects the proportion of the total observed individual variation in modern contraceptive utilization that is attributable to cluster variations. PCV was computed in the following formula: (Va − Vb)/Va, where Va is the variance of the empty model, whereas Vb is the variance of the subsequent models. The MOR was used to evaluate the cluster-level variance in the likelihood of current modern contraception use. This was assessed by contrasting the median likelihood of current modern contraception use among women who lived in clusters with the lowest risk and those who lived in areas with the highest risk. The MOR was calculated using the following formula: Exp(√2 × VA) × 0.6745 ≈ Exp(√VA) × 0.95, where VA is the area level variance.
Ethical approval
This study is a secondary data analysis based on publicly available Demographic and Health Survey (DHS) data. The DHS Program obtained ethical clearance for data collection from the Institutional Review Board (IRB) of ICF (Inner City Fund) and the relevant national ethics committees in each participating country. Informed consent was obtained from all survey participants by DHS enumerators prior to data collection. For this secondary analysis, additional ethical approval was not required as no personally identifiable information is included, and the data are anonymized and publicly accessible. This is in accordance with the DHS Program data usage policy and relevant guidelines for secondary data use (see: https://dhsprogram.com). We registered and received approval to use the data via the DHS Program’s data access portal.
Results
Individual-level characteristics
A total of 3149 married women were surveyed, and after applying sampling weights to account for the complex survey design, a weighted sample of 3102 women was used for all analyses in this study. About 46.3% of respondents were aged 35–49 years. Female-headed households accounted for 24.2% of the sample. The vast majority of participants (98.4%) identified as Christian. Nearly half of the women (48.1%) were unemployed. Regarding education, most women had attained secondary education (52.7%), while the majority of their husbands had completed either primary or secondary education. Women with one to two living children represented 63.2% of the sample. Approximately 48.9% of women had no children under the age of 5. About 32.9% of women belonged to the poor wealth index category. In addition, 67.9% of women were exposed to media, and 98.6% were knowledgeable about modern contraceptive methods. Furthermore, 47.4% of women reported making their own decisions regarding contraceptive use (Table 1).
Individual-level characteristic.

Community-level characteristics
A total of 400 EAs (clusters) were included as units of analysis. Participants were drawn from 10 districts, with representation ranging from 2.95% in Qacha’s Nek to 32.5% in Maseru. Half of the women (49.7%) resided in rural areas. The Basotho ethnicity accounted for 97.1% of respondents. Over one-third of women (38.4%) lived in communities with low literacy levels, and nearly two-thirds (63.8%) were from communities classified as having a poor wealth index. In addition, two-thirds (66%) of participants came from communities with low media exposure, while about one-tenth (10.6%) lived in communities with limited knowledge of modern contraceptive methods. One-fourth of women (25.9%) reported that distance to a health facility was a major barrier to accessing care (Table 2).
Community-level variables.

Current use of modern contraceptive methods in Lesotho
Of the 3102 weighted women surveyed, 65.6% reported using modern contraceptive methods at the time of the survey. Nevertheless, a notable proportion either did not use any contraception or relied on less effective methods: 32.2% used no method, 0.2% relied on folkloric methods lacking a scientific basis (e.g., herbs or charms), and 2% used traditional methods with lower effectiveness (e.g., rhythm or withdrawal; Figure 2).
