
Abstract
Introduction:
In Ethiopia, only one in ten reproductive-age women use long-acting reversible contraceptives. Evidence on the utilization of these methods and associated factors among sexually active reproductive-age women in the pastoral area of Northeast Ethiopia is limited. Thus, this study aimed to assess the utilization of long-acting reversible contraceptives and associated factors among sexually active reproductive-age women in the pastoral community of Northeast Ethiopia.
Methods:
A community-based cross-sectional study was conducted from 1 to 30 April 2021 among 572 reproductive-age women selected by a systematic random sampling method. Data were collected using a structured interviewer-administered questionnaire and entered into Epi-info version 7 and then finally exported to Stata version 16 for further analysis. Bivariable and multivariable binary logistic regression analyses were done to identify factors affecting the utilization of long-acting reversible contraceptives. Odds ratio with the corresponding 95% confidence interval were computed and the statistical significance of the explanatory variables was declared at p-value < 0.05.
Results:
Overall, the utilization of long-acting reversible contraceptives was (24.3%; 95% confidence interval = 20.9%–28.0%). It was also revealed that being Orthodox (adjusted odds ratio = 4.10; 95% confidence interval = 2.20–7.65) and Protestant (adjusted odds ratio = 7.86; 95% confidence interval = 1.26–18.97) religion followers, attending higher education (adjusted odds ratio = 3.31; 95% confidence interval = 1.37–7.98), and having a husband who attended higher education (adjusted odds ratio = 4.37; 95% confidence interval = 1.98–9.67) were associated with an increased odds of using long-acting reversible contraceptive methods. Besides, having a good (adjusted odds ratio = 6.69; 95% confidence interval = 2.64–16.95) and moderate (adjusted odds ratio = 3.03; 95% confidence interval = 1.06–8.56) knowledge, and positive attitude (adjusted odds ratio = 3.65; 95% confidence interval = 1.90–7.01) toward long-acting reversible contraceptives were also associated with the utilization of these methods.
Conclusion:
Less than one-fourth of sexually active reproductive-age women in the study area were using long-acting reversible contraceptives. Thus, improving women’s and husbands’ education and women’s knowledge and attitude toward long-acting reversible contraceptives is important to scale up the uptake of these contraceptive methods.
Keywords
Introduction
In developing countries, where access to contraceptives is mainly affected by an inadequate number of trained providers, transportation problems, fewer method options, and stock-outs, 1 unintended pregnancy remains a global public health problem. The rate of unintended pregnancy is higher in developing countries (65 per 1000 women aged 15–44 years) compared to the developed regions (45 per 1000 women aged 15–44 years), of which 59% end in abortion. 2 In Ethiopia, its prevalence ranged from 26% to 31%. 3
Long-acting reversible contraceptives (LARCs) are the most effective birth control methods that can prevent unintended pregnancy for an uninterrupted period of 3–12 years. 4 They include hormonal and non-hormonal intrauterine contraceptive devices (IUCD) and implants (Implanon and Jadelle) that are placed in the uterus and under the skin of the upper arm, respectively, to generate their mechanism of action. 4 Although LARCs are effective in preventing unwanted pregnancies, 5 only 15% of reproductive-age women around the globe use these contraceptive methods. 6 Studies in Nigeria, Malawi, Zimbabwe, Gambia, Uganda, and Kenya found that the utilization of LARCs was 39%, 7 10%, 8 9%, 8 89%, 9 32%, 10 and 21%, 11 respectively.
In Ethiopia, the utilization of LARCs at the national level was 11%. 12 Studies done in specific areas across the countries revealed that the utilization of these contraceptive methods ranged from 4% to 45%.13–17 Previous studies have revealed a higher use of LARCs among married, educated, and older women, and those with smaller family sizes, lower monthly income, and fewer living children. On the other hand, living in rural areas, traveling a long distance to the nearest health facility, not having a history of abortion, not being exposed to mass media, not having a history of contraceptive use, and having inadequate knowledge about contraceptives were found to have a negative effect on the utilization of LARCs.14–21
Ethiopia has implemented different strategies to scale up the utilization of LARC like training health professionals and health extension workers on counseling and provision of contraceptives, establishing a health development army as means to disseminate information regarding contraceptives, and expanding service delivery points to community-based family planning services, social marketing, and outreach service delivery. However, despite these efforts, the utilization of long-acting contraceptives remains low. 22
Moreover, in the Afar region where the fertility rate is higher (5.6 children), only 2.5% of women of reproductive-age use these contraceptive methods. 23 Besides, evidence from the community-based studies on the factors affecting the utilization of these methods in the Afar region is limited. Thus, the current study was intended to assess the utilization of long-acting contraceptive methods and associated factors among sexually active reproductive-age women in the pastoral community, Afar region, Northeastern Ethiopia.
