
Abstract
Among the approaches to functional hand rehabilitation after stroke, the use of hand rehabilitation robots can provide functional training of the hand or assist the paralyzed hand in activities of daily living, and in particular, intelligent control strategies play a very important role in rehabilitation robotics. The purpose of this review is to summarize the current status of commercially available intelligently controlled hand rehabilitation robots developed in recent years. Firstly, we summarize the theoretical basis of post-stroke hand rehabilitation in the reviewed literature, and the intelligent control strategies of hand rehabilitation robots. Then, representative intelligently controlled hand rehabilitation robots are listed. Finally, we discuss the future directions of the intelligently controlled hand rehabilitation robots. The results show that the development trend in recent years is more inclined to: combining the theoretical basis of stroke hand rehabilitation and studying intelligent control methods of hand function rehabilitation robots that combine human bioelectrical signals to achieve prediction of patients’ motor intentions and also induced stimulation of neuroplasticity in the brain. As well as fusing different bioelectrical signals as a way to improve the applicability of the assistive device in real life. This paper will help researchers to understand the current state of the art regarding intelligently controlled hand rehabilitation robotics after stroke in recent years.
Introduction
The hand, as one of the most important and joint freestanding parts of the human body, can greatly affect daily life if it is injured or has motor impairment. Stroke, a common high-risk disease among middle-aged and elderly people, can directly exacerbate the occurrence of hand motor dysfunction.1–6 The seventh national census recently announced that China is still the most populous country, but the aging population is increasing and the stroke patient base is increasing dramatically. Currently, the prevalence of stroke in China is about 1 case per 182 people, and with a total population of 1.4 billion, the number of stroke patients is about 7.69 million, of which the disability rate is about 1/3. 7 In stroke patients with hand motor impairment, a certain degree of rehabilitation can be achieved if a positive attitude and scientific rehabilitation methods are used to achieve the basic goal of self-care. The rehabilitation modalities are also relatively diverse and usually use reducing spasticity, increasing neuroplasticity, repairing damaged motor nerves, strengthening the training of finger joint flexibility, relieving excessive muscle tone in the hand, and maintaining muscle memory.8,9 Neuroplasticity, also known as neuroplasticity, or brain plasticity, refers to “the ability of neurons and neural networks in the brain to change their connections and behavior in response to new information, sensory stimuli, development, injury, or dysfunction.” Neuroplasticity acts as the “Achilles tendon” of the brain, inducing the brain.10–21
Based on the above-mentioned mechanisms of hand rehabilitation, patients usually use manual rehabilitation, that is, a professional rehabilitator to help them with joint muscle training and rehabilitation.22,23 Although this type of rehabilitation is effective and well-targeted, the cost of rehabilitation is prohibitive to the average family. At the same time, the effectiveness of this type of rehabilitation is not standardized and is largely determined by the level of expertise of the rehabilitator, and the lack of physical ability of the rehabilitator during long hours of rehabilitation training can directly affect the effectiveness of rehabilitation. Based on the above-mentioned problems of manual rehabilitation, the emergence of hand rehabilitation robots is a blessing for stroke patients, which is expected to improve the rehabilitation rate of hand functional movement disorders and enable more patients to restore their self-care status. 24 The study of hand rehabilitation robots first originated in Europe and the United States, and the real productization of hand rehabilitation robots was achieved in the early 21st century. 25 In the early stage of development, hand rehabilitation robots did not have a feedback adjustment system and used open-loop control, which could not provide feedback on the finger joint bending angle and contact force information during the rehabilitation hand movement, and the movement was controlled by a predetermined fixed program. Since patients need to perform multiple hand rehabilitation exercises to achieve effective rehabilitation training results, CPM (Continuous Passive Motion) type hand rehabilitation robots are relatively rare. For example, the finger and wrist joint rehabilitation device developed by KINETEC, 26 France. The ARTRMOT finger rehabilitation device produced by ORMED, 27 Germany. And the RELIVER RL-100 hand rehabilitation training device developed by MAREF, 28 Korea.
