
Abstract
Quantifying women’s empowerment has gained prominence as a research focus globally. We conducted a systematic review of the literature examining the measurement of women’s empowerment in sub-Saharan Africa (SSA). The objectives of the study is to describe quantitative measurements of women’s empowerment based on individual-level data. We searched PubMed/Medline, Scopus and ScienceDirect databases, along with forward and backward citation tracking, for studies published between 2010 and 2025. The search yielded 1898 records, of which 98 studies met the inclusion criteria. All included studies were peer-reviewed, conducted either across multiple countries or within specific national contexts and analysed data from women of reproductive age. The review revealed considerable variations in the definition of women’s empowerment indicators, the conceptualization of dimensions and a general lack of consensus regarding what specific indicators were intending to measure. This review offers a comprehensive synthesis of the existing quantitative evidence on women’s empowerment measurement in SSA. Furthermore, the findings underscore that empowerment is inherently multidimensional, encompassing aspects such as women’s decision-making, control over resources and autonomy in sexual and reproductive matters. Importantly, the selection of dimensions and indicators is often constrained by the availability of relevant data.
Introduction
Discrimination that hinders women from attaining good health and achieve fulfilling lives occurs across various levels of society. These constraints are deeply connected to the limited power, influence, choices and autonomy available to women. In addition to promoting gender equality, empowering women is recognized as a key strategy for addressing poverty, hunger and disease, particularly among women in developing countries.
This literature review follows the definition and concept of empowerment by Kabeer 1 who defined empowerment as a transformative process whereby individuals acquire the ability and power that have been previously denied. This definition views empowerment as a dynamic and interconnected process that includes access to material, human and social resources (pre-conditions), the capacity to set and pursue personal goals (agency) and the realization of desired outcomes (achievement). 2 Recently, more than ever before, scholarly attention has turned to the subject of women’s empowerment. Proponents of women’s empowerment have highlighted its importance, not only as a human right but also to attain health and population goals. 3 Empirically, there is a link between the Women’s empowerment and associated health outcomes, as well as lower fertility preference, 4 family planning, children’s health and nutrition,5–8 improvements in maternal health6,9 contraceptive use 10 and use of antenatal care.11–14 Moreover, the quest to meaningfully measure women’s empowerment is becoming increasingly important in sub-Saharan Africa (SSA) where development is lagging.
As women’s empowerment gains prominence in research across various regions, a wide range of measurement approaches has become increasingly common in the global development agenda. While such measures are important, scholars have struggled to agree on a universal metric to measure women’s empowerment. The adversity faced by scholars may be due to the different forms that empowerment can take, depending on the conditions relating to the individual and their environment. To enhance understanding of the challenges in measuring women’s empowerment, we conducted a systematic literature review examining how women’s empowerment has been measured in SSA and further aimed at summarizing the indicators based on individual-level data and methodologies used to derive them.
Theoretical framework
This study is grounded in liberal feminist theory, which advocates for comprehensive gender equality and the empowerment of women by promoting their access to public institutions and prioritizing women’s issues in national discourse. 15 Liberal feminism emphasizes the importance of educational reforms and the implementation of appropriate legislation as key strategies to address gender disparities. These measures aim not only to reduce inequality between men and women but also to transform societal norms and beliefs. 16
The initial measures of gender dimension of development were done in the 1990s via the United Nations Development Programme (UNDP)’ gender related development index and gender empowerment measure drawing on Amartya Sen’s capability approach. 17 Since then, various indices have been developed by different researchers using different methodologies to measure gender inequality and women’s empowerment.
Together with criticism of the UNDP global indices, the complexity of measuring empowerment emerged. According to Ewerling et al. 17 and Asaolu et al., 18 empowerment is understood to possess several key characteristics: (i) it is a latent construct, meaning that observed behaviours serve only as proxies for an underlying phenomenon; (ii) it can be either intrinsic, reflecting internal agency or instrumental, serving as a means to an end; (iii) it may be universal or context-specific, varying across cultural and social settings; (iv) it can be achieved individually or collectively, indicating that empowerment operates at multiple levels, including the individual, household, community and national levels; (v) it spans various dimensions such as familial, economic, psychological, socio-cultural, legal and political each offering a different lens of application; and (vi) its assessment depends on what is being measured, who is doing the measuring (self-assessment or external evaluation) and the methodology employed, whether qualitative or quantitative.
