
Abstract
Background:
Discontinuation of contraceptives without any change in fertility intention is often associated with unintended pregnancy which ends up with induced abortion and unplanned birth. Despite the Ethiopian government’s emphasis on the provision of long-acting contraceptive methods, little attention has been paid to the study of its discontinuation; particularly, no study has been reported in the study area. Thus, this study aimed to assess the discontinuation rate of long-acting reversible contraceptives and associated factors among reproductive-age women in Butajira town, Central Ethiopia, 2020.
Methods:
Community-based cross-sectional study was conducted from 1 April to 1 May 2020. A systematic random sampling method was used to select 227 women. Data were collected by a structured and pretested questionnaire. Epi-data (version 4.6.2) and Statistical Package for the Social Sciences (version 25) were used for data entry and analysis, respectively. A multivariable logistic regression model was used to predict the relation between dependent and independent variables. Finally, a significant statistical association was assured using an adjusted odds ratio at a 95% confidence interval and p value < 0.05.
Results:
This study revealed that the discontinuation rate of long-acting reversible contraceptives was 50 (22.5%; 95% confidence interval: 17.8–27.2). The main reason for discontinuation was facing side effects 26(52%); from these menstrual disruption 19 (73.1%) was the main reason. Time consumed to reach the health facility (adjusted odds ratio: 6.16, 95% confidence interval: 1.46–25.97), desire to have more children (adjusted odds ratio: 5.3, 95% confidence interval: 1.13–24.81), and counseled about the benefit of long-acting reversible contraceptives (adjusted odds ratio: 0.08, 95% confidence interval: 0.02–0.39) were predictors of discontinuation of long-acting reversible contraceptives.
Conclusions and Recommendations:
This study showed that the discontinuation rate was high when compared to Ethiopian Demographic Health Survey 2016. Routine pre-insertion counseling about the benefits and side effects of long-acting reversible contraceptives by healthcare providers is highly recommended. In addition, we recommend further trials using larger sample sizes on predictors of discontinuation of long-acting reversible contraceptives.
Keywords
Introduction
Long-acting reversible contraceptive (LARC) methods (implants and intrauterine devices) are among the subclass of modern contraceptive methods. They provide effective contraception for a long period of time without requiring the action of the user and with minimal load to the user after initiation. 1 Women can prevent unwanted pregnancies at least for 3 years after using implants and 10 years after using copper intrauterine device (IUD) with the immediate return of fertility after removal of these devices. 2 Contraceptive utilization helps couples and individuals to decide freely the number and spacing of children. The growing use of the contraceptive method has resulted in the improvement of health-related outcomes, such as maternal mortality and infant mortality. 3
Contraceptive discontinuation is a worldwide problem that may be connected with the occurrence of unintended pregnancy. Every year, about one-third of the 182 million pregnancies occurring worldwide are unplanned. Contraceptive discontinuation may indicate a missed opportunity to promote and sustain contraceptive use, and, therefore, it can be used to measure the effectiveness of family planning services. 4 The discontinuation of contraceptives including LARCs without any change in fertility intention is often associated with unintended pregnancy which ends up with induced abortion and unplanned birth. 5
Even though many experts believed LARC to have higher continuation rates as compared to other methods of contraceptives but evidence from different studies indicated that discontinuation has been increasing. The Demographic and Health Survey (DHS) analysis of 60 countries reported that the discontinuation rate of an IUD was 14.3%. 6 Based on the report of developing countries 13.1%, 26.3%, and 36.7% of IUD users women discontinued at the first 12, 24, and 36 months, respectively. 7 Evidenced from 60 DHSs three months after discontinuation revealed that 40% or more women were at risk of conception: in Egypt (40%), Ethiopia (42%), Kenya (51%), Malawi (73%), Tanzania (56%), and Zimbabwe (47%). 6