In addition to CPM-type hand rehabilitation robots, there is also a class of ARM (Active Repetitive Motion) type hand rehabilitation robots that help patients who have reached a certain level of muscle strength to conduct rehabilitation training. For example, Gloreha, 29 an Italian company, has developed an intelligent motor-driven flexible hand rehabilitation robot. The intelligent rehabilitation glove has rich human-computer interaction functions, and patients with stroke or hemiplegia wear it and are guided by 3D video, color and sound through motor imagery, mirror therapy, active-passive training, two-handed movement, and task-oriented rehabilitation training through the drive of five motors. It can promote the rehabilitation of functional fine hand movements and grasping, as well as the patient’s cognitive function, hand-eye coordination, and the rehabilitation of other sensory nerves in the body. The rehabilitation hand is easy to put on, but lacks manual active movement intention prediction and uses the patient’s own physiological signals for active rehabilitation training.
Sierotowicz et al. 30 of the Institute for Robotics and Mechatronics at the German Aerospace Center (DLR) designed an EMG-driven, machine-learning controlled soft glove for grip assistance and rehabilitation. Soekadar et al. 31 published three papers, in 2014, 2015, and 2016, describing a novel brain/neuro-computer interaction (BNCI) system for controlling a hand exoskeleton robot that integrates electroencephalography (EEG) and electrooculography (EOG). The use of deep learning and machine learning algorithms in intelligent control can substantially improve the accuracy and robustness of control. 32 For example, when controlling a hand rehabilitation robot using EMG signals, it is necessary to analyze the EMG signals during limb movements, by comparing their characteristic differences. Different movement patterns are identified and the external device is controlled in real time so that it simulates the human hand movement patterns. Subasi et al. 33 used wavelet analysis to first extract the features of the surface muscle signals and then used neural networks to perform pattern classification experiments on the extracted EMG feature signals, and their correct recognition rate reached 90.7%.
The analysis of the above-mentioned categories of hand rehabilitation robots shows that the research direction in recent years has been more toward intelligent control strategies for hand rehabilitation robots. Although, many review articles on hand rehabilitation robots have been published today.34,35 We have also published a review on the development of hand rehabilitation robots after stroke, drive modes, training modes, and control strategies. 36 However, we did not describe in detail the intelligent control strategies of hand rehabilitation robots, as well as did not summarize the development of commercially available intelligent controlled hand rehabilitation robots specifically. In this paper, we systematically review the theoretical basis of stroke hand rehabilitation, focus on an overview of the classification of intelligent control strategies, and briefly summarize the current status of commercial intelligent control hand rehabilitation robot development in recent years. The basic outline of the content covered in this paper is shown in Figure 1. The rest of the paper is organized as follows: Section “Methods” describes the theoretical foundations of stroke hand rehabilitation. Section “Theoretical basis of hand rehabilitation in stroke” describes the classification of intelligent control strategies, which broadly includes non-biosignal control and bioelectrical signal control. Section “Classification of intelligent control strategies” summarizes the current status of commercial intelligent control hand rehabilitation robot development. In Section “Current status of development of commercial intelligent controlled hand rehabilitation robots,” the limitations and future directions of the research are discussed and summarized. In Section “Discussion,” the full text is summarized.

The basic outline of the contents is covered in this paper.
Methods
A chronological review of several reputable literature databases, namely Science Direct, PubMed, IEEE Xplorer, SciVal, and Google Scholar, was conducted to identify trends in intelligent control strategies in hand rehabilitation robots after stroke from 2010 onwards. The keywords used to examine more classified papers were “hand rehabilitation” and “hand exoskeleton.” The search results were further filtered using the keywords “post-stroke,”“intelligent drive,”“rehabilitation,” and “control.” A set of inclusion and exclusion criteria was then applied to select the appropriate literature.
Inclusion and exclusion criteria
The following inclusion and exclusion criteria were used to screen out discrete knowledge critical to the systematic review and temporal review of intelligent control strategies with functional post-stroke hand rehabilitation robots.
Inclusion criteria
This study introduces and applies active control techniques to develop hand rehabilitation robots, including wearable gloves, hand exoskeletons, or new hand exoskeletons that combine both.
The study demonstrates the following three attributes of the control system aspects of the designed hand rehabilitation robot: active control, sensor control, and bioelectrical signal control.
This paper is available to the authors and is a scientific article written in English.
The device is used for rehabilitation or assistive purposes.
Exclusion criteria
The device was originally intended for use on body parts or limbs other than the hand.
The device was a prosthesis or anthropomorphic hand for the treatment of a lost limb.
The device was used other than that for rehabilitation and assistance for activities of daily living (ADL).
