
Abstract
Background:
Women’s empowerment is essential for achieving sustainable development goals. It involves enabling women to take control of their lives by giving them the agency, resources, and opportunities they need to make their own choices and reach their full potential. If more women are empowered to use modern contraceptives, greater reductions in maternal mortality will follow. By understanding this association, we can identify key women empowerment dimensions that have an association with family planning utilization and consider ways forward to improve reproductive health outcomes for women.
Objective:
This study aimed to investigate the association between women’s empowerment and modern contraceptive utilization among married mothers in Ethiopia.
Design:
A facility-based quantitative study was employed.
Methods:
A facility-based quantitative cross-sectional study was employed among 305 mothers selected by systematic random sampling at Jimma Town Public Hospital from July 1 to August 31, 2022. The interviewer-administered questionnaire was used for data collection. The collected data were entered into EpiData Manager, version 4.6.0.6, and then exported to SPSS, version 26. Bivariate and multivariate logistic regression analyses were used to investigate the associations between the dependent and independent variables.
Results:
Among a total of 305 study subjects, 301 were used in the analysis. Approximately 65% (95% CI = 59.8, 70.8) of the women utilized modern contraceptive methods. High general self-efficacy (AOR = 4.17; 95% CI = 2.11, 8.23), an internal locus of control (AOR = 3.92; 95% CI = 2.01, 7.65), labor work participation (AOR = 4.53; 95% CI = 1.99, 10.31), and enrollment in elementary education (AOR = 8.30; 95%; CI = 2.96, 23.27) have a statistically significant association with modern contraceptive utilization.
Conclusion:
Numerous dimensions of women’s empowerment are significantly associated with modern contraceptive utilization. The dimension of women’s empowerment needs considerable focus from stakeholders to empower women and enable them to utilize contraceptives and other maternal healthcare services.
Plain language summary
Women’s empowerment is a core agenda of the Sustainable Development Goals, particularly Goal 5, which is dedicated to achieving equality and empowering all women and girls. It is argued that women’s empowerment is key to women’s utilization of sexual and reproductive healthcare services. Previous studies have attempted to link women’s empowerment with reproductive healthcare utilization, despite numerous limitations such as reliance on demographic and health survey data and the study of only a few dimensions or components of women’s empowerment. This motivated us to investigate the association between women’s empowerment and modern contraceptive utilization among married mothers in Ethiopia.
The research team reviewed the available literature to identify commonly agreed-upon dimensions of individual women’s empowerment. Then, we recruited married mothers to assess their modern contraceptive use and its association with these different empowerment dimensions.
This study highlights the association between women’s empowerment and contraceptive utilization among women. A majority of participants utilized modern contraceptives; however, women with greater empowerment in dimensions such as general self-efficacy (an individual’s belief in their capacity to execute behaviors necessary to achieve specific performance attainments), internal locus of control (those who believe they have control over their own behavior), labor force participation (those who have jobs outside of the home), and formal education were more likely to utilize contraception than their counterparts.
This study identified key empowerment dimensions for future interventions to improve contraceptive utilization. Focusing on internal aspects of empowerment, such as self-efficacy and internal locus of control, may increase modern contraceptive use in Ethiopia. Additionally, targeting women with low educational attainment and those not participating in the labor force is crucial to ensure equitable access to contraceptive services.