According to Ethiopian DHS 2016, the overall discontinuation of contraceptives at 12 months was 35%, of which 13% of them were IUD users and 11% of them were implant users among reproductive-age women. 8 The quality of family planning services plays an important role in contraceptive use because it is likely to affect adoption and contraceptive continuation. 9 From the existed limited research socio-demographic characteristics (age, marital status, and educational status), reproductive-related characteristics (history of abortion, number of living children, and parity) and method-related factors (side effect, counseling, satisfaction with the service given, information about family planning) were factors associated with discontinuation of LARCs.9–12
In 2003, the Ethiopian Ministry of Health implemented the health extension program, which was aimed to increase access to reproductive health care including family planning.13,14 In spite the Ethiopian government had been working on improvement of reproductive health services and making health facility services accessible and usable for all reproductive-age women over the past decade, encouraging contraceptive continuation has been given less concern than enhancing new adopters in the country. 15
There is no study conducted on the discontinuation of IUDs and other Implants (Jadell) in Ethiopia except for a few studies on implant discontinuation. Moreover, assessing the discontinuation rate of LARCs and factors associated with methods is important to guide public health planners, policymakers, and implementers to plan and design appropriate intervention strategies in order to enhance the LARC method continuation rate. Therefore, the main aim of this study was to determine the discontinuation rate of LARCs and associated factors among reproductive-age women in Butajira town, Central Ethiopia, 2020.
Methods
Study area and period
The study was conducted in Butajira town from April 01 to May 01, 2020. Butajira is a town found in Central Ethiopia and 109 km far from Addis Ababa. It is located at the base of Zebidar Massif in the Gurage zone, Southern Nation Nationalities and Peoples Region (SNNPR), and is surrounded by the Meskan district. According to the 2007 Central Statistical Authority 16 (CSA) report, the total population was 33,406 of them; 16,923 were men and 16,483 were women. According to the 2009 Butajira Demographic Surveillance System (DSS) report, the number of women in the reproductive-age group was 11,133. 17 In terms of the distribution of health facilities, there are one public hospital and one health center in the town. Butajira was conveniently selected as the study area because the study was conducted during COVID-19 pandemic travel restrictions.
Study design and population
A community-based cross-sectional study design was conducted among LARC users to determine the discontinuation rate of LARC methods in Butajira town. All reproductive-age women (15–49) who inserted LARCs 1 year before the data collection time in Butajira town were the source population. Women who inserted LARC in each household were identified using the family folder list with the help of health extension workers. Those reproductive-age women who have been using LARCs from March 01, 2019, to March 01, 2020, were included in the study. Those who have been using LARC in town, but not currently living in Butajira town were excluded from the study.
Sample size determination and sampling procedure
To determine the sample size for this study, the outcome variable and various factors significantly associated with the outcome variable were considered. The sample size was calculated for each specific objective separately, and the largest sample size was taken to be used for this study. This way, the sample size calculated for the first objective is found to be larger and used for this study. The sample size was determined by using a single population proportion formula

With a 0.05 margin of error (d), a 95% confidence interval (CI), and a 16% proportion of early implant discontinuation (P) taken from a study done in Hawassa,
9
because there was no report on LARC discontinuation in Ethiopia. By adding a 10% non-response rate, final sample for this study was
Regarding the sampling procedure and sampling technique, all five Kebeles in Butajira town were included. A list of LARCs was taken from family planning registration books of the health center and hospital. For the sake of maintaining confidentiality and privacy, identification number was given in place of the name for each user. The identification number and address were used to select study participants. A systematic sampling method was used to select study participants until the sample size was enough for each kebele. With a total of LARC users in Butajira town where N = 667 and total sample size n = 227 an interval of k = 667/227 = 3, then every third woman was selected from the list. For women who were not at the home repeated visit was made and tried to decrease the non-response rate (Figure 1).

Conceptual framework for assessment of LARC discontinuation and associated factors among reproductive-age women in Butajira town; constructed from reviewed.