This study was not sufficiently informative in terms of design, which made the analysis unclear.
A framework was developed to analyze the relatively large number of studies found in the literature search. The aim was to extract the various techniques used in the developed devices and present them in a logical and systematic order so that future designers could gain knowledge of existing methods. These devices are classified according to their control methods, and then, the extracted control design methods provide a broad decomposition of the control methods used for each device. Finally, the current state of development of commercially available intelligently controlled hand rehabilitation robots in recent years is summarized. While this framework does not address the exact construction process of the device, its potential lies in the various building blocks needed to design the device and the methods that have been explored.
Theoretical basis of hand rehabilitation in stroke
The ultimate purpose of the hand function rehabilitation training robot is to meet the rehabilitation needs of stroke patients with hand dysfunction. Therefore, before analyzing and designing the hand function rehabilitation training robot, the causes of stroke leading to hemiplegia and the feasibility of hemiplegia rehabilitation are first given. Stroke rehabilitation is a long and complex process, and it is particularly important to explore the link between intelligent control strategies of stroke hand rehabilitation products and the promotion of motor, cognitive and neurological recovery. In this section, we will provide an overview of the basic theory of stroke hand rehabilitation and focus on intelligent rehabilitation control strategies to refine design principles that are consistent with stroke hand rehabilitation training, as well as to understand current domestic and international research trends in the field of hand rehabilitation robots in order to provide theoretical support for research on stroke hand rehabilitation.
Stroke is a common acute cerebrovascular disease in clinical practice, which is caused by the dysfunction or death of central neurons in the brain due to insufficient blood circulation supply to the brain caused by risk factors such as hypertension, smoking, obesity, hyperlipidemia, and diabetes. In practice, there are two types of strokes: hemorrhagic stroke, which is caused by bleeding, and ischemic stroke, which is caused by blockage of blood vessels. A hemorrhagic stroke is a stroke in which blood enters the brain tissue directly due to intracranial hemorrhage, which causes the death of brain cells in the area and eventually leads to brain tissue dysfunction, and can be subdivided into internal and external hemorrhage. Internal hemorrhage refers to intracranial cerebral hemorrhage or intraventricular hemorrhage, while external hemorrhage refers to hemorrhage between the dura mater and skull or between the arachnoid and soft spine; ischemic stroke refers to a decrease in blood supply to a part of the human brain, which causes the death of brain cells in that area and leads to brain tissue dysfunction. 37
The human brain can be divided longitudinally into two parts, called the left half of the brain and the right half of the brain, the left and right half of the brain in the human body functions are divided, but the left half of the brain and the right half of the brain are not completely independent of each other, they collaborate with each other to control the functions of the human body.
The left side of the brain manages the movement of the right side of the body through the motor nerve, while the right side of the brain manages the movement of the left side of the body through the motor center, which shows how a stroke can cause hemiparesis in humans. Either the left or right side of the brain is affected, resulting in hemiparesis. Stroke induces brain cell death and damage to the cortical nerve centers, resulting in hemiplegic sequelae. Blockage of nerve pathways in the brain is the root cause of limb impairment in the upper extremities, lower extremities, and hands, so the most important thing in stroke rehabilitation is to repair damaged nerve pathways while restoring hand function. Rehabilitation training is the main method to improve the sequelae of stroke, especially for hand movement disorders, which can restore patients’ ability to take care of themselves to the maximum extent. Brain plasticity is the scientific basis for the treatment of brain injury and the main theoretical basis for stroke rehabilitation. Through reshaping activities such as behavior, environmental stimulation, thinking and emotion, old neural pathways can be retrained or new neural pathways can be induced to improve the reduced motor function of the hand due to brain injury, thus facilitating the rehabilitation process. In addition, the patient’s active participation plays a key role in neural remodeling and motor learning, and the systematic rehabilitation training will directly determine the possible degree of rehabilitation treatment.
Hand disorders are caused by the loss of upper motor neuron regulation in the body’s motor system, resulting in dysfunctional coordination between the affected hand clusters and abnormal muscle tone, resulting in motor dysfunction. Stroke rehabilitation training for hand disorders is complex and variable, especially hand dysfunction. Swedish physiotherapists have proposed the Brunnstrom assessment method based on hand function characteristics, which assesses stroke hand rehabilitation into six different stages, as shown in Table 1, with differences in the rehabilitation goals and rehabilitation training methods corresponding to each stage.
