
Abstract
Background:
High fertility and rapid population growth can threaten human development and increase risks to maternal and child health. The diffusion of the benefits of lower fertility requires readiness to plan, and willingness and ability to adopt and use family planning measures.
Objective:
This assessment aimed to explore the readiness, willingness, and ability (RWA) among selected Ethiopian communities, and identify the facilitators and impediments of fertility transition.
Design:
This exploratory phenomenological qualitative study collects data from purposefully selected community members and experts in Addis Ababa, Arbaminch, and Jigjiga.
Method:
The analysis follows deductive coding and a thematic presentation of findings under the RWA domains. Readiness deals with four themes: (1) the rationalization of the value of children, (2) recognition of the burden of high-risk fertility, (3) readiness to define the ideal number of children, and (4) socio-cultural norms about family size. Willingness contains three themes: (1) the psychosocial legitimacy of contraceptives, (2) the religious legitimacy of contraceptives, and (3) women’s power to cope with barriers to family planning. The ability domain contains (1) women’s knowledge about contraception and (2) access to and utilization of contraceptives.
Results:
The communities involved in this study recognized the burden of high-risk fertility behaviors (early-age fertility, and frequent and many births), but they prefer large family sizes. Consequently, they exhibit good family planning willingness and practice for birth spacing but not for birth limitation. Recognizing the socio-economic burden of high-risk fertility, accepting and using contraceptives for the health of mothers and children are possible facilitators of fertility transition. Conversely, the desire for high parity, husbands and religious disapproval of contraceptives, side effects of contraceptives, and limited access to method mix are possible impediments.
Conclusion:
The RWA to space births are adequately diffused and adopted by the community, but birth limitation is not yet recognized. Beyond promoting birth spacing, Ethiopia’s fertility transition requires a shift in societal values from large to small family size. Overcoming barriers to contraceptive use also requires tailored efforts to improve the availability of method mix and involve male and religious leaders.
Introduction
High fertility and rapid population growth delay human development, pose health risks for children and their mothers, and worsen environmental threats. 1 Fertility decline mainly occurs because of delayed initiation of childbearing, prolonged birth intervals, and early termination of childbearing. 2 In 2019, the global lifetime fertility rate reached 2.5 per woman, ranging from as low as 1.7 live births in Europe and North America to as high as 4.6 in Sub-Saharan Africa (SSA). 3 Studies on fertility transition in SSA, including Ethiopia, have shown that fertility decline started late, progress has been slow, and there are significant urban–rural, regional, and socio-economic differences.4 –6 Through direct and indirect efforts, Ethiopia’s total fertility rate has decreased from nearly 8–4 live births per woman over the last three decades. 7 While some quantitative surveys have examined fertility rates,8 –14 little is known about how the community perceives, adopts, and practices fertility decline. This study aims to address this gap by exploring how communities conceptualize, accept, and implement fertility decline.
Theoretical background
In the mid-1980s, the Princeton European Fertility Project and the World Fertility Survey revealed that structural and economic changes alone could not fully explain the fertility transition in Europe.15,16 This led researchers to consider the role of diffusion theory. Diffusion theory highlights the spread of new attitudes and behaviors related to family planning, shaping individuals’ values, and practices regarding childbearing. 15 Fertility decline is seen as a result of the adoption of new attitudes and behaviors related to family planning, which spread from innovators to adaptors through a diffusion process. 15 This process includes ideational innovation (acquisition of values, knowledge, and attitudes) and behavioral innovation (use of contraceptive techniques). Social capital, such as access to education, media, income, and health services facilitates the diffusion process.17,18
Assessing the components and effects of social dynamics and social capital is a complex task. The readiness, willingness, and ability (RWA) model developed by Coale 19 and tested by Lesthaeghe and Vanderhoef 20 framed the diffusion process with structural determinants of fertility. Readiness involves the cost–benefit analysis of family planning, willingness refers to the acceptance of new ideas and measures for family planning, and ability refers to the voluntary use of contraceptives.20,21 This framework has been used to study the impediments to fertility transition in the United States (Hacker 22 and contraceptive use patterns in Europe, 23 and various countries24 –26). Following this diffusion framework, this study aims to apply the RWA framework to assess community RWA and identify facilitators and barriers to fertility transition in Ethiopia.
Methods
Study design and setting
This exploratory phenomenological qualitative study collects primary data from three areas (Addis Ababa, Arbaminch, and Jigjiga) purposively selected to represent societies with different socio-economic contexts and levels of fertility. Addis Ababa, the capital city of Ethiopia, is a metropolitan city known for having the lowest fertility rates in the country. Arbaminch City in the Southern Central Ethiopia Regional State represents populations with both urban and rural livelihoods with moderate fertility rates. Jigjiga, the capital city of Somalia regional state, is known for having the highest fertility rate in Ethiopia. Addis Ababa has a multi-ethnic and multi-religion population, while the latter two have some dominant groups (the majority of residents in Arbaminch are Christians, while those in Jigjiga are Muslims). 7 Community participants from Addis Ababa and Jigjiga are urban residents, while those from Arbaminch come from urban and rural settings. In each of the three regions, districts and kebeles (lowest administrative unit) were randomly selected. Urban kebeles from Addis Ababa and Jigjiga cities and semi-urban and rural kebeles from Arbaminch City were selected. Under the guidance of data collectors, participants who fulfilled the criteria were identified by community health workers.