Operational definitions
Data collection tool and procedure
Data were collected using an interviewer-administered pretested questionnaire. The questionnaire was prepared from reviewed literature9,10 and modified accordingly to suit the study. The questionnaire was prepared first in English and translated to Amharic then translated back to English by official language translators to evaluate its consistency. The final version of the tool was edited; the Amharic version of the questionnaire was used for data collection. Five undergraduate Midwifery students and 2 BSc degree holder midwives and nurses were recruited as data collectors and supervisors, respectively. Women who inserted LARC in each household were identified using the family folder list with the help of health extension workers. The interview technique was used to collect data with a structured and pretested questionnaire.
Data quality control
To assure the quality of data, the questionnaire was pretested. It was done in Wolkite town Edgetber health center on March 10–11 before conducting the major study on about 5% of the sample to assess the clarity, sequence, consistency, understandability, and total time taken to complete the questionnaire. After pre-testing the questionnaire, revisions and amendments were made accordingly. Two days’ training was given for data collectors and supervisors on the overall study protocols including the objective of the study, methodology, data collection procedures, how to interview, recording of study subjects’ responses, and checking the questionnaire for completeness. The supervisors and principal investigators checked and revised the completeness of the questionnaire and offer necessary feedback to data collectors.
Data processing
The collected data were coded, cleaned, and entered into Epi-data version 4.6.2. Then, the analysis was made with Statistical Package for Social Science (SPSS) version 25. Missing values and outliers were checked by running frequencies for all variables and cross-checked with the raw data in the hardcopy of the questionnaire. Cross-tabulation was done to check whether the variables fulfill the assumptions of logistic regression. Variables with very few frequencies were merged and recoded.
Variables of the study
The dependent variable for this study was discontinuation rate LARC, which was measured as Yes/No. The independent variables include socio-demographic-related factors (age, religion, marital status, educational status of woman, educational status of husband, occupational status of women, occupational status of husband, family income), health system-related factors (health extension workers availability, time taken to reach to health institutions), reproductive-related factors (parity, number of living children, history of abortion, desire of pregnancy, time to get pregnancy) and method-related factors (information about LARC, history of family planning before LARC, type of contraceptive before LARC, responsible person for choosing LARC, counseling service, and satisfaction with the service; Figure 2).

Schematic presentation of the sampling procedure for discontinuation rate of long-acting reversible contraceptives and factors associated factors in Butajira town public health institutions, Central Ethiopia, 2020.
Statistical analysis
Descriptive analyses such as frequency, percentage (for categorical variables), mean, and SD (for continuous variables) were done. The results were presented using tables, graphs, and figures. Bivariable and multivariable logistic regression analyses were performed using ENTER method to show the relationship between dependent and independent study variables. Independent variables with a p value of ⩽0.20 in bivariate analysis were selected for a multivariable logistic regression model after checking for multi-collinearity using the variance inflated factor (VIF) and standard error. Association was described using an adjusted odds ratio along with 95% CI, and a p value < 0.05 was considered statistically significant.
Results
Socio-demographic characteristics
A total of two hundred twenty-two participants have responded to the questionnaire, making a response rate of 97.8%. The age of respondents was between 20–35+ years with a mean age of 28 ± 4.9 years. One hundred forty-three of the participants (64.4%) were Muslim by religion, 205 (92.3%) were married, and 83 (37.4%) women were housewives. Half of the respondents have a monthly income of 500–1000 Ethiopian Birr (ETB) with a mean of 740.50 ± 238.20 per month (Table 1).
Socio-demographic status of women who ever used long-acting reversible contraceptives in 2019/2020 in Butajira town, Central Ethiopia, 2020 (n = 222).

Health system-related characteristics
The majority of women had access to got health extension workers in their area 200 (90.1%) and 91 (41.0%) of women consumed less than 30 min to reach the health facilities (Table 2).
Health system–related characteristics of women who ever used long-acting reversible contraceptives in 2019/2020 in Butajira town, Central Ethiopia, 2020 (n = 222).