Stroke hand function rehabilitation cycle chart.

The six stages of the Brunnstrom method have been widely used in clinical practice, and rehabilitation training programs have been proposed according to the characteristics of the hand at different stages. For patients with stage I to stage II spasticity, the hand is basically inactive, and passive rehabilitation training methods are mainly carried out at this stage, such as physical factor therapy, stretching training, and specific rehabilitation training movements driven by the rehabilitation therapist with the help of external force; for patients with late stage IV spasticity, the hand has the ability to move in a small range and can control simple movements. For patients in late stage V and VI spasticity, the hand is able to selectively move on its own and has a certain muscle strength, so active intensive rehabilitation training can be chosen during this period to provide certain resistance to strengthen the flexibility, coordination and strength of hand function, and improve the grip and fine manipulation. Due to the limitations of medical resources and treatment costs, patients in these two stages need to be transferred to their homes for independent rehabilitation training, but due to the lack of professional guidance and supervision and human inertia, they often fail to attract patients’ attention. These two stages are important periods for recovery and should not be taken lightly. Therefore, for stroke patients in stages V and VI, intelligent control strategies are integrated into the hand rehabilitation robot, which can help patients efficiently perform hand training and return to activities of daily living as soon as possible.
Classification of intelligent control strategies
Many challenges remain with existing hand rehabilitation robots, both in hardware and software. A major challenge is that devices often lack sufficient awareness of user behavior and intent, which largely limits the performance of user interaction control. The optimal interaction is one in which the hand rehabilitation robot allows the human to simply and naturally execute movements without redundant communication with the device, and this interaction must be recognized through appropriate sensor interfaces to activate motion execution. To approach this optimal state, the interaction interface should be as close to the human nervous system as possible.
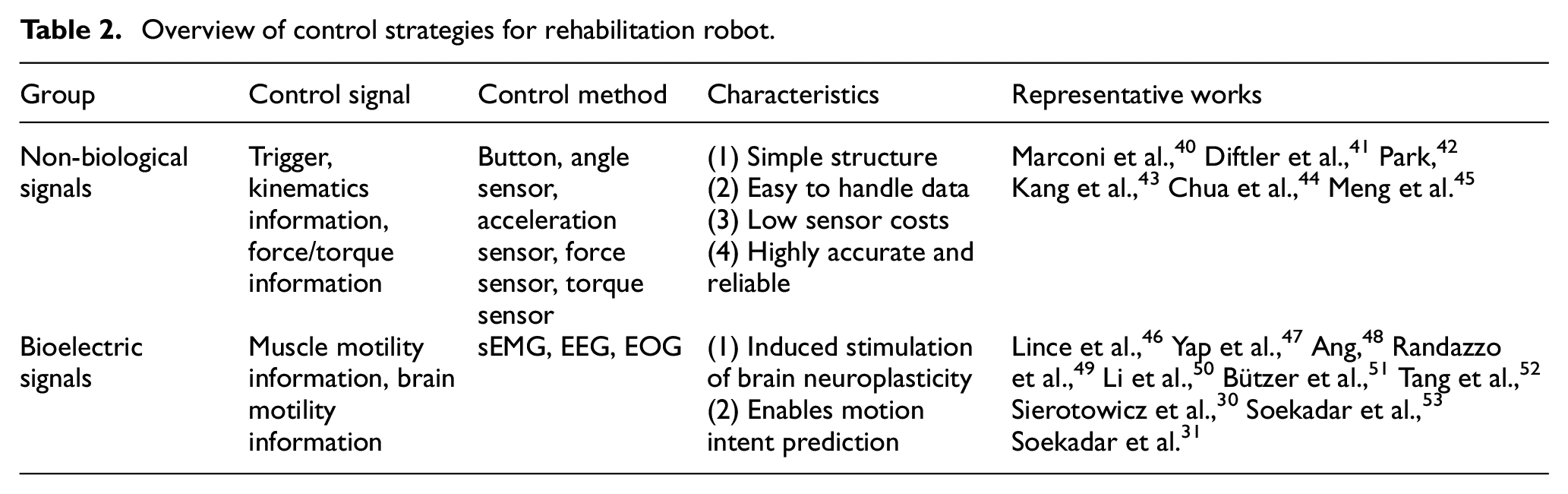
The choice of input signal sensors for hand rehabilitation robot control can be divided into biological and non-biological signals. Non-biological input signals have been successfully used to control a variety of devices, such as angle sensors, force sensors, acceleration sensors, and other signals. These signals have high accuracy and reliability and reflect the user’s motion process well. 38 However, before a hand rehabilitation robot can start providing support, it must be able to predict the user’s intention to generate motion in the joint to activate the hand rehabilitation robot’s power unit. Therefore, the interactive control method for the hand rehabilitation robot must find an appropriate input signal and provide information about the user’s motion intention without any delay. Bio-signals, especially bioelectrical signals, are coming to the forefront of many scholars as control signals that can better interpret the user’s intention. These signals provide a good balance between the initial motion intent and signal interpretability. Proportional control of bioelectrical signals provides a continuous output signal from the human to the device by rectifying and smoothing the signal directly as the desired angle, speed, torque, or other device output. 39 Table 2 summarizes the classification of intelligent control, control sensors, and their characteristics.