Methods and materials
Study area
This study was conducted in Samara-Logia city administration, which is found in the Awsi-rasu zone of the pastoral region, Afar, Ethiopia. It is situated at a distance of 574 km from Addis Ababa, the capital of Ethiopia. According to the 2019 population projection, it has a total population of 43,203 of which 21,169 are females and 22,034 are males. This city is administratively divided into eight kebelles (the smallest administrative unit in Ethiopia) and has a total of 9864 reproductive-age women.
Study design and period
A community-based cross-sectional study was conducted from 1 to 30 April 2021 to assess the utilization of long-acting contraceptives and associated factors among sexually active reproductive-age women in Samara-Logia city administration, Northeast Ethiopia.
Population
All sexually active reproductive-age women who resided in Samara-Logia city administration for at least 6 months before this study was the source population. The study population was all sexually active reproductive-age women selected by systematic random sampling method in the randomly selected kebelles of Samara-Logia city administration.
Eligibility criteria
Sexually active reproductive-age women who were unable to provide the relevant information due to severe medical and mental illnesses and those who resided in the study area for less than 6 months were excluded from the study. Moreover, pregnant women and those who reported not having sexual intercourse in the last 4 weeks before this study were also excluded.
Sample size determination
For the first objective, a sample size of 376 was estimated using Epi-Info version 7.2.3.1 assuming the proportion of reproductive-age women using LARC to be 33.4% 24 taken from the study conducted previously, 5% margin of error, 95% confidence level, and 10% non-response rate. For the second objective, a sample size of 572 was calculated using Epi-info considering a 95% confidence level, power of 80%, the ratio of exposed to unexposed to be 1:1, LARC utilization among women with a negative attitude (proportion of outcome in the unexposed group) of 27.6%, LARC utilization among women with a positive attitude (proportion of outcome in the exposed group) to be 40.2% 24 and non-response rate of 10%. Finally, the largest sample size (i.e. the sample size for the second objective) was considered as the final sample size for this study.
Sampling procedures
Out of eight kebelles in Samara-Logia city administration, four kebelles were selected by lottery method. Two days before the data collection, a census was conducted to identify the households with eligible women and the number of sexually active reproductive-age women in each of the randomly selected kebelles. Then, based on the number of sexually active reproductive-age women, the sample size was proportionally allocated to each kebelles. Finally, the sampling interval was estimated (k = 9) and eligible reproductive-age women were selected using systematic random sampling. In households with more than one eligible woman, the lottery method was used to select a woman to be included in the study (Figure 1).