Reproductive history-related characteristics of women
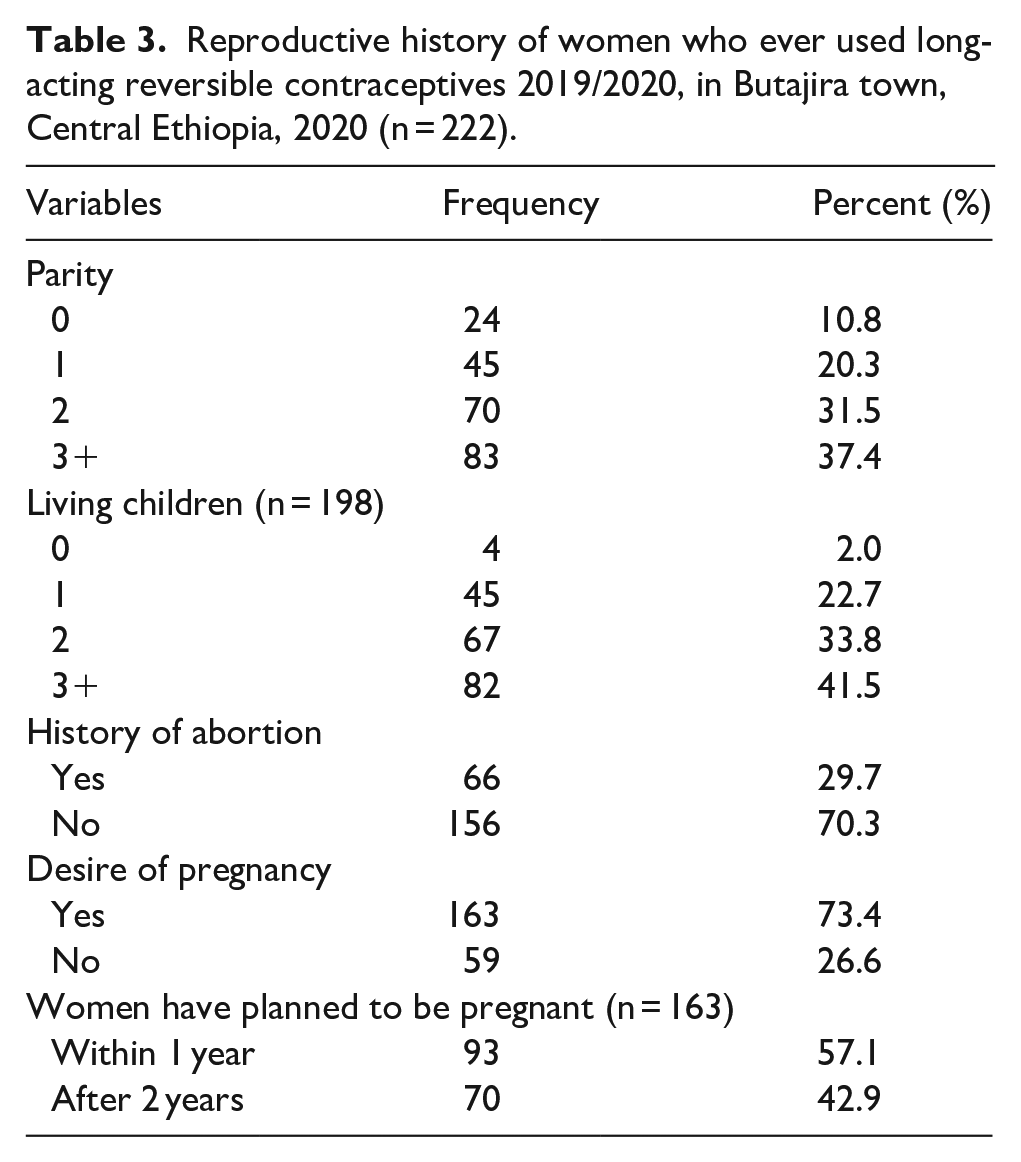
Reproductive history was one of the factors that were assessed in this study. More than half 115(51.8%) of the respondents had given birth one to two times. Out of those 112(56.5%), respondents had one to two alive children. Among total respondents, 66(29.7%) had a history of abortion, and 163(73.4%) desired to have more children (Table 3).