Overview of control strategies for rehabilitation robot.
Non-biological signals
Non-biological input signals have been successfully used to control signals from various devices such as trigger switches, angle sensors, force sensors, inertial measurement units (e.g., accelerometers, gyroscopes, magnetometers), etc. 54 These signals have high accuracy and reliability and can reflect the user’s motion well.
Trigger control
A trigger refers to a button that the user must press to perform a task, such as closing the hand to grasp an object or opening the hand to release. 55 Electrical switches are also used to select the type of training for the user or therapist to choose.
Angle signal control
The bending angle of the finger can be used as an input signal for the position controller to operate the hand rehabilitation robot, as an important indicator to assess the degree of rehabilitation of the patient’s finger or as a signal for position-based impedance control. For the measurement of finger motion, bending sensors or rotary encoders can be used. 56 The well-known theory of impedance control methods was proposed by Hogan 57 in the 1980s in the study of contact control of robot ends with the environment. Impedance control is divided into two different control results based on force and position. The position-based impedance control consists of two parts, the position control inner loop and the impedance control outer loop, where the position control inner loop processes three data, the desired position, the position compensation amount, and the actual position, so that the actual position of the robot tracks up to the desired position. And the impedance control outer loop is to process the difference between the desired force and the actual force to get the position correction amount. These will continuously adjust the target impedance model parameters by actually detecting the force between the robot and the environment, and then control the robot’s position through the position controller to achieve force control.
Pressure signal control
The pressure transducer is an important indicator to assess the degree of rehabilitation of a patient’s finger during the rehabilitation process. At the same time, real-time monitoring of the pressure applied to the patient’s fingers can also enhance the safety of the rehabilitation system. Since many hand rehabilitation institutions are not designed with corresponding passive power feedback actuators. During the patient active training mode, a pressure sensor is required to work with the actuator to achieve the effect of providing impedance to the patient’s finger. When the pressure sensor detects that the pressure generated by the patient’s finger reaches a given value, the actuator provides power. Force-based impedance control is achieved by controlling the joint actuation torque to adjust the end contact force and displacement. In the force-based impedance control method, the robot reflects the end impedance characteristics of the robot by controlling the robot joint torque through feedback based on the contact force between the end and the environment. 58 In practical applications, the robot end position and contact force are detected in real time, and the grid feedback position and desired impedance model generate the desired force output, and the difference between the desired force and the actual contact force is taken, and the control torque is calculated by the robot dynamics model based on the force error as the joint driving force, so that the robot’s system behaves as the desired impedance model characteristics. Therefore, force-based impedance control must first determine an accurate kinetic model of the robot before the desired impedance model and accurate contact force control can be achieved.59–61
Inertial measurement unit
Inertial sensors are characterized by their ease of wear, high sensitivity, and more widespread use. The collected inertial measurement units can reflect the state as well as the direction of the motion movement, which contains acceleration, gyroscope, and magnetometer information. Liu et al. 62 performed gesture recognition for inertial electromechanical systems and proposed a bidirectional long short-term memory loop neural network (BLSTM-RNN) algorithm for gesture classification of acceleration and angular rate, and its classification Wang et al. 63 used a combination of DTW and sparse representation of acceleration signals to recognize 10 dynamic gestures and validated them on an Android cell phone system, which showed good recognition performance. Hsu et al. 64 used a digital pen based on inertial sensors combined with DTW algorithm for writing gestures and verified the effectiveness of the method experimentally. Gupta et al. 65 used acceleration and gyroscope sensors to achieve continuous recognition of gestures and also accomplished the function of predefining gestures and controlling smart applications on smartphones.