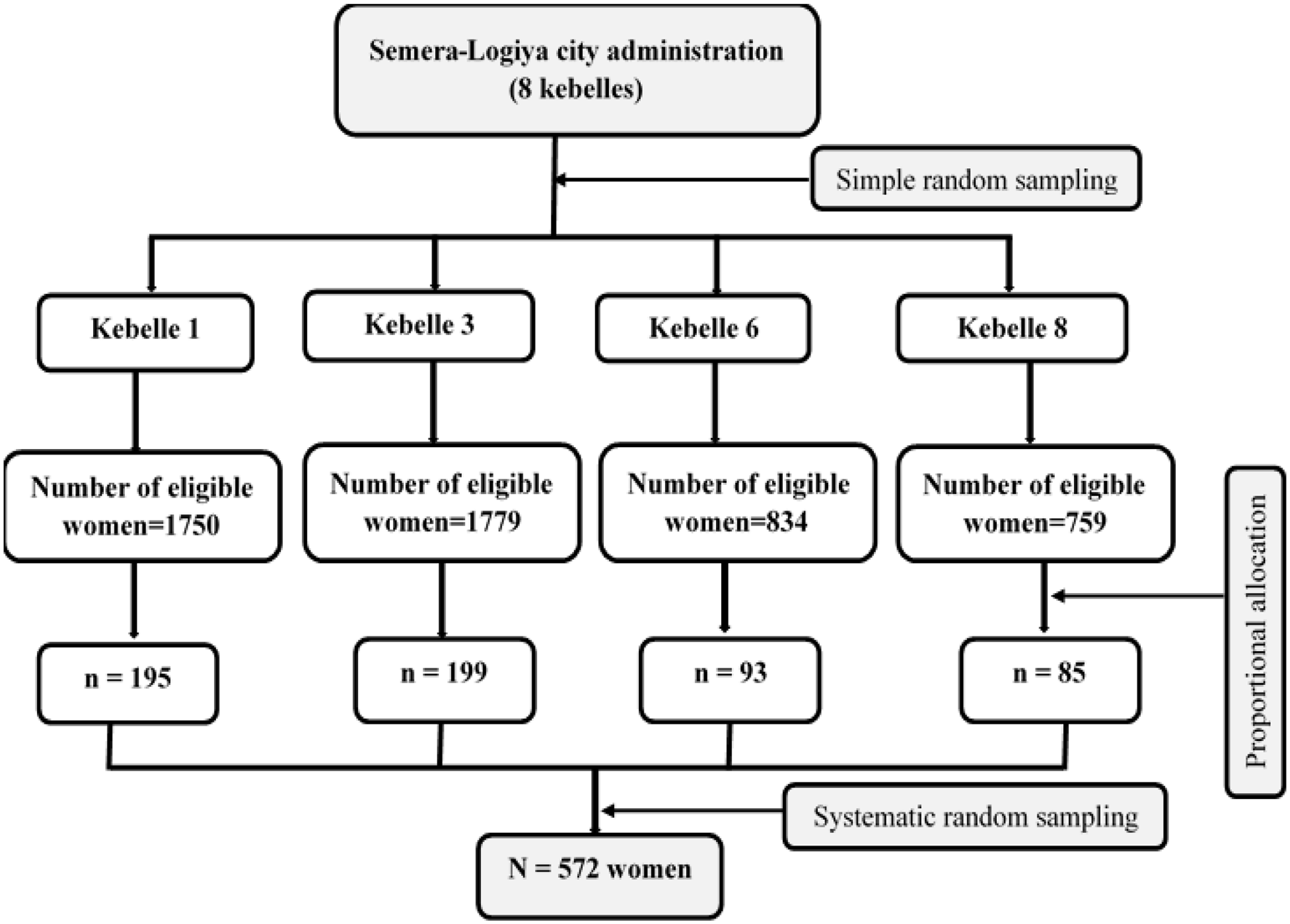
Schematic presentation of sampling procedures for the study on the utilization of long-acting reversible contraceptives and associated factors among sexually active reproductive-age women in Samara-Logia city administration, Northeast Ethiopia, 2021.
Study variables
The dependent variable in this study was “current utilization of long-acting reversible contraceptive methods” among sexually active reproductive-age women, which was dichotomized as “Yes” (when women reported currently using the LARC method) and “No” (when women reported not using the LARC method). Independent variables included socio-demographic characteristics (age, religion, ethnicity, marital status, nature of marriage, duration of union, women’s education and occupation, husband education and occupation, household monthly income, possession of radio and/or TV, and family size), obstetric variables (ever gave birth, age at marriage, age at first birth, number of living children, current desire for children, number of pregnancies, history of unintended pregnancy, history of abortion, decision-maker on the number of children, type of contraceptive used before), and information-related variables (heard about LARCs, knowledge, and attitude toward LARCs).
Definitions of variables
Sexually active reproductive-age women: reproductive-age women (15–49 years) who reported that they have had sexual intercourse, regardless of their marital status in the last one month during the period of data collection were considered as “sexually active.”