Numerous indicators were used to capture the complex and multidimensional construct, encompassing various indicators, along with various conditions and factors that influence it. Kishor and Gupta 19 argued that in addition to the indicators of evidence of empowerment, indicators pertaining to access to potential sources for empowerment as well as indicators for setting for empowerment is crucial in operationalizing women’s empowerment. Many of these indicators, particularly those related to women’s empowerment, have been incorporated into nationally representative Demographic and Health Surveys (DHSs). Key indicators of women’s status and empowerment commonly used in national surveys include: literacy and educational attainment; employment status and type of occupation; control over personal earnings; age at first marriage and first birth; contraceptive use; spousal age and education differences; participation in household decision-making; attitudes towards wife-beating; beliefs about a woman’s right to refuse sex with her husband; and barriers women face in accessing healthcare for themselves. In certain countries, additional questions were included to empowerment measures such as autonomy in spouse selection, support from the natal family, ownership of assets, financial decision-making for different purposes, awareness and participation in microcredit initiatives, attitudes towards gender roles, freedom of movement, membership in formal or informal associations and access to banking services.
Materials and methods
Search strategy
We conducted an electronic database search for articles on women’s empowerment on 10 May 2023, with an update completed on 10 June 2025. The databases included PubMed, Scopus and ScienceDirect. The following search terms were used individually and in various combinations: ‘female empowerment’, ‘women’s empowerment’, ‘women empowerment’, ‘women’s autonomy’ and ‘sub-Saharan Africa’ to identify research studies published between 2010 and 2025. The search strategy also incorporated a manual search to identify additional relevant research on the same topic.
Inclusion criteria
In this systematic literature review, studies were considered eligible if they were (i) published in the English language between 2010 and 2025; (ii) applied quantitative analysis; (iii) examined female/women’s empowerment either as an independent variable or dependent variable and described how it was measured; (iv) conducted or analysed data from countries in the SSA region and (v) that relied upon individual level data. The research titles and abstracts were evaluated against these inclusion criteria.
All studies that met the inclusion criteria were imported to Rayyan (a web application designed to facilitate the screening process for researchers working on systematic reviews, scoping reviews and other literature review projects) and duplicates were removed followed by the manual revision. At the first stage of study selection, titles and abstracts of the remaining articles were independently screened by two reviewers (IS and OO). To ensure the quality of the assessment, each study was critically appraised using the Critical Appraisal Skills Programme checklist (Supplemental Table S2). The appraisal focused on key aspects including the validity of the study design, methodology and reported results. Based on these criteria, each study was rated as having a high, moderate or low risk of bias. In the event of conflicts over inclusion, a third reviewer (LK) was involved for resolution. The full texts of the articles that satisfied the inclusion criteria were obtained and examined, while articles that did not fit the inclusion criteria were excluded. Articles with uncertain eligibility were retained for full-text review. The articles selected in the previous screening phase were reviewed in full, and relevant data were manually extracted and independently recorded in a structured spreadsheet by each of the three reviewers. The key information extracted from each article included authorship, title, study location, data, participant details, women’s empowerment and measures of women’s empowerment. Moreover, reference lists of the included studies were screened for further relevant documents. Any disagreements regarding article inclusion were resolved through consensus. All analyses were based on previously published articles; therefore, no ethical approval or patient consent was required.
Results
Search results
The search yielded a total of 1898 publications across all databases used. After removing duplicates, 1846 articles were screened based on title and abstract, of which 1682 were excluded. A total of 164 full-text articles were then assessed for eligibility, leading to the further exclusion of 74 articles. These 74 articles were excluded with reasons such as (i) irrelevant women’s empowerment (WE) measure due to the usage of non-WE oriented indexes, (ii) insufficient data due to the lack of explanation on how WE was measured in their study and (iii) qualitative studies of WE phenomenon rather than quantifying it. This resulted in 90 publications being included in the review. Additionally, the manual searching identified eight more articles. Therefore, the final number of publications included in this review was 98, as shown in Figure 1. Supplemental Table S3 shows the characteristics of the 98 studies included in this review. Of the 98 publications included, 95.9% (n = 94) were rated as having a low risk, while 4.1% (n = 4) were rated as having a moderate risk (Supplemental Table S2).

Flowchart of the study selection procedure.