Sample size and sampling
This assessment collects data from 27 female and male community members and 15 key informants. We purposefully select women and men with high and low parities. High parity is considered if participants have eight or more children at any age or four or more children before they reach the age of 30. On the other hand, low parity is considered if they have three or fewer children for those aged less than 30 years, or five or fewer children for those aged 50 or more years. Then the community health workers selected one kebele (the lowest for the formal administrative unit) from each district. Participants who fulfilled the criteria were identified by community workers. Moreover, both Muslim and Christian religious leaders were also interviewed. Key informants were selected based on their work relevance to population or family planning aspects by discussing with the head of select sector offices. The detailed background characteristics of participants are annexed in Table 1.
(a) Background profile of in-depth interview participants in Addis Ababa, Arbaminch, and Jigjiga-Ethiopia (December 2023).

Data collection methods
This study collects data from November to December 2023 using in-depth interviews (IDI) and key informant interviews (KII). Three data collectors, who are not residents of the data collection area, were recruited and trained on data collection tools and interview techniques. Three different semi-structured discussion guides were prepared to interview experts, community members, and religious leaders (Supplemental Material 1). The guide for IDI was pretested among four women and the feedback from the pretest was used to identify appropriate words for asking sensitive issues. All interviews were audio recorded and transcribed. Data saturation was determined by the lack of newly emerging concepts from recruiting additional participants. The principal investigator conducted KII and checked the quality of the transcriptions and data saturation. We also received feedback from three key informants and ensured whether the transcripts reflected their views.
Data coding and analysis
A deductive coding following the RWA framework is conducted using NVivo version 14 (QSR International coppy right 1999-2022). Final codes were organized into themes and categories and reports were generated in a Word document. The analysis follows a thematic presentation of the concepts, codes, and categories under each of the RWA domains. Readiness deals with four themes: (1) the rationalization of the value of children, (2) recognition of the burden of high-risk fertility, (3) readiness to define the ideal number of children, and (4) socio-cultural norms about family size. The community willingness also contains three themes: (1) the psychosocial legitimacy of contraceptives, (2) the religious legitimacy of contraceptives, and (3) women’s power to cope with barriers to family planning. Finally, the ability domain is schematized into (1) women’s access to information and knowledge about contraception and (2) access to and utilization of contraceptives. Trustworthiness is maintained by training data collectors, close supervision of the fieldwork, member checking by key informants, and keeping a record of all processes. The reliability of the findings is maintained by ensuring the credibility of the data collection process, systematic approach to data analysis, and triangulation of findings by source and setting. Moreover, findings are interpreted by reiterating reports of national surveys and programmatic policy documents. The principal investigator who writes this manuscript is a reproductive health professional who believes in the reproductive rights of individuals and couples while recognizing the public health and developmental impacts of having voluntary, right-based family planning. The manuscript was organized using the Standards for Reporting Qualitative Research (SRQR; Supplemental Material 2). 27
Results
Community readiness to adapt to the ideation of low fertility
Theme 1: Readiness to rationalize the value of children
The first theme of readiness presents participants’ values for children coded into economic, psychosocial, or religious perspectives.
Children as the gift of God: “Children are the gift of God” is the first word-of-mouth for the majority of participants. Participants view children as a sign of blessing from God.
I love children too much. A child is the most expensive gift from God. You can work and get money, but you cannot make a child unless God gives you. A child is a wealth and a gift of God. (32-year-old, female Jigjiga)
Psychosocial value of children: For most participants, children are viewed as a source of love, courage, and social respect. They perceive that the psychological satisfaction they get from children is more than any material value. For some people, having many children in the current economic crisis is considered a pride rather than a challenge. Mothers considered such love and affection from children superior to the economic challenges they face. A woman from Addis Ababa stated that: To be honest, I have approached many individuals for loans to meet the daily needs of my children and have been preoccupied with repaying those loans. However, when I see my children thriving, I feel an overwhelming happiness, even in difficult times. When I feel down, a simple touch from my child gives me joy. My children kiss me and tell me, “My mother, we will be rich,” which makes me happy. My kids are my resource. I consider myself fortunate. (30-years-old female, Addis Ababa)