LARCs. This included hormonal and non-hormonal IUCD, Implanon, and Jadelle. IUCDs are placed in the uterus and can prevent unintended pregnancy for 10–12 years, while Implanon and Jadelle are placed under the skin of the upper arm and can prevent unintended pregnancy for 3 and 5 years, respectively.
Knowledge about LARCs. This was assessed using six knowledge-related questions and women were categorized into three groups based on the number of questions correctly responded. Thus, women who correctly responded to less than 60% of knowledge questions were coded as having “poor knowledge,” those who provided correct responses to 60%–79% of questions were coded as having “moderate knowledge,” and women who correctly responded to 80% of question and above were categorized as having “good knowledge.” 14
Attitude toward LARCs: This was measured using six items on a 3-point Likert-type scale (1 = neutral, 2 = disagree, and 3 = agree). Then, the mean score of the responses for six items was obtained and women with a score greater than or equal to the mean value were considered as having a “positive attitude” and those with a score less than the mean score were grouped as having a “negative attitude” toward LARCs. 14
Data collection tool and procedures
Data were collected using a pretested structured interviewer-administered questionnaires adapted from the literature.19,20,24–28 The questionnaire was initially prepared in English and translated to Amharic and local (Afaraf) languages to fit the context. The Amharic- and Afaraf-version questionnaires were translated back to English to check for the logical follow and consistency of the meaning. Four female health professionals with diploma qualifications who were fluent in both Amharic and Afaraf languages were recruited as data collectors and two health professionals with BSc qualifications were employed as supervisors.
Data quality control
Data collectors and supervisors were trained for 2 days on sampling techniques and data collection tools and procedures. Before pretesting and actual data collection, the data collection instrument was checked by maternal and reproductive health experts for validation. The tool was pre-test on 29 sexually active reproductive-age women in Dubti town and modified based on the results of the pretest. Supervision of the data collection activities was undertaken by two health professionals and the collected data were checked for completeness, accuracy, and consistency by supervisors on daily basis. Data were cleaned and cross-checked by the principal investigator before entry and analysis.
Data management and statistical analysis
Data were entered into Epi-info version 7.2.3.1 and exported to Stata version 16 for further analysis. Descriptive results were presented by the text, frequency tables, and figures. Bivariable binary logistic regression analysis was done and variables with p-value < 0.25 were considered as the candidate variables for the final model. Finally, a multivariable binary logistic regression analysis was carried out to identify factors affecting the utilization of LARCs. Adjusted odds ratio (AOR) with the corresponding 95% confidence interval (CI) was computed and the statistical significance of the explanatory variables was declared at a p-value < 0.05. Multicollinearity between the independent variable was checked using variance inflation factor (VIF) and the VIF values for the variables included in the final model were less than 10, indicating there was no collinearity between variables. The model fitness test was checked using the Hosmer and Lemeshow goodness-of-fit test and the p-value of this test was 0.41 suggesting the model was best fitted.
Ethical approval and consent to participate
Ethical approval was obtained from the Research Ethics Review Committee of the College of Medicine and Health Sciences, Samara University dated 5 May 2021 and numbered ERC0021/2021. A formal letter of permission to conduct this study was also received from the administration of Samara-Logia city. Written informed consent was obtained from each study participant before the interview. Confidentiality was maintained by excluding personal identifiers of the study participants and the collected data were not shared with anybody other than the authors mentioned in this work.
Results
Socio-demographic characteristics
A total of 569 sexually active reproductive-age women were included in the study, giving a response rate of 99.5%. Five hundred thirty-one (93%) women were in the age group of 20–34 years, with a mean age of 27.4 ± 4.0 (SD) years. More than half (57.6%) of women were Muslim religion followers and the majority of them (86.3%) were married, of which 446 (78.4) were in a monogamous union. Regarding educational status, 177 (31.1%) women and 166 (33.8%) husbands of women included in this study did not attend formal education (Table 1).
Socio-demographic characteristics of sexually active reproductive-age women in Samara-Logia city administration, Afar, Northeast Ethiopia, 2021 (n = 569).