Reproductive history of women who ever used long-acting reversible contraceptives 2019/2020, in Butajira town, Central Ethiopia, 2020 (n = 222).
Contraceptive and counseling-related characteristics
More than half 131(59.0%) of respondents had information about LARCs before insertion. The LARCs had selected by women 130(58.6%) and the majority of 181(81.5%) women who have been using implants. One hundred forty-eight (66.7%) were counseled about the side effect of LARCs, and 145(65.3%) of respondents have been satisfied with the service given before insertion (Table 4).
Contraceptive and counseling-related characteristics of women who ever used long-acting reversible contraceptives in 2019/2020 in Butajira town, Central Ethiopia (n = 222).

HEW: health extension worker; IUCD: intrauterine contraceptive device; LARC: long-acting reversible contraceptive.
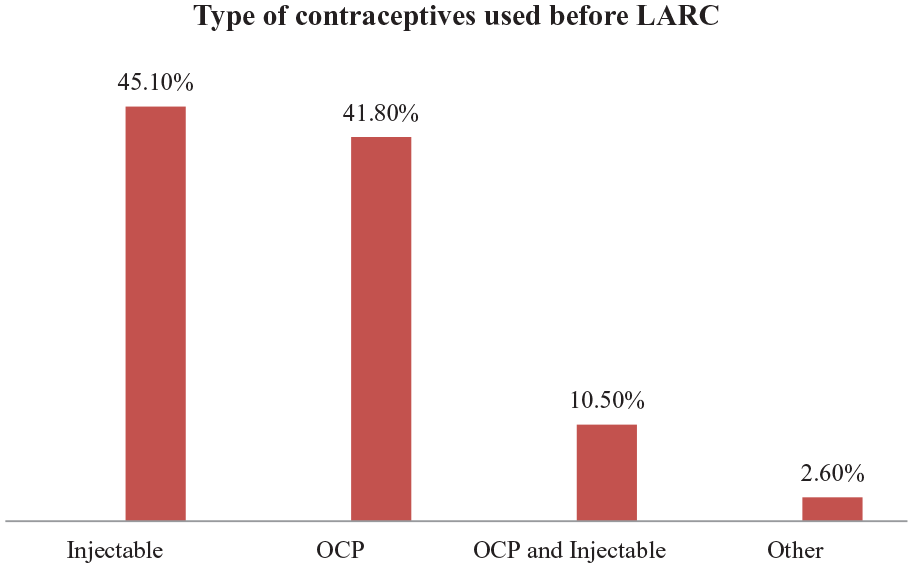
Type of contraceptives used before LARC
The majority of participants had used contraceptives before the insertion of LARCs, 68(45.1%) injectable followed by 63(41.8%) oral contraceptive pills (OCP; Figure 3).
Contraceptive history among women who ever used long-acting reversible in 2019/2020 in Butajira town, Central Ethiopia, 2020 (n = 151).
The magnitude of LARCs discontinuation rate
The result demonstrated that the discontinuation rate among 222 women who ever used LARCs within 1 year was 50(22.5%); 95% CI(17.8–27.2) and from these discontinuers, 39(78.0%), 7(14.0%), and 4(8.0%) discontinued Implanon, Jadelle, and IUD, respectively. Women discontinued LARCs between 3 and 12 months with a mean of 5.9 ± 3.02 months. The majority of the women removed LARCs 37(74%) over 3–6 months, followed by 13(26%) over 7–12 months (Figure 4).

Proportion of LARC discontinuation among LARC users in Butajira town 2020 Central Ethiopia (n = 222).
Reason for discontinuation of LARCs
Women discontinued LARC mainly due to facing side effects 26(52%) followed by the desire to have a child 11(22%) and 10(20%) health concerns. The most common complaints among women who faced side effects were menstrual disruption 19(73.1%), headache 6(23%), method inconveniency 4(15.4%), weight gain 2(7.7%), insertion site arm pain 2(7.7%), and abdominal pain 2(7.7%; Figure 5).