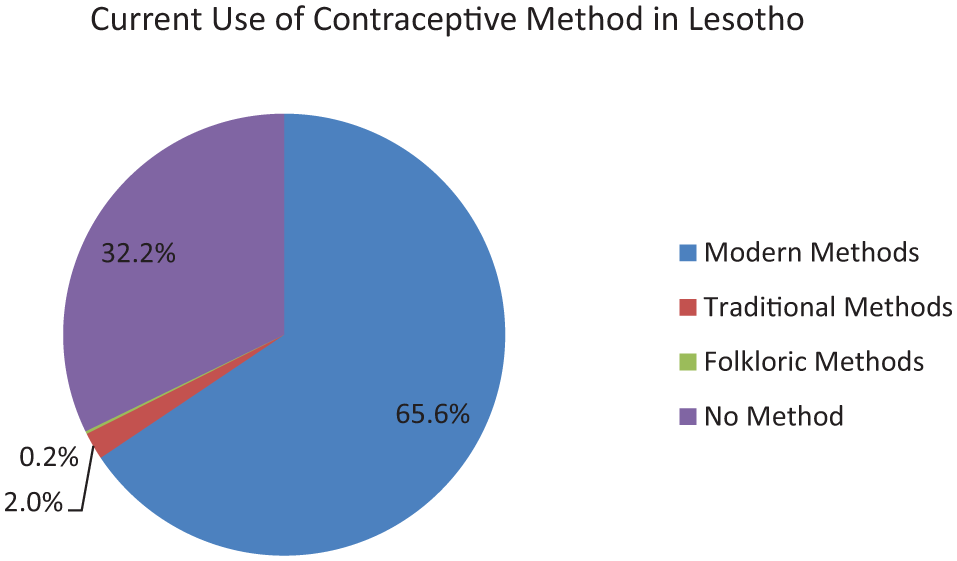
Current modern contraceptive use by method type.
Individual and community-level factors associated with current modern contraceptive use among women in Lesotho
Model selection: The model fitness statistics indicate that adding individual and community-level predictors substantially improved the fit compared to the null model. The log-likelihood ratio increased (became less negative), while the deviance, AIC, and Bayesian Information Criterion values consistently decreased across models, with the lowest values observed in the full model, suggesting that the combined model best explained the outcome (Table 3).
Associated factors of modern contraceptive use.

AIC, Akaike Information Criterion; BIC, Bayesian Information Criterion; ICC, intra-class correlation coefficient; LLR, log-likelihood ratio; MOR, median odds ratio; PCV, proportion change in variance.
The asterisk (*) indicates statistical significance at p < 0.05.
Results of fixed effects (measures of association)
Women aged 35–49 were less likely to use modern contraceptives compared to younger women (AOR = 0.65, 95% CI: 0.43–0.98), suggesting a decline in contraceptive demand with age. Women with primary (AOR = 4.5, 95% CI: 1.9–10.4), secondary (AOR = 5.6, 95% CI: 2.4–13.1), or higher education (AOR = 6.1, 95% CI: 2.3–16.5) were four to six times more likely to use modern contraceptives than those with no education. Similarly, women whose husbands had higher education were nearly twice as likely to use them (AOR = 1.8, 95% CI: 1.02–3.2). In addition, employed women had greater odds of contraceptive use compared to unemployed women (AOR = 1.4, 95% CI: 1.07–1.5), underscoring the role of economic empowerment in reproductive choices. Women with one to two children were almost ten times more likely to use contraceptives (AOR = 9.7, 95% CI: 6.3–14.9), and those with three or more children were about 16 times more likely (AOR = 16.4, 95% CI: 9.0–29.9) compared to women with no children. Joint decision-making with husbands also significantly increased the likelihood of contraceptive use (AOR = 1.45, 95% CI: 1.13–1.7), underscoring the importance of spousal communication and shared responsibility. Furthermore, women with knowledge of modern contraceptives were nearly twice as likely to use them (AOR = 1.8, 95% CI: 1.09–3.7), highlighting the central role of awareness in uptake. At the community level, significant geographic disparities were observed, as women from districts such as Berea, Maseru, Mafeteng, Mohale’s Hoek, Quthing, Qacha’s Nek, Mokhotlong, and Thaba-Tseka had lower odds of contraceptive use compared to those in Butha-Buthe (Table 3).
Results of measure of variation: Measures of variation showed that the ICC decreased from 14.7% in the null model to 11.1% in the full model, implying that a considerable proportion of between-district variation was explained by the included predictors. Similarly, the MOR declined from 1.36 to 1.28, indicating reduced unexplained heterogeneity across districts. The PCV increased progressively, reaching 33% in the full model, which means that one-third of the community-level variance in contraceptive use was accounted for by both individual and community-level factors (Table 3).
Discussion
This study assessed the prevalence and associated factors of current modern contraceptive use among married women in Lesotho using the most recent data from the 2023 to 2024 LDHS.