A religious leader also describes that children in Ethiopia are viewed as a means of insurance, social privilege, and religious blessings: When the family grows older, the child takes the responsibility of supporting the entire family, including family rituals and ceremonies. Hence, we can conclude that children are seen as both a resource and a source of joy, a precious gift from God. (Male, religious leader, Addis Ababa)
Economic value of children: The economic value of children is described in terms of source of income, labor for agricultural activities, and viewed as insurance when parents get old. Participants from rural areas value a large number of children to get adequate labor for agricultural activities: A man said: Now I’m in front of God, who gave me many children. I am the beneficiary; my children are helping me with many agricultural activities like carrying coffee plants, and other home-based activities. (40 years old male, Arbaminch)
In urban areas, the economic value of children is viewed in terms of returning investment from education or from economic remittances from those who migrated. The large number of children is also linked with better cumulative benefits, especially during holidays and ceremonies. Due to the uncertainties on the quality and commitment of children, some participants also perceived that having a large number of children would increase the probability of becoming a hard worker and responsible. Participants also believe that every child comes with their endowments and is likely to support the family and the country: In the beginning, I told you that children are love and wealth for the family. For me, all seven children will bring wealth. I believe and see in my life that my economic status has been improving as I give birth to more children. As they grow, children also benefit a country and all people including you. (32-year-old female, Jigjiga)
Theme 2: Recognition of consequences of high-risk fertility
This theme discussed the socio-economic burden of high-risk fertility (early, frequent, and multiple births). Both men and women recognize that teenage pregnancy exposes women to induced abortion, and makes their labor difficult, leading to bleeding, episiotomy, fistula, operation, uterine rupture, and death. Young mothers are also said to be economically poor, dependent on their husbands, unskilled in managing their family and caring for their children, and more likely to face divorce. The following personal story is said to be common for many women in Jigjiga: When I was 14 years old, my family forced me to get married and have kids. My father chose the person I married. Consequently, my labor was tough, and the doctor told me that my uterus was not developed and could not handle the fetus, for which I had to spend much time in the hospital. My children and I faced several challenges. Since I was a little child, and I gave many successive births, I was not able to give my children what they want. (27-year-old female, Jigjiga)
Participants also recognize the economic burden and the medical and social consequences of close birth intervals. Childhood problems such as diminished balanced diet, stunting and retardation, repeated illnesses, and denial of love and care are raised. Blood loss, miscarriage, fistula, not being well prepared for the next pregnancy, workload, tiredness, poor self-care, looking older for her age, and divorce were also raised as maternal complications of frequent childbirth. A young mother stated that: Now, I am a nursing mother. If I do not take contraceptives, I may get pregnant before the first birthday of my child; almost double children. Then the child may grow improperly, may not get food on time, and not be washed properly. The mother also gets problems; when she frequently delivers, her womb could be damaged. If the mother is not healthy, the child may get problems. (27-year-old female, Arbaminch)
However, some participants attribute the burden of early age and frequent birth to poverty and lack of adequate care during maternity. A woman stated that: I recommend women to have a baby early before their age reaches the postmenopausal period. . . . If there are vegetables from the yard and animal products like eggs or milk, there will not be a problem for the child even when she gives birth frequently. (37-year-old female, Arbaminch)
Despite their desire for high fertility, women, especially in Addis Ababa, recognized that the current living standards and childbearing are expensive and demanding. An older woman describes this by comparing the previous and current challenges of childbearing.
Nobody finds it unpleasant to have several families; everyone wants many children. However, the current generation requires more resources. Today, having four children is sufficient because the cost of raising a child, including expenses for milk, diapers, and education, has become very expensive. (60-year-old female, Addis Ababa)