These non-biological input signals have high accuracy and reliability and reflect the user’s motion process well. However, before a hand rehabilitation robot can begin to provide support, it must be able to predict the user’s intention to generate motion in the joint to activate the hand rehabilitation robot’s dynamics. Therefore, the interactive control method for the hand rehabilitation robot must find an appropriate input signal and provide information about the user’s motion intention without any delay.
Bioelectric signals
Human bioelectrical signals are the potentials excited by the transmission of neurons containing information about human behavior to the relevant tissues or organs, and directly reflect human intentions. The relationship between muscle and electricity was discovered by Luigi Galvani in his frog experiments in 1786 and further investigated in 1791. With the progress of science, the practicality and application space of bioelectric signals were gradually discovered and expanded, and it is widely used in the fields of prosthetic control, sports rehabilitation, and art installations. Five types of bioelectric signals, namely, muscle electrical signal (EMG), electrocardiographic signal (ECG), electrooculogram (EOG), electroencephalographic signal (EEG), and evoked potential/event-related potential (EP/RP), can be captured by surface electrodes. Based on these types of bioelectric signals, which can be easily captured by surface electrodes and converted into computer commands, active rehabilitation training content can be provided to patients by hand rehabilitation robots.66,67 Since EEG and EMG signal acquisition and processing technologies are relatively mature and rich in information, interactive systems based on this information have been favored by many researchers at home and abroad. In this paper, we focus on the application of surface muscle electrical signals (sEMG), electroencephalographic signals (EEG), and electrooculographic signals (EOG) that are commonly used to control hand rehabilitation robots.
Electromyography (EMG)
From neurological studies in the last decade, it has been found that the most accurate approach to control signal input is based on the application of electromyographic (EMG) signals, specifically the integrated analysis of muscle movement and the brain processing that accompanies it.
EMG signals originate from alpha motor neurons in the spinal cord, whose axons extend to the muscle fibers and constitute a biochemical coupling with them via the motor end plate. Alpha motor neurons together with all the muscle fibers they innervate form the motor unit (MU), 68 which is the smallest functional unit of muscle contraction, and the structure of the motor unit is schematically shown in Figure 2(a). 69 The microstructure of the muscle ganglion at the axon terminal of a neuron is shown in Figure 2(b),when an α motor neuron generates a nerve impulse, the impulse reaches the axon terminal of the neuron along the axon and stimulates the presynaptic membrane to release acetylcholine (Ach), and the motor end plate specifically binds to acetylcholine to generate an end plate potential, which is superimposed in space and time to generate an action potential. This is followed by an excitation-contraction coupling reaction, which ultimately causes a contractile response in the muscle. The action potential generated by a single muscle fiber is called the single fiber action potential (SPAP), and the simultaneous excitation of all muscle fibers innervated by the same motor unit, where the combination of all muscle fiber action potentials is called the motor unit action potential (MUAP). The continuous release of motor unit action potentials will produce a motor unit action potential sequence (MUAPT). After the MUAPT sequence is conducted through muscle, subcutaneous tissue and skin, it is superimposed on the skin surface together with environmental noise to form a surface EMG signal.

(a) Motion unit structure and (b) neuromuscular ganglion microstructure.
EMG can be extracted by needle electrodes inserted directly into the muscle or by using a less invasive surface electrode approach. The needle electrode approach ensures a more accurate recorded signal that can more closely match the electrical activity of the muscle source. To address the various inconveniences associated with invasive electrodes, Hermens et al. 70 proposed the surface EMG signal detection technique in 1984, which acquires human surface EMG signals through non-invasive electrodes. Compared to invasive myoelectrodes, non-invasive myoelectrodes are able to acquire EMG signals on the human skin surface without damaging human tissues. The surface EMG signal acquired by non-invasive myoelectrodes is the superposition of multiple motor unit action potentials (MUAP) in time and space after transmission through the human subcutaneous tissue to the skin surface. Non-invasive myoelectrodes are widely used in medical and rehabilitation fields because of their non-invasive nature, ease of operation, and patient acceptance. 71 The EMG signal acquired by non-invasive myoelectrodes is called surface EMG signal. The non-invasive nature of surface electrodes to measure EMG signals has played a great role in the promotion of EMG signals in daily applications. Although there is more or less muscle activity overlap due to the use of skin surface electrodes for signal acquisition, they are also able to provide sufficient information in various applications. sEMG signals have been a commonly used bioelectric signal in human-computer interaction control because they directly reflect the user’s muscle activity.72,73 Currently, myoelectric control strategies based on manual action pattern recognition are mainly studied at home and abroad to realize the control of hand rehabilitation robots, as shown in Figure 3.