Obstetric characteristics
The mean age of respondents at first marriage was 18.9 ± 2.1 (SD) years and 262 (52.0%) women were married at the age of 18 years or above. Five hundred one (88.1%) women ever gave birth and the mean age at first birth was 20.0 ± 2.3 (SD) years, of which 387 (76.8%) gave their first birth at the age of 18 years or above. More than one in four women (45.8%) had three to four children, 36 (6.3%) and 41 (7.2%) women encountered unintended pregnancy and abortion, respectively. For 400 (81.5%) women, the decision regarding the number of children was jointly made by women and their husbands. Furthermore, 379 (77.2%) women did not discuss contraceptives with their husbands or partners and 370 (75.4%) did not have their husband’s support for contraceptive use (Table 2).
Obstetric characteristics of sexually active reproductive-age women in Samara-Logia city administration, Afar, Northeast Ethiopia, 2021 (n = 569).

LARC: long-acting reversible contraceptives.
Women’s knowledge about LARCs
Overall, more than half (51.3%) of sexually active reproductive-age women in this study had good knowledge about LARCs, while 138 (24.3%) and 139 (24.4%) had moderate and poor knowledge about these contraceptive methods, respectively. The majority of study participants (94.1%) mentioned that IUCD is not appropriate for women at higher risk of sexually transmitted infections and 483 (84.9%) reported that implants prevent pregnancy for at least 3 years. Moreover, 171 (30.1%) women stated that IUCD has no interference with sexual intercourse and desire. Less than 50% (48.0%) of the study participants stated that LARCs are not immediately reversible. More than three-fourths of women (77.3%) mentioned that IUCD can prevent pregnancies for more than 10–12 years and 504 (88.5%) stated that implants require minor surgical procedures during insertion and removal.
Women’s attitude toward LARCs
Regarding attitude toward LARCs, 386 (67.8%) women had a negative attitude. More specifically, 401 (70.5%) of the respondent agreed that using these methods might restrict normal daily activities and 491 (86.3%) women disagreed that using LARCs did not store blood in the abdomen and cause cancer. About half (50.6%) of respondents agreed that insertion and removal of IUCD were not painful and 172 (30.2%) agreed that using implants did not cause heavy and irregular menses. In addition, 291 (51.1%) and 362 (63.6%) women agreed with the statements that using LARC requires good nutrition and IUCD insertion causes loss of privacy, respectively.
Utilization of LARCs