Theme 3: Readiness to define the ideal number of children
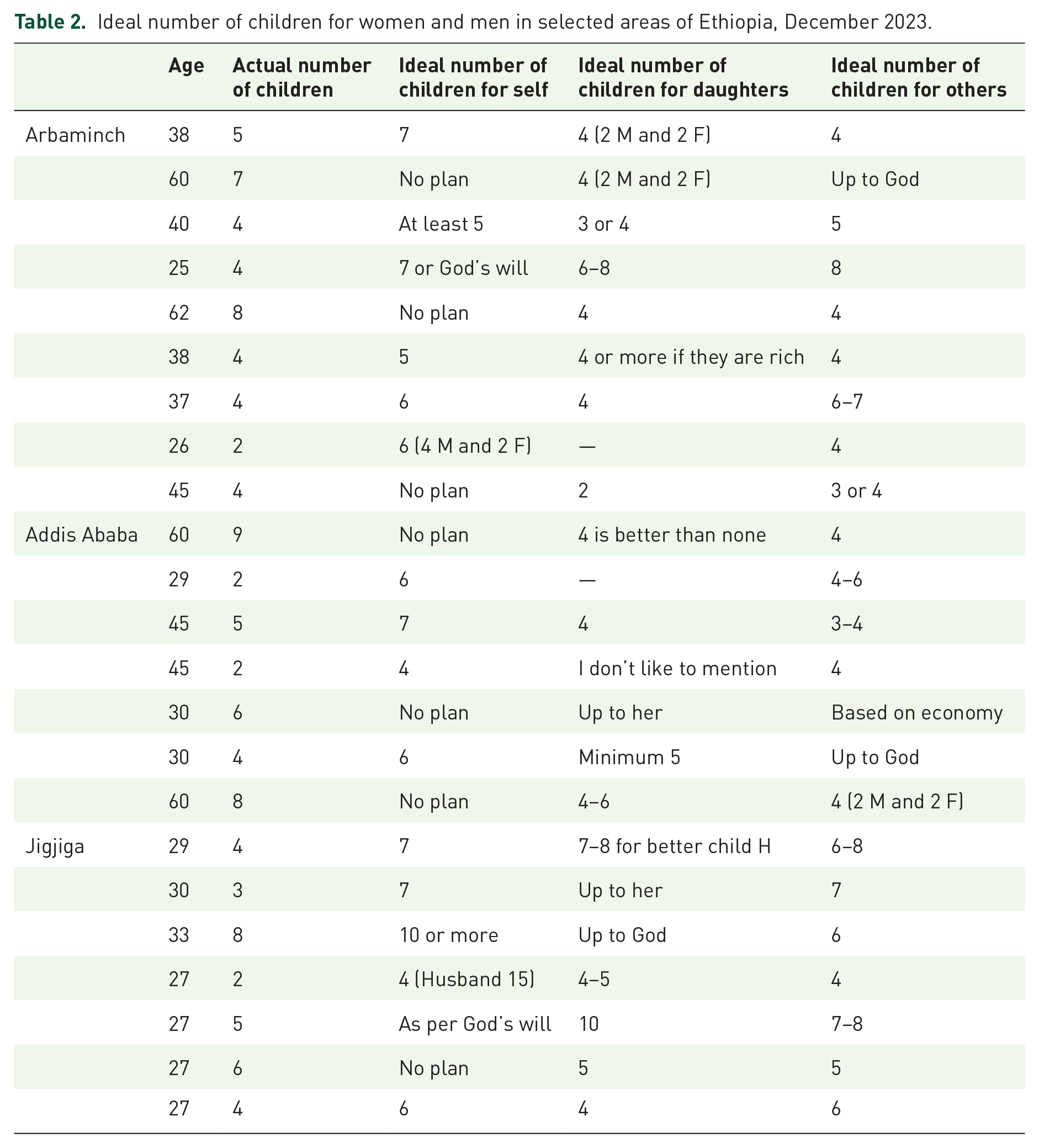
This theme deals with participants’ ideal number of children and their desire to limit fertility. The fourth theme captures socio-cultural norms favoring high fertility. Community participants mentioned the ideal number of children for themselves, their daughters, and others. For some participants, however, it is not even normative to comment on the ideal number of children. According to the data collectors’ reflection, many participants were not interested in responding to a question on their ideal number of children; some of them reacted with negative emotion, while others kept silent despite probing. Those who numerate their parity size also desire a high parity: I heard a proverb that “a man with one eye won't be able to play with soil.” My goal was to have twelve children, but right now, it is difficult to reach that goal. For my daughter, I wish to have up to five children because the time may not be good for her. (27-year-old female, Addis Ababa)
As shown in Table 2, many participants mentioned a smaller number of children for their daughters than for themselves, wishing lower parity for the next generation. However, the overall ideal fertility is high, ranging from 4 up to 10 or unspecified. Among women who numerate their desire with uncertainty, four is the minimum stated number. A 32 years old woman from Jigjiga said that: Thanks to God, I have seen what giving birth is because I have two children now. I will accept what God gives me, but I want four children—two females and two males. I believe that I will bear these two children and add another two. Then I will work for their future lives because I do not think having many children will benefit me.
Ideal number of children for women and men in selected areas of Ethiopia, December 2023.
Theme 4: Socio-cultural norms about family size
Socio-cultural norms in Ethiopia favor high fertility and extended family trees. Privilege for large families, religious and husband influences, cultural views of girls’ marriage, polygamy, and son preference are the main socio-cultural factors affecting fertility behaviors.
Having a large family is seen as a privilege: In all three study sites, families with a large number of children are perceived to receive better cumulative support and social respect. Children are expected to handle social and parental responsibilities during all rituals, whether good or bad. According to one respondent, small-sized households were stigmatized when hosting religious and cultural gatherings such as the commemoration of the finding of the True Cross (“Demera”). The desire for a large family is also derived from the social preference of a male-dominant family and clan. Participants from the Arbaminch area justified their preference for accomplishing laborious social and economic responsibilities and inheriting rural agricultural resources. Culturally, a man with a higher number of male children receives better respect from his social network, making him proud of his numerous sons. The pride and respect come not only from the psychological and economic roles of the sons but also from the contribution of the male population to his clan. Living in a pastoralist community exacerbates this gender and cultural value for more children. An expert described that: Pastoralist communities still face scarcity of water and grazing for their animals; they migrate from place to place and fight with other clans. Therefore, contributing many male children to the clan is considered a privilege and a responsibility because those males are critically needed to manage the movement from place to place and the fighting for resources. (Male government population officer, Jigjiga)
Husbands’ influence: The husband and his family’s desire for more children can also influence women’s value for children. Such influences vary across communities. It is common in Jigjiga but less so in Addis Ababa and Arbaminch. A man in Addis Ababa stated that: I am the one who wants more children. In my original place, I am the one from our clan and I inherited agricultural land from 4 households’. Then, I want children who can construct their house in each agricultural land. However, if she couldn’t give birth, I can’t force her. (45 years old male, Adds Ababa)
In Jigjiga, the husband and his parents not only have a higher desire for children, but they are also the decision-makers regarding fertility behaviors. Husbands’ family members insist that a woman give birth to many children; otherwise, they may suggest divorce. A woman from Jigjiga stated: If a woman doesn’t give birth to many children, there is influence from her husband, who is also influenced by his relatives. His relatives tell him, “Why limit the children? We need to see many family members and be happy with that. If your wife can’t give birth to many children, you should marry another woman.” This is because children are seen as the root of their fathers’ families. (29-year-old female, Jigjiga)