Study characteristics
All selected publications were published as peer-reviewed papers and proposed women’s empowerment measures based on data collected at the individual level measures. Of the 99 publications, 78.6% (n = 77) relied on data exclusively from the nationally representative DHSs, 3.1% (n = 3) used DHSs data with the Indian National Family Health Survey, 20 DHS together with Multiple Indicator Cluster Survey (MICS)21,22 and the remaining 18.4% (n = 17) were based on other surveys or primary data sources. In addition to studies conducted in SSA countries, the analyses also included five publications20,23–26 that drew on data from both SSA and other low-and middle-income countries. Approximately 55.1% (n = 54) of the publications were based on data from individual countries within the region namely: Uganda,10,27–29 Nigeria,6,30–35 Ethiopia,13,36–45 Benin, 46 Zambia, 47 Kenya,48–51 Democratic Republic of Congo (DRC),52,53 Burkina Faso,54,55 Namibia, 56 Zimbabwe,57,58 Sierra Leon,42,59 Ghana,60–65 Mozambique,66,67 Cameroon,14,68 Tanzania,69,70 Rwanda,71,72 Chad 22 and the Gambia. 73 The remaining 44 studies4,7–9,11,12,18,20,21,23–26,33,74–103 utilized pooled data from multiple SSA countries, allowing for comparative analyses across countries within the region and, in some cases, beyond.
Given the specific survey design, most DHS-based publications analysed the empowerment of women of reproductive age (15–49 years). However, two studies diverged from this: one focused on women aged 35 years and above, 4 and another on women aged 20–49 years. 70 Four studies specifically targeted rural-based married or partnered women,34,44,60,90 while one study centred on urban-based women. 31 Seven studies43,52,62,86,89,97,99 examined women with children under the age of 5 and two studies analysed responses from couples.9,48 One study 23 utilized data from the World Bank Annual Report and applied global indices developed by the United Nations, that is, the gender gap index, gender equity index and social institutions and gender index. As a result, the study did not involve a specific population sample. The characteristics of the publications and the corresponding reference are presented in Tables 1 and 2.
Characteristics of the publications proposing a women’s empowerment measure (n = 98).
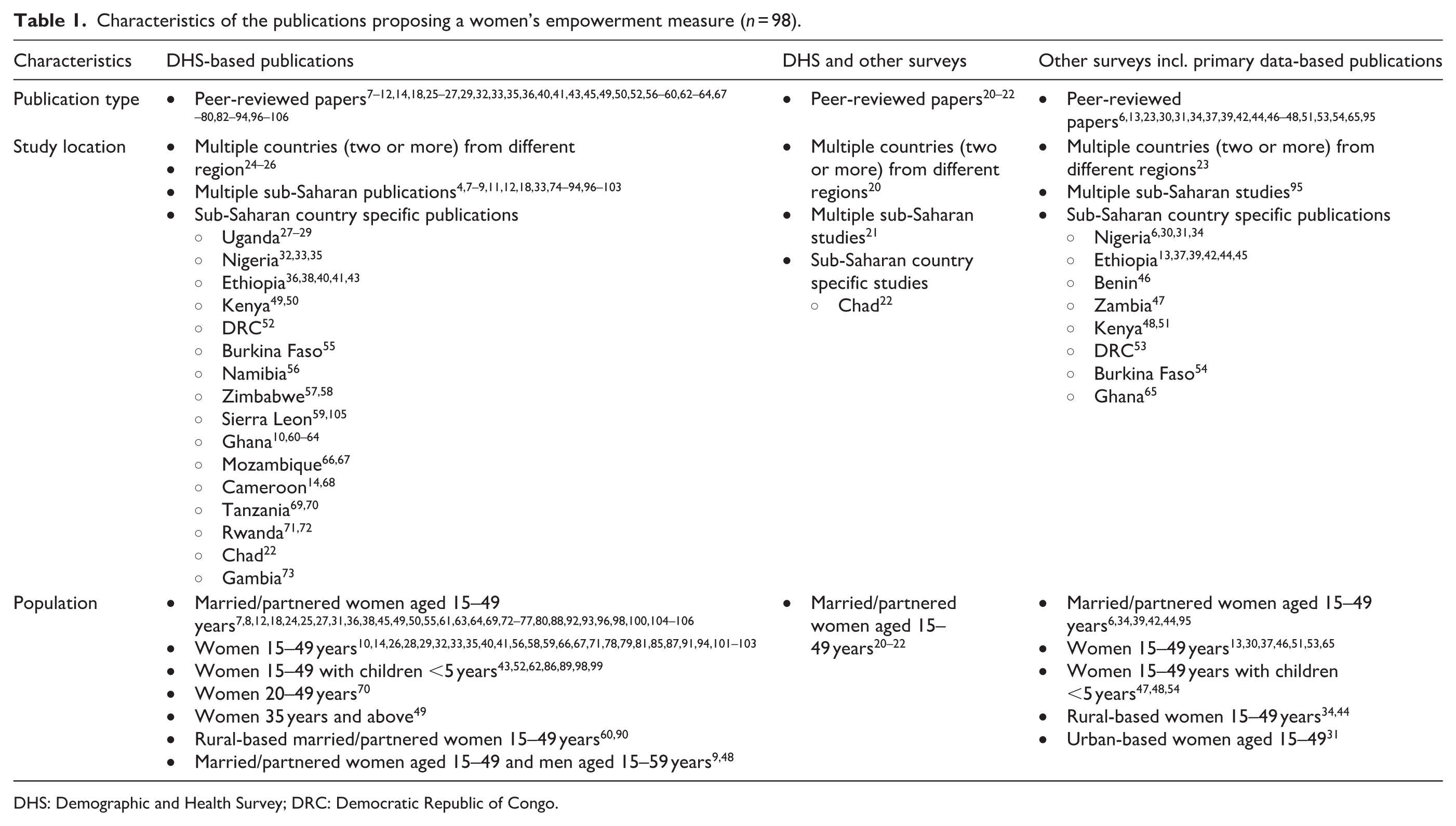
DHS: Demographic and Health Survey; DRC: Democratic Republic of Congo.
Measures of women’s empowerment in SSA, indicators and publications.

GEI: gender equity index; SIGI: social institutions and gender index; SSA: sub-Saharan Africa; STD: sexual transmited diseases.
Women’s empowerment measures