Introduction
The concept of women’s empowerment is deeply rooted in the sustainable development goals (SDGs), which recognize its fundamental importance in driving development, improving reproductive health outcomes, and positively impacting maternal healthcare service utilization.1,2 The Sustainable Development Goal 5 (SDG-5) aims to attain gender equality and empower all women and girls.3 –5 As Naila Kabeer defined, women’s empowerment is the process by which those who have been denied the ability to make strategic life choices acquire such an ability through agency, resources, and achievement. 6
Theorist from different discipline agree with these three conceptual domains of women’s empowerment definition of Naila Kabeer. They enhanced her definition as an expansion of strategic life choices, strengthening of the voice, and expanding of aspirations. 7 Other researchers also considered the above three domains to measure women empowerment and these domains have about 11 dimensions such as locus of control, general self-efficacy, self-esteem, attitude to gender norms, decision-making participation, freedom of mobility, education, labor force participation, exposure to media, age at pivotal life events which includes first age of marriage and childbirth.8 –11 These dimensions can be categorized as personal, relational, and environmental depending on the level at which they occur. 10
The significance of women’s empowerment is widely acknowledged as a crucial mechanism for facilitating the availability of reproductive and sexual healthcare services for enhanced maternal well-being, including family planning utilization. 12 The utilization of family planning has the potential to prevent one-third of maternal deaths by enabling women to delay childbirth, avert unintended pregnancies, and mitigate the risk of unsafe abortions. 13 In sub-Saharan Africa, only 18.36% of reproductive-age women utilize modern family planning. 14 Despite the government’s efforts, findings indicate that only 28.1% of Ethiopian women utilize modern contraceptives. 15
This low rate of contraceptive use could be attributed to the prevalent disempowerment of women in developing nations, which often leads to reduced access to healthcare services, including modern contraceptives. Factors contributing to this disempowerment include lower decision-making power, low labor force participation, domestic violence, child marriage, adolescent pregnancy, poverty, and illiteracy. 16 Consequently, inadequate women’s empowerment is a key factor contributing to elevated rates of maternal mortality and morbidity, which are largely preventable. 17 Recent findings show that an estimated 810 pregnant and postpartum women die daily from preventable causes. 18 Notably, Africa accounts for approximately 50% of the global burden of preventable maternal mortality, while developed nations represent a mere 0.6%. 19
However, modern contraceptive utilization averts maternal mortality by preventing unplanned pregnancy and its consequences such as unsafe abortion. 20 Findings show that if women utilize modern contraceptives and unmet needs are fulfilled, it can reduce maternal mortality by 44%. 21
Despite government efforts to increase modern contraceptive utilization, it is alarmingly low in Ethiopia. Findings show that the overall prevalence of contraceptive utilization in Ethiopia is only 29.75%. 22 Even though the findings show consistent positive associations between empowerment and modern contraceptive utilization 23 ; only 6% of Ethiopian women in marriage were empowered. 24 The research regarding women’s empowerment and its association with family planning is limited. 23 Furthermore, existing studies predominantly rely on secondary data sources and often incorporate only limited dimensions of women’s empowerment when examining its association with modern contraceptive utilization.25 –27
There is a need for additional primary research that comprehensively assesses various dimensions of women’s empowerment and its association with contraceptive behavior, particularly in the context of Ethiopia, to provide a nuanced understanding of this relationship. Hence, this research investigated the association between women’s empowerment dimensions and modern contraceptive utilization among married mothers at Jimma Town Public Hospitals in 2022.
Methods
Study setting
The study was carried out at public hospitals in Jimma Town, Ethiopia. Jimma Town has two public hospitals, Jimma Medical Center and Shanan Gibe Hospital. It is located at latitude 7°41′3.59″N longitude: 36°49′31.79″E. Jimma Medical Center serves a 15,000,000 population residing in the southwest part of Ethiopia. Jimma Medical Center is the leading teaching and tertiary hospital in Ethiopia and provides services for approximately 15,000 inpatients, 160,000 outpatient attendants, 11,000 emergency cases, and 3888 deliveries annually. Shanan Gibe Hospital is a general hospital; on average, it provides services for 2040 deliveries annually. Approximately 988 women attended delivery and postpartum services at both hospitals during the 2-month duration. The study area was selected as it represented a hospital with high efficiency and performance, and its population was representative of the broader region. The data were gathered between July 1 and August 31, 2022.