The findings revealed that 65.6% of married women reported current use of modern contraceptives. At the global level, the demand for family planning remains high, with 1.1 billion women of reproductive age needing it in 2021—yet 164 million still lack access. 9 Lesotho’s contraceptive prevalence indicates some progress in addressing this unmet need, but persistent gaps among specific population subgroups reflect broader trends across sub-Saharan Africa, where usage varies by region and cultural norms.10 –17 This figure is substantially higher than the sub-Saharan African average of 18.4%–29.6%13 –17 and the continental average of 26%. 12 This rate also exceeds those reported in countries such as Guinea (6%) and Zambia (12% among adolescents), yet still falls short of levels observed in some areas, such as Zimbabwe (62%) and certain districts in South Africa, where contraceptive use reached as high as 84%.12,22,23 This prevalence also surpasses earlier regional reports, such as Ethiopia’s 28%–37%18 –20 and even the 2019 estimate from Sierra Leone (20.9%). 21 The comparatively high uptake in Lesotho may reflect ongoing government-led family planning initiatives, expanded access, or growing societal acceptance of contraception among married women, and aligns with expected trends based on regional programs. However, these benefits remain partially unrealized in many developing countries, where postpartum contraceptive use is limited, largely due to the high proportion of home births and insufficient postpartum follow-up.6 –8 Although this study focused on married women, the observed uptake contrasts with earlier findings among adolescents in Lesotho, where contraceptive knowledge and use were limited. 24 Only one-third of teenagers reported using contraceptives, and just 20% were aware of their role in preventing HIV/STIs. This highlights the need for age-specific programming and continued investment in adolescent sexual and reproductive health education to close knowledge gaps and expand access across all age groups. The findings highlight the central role of family planning in reducing maternal and neonatal mortality by preventing unintended and high-risk pregnancies.4,5 Despite progress, barriers persist, particularly among older reproductive-age women and those in culturally conservative districts. Addressing knowledge gaps and strengthening health system resilience, especially in the post-pandemic context, is essential to sustain gains. Lessons from regional initiatives, including Sierra Leone’s Free Health Care Initiative and targeted district-level programs in South Africa, can guide locally tailored strategies to enhance equitable contraceptive coverage.21,23
Unlike previous studies conducted in other African countries,12,28 the present study did not find a significant association between age group (25–34 years vs 15–24 years) and modern contraceptive utilization. In contrast, women aged 35–49 years had lower odds of using modern methods than adolescents, which may reflect declining fertility, perceived reduced need, or age-related misconceptions. These findings suggest that programs should tailor messaging to older reproductive-age women, an area less emphasized in previous interventions. Employed women were more likely to use modern contraceptives than unemployed women. This aligns with studies suggesting that women’s empowerment enhances autonomy and access to reproductive health services,25,26 and that employment may provide the financial means to obtain these services. The findings also highlight the importance of partner involvement in contraceptive decision-making, as women who made decisions jointly were more likely to use modern methods, consistent with the 2018 Mali DHS results. 27 Programs that promote couple communication and shared reproductive health decision-making may be effective in improving uptake. Women with at least primary education were more likely to use modern contraceptives than those without, as education improves their reproductive health knowledge, access to family planning information, household decision-making autonomy, and reduces financial and social barriers. 14 , 25 –28 Women with at least one living child were approximately 10 times more likely, and those with 3 or more children nearly 16 times more likely, to use modern contraceptive methods compared to women without children. These findings suggest that contraceptive use increases with fertility experience, possibly due to heightened awareness of child-spacing benefits, postpartum counseling, or concerns over the financial and caregiving burden of larger families. This trend has been observed across studies.18,29 The analysis revealed that women who had knowledge about contraceptives were nearly two times more likely to use them, demonstrating a strong, significant relationship between knowledge and utilization. This is particularly relevant in the Lesotho context, where previous studies have found that while 64.5% of respondents understood that contraception prevents pregnancy, only 20% were aware of its role in preventing HIV and other STIs. 24 This highlights an important gap in comprehensive knowledge, particularly among adolescents and younger women. The limited understanding of broader contraceptive benefits beyond pregnancy prevention poses a significant barrier to informed decision-making and sustained