Measuring women’s empowerment is inherently complex. This is reflected in the fact that all publications consistently acknowledged its multidimensional nature, highlighting that empowerment encompasses various overlapping and context-specific domains. The review revealed varying terminology used to describe its components of empowerment. Terms such as empowerment areas, components, dimensions, domains, indicators, indices, measures and variables were used interchangeably. Notably, there is no established consensus on the hierarchical structure or comparability of these terms across selected studies.
In Table 2, we listed dimension/domains along with the corresponding variables, as assigned by the study authors. For ease of presentation, the various sub-dimensions were grouped into four overarching dimensions: familial/interpersonal, socio-cultural/psychological, economic and human and social assets empowerments. An additional category, termed others, was used for sub-dimensions that did not fit neatly into the four overarching dimensions. The average number of dimensions used to measure women’s empowerment was 3.3, ranging from a single dimension, primarily based on DHS-derived decision-making/women autonomy indicators22,32,38,47,52,63,65,74,104 to 11 dimensions in studies utilizing primary data. 13
The most commonly used dimension of women’s empowerment, identified in 76 studies, was socio-cultural/psychological empowerment. This dimension was commonly measured through a set of questions assessing whether a woman believes a husband or partner is justified in beating his wife under specific circumstances. These scenarios typically included: going out without the husband’s permission, neglecting the children, arguing with the husband, refusing sex or burning the food. This construct, referred to variously as attitudes towards violence, perceptions of violence, violence against women or attitudes towards wife-beating, were used in 28 studies,7,8,10–12,14,20,24,40,42,55–57,60,61,66,69,73,78,79,82,83,85,87,92,94,102,105 making it the most consistently applied set of indicators for this dimension.
The familial/interpersonal empowerment, focusing on women’s decision-making power or women’s autonomy was the second most reported subcategory of women’s empowerment used in 74 publications. While certain studies have categorized dimensions such as financial autonomy,39,95 partner prohibition6,30 and access to healthcare,11,18,24,40,49,55,69,106 etc. the variables within these domains predominantly capture women’s decision-making capacities and their dependence on partners for issues pertaining to their own well-being and that of household members.
Most publications (n = 25) in this dimension combined two or three variables of decision-making mostly found in the DHS questionnaire such as the person responsible – respondent’s healthcare, on large household purchases, on visit to family or relatives.