Population, sampling procedure, and data collection method
Data were collected from a facility-based cross-sectional study conducted at two public hospitals in Jimma Town: Jimma Medical Center and Shanan Gibe Hospital. All mothers who attended delivery and postpartum service were the source population of the study. In addition, those who fulfilled the eligibility criteria and were available during the data collection period were the population of this study. The inclusion criteria of the study were willingness to participate in it. Mothers with major psychiatric illnesses were excluded. Single population proportion formula was used to determine the sample size. The average of the monthly reports from the first year before the data collection period was used to estimate the number of mothers who attended delivery and postpartum services at the Jimma Medical Center and Shenen Gibe Hospital.
This study focused specifically on married women of reproductive age, as several key dimensions of women’s empowerment, such as attitudes toward domestic violence, household decision-making, and other factors, are particularly relevant and impactful within the context of marriage. Specifically, mothers are more likely to experience the motherhood penalty, an unequal division of labor, 28 and reduced decision-making autonomy regarding both their own lives and their children’s well-being. This increased vulnerability makes them a particularly relevant population for this research.
The sample size was calculated by considering the estimated 2-month reporting of both hospitals, 988. The following assumptions were used during the calculations: Za/2 = standard score for 95% confidence interval for two-sided normally distributed data, which was 1.96; p = the proportion of recommended maternal healthcare utilization taken from relevant literature, which was 47.5% 29 ; and d′ margin of error, 0.05.

then

The estimated number of mothers attending delivery and delivery postpartum in Jimma Town Public Hospital was 988, for which fewer than 10,000 correction formulas were used.

After adding a 10% nonresponse rate, the final minimum sample considered for the study was 305.
To obtain individual participants, first, proportional allocation to each hospital was made by considering the recent 1-year average delivery and postpartum service utilized; there were 648 participants at the Jimma Medical Center and 340 at Shanan Gibe Hospital.
The sampling interval (K) was subsequently calculated by dividing the total number of women by the sample size (n/n = 988/305 = 3). After the first respondent was randomly selected via the lottery method, three mothers who attended delivery and postpartum services were interviewed via a systematic random sampling method.
The data were collected via a structured interviewer-administered questionnaire. The items regarding the justification of wife-beating, household decision-making participation, and other age-related variables were adapted from SWPER Global, which was validated by the Demographic and health survey. 1 The justification of wife-beating is measured by asking whether women justified wife-beating at least under one of the five conditions that show the acceptability of domestic violence. Household decision-making participation assesses whether women can decide alone or jointly on their health care, the number of children they want, large household purchases, and children’s education. Age-related empowerment assesses age at pivotal life events such as marriage and childbirth. Child marriage and adolescent pregnancy indicate a lack of empowerment. 30
The seven locus-of-control items were adapted from Psychological Coping Resources by Pearlin and Schooler. 31 Self-esteem was measured by the Rosenberg Self-Esteem Scale. 32 General self-efficacy was measured by using the General Self-Efficacy Scale (GSES), developed by Schwarzer and Jerusalem and widely used worldwide; this scale includes information about female empowerment, and it has been reported that Cronbach’s alphas range from 0.76 to 0.90.9,33. The variable for women’s participation in the labor force was adapted from a previous study and was measured through six items. 25 The tool for freedom of mobility comprises six items adapted from previous women’s empowerment research (reported Cronbach’s α = 0.84). 34 The tool for measuring family planning utilization and sociodemographics was adapted from an existing survey in Ethiopia that reported a Cronbach’s alpha of 0.976. 35
The data were collected by three female midwives under the supervision of one more experienced Master of Science holder, Midwifery professional. The tools were in English, which were translated to Afaan Oromo and translated back to English before data collection by professional translators, and then researchers checked back translated alignment with the original English questionnaire to avoid potential errors and mistranslation.
To maintain data quality, a pretest was performed on 10% of the sample population at Wallaga University Referral Hospital before actual data collection. Then, the data collection time was estimated, and modifications of tools, such as rephrasing difficult-to-understand questions, clarity of items, and assessed internal consistency of translated scale items were assessed (Cronbach alpha’s values are as follows: freedom of movement, 0.839; locus of control, 0.793; self-esteem, 0.89; general self-efficacy, 0.907; decision-making, 0.73; wife-beating, 0.80; labor force participation, 0.949), and logical order of questions was assessed and modified depending on the pretest.