Overall, the utilization of LARC methods among sexually active reproductive-age women in the study area was 24.3% (95% CI = 20.9%–28.0%). Out of women who used these contraceptive methods, 120 (87.6%) were using implants (Implanon and Jadelle) and 17 (12.4%) were using IUCD. It was also found that as the women’s level of education increased the utilization of these methods increased from 12.3% among women with no education to 43.4% among women who attended higher education (Figure 2). Similarly, the utilization of these contraceptive methods was increased with women’s knowledge about these methods (Figure 3).

Utilization of long-acting reversible contraceptives across women’s education in Samara-Logia city administration, Afar, Northeast Ethiopia, 2021 (n = 569).
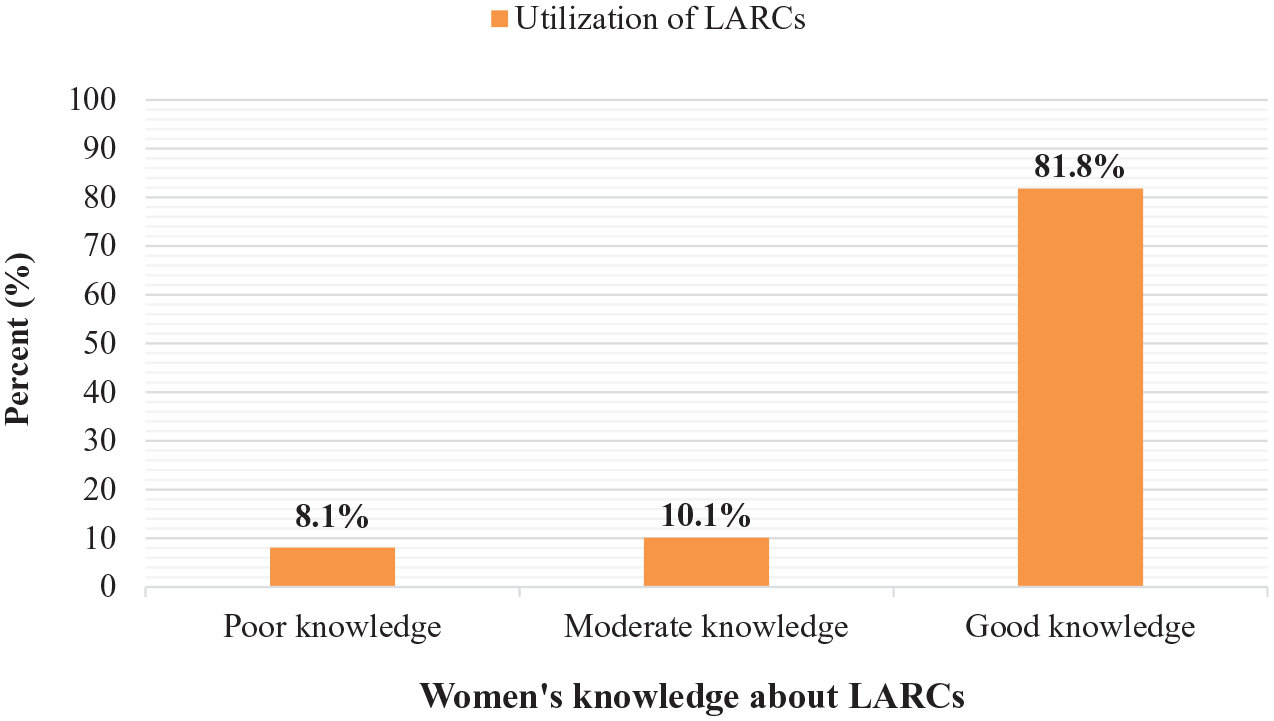
Utilization of long-acting reversible contraceptives across women’s knowledge about LARCs in Samara-Logia city administration, Afar, Northeast Ethiopia, 2021 (n = 569).
Factors affecting the utilization of LARCs
In the crude analysis, religion, nature of marriage, women’s education and occupation, husbands’ education, age at first marriage and childbirth, women’s knowledge and attitude toward LARCs, and husbands’ support for using contraceptives were significantly associated with the utilization of LARCs. However, in the adjusted analysis, only religion, women’s and husbands’ education, knowledge, and attitude toward LARC were found statistically significant. Based on this, the likelihood of using LARCs was increased among Orthodox (AOR = 4.10; 95% CI = 2.20–7.65) and Protestant (AOR = 7.86; 95% CI = 1.26–18.97) religion followers, those who attended higher education (AOR = 3.31; 95% CI = 1.37–7.98), and whose husbands attended higher education (AOR = 4.37; 95% CI = 1.98–9.67). Moreover, having a good (AOR = 6.69; 95% CI = 2.64–16.95) and moderate (AOR = 3.03; 95% CI = 1.06–8.56) knowledge, and positive attitude (AOR = 3.65; 95% CI = 1.90–7.01) toward LARCs were associated with an increased odds of using these methods (Table 3).
Results of bi- and multivariable logistic regression analyses for factors affecting the utilization of LARCs among sexually active reproductive-age women in Samara-Logia city administration, Afar, Northeast Ethiopia, 2021.

LARCs: long-acting reversible contraceptives; COR: crude odds ratio; AOR: adjusted odds ratio; CI: confidence interval.
Statistically significant variables at p-value < 0.05.
Discussion
This study aimed to assess the utilization of LARCs and associated factors among sexually active reproductive-age women in the pastoral community of Northeast Ethiopia. Accordingly, the overall utilization of these contraceptive methods was 24.3% (21.9%–28.0%), which is similar to the findings of the studies in Bahir Dar (20.7%), 29 Hawassa (22%), 30 Gojjam (22.7%), 16 Wolaita (23%), 31 Mizan-Aman (25.1%), 32 and Shashemene (28.1%), 33 Ethiopia.