use. Significant district-level disparities were observed, with contraceptive uptake consistently lower across all districts compared to Butha-Buthe. These disparities likely result from a combination of geographic and infrastructural barriers, sociocultural attitudes, and uneven program implementation. The situation may have been exacerbated in the post-pandemic period, as health systems adapted to service disruptions caused by COVID-19, 45 potentially limiting access in already underserved areas. Evidence from South Africa and Zambia demonstrates that local-level strategies—such as mobile outreach, youth-friendly services, and community engagement—can effectively bridge such gaps.22,23 In addition to structural challenges, cultural and religious norms remain significant barriers in Lesotho, particularly affecting adolescents and unmarried women. Previous studies have shown that taboos, limited youth-friendly services, and provider-related stigma discourage open discussion and use of contraception.24,31,32 Although this study focused on married women, these same social norms may also influence their contraceptive decisions, especially in more conservative districts. Lessons from initiatives such as the Free Health Care Initiative in Sierra Leone 21 and successful local-level programs in South Africa 23 illustrate how political commitment and targeted service delivery can substantially improve uptake. Building on this evidence, Lesotho can strengthen its progress by adopting similar district-specific strategies to promote equitable and sustainable family planning services nationwide.
Strengths and limitations of the study
This study has several strengths, including the use of the most recent nationally representative LDHS data, a large sample size, and the application of multilevel modeling to account for both individual- and community-level factors. Nevertheless, some limitations should be acknowledged. First, the cross-sectional design limits the ability to draw causal inferences. Second, self-reported contraceptive use may be affected by recall bias or social desirability bias. Third, some important variables, such as service quality, reliability of supply chains, and provider attitudes, were not captured in the dataset. Fourth, residual confounding cannot be ruled out despite adjustment for multiple covariates. Fifth, potential classification errors may have arisen in constructing community-level factors, and the assumption that women remained in the same communities or marital status over time may not hold, particularly in the context of male migration. Sixth, the exclusion of unmarried women restricts the generalizability of the findings, as their contraceptive needs may differ from those of married women. Future analyses should therefore include unmarried women and adolescents to provide a more comprehensive understanding of contraceptive utilization among all women of reproductive age. Finally, the use of aggregated community-level variables may introduce ecological bias, as these measures do not always accurately represent individual-level characteristics.
Programmatic and policy implications
Priority should be given to districts with lower contraceptive use by improving supply chain reliability (especially for injectable and implants), expanding mobile outreach, and strengthening facility readiness.
Counseling should be tailored for older women and by parity to ensure that messages address the unique needs of each reproductive subgroup. In addition, family planning programs should support women in managing contraceptive needs during periods of spousal absence, including flexible resupply options and discreet methods.
Male involvement can be encouraged through couples counseling and community dialogue, while ensuring that women retain independent access to services.
Family planning should be integrated with women’s education and empowerment programs to enhance access and equity.
Communication strategies should expand comprehensive knowledge beyond pregnancy prevention to include the broader role of contraception in promoting maternal and child health.
Conclusion
While current modern contraceptive use among married women in Lesotho is relatively high, disparities persist by age, education, employment, parity, decision-making dynamics, and geographic location. Targeted and context-specific interventions such as counseling tailored to age and parity, promotion of joint decision-making, integration with women’s empowerment programs, and district-level resource allocation are essential to increase uptake. Future research should include adolescents and unmarried women to gain a comprehensive understanding of contraceptive needs across all reproductive-age groups.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251385304 – Supplemental material for Prevalence and determinants of current modern contraceptive use among married women aged 15–49 in Lesotho: analysis of 2023–2024 Lesotho Demographic and Health Survey
Supplemental material, sj-docx-1-reh-10.1177_26334941251385304 for Prevalence and determinants of current modern contraceptive use among married women aged 15–49 in Lesotho: analysis of 2023–2024 Lesotho Demographic and Health Survey by Temesgen Gebeyehu Wondmeneh, Kusse Urmale Mare, Hiwot Altaye Asebe, Bizuneh Fantahun Kase and Abdu Hailu Shibeshi in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.