Other notable categories included education/social independence, addressed in 26 studies and economic empowerment and labour force participation, which were collectively featured in 28 publications. Additionally, knowledge level was examined in 14 studies, while access to healthcare indicators appeared in 12 studies. All remaining sub-dimensions and subdomains were covered in fewer than 10 publications. Rather than developing their own measures, several studies employed established frameworks such as the African-based Survey-Based Women’s Empowerment Index (SWPER),21,41,43,64,89,91,97–99,101,103 the updated version SWPER global45,100 and the Harvard Gender Roles Framework.35,59,93
Discussion
This study provided a comprehensive appraisal of evidence describing women’s empowerment measures in SSA. The findings from this study help to paint a complete picture of the complex women’s empowerment measurement in relation to gender and development monitoring in the region. The literature review revealed a great heterogeneity of definitions and dimensions of women’s empowerment which constitute a challenge in defining a measure suitable for comparison across population and over time.
Despite satisfying interest in the subject, many studies involved DHS data which indicate the importance of the survey to women’s empowerment measurement construct. The results revealed that the majority of DHS-based studies used data collected from mostly East and West African countries. Although some studies that focused on MICS data included Southern African countries, country-specific studies from within the region were limited. Identified studies were conducted in the DRC,52,53 Mozambique,66,67 Namibia, 56 Tanzania, 69 Zambia 47 and Zimbabwe.57,58 The relatively low number of studies from Southern Africa may be attributed to the prioritization of other regions (east and west Africa) by international and regional development agencies, often based on perceived developmental needs, larger population sizes, higher fertility rates and greater health burdens.
The DHS datasets play a pivotal role in providing a standardized measurement which are beneficial for comparing various populations in diverse cultures. However, context-specific measures can provide opportunities to reflect women’s life experiences in the contexts in which they live. 105 Such studies, in particular the ones that applied primary data provided additional indicators to the measure which is not available in the DHS standard questionnaire. Moreover, the degree of women’s empowerment is affected by numerous elements at various intrapersonal, interpersonal and ecological levels. Hence, social, economic and cultural systems are (very) crucial in defining the boundaries of empowerment in specific contexts. Other factors, such as the availability and accessibility of health services, women’s position in society and the cultural expectations of women, effectively influence women’s empowerment regardless of their individual or household characteristics.
Household decision-making, attitudes towards violence and control over sexual relations were the most frequent measures of women’s empowerment used in the reviewed studies of this systematic review. This is not surprising, as women’s decision-making was one of the earliest ways of operationalizing women’s empowerment, on which the DHS – commonly used dataset for women’s empowerment measures – is based. The frequent use of decision-making and attitudes towards violence as core domains of women’s empowerment in SSA is contextually appropriate, given the prevailing cultural norms and patriarchal systems that have historically excluded women from decision-making processes and often justified violence as a means of enforcing culturally prescribed gender roles and behaviours.
This systematic review study had several potential limitations. Firstly, most of the research studies reviewed in this study used data from the DHS, which exclude never-married women as a focus of their study. Secondly, only a few studies included matched couples or male perspectives on women’s empowerment and fertility preferences. Collecting information from both partners and analysing it can provide the opportunity to account for men’s characteristics and opinions on women’s empowerment.
Conclusion
This systematic review provided a comprehensive synthesis of the available quantitative evidence of women’s empowerment measurement in SSA. It revealed considerable variations in the definition of women’s empowerment indicators, the conceptualization of dimensions and a general lack of consensus regarding what specific indicators were intending to measure. The most frequently employed dimensions in the measurement of women’s empowerment included decision-making authority, attitudes towards gender-based violence and control over sexual relations. Moreover, this review confirms that measuring empowerment is multidimensional, spanning women’s decision-making and control over resources and sexuality. It is noteworthy that qualitative research is essential for defining the various dimensions of women’s empowerment and outlining the ways in which women may be more empowered. However, the choice of dimensions to include was limited by the availability of data. More studies on women’s empowerment in the Southern African region of the SSA are further recommended to be carried out. In addition, context-specific studies with a specific focus on Southern Africa are required to add to the few existing literatures of women’s empowerment measure using primary data.
Supplemental Material
sj-docx-1-whe-10.1177_17455057251401817 – Supplemental material for Women’s empowerment measurements in sub-Saharan Africa: A systematic literature review
Supplemental material, sj-docx-1-whe-10.1177_17455057251401817 for Women’s empowerment measurements in sub-Saharan Africa: A systematic literature review by Immanuel Shipanga, Opeoluwa Oyedele and Lawrence Kazembe in Women's Health
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
This study is not applicable for ethical approval because all analyses were conducted using previously published studies.
Consent to participate
All analyses were conducted using previously published studies, thus informed consent from respondents or patients were not required.
Consent for publication
Not applicable.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.