However, our finding is higher than the results of the studies done in Silte (18.3%) 14 and Mekelle (16.4%), 34 Ethiopia. In contrast, this prevalence is lower than the findings of the studies conducted in Gondar (33.7%), 6 Harari (38%), 35 Afar (33.4%), 24 and Lay-Armachiho (44.7%), 28 Ethiopia, and Uganda (31.7%), 10 Nigeria (38%), 7 and Gambia (89%). 9 This discrepancy might be due to the methodological differences and variations in the study time and setting, outcome variable definition, and background characteristics of women included in the studies. For instance, most of the previous studies were health institution-based and some of them included Depo-Provera6,10 in the definition of LARC methods.
The result of multivariable logistic regression analysis showed that religion, women’s and husband’s education, women’s knowledge, and women’s attitude toward LARCs were the factors significantly associated with the utilization LARCs. For instance, the odds of using LARCs among Orthodox (AOR = 4.10; 95% CI = 2.20–7.65) and Protestant (AOR = 7.86; 95% CI = 1.26–18.97) religion followers were increased by about four and eight times, respectively, compared to Muslim religion followers. This finding is in agreement with the result of a study in Nigeria. 7
It was revealed that the likelihood of using LARCs among women who attended higher education was more than three times higher (AOR = 3.31; 95% CI = 1.37–7.98) compared to those with no formal education. This finding is similar to that of Kenya, 11 Gondar, 6 and Harari, 35 Ethiopia. This can be explained by the fact that educated women might have a better awareness of the benefits of contraception methods and thus be more likely to use the contraceptive methods compared to uneducated women.
A similar association was found between women’s use of LARCs and their husband’s educational status. Hence, the odds of using these contraceptives among women whose husbands attended higher educational levels (AOR = 4.37; 95% CI = 1.98–9.67) were increased by more than four times compared to those women whose husbands had no formal schooling. This finding is in line with the results of the previous studies in Southeastern Ethiopia 15 and Nepal. 36
In this study, women who had a good (AOR = 6.69; 95% CI = 2.64–16.95) and moderate (AOR = 3.03; 95% CI = 1.06–8.56) knowledge about LARCs were more than six and three times more likely to use these contraceptive methods, respectively, compared to those having poor knowledge. This finding is consistent with the results of the studies in Ethiopia24,30 and Indonesia. 27 This might be because having better information about contraceptives might enable women to realize the advantages of using these services which in turn results in the utilization of the contraceptive methods.
The likelihood of using LARCs was also found to be increased by 3.65 times among women with a positive attitude toward LARCs (AOR = 3.65; 95% CI = 1.90–7.01) compared to women with a negative attitude. This finding is supported by previous studies conducted in Northwest Ethiopia, 21 Wolaita, 31 Oromia, 26 and Tigray, 34 Ethiopia, which reported having a positive attitude as an enabling factor for the utilization of long-acting contraceptive methods. This might be because having a positive attitude could avoid women’s misconceptions and wrong social beliefs about contraceptives and thus encourage them to use the service.
Limitations of the study
Although we conducted a community-based study, its cross-sectional nature does not show the cause-and-effect relationship between the explanatory and outcome variables. In addition, respondents might not have fully disclosed their opinion regarding LARCs and abortion history due to social desirability bias that might have affected the results of the study.
Conclusion
The utilization of LARCs in this study was relatively low. Religion, women’s education, husband’s education, and women’s knowledge and attitude toward LARC methods were identified as the factors affecting the utilization of LARCs. Thus, improving women’s education, addressing religious barriers, and health information dissemination to fill the knowledge and attitudes gaps are crucial in scaling up the utilization of these contraceptives.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221116514 – Supplemental material for Factors affecting utilization of long-acting reversible contraceptives among sexually active reproductive-age women in the pastoral community of Northeast Ethiopia: A community-based cross-sectional study
Supplemental material, sj-docx-1-whe-10.1177_17455057221116514 for Factors affecting utilization of long-acting reversible contraceptives among sexually active reproductive-age women in the pastoral community of Northeast Ethiopia: A community-based cross-sectional study by Kusse Urmale Mare, Ezana Abrha, Ebrahim Mohammed Yesuf, Setognal Birara Aychiluhm, Abay Woday Tadesse, Simeon Meskele Leyto, Kebede Gemeda Sabo, Getahun Fentaw Mulaw, Osman Ahmed Mohammed and Oumer Abdulkadir Ebrahim in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.