Study variables and measurements
The dependent variable was modern family planning utilization, which included injectable contraceptives (depot medroxyprogesterone acetate (DMPA)), combined oral contraceptive or/and progesterone-only pills, contraceptive implants, and intrauterine contraceptive devices. Traditional natural family planning is not included.
Questions regarding sterilization were not included in the study questionnaire. As the participants were mothers in the immediate postnatal period, it was deemed inappropriate to inquire about sterilization at this time. Furthermore, condoms and the Standard Days Method were excluded from the analysis as they were not reported as methods of contraception used by any of the women in this study.
The independent variables included were child marriage, adolescent pregnancy, education, household decision-making, attitudes toward violence, freedom of mobility, locus of control, self-esteem, general self-efficacy, weekly media exposure, and participation in the labor force. Sociodemographic factors such as residence and religion were treated as potential confounding variables in the final model.
To measure women empowerment, variables have been selected based on a comprehensive review of relevant literature. These variables were chosen to capture the diverse aspects of women’s empowerment in low- and middle-income countries.8 –11 Our approach to measuring women’s empowerment, including the decision to avoid establishing a cutoff point, was informed by previous research. 11
Statistical analysis
The data were checked, coded and edited properly, entered into EpiData, version 4.6, manufactured by the Epidata Association, Odense, Denmark and subsequently exported to IBM SPSS, version 26, for analysis. The data were subsequently recoded for analysis, after which further cleaning