Polygamy: Participants mentioned that polygamy is practiced in their community for various reasons. Culturally, polygamy is a means to achieve men’s dreams of having more sons and contributing to their clan. To meet men’s desire for a high number of male children, women in polygamous marriages compete to give birth to more children and gain recognition from the husband and his family. Moreover, marrying more wives increases the total number and the chance of having more sons. A religious leader also justified this practice as a means to ensure women’s well-being, including childbirth, and as a solution for potentially replacing men who lost their lives due to war. From an economic perspective, having more than one wife from different places executes and preserves agricultural assets: In our culture, it is common for a person to have two wives and about 6-7 children from each wife. For instance, I live in Addis Ababa while I have agricultural land in a rural area. To have children who can maintain that land and inherit it, I also get married there. (45-year-old male, Addis Ababa)
Religion: From a religious perspective, having many children is seen as a sign of blessings from God. For Muslim participants, specifying a specific number of children and relating their value to socio-economic conditions is considered depravity against divine law. Religious leaders also disagree with the idea of specifying or planning fertility rates for economic reasons; instead, they endorse spacing for child health. A religious leader also stated: I belief that God has created us to procreate and that there is no religious doctrine prohibiting reproduction out of concern for meeting basic needs such as shelter and food. The idea is that if we work hard, God will grant us good health, physical appearance, and land to cultivate. In the Muslim religion, it is preached that even if one has very little, they should get married early as it paves the way for having children. (Male religious leader, Addis Ababa)
Aspiration for girls’ marriage: Despite the understanding of the consequences of early marriage presented below, some participants view early marriage and childbearing as advantageous in the presence of adequate care and nutrition. Some believe that marriage is a mandatory part of female life, and families tend to marry off their girls when they get the opportunity. A woman from Jigjiga states that “the community still supports early marriage by using proverbs such as ‘a woman is either for her marriage or for her tomb’ (ሴት ልጅ ወደ ትዳርዋ ወይም ወደ መቃብሯ).” Religious leaders also question the appropriateness of the specified legal age for first marriage (18 years) for the current generation, claiming that it exposes youth to premarital sex before this age. A man complained: “There is a family law prohibiting marriage before the age of 18, but who is concerned about the women who have experienced premarital sexual assault before the age of 14?”
Community willingness to accept contraceptives
Theme 1: Psychosocial legitimacy of contraceptives
Both women and men have favorable attitudes and are eager to discuss the role of contraceptive methods in ensuring better childcare, development, and women’s well-being. They are also committed to recommending contraceptives to others and spreading messages about the benefits of contraception. Despite fears of side effects and religious objections, there is no socio-cultural taboo or resistance to contraceptive practices. Figure 1 summarizes the communities’ word-of-mouth regarding the benefits of contraceptives.

Maternal and child health benefits of women recognized by women and men participants in Ethiopia, December 2023.
According to key informants, there is a disparity in the acceptance of family planning services between agrarian and pastoralist communities. It is well accepted among agrarian communities, while resistance exists in pastoralist communities. A senior population expert stated, “During the early extensions of family planning, I observed an unexpectedly high desire for contraceptives among farmers.” Local people were accepting modern contraceptives by saying, “The bed produces kids while the farm fears crops (‘መደቡ ልጆች አፈራ፣ መሬቱ እህል ፈራ’).” In pastoralist areas, the desire for a high number of sons, religious beliefs, and husband influence impede the ideation and behavioral adaptation of contraceptives. Husbands and their relatives desire large families and oppose modern contraceptives. The influence of husbands is not always negative; participants also report the presence of cooperative husbands, especially in overcoming religious fears about using contraceptives. Perceived and actual side effects are also intensively expressed as a psychological cost of contraceptive adaptation. Experts also share the idea that women are complaining about family planning providers. A health extension worker shares her experience: The community is complaining to us, saying “The government makes us infertile; we become infertile because of you’ They accept the idea of family planning, but they are not comfortable with all contraceptive methods due to side effects like bleeding, delayed fertility, husbands’ disapproval, discomfort during sex, etc.” (Health extension worker, Addis Ababa)
Theme 2: Religious legitimacy of contraceptives