Reason for discontinuation among women who ever used long-acting reversible contraceptives 2020 in Butajira town, Central Ethiopia, 2020 (n = 50).
Factors associated with a discontinuation rate of LARCs
Socio-demographic-related characteristics, health system-related characteristics, reproductive-related characteristics, and family planning and counseling-related characteristics were included in the analysis to see the significant association with LARCs discontinuation rate. All variables were first tested in bivariable logistic regression analysis. Hence, independent variables with a p value ⩽ 0.20 were entered into multivariable logistic regression analysis. Multivariable logistic regression analysis showed that time consumed to reach the health institutions, desire to have more children, and counseled about the benefit of LARCs before insertion were found to have a statistically significant association with the discontinuation of LARCs. The result demonstrated that women who had consumed 60 min and more to reach the health facilities were six times more likely to discontinue LARCs compared to women who had consumed less than 30 min to reach the health facilities (AOR = 6.16 (95% CI: 1.46–25.97). Women who desire to have more children were five times more likely to discontinue LARCs as compared to women who have no desire to have more children (AOR = 5.30 (95% CI: 1.13–24.81). Women who were counseled about the benefit of LARCs are more likely to continue compared to women who were not counseled about the benefit of LARCs (AOR = 0.08(95% CI: 0.02–0.39; Table 5).
Factors associated with a discontinuation rate of long-acting reversible contraceptives in Butajira town in 2019/2020, Central Ethiopia, 2020 (n = 222).

Statistically significant at p value < 0.05.
Discussion
The study found that the discontinuation rate was 22.5% with a mean of 5.9 ± 3.0 months. This finding is higher than the study done in the United States, Pakistan, Vietnam, and Hawassa9,11,19,20 but lower than the study done in Nepal, South Africa, Nigeria, and Ambo.12,21–23 This discrepancy may be due to differences in study design, sample size, and duration of the study. Moreover, it may be due to the present study included all types of LARCs (Implanol, Jadelle, and IUD), but other studies included only one type of LARC. In addition, it might be due to the study setting as this study was only done in the urban area whereas other studies were done in either rural or urban or both. Finally, it may be due to the educational status of women as in this study majority of women had no formal education whereas in other studies majority of participants were above primary.
This study found that majority of women were younger in parallel with a study done in Hawassa, South Africa, and Pakistan.9,20,21 This may be because it does not require frequent visits to health institutions until they need to remove it and keep privacy. Young women may have intended to have children, and as a result, high discontinuation rate of LARCs.
The study revealed that the main reason for discontinuation of LARCs was facing side effects, desire to conceive, and health concerns in line with the study in Australia, Vietnam, India, and South Africa.11,21,24,25 Menstrual disruption was the main side effect faced among discontinuers. Menstrual irregularity may not cause serious health problems but interferes with daily activity especially sexual activity with their husband. Discontinuation due to side effects was a result of inadequate counseling and information on possible side effects before insertion of long-acting contraceptives. Giving adequate counseling and information on possible side effects could ensure the continuation of LARCs.
From independent factors time consumed to reach health institutions,’ desire for having more children, and pre-insertion counseling were predictors for discontinuation of long-acting reversible. The odds of time consumed 60 min and more to reach health facilities was six times more likely to discontinue long-acting contraceptives compared to women who have consumed less than 30 min to reach the health facilities which is consistent with studies in Pakistan. 20 This is related to the fact that being unable to get to the health facility nearby and traveling long distances make difficult repeated visits. This may result in the discontinuation of LARCs. In addition in the present study, 46% of discontinuers consumed >60 min to reach the health facility. Those women who have the desire to have more children were five times more likely to discontinue LARCs when compared to those who have no desire to have more children which is inconsistent with a study in Debre Tabor town. 18 This might be the difference in the denominator. In the present study, the denominator was all LARCs but in a study in Debre Tabor, the denominator was all women who request the removal of long-acting contraceptives. Moreover, it may be due to differences in the educational attainment of respondents. In the present study, most of the participants had no formal education compared to the study participants in Debre Tabor, most of the respondents were above primary. Finally, it might be due to the socio-cultural differences of participants across the study area.