was performed. A descriptive analysis was also performed. All women’s empowerment dimensions and other covariates (residency, religion), were entered into bivariate logistic regression analysis, and independent variables with p < 0.25 were considered for candidates for multivariable logistic regression analysis. Child marriage status was left in the analysis due to collinearity related to adolescent pregnancy. According to the multivariate logistic regression model, variables with p < 0.05 were significantly associated with contraceptive utilization. The Hosmer and Lemeshow goodness-of-fit test showed that the selected model was a good fit for the dataset since the p value was 0.316. The relationship between the women’s empowerment dimension and modern contraceptive utilization was evaluated after adjusting for the covariates by using an adjusted odds ratio at a 95% confidence interval and a p value <0.05 to declare significant associations. Finally, the findings are presented in the text, tables, and graphs. The STROBE Guidelines were used as a framework when preparing the manuscript. 36
Results
Study recruitment results and sociodemographic characteristics
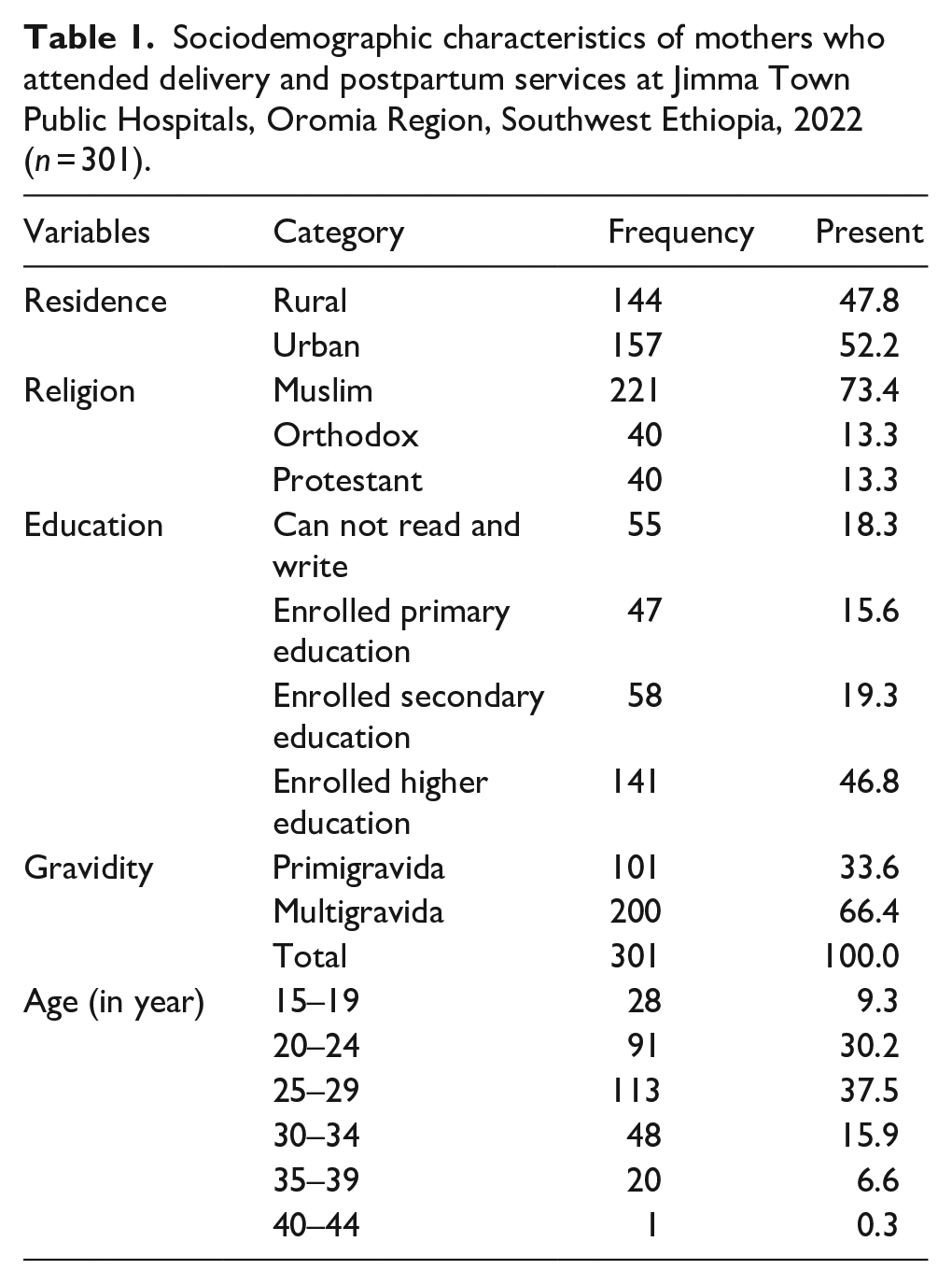
Among a total of 305 study subjects, 301 were included in the analysis. Four questionnaires were rejected due to incomplete information. The participants’ mean age was 26 ± 5 years. Of these, 53.4% were aged between 25 and 34 years, and the majority of participants were Muslims (73.4%; Table 1).
Sociodemographic characteristics of mothers who attended delivery and postpartum services at Jimma Town Public Hospitals, Oromia Region, Southwest Ethiopia, 2022 (n = 301).
Modern contraceptive utilization
This study revealed that approximately 65%, 95% CI (59.8, 70.8), of the women utilized modern contraceptive methods (Figure 1).