Findings regarding the religious legitimacy of contraceptives have three perspectives. First, Christians are in favor of contraceptive use and indicate that there is no clear doctrine prohibiting it. Second, some Muslim women and leaders approve contraceptive use only for the health of the mother and children. The third perspective, which again arises from Muslims, is total avoidance of modern contraceptives for any reason and natural contraceptives for economic reasons. Family planning for economic reasons and inserting foreign matter into the body to achieve this is considered a sin or “haram” by the Muslim participants. Acknowledging the economic rationale of birth limitation as a religious offense, some participants also raised that there are no clear religious orders about the use of contraceptives: For me as a Muslim, it is quite challenging to use contraception because it is strictly forbidden to use contraceptives as it is considered as ending life. However, some individuals ignore these teachings and make their own choices. The issue is very complicated because whether family planning methods should be used or not is not explicitly stated by religious leaders. (29-year-old female, Addis Ababa)
A population expert also witnessed that religion is still a barrier for women not seeking contraceptive services. He noted that it is the husband, not the woman, who can discuss contraceptive issues with religious leaders: If the husband limits childbirth by saying, “I have no adequate income to feed my children,” the religious leader declares it as “Haram,” because it is believed that children belong to Allah and Allah would feed them. However, if it is considered for the health of children or mothers by spacing births, the religious leader may not say anything. (Male, government population expert, Jigjiga)
On the contrary, some participants disregard the effect of religion and use or promote contraceptive use. Population experts also believe that religious institutions and leaders are either neutral or supportive of the advocacy of contraceptives: Religious leaders have no problem with family planning; they advise us to do our work silently. On the ground, I realized priests were teaching about family planning. I saw a Muslim leader providing contraceptives in a remote area (name anonymous). So, there is no problem from the society or the religious aspect. (Female, government population expert, Addis Ababa)
Theme 3: Women’s power to cope with barriers to contraceptives
Women in the Addis Ababa and Arbaminch areas are less likely to face barriers and more likely to cope with any challenges. On the contrary, women in Jigjiga are more likely to face contraceptive prohibitions but less likely to cope with those challenges. Women who are unable to convince their husbands to use contraception do so secretly. The influence of the husbands’ relatives is also another obstacle. Women from Jigjiga and Arbaminch share their experiences of coping with these challenges: I pass through lots of challenges, especially from my husband’s family. When I spaced for my second birth, they were nagging me, saying, “Why don’t you give birth?”. . . It is because I am educated that I can convince them and cope with the challenge. If uneducated women face the same problem, she will be forced to conceive soon or divorce from her husband. (32-year-old female, Jigjiga) I take contraceptives hiding from my husband and his relatives. (25-year-old female, Arbaminch)
Women’s ability to use contraceptive methods
Theme 1: Access to information and knowledge about contraceptive services
Participants listed various contraceptive methods. Injectable and Implanon were commonly mentioned options across the three geographic areas, with women in Jigjiga also mentioning breastfeeding. The main message participants heard was about spacing childbirth through contraceptive use. They also knew that they could obtain contraceptives for free at public health institutions and with payment at private facilities. Mass media and social media were rarely mentioned as sources of information. Information provided by health professionals during mothers’ visits to health facilities and education by community health workers were the primary sources of information about contraceptives: There is a health extension worker in our area who always teaches us to plan our families. She provides education about family planning in the development groups and one-to-five networks. (40-year-old female, Arbaminch)
Theme 2: Access and utilization of contraceptive methods
Access to family planning information and contraceptive services was almost universal. Women reported that they could easily access contraceptive services from health extension workers or during their visits to nearby health facilities. The availability of methods in nearby health facilities, education by health extension workers, and counseling by service providers contributed to women’s uptake of contraceptives: I am using an implant in my left hand after my second birth. Nobody forces me to use it, but it is for the health of my children and to ensure they receive the love they deserve from their mother. I want to space my children by 2 to 3 years so they can have their own time, and it also gives me time. (27-year-old female, Jigjiga)