The present study showed that women counseled about the benefit of the LARCs were less likely to discontinue LARCs compared to women who were not counseled about the benefit of long-acting contraceptive methods which is inconsistent with the study done in Hawassa, Dale district of south Ethiopia and Debre Tabor.9,10,18 In other studies, pre-insertion counseling about the benefit of LARCs did not associate with the discontinuation of LARCs. This discrepancy might be due to socio-cultural differences. Pre-insertion counseling about the benefit of LARCs helps for ensuring continuation rate by tolerating side effects.
Family planning service providers should inform clients about available methods, individual screening of a client’s needs, and support a client’s selection of methods of their choice. Providing quality family planning counseling services is vital for maximizing service utilization. Quality family planning counseling requires that providers offer impartial advice on a broad mix of methods, by sharing details on side effects and the effectiveness of methods. Realizing quality family planning counseling can improve utilization, improve client satisfaction, and influence the likelihood of discontinuation or switching to another method. 26 In addition, should counseling services for those clients who came to clinics to remove LARCs.
The study assessed the discontinuation of LARCs, a current public health concern that may lead to a program failure. In addition, this community-based study fills the gap of other institution-based studies. The findings of this study should be considered with regard to the following limitations. Since the data on dependent and independent variables were collected at the same point in time, no causal interpretation can be made of the relationships between variables. The result of this is not generalizable where the place of residence is rural. The study may have social desirability biases and recall bias of respondents.
Conclusions and Recommendations
The study concluded that LARC discontinuation is high (22.5%) when compared to Ethiopian Demographic Health Survey (EDHS) 2016. The main reasons for discontinuation of LARCs were facing side effects, desire to conceive, and health concerns. Time taken to reach health institutions, desire for pregnancy, and being counseled about the benefit of long-acting contraceptives were predictors of discontinuation of LARCs. Routine quality pre-insertion counseling about the benefits and side effects of LARCs by family planning service providers is highly recommended. In addition, we recommend further trials using larger sample sizes on predictors of discontinuation of LARCs.
Supplemental Material
sj-docx-1-whe-10.1177_17455057221104656 – Supplemental material for Discontinuation rate of long-acting reversible contraceptives and associated factors among reproductive-age women in Butajira town, Central Ethiopia
Supplemental material, sj-docx-1-whe-10.1177_17455057221104656 for Discontinuation rate of long-acting reversible contraceptives and associated factors among reproductive-age women in Butajira town, Central Ethiopia by Haregwa Asnake Weldekidan, Semarya Berhe Lemlem, Workinesh Sinishaw Abebe and Seboka Abebe Sori in Women’s Health
Footnotes
Acknowledgements
The authors would like to acknowledge Addis Ababa University, College of Health and Medical Sciences for its financial support for data collection through its Post-Graduate Student Grant Scheme. They also want to thank the study participants, data collectors, supervisors, health institutions administrate, data clerks, and all others who directly or indirectly contributed to this work for their kind cooperation and invaluable collaboration.
Author contribution(s)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical clearance was obtained from the Institutional Review Board of School of Nursing and Midwifery, College of Health Sciences, Addis Ababa University (IRB: CHS/MIB/112). After the permission letter is obtained from the school of graduate office, the letter was submitted to the Gurage zone health bureau. An official letter of cooperation was obtained from the Gurage zone health bureau and was presented to the heads of the hospital and health center. Participants were informed clearly about the purpose and benefits of the study. The respondents were told that they have the right not to participate in the study or withdraw from the study at any time or stage of the interview. Written informed consent was obtained from the participants. Only those who signed written consent participated in the study. The confidentiality of respondents was maintained throughout the research process.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A small grant for data collection was obtained through grants offered by the Addis Ababa University Postgraduate Office (grant no: 278/20).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.