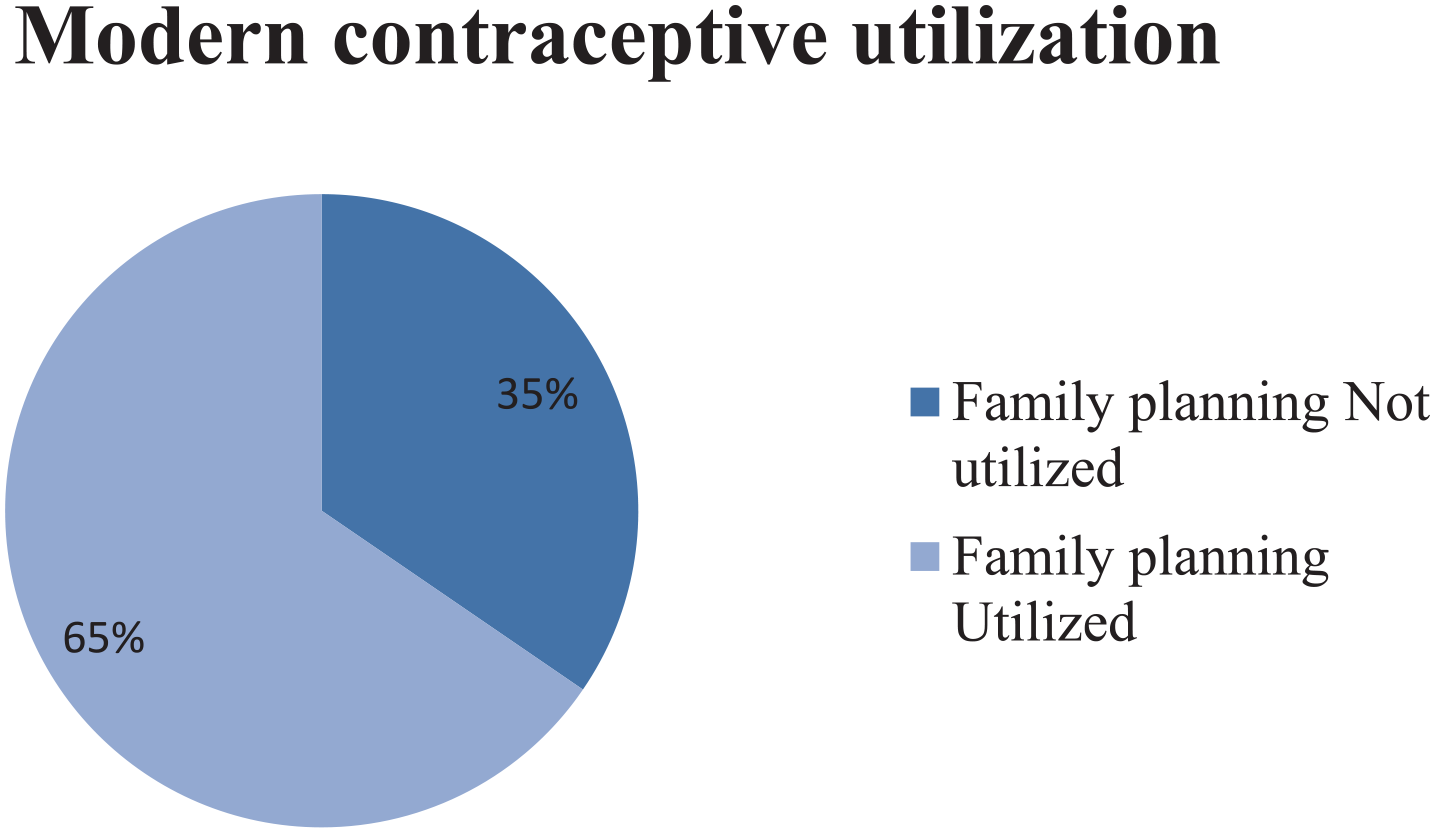
Prevalence of modern contraceptive utilization among mothers attending delivery and postpartum services at Jimma Town Public Hospitals, Oromia Region, Southwest Ethiopia, 2022 (n = 301).
The association between women’s empowerment dimension and modern contraceptive utilization
All 10 dimensions of female empowerment were assessed with respect to contraceptive utilization. While the majority of the dimensions had no statistically significant association with modern contraceptive utilization, general self-efficacy, locus of control, labor force participation, and education had statistically significant associations with modern contraceptive utilization (Table 2).
Bivariate and multivariate logistic regression results for the association between women’s empowerment and modern contraceptive utilization among mothers receiving delivery and postpartum services at Jimma Town Public Hospitals, Oromia Region, Southwest Ethiopia, 2022 (n = 301).

Women’s empowerment dimensions were adjusted for residence and religion, which are considered as potential confounding variables.
Indicates that the adjusted odds ratio was significant at p < 0.05.