Fear of side effects, religious concerns, husbands’ disapproval, not getting the preferred method, and frequent closure of health posts were the main impediments to using modern contraceptive methods. These challenges varied geographically. Fear of actual and perceived side effects was mentioned across the three study areas. While religion, husband influence, and lack of awareness were common barriers in Jigjiga town, shortages of contraceptives and side effects were commonly mentioned barriers in Arbaminch. Among women ready to plan their fertility, fear of side effects was the main barrier to contraceptive uptake. Delaying fertility, weight gain, abnormal bleeding, and dizziness were the most reported side effects. Despite women’s concerns about side effects, many interviewed experts and service providers considered them to be perceived rather than actual problems. Both men and women also complained about health professionals refusing to remove contraceptives. Some women continued with their contraceptives despite side effects, while others discontinued use: There is an implant that lasts for three years. We heard some women who use this contraceptive complain about side effects like dizziness, blood loss, and hunger. When health professionals refused to remove the implant, some women tried to remove it themselves using local materials like knives or other methods. I have seen people like this in our area. (40-year-old female, Arbaminch)
While experts noted a shortage of supplies for long-acting contraceptives, the inability to receive an “injection” was the most common complaint among community members. This led to unplanned pregnancies, the use of non-preferred methods, or purchasing from private pharmacies. One woman stated: There is my friend who uses a three-month injectable, but she comes back without being injected because there is no one available at the facility. The health extension worker said contraceptives are out of stock. Those with money buy the injection from private pharmacies, but those without may end up pregnant. (40-year-old female, Arbaminch)
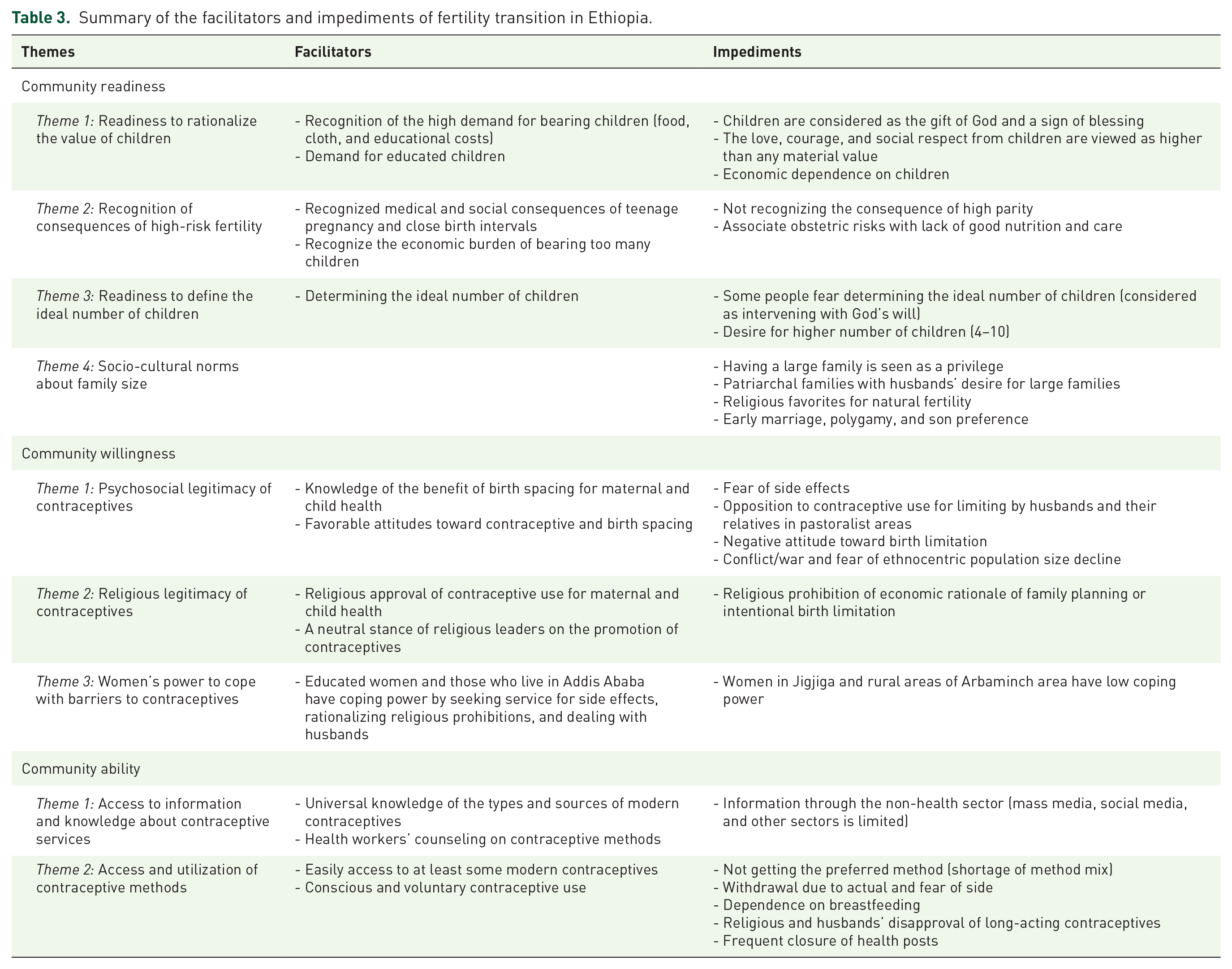
The findings presented above reflect the community’s RWA to adopt the ideation, technologies, and practices of family planning. In each domain of fertility transition, there are developments and drawbacks reflected by both the community and religious leaders. To better understand the facilitators and barriers of fertility transition, the main concepts under each theme are summarized under the RWA framework (Table 3).
Summary of the facilitators and impediments of fertility transition in Ethiopia.
Discussions
By exploring the lived experiences of women, men, and expert opinions, this qualitative study revealed the community’s RWA regarding family planning. It also identified the facilitators and impediments to women’s adoption of family planning. The findings showed strong community readiness, willingness, and actual measures for delaying and spacing childbirth. However, the ideation and practice of fertility limitation are not widely accepted.
According to the RWA model of fertility transition, the first step is for parents to consciously calculate the cost–benefit of the number of children and understand the benefits of planned and lower fertility. 20 This study found that communities view children as a blessing from God, a source of love, joy, pride, labor, and a means of economic gain. These values are similar to those in other societies28 –31 and in line with the child value theories. 32 An important development in community readiness is that women and men are capable of recognizing the well-known health, economic, and social burdens of early age, frequent, and multiple childbearing. 33 They also recognize that the demand and cost of childbearing have increased and become a burden to parents (erosion of the traditional belief a child will grow by his fortune). They also realize that delaying childbirth and spacing births have paramount advantages for the mother, child, and family.
Planning to have a fixed number of children is crucial for fertility transition. 34 The majority of participants in this study specified their ideal number of children for themselves and their daughters. However, there is a desire for a high number of children ranging from four children in educated and urban settings up to seven or more in the rural, uneducated, and Muslim communities. Similarly, women’s ideal number of children reported by the 2016 Ethiopian Demographic and Health Survey (EDHS) is high, with the mean ranging from 3.7 in Addis Ababa to 10.7 in Somalia. 7 According to the demand theory of fertility transition, fertility decline follows an ideational and behavioral innovation of the shift from high-quantity-low-quality to high-quality-low-quantity children.35,36 However, if our study participants have adequate resources and assets, they tend to have more births rather than increasing their investment in the quality of fewer children. Such demand for a higher number of children is common across African countries 37 and is a potential impediment to accepting family planning measures.
The concept of family planning, diffused primarily as contraceptive use for birth spacing, is considered essential for the health of mothers and children, and to cope with the economic challenges of childbearing. Contraceptives are generally perceived as morally legitimate, socially and psychologically acceptable, and programmatically supported means of birth spacing. The EDHS and other studies also showed a positive attitude toward contraceptives.7,38,39 Understanding the benefit packages and women’s empowerment are important contributors to the adoption of family planning methods. 40 The acceptance of contraceptive practice not only prevents unwanted pregnancy but also serves to diffuse the ideation and practice of low fertility. 41 In contrast to these developments, the willingness and practice of family planning for birth limitation is poor. These findings are anticipated because the national family planning guidelines in Ethiopia also give due emphasis to birth spacing and the health rationale of the family planning programs rather than fertility limitations.42,43 The socio-cultural norms favoring high fertility are also possible reasons for not adopting contraceptives for birth limitation. Studies in Ghana and other SSA countries also found similar acceptance of birth spacing but hesitation toward birth limitation.44,45
Women’s knowledge and ability to access and use contraceptive methods are vital for fertility transition. 20 Similar to findings from other studies,38,46 participants in this study are well-informed about the types and sources of contraceptives. There is also commendable accessibility and utilization of contraceptives. As reported in the national surveys, women’s contraceptive use for spacing has increased over time. 46 Despite such contraceptive uptake, there has not been a significant change in the proportion of optimal birth spacing over the last two decades. 47 Whether such contraception for spacing can bring about fertility transition depends on how long women stay with effective contraception. A woman who is not ready or willing to limit her fertility is more likely to discontinue contraception once she feels safe to conceive, and she is less likely to tolerate side effects. The 2016 EDHS reported an annual prevalence of 35% contraceptive discontinuation, with the desire to conceive and side effects being the primary reasons. 7 Moreover, the cumulative impact of contraception for spacing may be offset by a decrease in breastfeeding and postpartum infecundity. Evidence regarding the role of contraceptives in reducing the desire for children and inducing transition is inconclusive or negligible.48,49
This study also identified factors affecting the community’s adaptation to the ideation and practice of contraceptives. Women, especially those living in Jigjiga, eastern Ethiopia, are influenced by their husbands’ preference for male children, large family sizes, and religious opposition to birth limitations. Their contraceptive practice is also inhibited by women’s decision-making power, lack of preferred methods, and contraceptive side effects. These factors align with findings from other studies in Ethiopia50 –55 and other African countries. 56 Among these barriers, women’s complaints of contraceptive side effects are intense and often linked to husbands and religious prohibitions.
The effect of religion on family planning, particularly among Muslim participants, is evident in women’s RWA to plan their fertility. Religiously, children are considered a fathomless gift of God, which discourages women from calculating the costs and benefits of having children. The perception that “God made you and will also bear you” impedes women from limiting childbearing for economic reasons. Religion also deters women from using modern contraceptives due to fear of the spiritual offense of inserting foreign bodies to prevent potential offspring. Other studies also indicate that religion supports birth spacing using breastfeeding but prohibits birth limitation.54,55,57,58 However, the overall effect of religion in Ethiopia may be bargained by the community’s high desire for birth spacing. The religious institutions and their leaders in Ethiopia are also said to be either supportive or neutral toward the family planning program. As noted in other studies too,52,53 husbands’ opposition to contraceptive use due to a desire for many children or fear of violating religious beliefs exacerbates psychological costs among women (e.g., fear of side effects and religious blame). To realize their desire for a son-dominant large family size, men also practice polygamy, which can increase the number of women in cohabitation, wives’ competition for more births, and potentially threaten childcare and survival. 59 Fear of contraceptive side effects, especially infertility, is a major concern among women who are willing to space their childbirth. Other studies also identified fear of side effects as a main client-side barrier to contraceptive use.7,51 The prevalence of perceived fear of infertility in rural Ethiopia is alarming. 60 This fear, along with other barriers, can hinder the adoption of contraceptives and may even lead to gossip that can reverse the hard-gained progress. 20
Using a comprehensive model and data from three socio-economically distinct populations, this study identified the facilitators and barriers of fertility transition in Ethiopia. Stratifying the facilitators and barriers across the RWA components facilitates understanding of the fertility transition. However, the ideas presented under RWA may not be mutually exclusive due to the similarities of the concepts. This study relies solely on qualitative data, and quantitative modeling of the RWA toward fertility limitation is recommended. Moreover, our sample is limited to those who ever give birth and the perspectives of people who do not childbearing is not included. The scope of the study is also limited only to three geographic areas which limits its capacity to reveal the perspective across different geographic areas.
Conclusion
While there is limited readiness, willingness, and practice toward birth limitation, there is sufficient willingness and adoption of contraception for birth spacing. Pro-natal cultural and religious beliefs, along with non-demographic rationalization of the family planning program, sustained the communities’ desire for high fertility. Although women are knowledgeable and accept contraception, there are still demand and supply side barriers to their actual utilization. In addition to minimizing these supply and demand side barriers, Ethiopia’s current economic, social, and demographic situation necessitates advocacy for accelerated fertility decline through the promotion of both spacing and limitation. Given the limited scope and qualitative nature of this study, further research is required to address the limitations and investigate the demographic impact of Ethiopia’s family planning programs.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251327037 – Supplemental material for Rationalization, facilitators, and impediments of fertility transition in Ethiopia: qualitative exploration of the community readiness, willingness, and ability
Supplemental material, sj-docx-1-reh-10.1177_26334941251327037 for Rationalization, facilitators, and impediments of fertility transition in Ethiopia: qualitative exploration of the community readiness, willingness, and ability by Tesfay Brhane Gebremariam, Mitike Molla and Wubegzier Mekonnen in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
The authors are grateful to all the regional officers who allowed the study, and to all participants of this research who provided their rich ideas. We acknowledge the data collectors for their commitment to conducting the interview and transcribing the data. We are also thankful to Addis Ababa University for approval and funding of the research. Finally, we also acknowledge the online language editing service from ![]() .
.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.