General self-efficacy was significantly associated with modern contraceptive utilization (AOR = 4.17; 95% CI 2.11, 8.23). When mothers believe in themselves in managing difficult problems, if someone opposes them, those who can find the means and ways to get what they want, stick to their aims, and accomplish their goals, and are confident that they can deal efficiently with unexpected events and know how to handle unforeseen situations, they believe that they can solve most problems if they invest the necessary effort; they can also remain calm when facing difficulties because they usually find several solutions to their confronted problems and think of a solution while they are in problem, usually handling whatever comes to their way utilizing modern contraceptives four times more than those who did not.
Having an internal locus of control was significantly associated with family planning utilization (AOR 3.92; 95% CI 2.01, 7.65; Table 2). Those who have a high internal locus of control disagree with having little control over things that happen to them; they believe in a way they can solve their problem; they believe that they can change many of the important things in their life; they do not feel helplessness; they do not claim that they have been pushed around in life; they believe that what happens to them majorly depend on themselves; they believe that they can do anything they have set their mind on.
Labor force participation was significantly associated with modern contraceptive utilization (AOR 4.53; 95% CI 1.99, 10.31). Those mothers who participated in labor work, worked throughout the years, and participated in professional work or skills had more history of modern family planning utilization than those who did not.
Education was significantly associated with modern contraceptive utilization (AOR 8.30; 95% CI 2.96, 23.27). Specifically, having an elementary education level had a significant role in the utilization of modern contraceptives in this study.
Discussion
The utilization of contraceptives by women plays a crucial role in safeguarding the health of both women and their children. Empowering women enables them to overcome obstacles within their families and communities and enhances their capacity to make informed decisions regarding the size of their families or the timing of pregnancies.37,38 This study investigated the associations between women’s empowerment dimensions and their use of modern contraceptives. Four dimensions of women’s empowerment—general self-efficacy, locus of control, labor force participation, and education—were found to have a statistically significant association with the utilization of modern contraceptives.
The current study showed that the majority of women utilized modern contraceptive methods. When we compare these findings with those of another study involving Ethiopian demographic and health surveys in the high-fertility region of the nation, 22 the prevalence of contraceptive utilization was greater in our study. This may be due to the fact that the majority of the study participants in our study were from urban communities (52.2%), had a higher education status (46.8%), and had a facility-based study design. Again, this number is greater than that reported in the study performed in Holeta, West Shewa Zone of central Ethiopia. 39
This may be due to the same reasons as those in the above study. Since 2019, there has been good progress in regard to family planning utilization in Ethiopian demographic and health survey, as trends show that modern contraceptive use among married women has increased over the last 15 years, from 8% in 2000 to 41% and 50% in urban settings in 2019. 40 .
Having high general self-efficacy has a statistically significant association with modern contraceptive utilization of approximately fourfold. Another study showed the same finding that general self-efficacy is correlated with voluntary acceptance of contraception, prevention of unintended pregnancies, and the intention to utilize contraceptive methods. 41 In addition, the findings from Kenya and Nigeria show that having high general self-efficacy has a strong association with modern contraceptive utilization. 42 Findings from Iran show that individuals with higher general self-efficacy are more likely to use contraception to avoid an unintended pregnancy. This is because general self-efficacy is a powerful predictor of behavioral intentions and can be attributed to the fact that a strong sense of efficacy improves the ability to cope with barriers. 43 This imply that high self-efficacy empowers women to believe they can successfully use contraception, leading to greater confidence in their ability to implement and maintain contraceptive practices.
Having an internal locus of control has a significantly positive association with modern contraceptive utilization. There were four times more women who had an internal locus of control than women who had an external locus of control. Research has shown that individuals with an internal locus of control are more likely to take proactive measures to manage their reproductive health, including the use of contraceptives. This association suggests that individuals who believe they have control over their lives are more inclined to make decisions regarding contraception based on their preferences and values. 44 Another study from Nigeria performed on adolescents also indicated that individuals with an internal locus of control were more likely to use a contraceptive, whereas those with externalities assumed a higher risk of sexual behavior 45 ; another study from the same country showed that women’s internal locus of control was a significant predictor of utilization of maternal health care. 46 These imply that a sense of control over one’s life and reproductive health increases the likelihood of engaging in behaviors that protect well-being, such as consistent contraceptive use.
Labor work participation has a statistically significant positive association with modern contraceptive utilization. This is in line with the studies from different parts of Ethiopia.47,48 In sub-Saharan Africa, a multilevel analysis showed that labor work participation has a positive statistically significant association with modern contraceptive utilization. 49 In this study, labor work participation was significantly associated with contraceptive utilization; conversely, another study showed that women’s contraceptive utilization enables women to participate in labor work. 50
In addition, in our study having primary-level education has a positive and statistically significant association with modern contraceptive utilization. Secondary education has no statistically significant association with modern contraceptive utilization in our study, and this might be because of underlying population characteristics and small sample size when compared with another national survey, which reports significant educational levels. 15 Multinational findings from East African countries 51 also indicate that education is an enabling factor for modern contraceptive utilization, which is in line with the findings of the current study.
Strengths and limitations
Due to the cross-sectional nature of the study data, establishing a causal relationship between women’s empowerment status and the utilization of modern contraception is not feasible. Additionally, defining and measuring empowerment accurately presents challenges. While the measures selected for this study encompass individual-level dimensions commonly used to assess women’s empowerment, it is important to acknowledge the inherent complexities of this concept. Finally, the generalizability of these findings to the diverse sociodemographic characteristics of the Ethiopian population should be approached with caution.
Implication for practice
This study indicates a significant association between women’s empowerment dimensions such as general self-efficacy, locus of control, labor work participation, and education. This means that women who feel confident in their abilities (general self-efficacy), believe they have control over their lives (locus of control), participate in paid work, and are educated are more likely to use modern contraceptives. This implies that barriers to contraceptive utilization are not only socioeconomic barriers. In other words, it is not just about money or access to services; women’s beliefs about themselves and their ability to make choices also play a major role. Psychological factors have also contributed to the contraceptive utilization of mothers as can be justified by this study. This study provides evidence that women’s psychological well-being and sense of agency are crucial for contraceptive use.
Recommendation
Healthcare professionals should prioritize interventions that target psychological factors influencing contraceptive utilization. These factors include general self-efficacy, self-esteem, and locus of control. Policymakers should prioritize policies that encourage and support women’s participation in the labor force and education. This empower women with economic independence and control over their finances empowers them to prioritize their health and utilize contraceptive. Further research can help determine the causal relationships between women empowerment dimension and contraceptive utilization, which lead to more effective interventions. Additionally, conducting a large national survey that includes qualitative components to investigate the influence of cultural and sociodemographic diversity is recommended.
Conclusion
Generally, the use of contraceptives among women is shaped by the dynamic interplay between women’s empowerment and other factors. 52 However, the dimensions of women’s empowerment, such as education, locus of control, general self-efficacy, and labor work participation, have significant associations with contraceptive utilization. The findings from this research suggest a positive relationship between certain aspects of women’s empowerment and the utilization of modern contraceptive methods. This aspect of female empowerment should considerably focus on stakeholders to empower women and enable them to utilize contraceptives and other maternal healthcare services.
Supplemental Material
sj-docx-1-whe-10.1177_17455057241310641 – Supplemental material for Association between women empowerment and contraceptive utilization in Ethiopia
Supplemental material, sj-docx-1-whe-10.1177_17455057241310641 for Association between women empowerment and contraceptive utilization in Ethiopia by Yonas Abebe, Robera Demissie Berhanu, Lencho Kajela and Yadeta Babu Bayane in Women’s Health
Supplemental Material
sj-pdf-2-whe-10.1177_17455057241310641 – Supplemental material for Association between women empowerment and contraceptive utilization in Ethiopia
Supplemental material, sj-pdf-2-whe-10.1177_17455057241310641 for Association between women empowerment and contraceptive utilization in Ethiopia by Yonas Abebe, Robera Demissie Berhanu, Lencho Kajela and Yadeta Babu Bayane in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.