Control method based on myoelectric pattern recognition.
EMG was first applied to motor intention recognition and control in the 1960s. 74 The control methods using EMG signals are broadly classified into switching control, proportional control, and pattern recognition control. Most of the early EMG control uses switch control, also known as threshold control. This control method generally uses the single channel EMG signal amplitude information as a switch, by comparing the size of the EMG signal amplitude and the set threshold value to control. When the EMG signal amplitude is greater than the set threshold value is on, and conversely is off, this control method is the most stable and simple, mostly used in commercial prosthetic devices. 75 Proportional control is a proportional mapping of the amplitude of the EMG signal to the controlled object, where the controlled object can be the position or speed of the motor rotation, etc. This control method is more in line with human habits than the switch control, and the user will feel more natural in the process of use, however, proportional control is suitable for controlling single-degree-of-freedom exoskeletons due to its mapping relationship, and it is difficult to cope with the complex situation of multi-degree-of-freedom. However, proportional control is suitable for controlling single-degree-of-freedom exoskeletons due to its mapping relationship, which is difficult to cope with myoelectric control in complex multi-degree-of-freedom situations. 76 Pattern recognition control is a method to obtain classifiers by computing statistical features of multiple myoelectric signals and use the classifier output results for motion intention recognition. 77 Pattern recognition control has been widely studied in the field of myoelectricity for the reason that this control method is applicable to the recognition of multi-degree-of-freedom motions. With the proposal and application of various novel mathematical modeling, signal analysis, and other signal processing methods, pattern recognition control can obtain considerable classification results even in multi-degree-of-freedom control scenarios, so this method is now widely used.
Whether a hand rehabilitation robot can assist patients well in completing rehabilitation training movements depends on how well the rehabilitation training system recognizes the movement patterns correctly.78,79 At the present stage, the pattern recognition of surface EMG signals mainly suffers from a single type of recognized movements, weak stability of experiments, and low real-time of algorithms. The results of related studies show that the difficulty of pattern recognition increases greatly with the increase of action types. Although the recognition rate of action patterns can be improved to some extent by increasing the data length of segmented continuous EMG signals, the delay in the signal processing process also relatively increases and eventually affects the real-time performance of the algorithm. In addition, the placement of the sampling electrodes has a great influence on the stability of the pattern recognition experiment. 80 Therefore, it is clear from the above factors that there is still a lot of work to be done in the research of pattern recognition of surface EMG signals for action pattern recognition with high correct rate and satisfying real-time requirements. In addition, the effectiveness of pattern recognition does not only lie in the extraction method of EMG signal features and the selection of classifier, but the arrangement of EMG signal sampling electrodes is also an important factor.
Tong et al. of the Department of Health Technology and Informatics, The Hong Kong Polytechnic University designed a hand rehabilitation exoskeleton based on myoelectric signal control Hand of Hope,81–83 as shown in Figure 4(a). The robot mainly consists of two modules, a hand exoskeleton that can adapt to different finger lengths and an embedded exoskeleton based on a human brain controller. The exoskeleton is driven by five finger assemblies driven by linear actuators for finger motion rehabilitation. Each finger component is mechanically linked to achieve flexion/extension of the MCP and PIP joints. The microcontroller controls the linear actuators by collecting surface EMG signals from the muscle groups located at the adductor pollicis brevis (APB) and extensor digitorum brevis (ED) tendons, respectively. An EMG-triggered control strategy was used to achieve hand-opening hand-closing movements by a 20% threshold of the maximum voluntary contraction (MVC) EMG signal at the APB and ED. A significant improvement in clinical performance was found in eight stroke patients by training them 20 times (3–5 times per week).
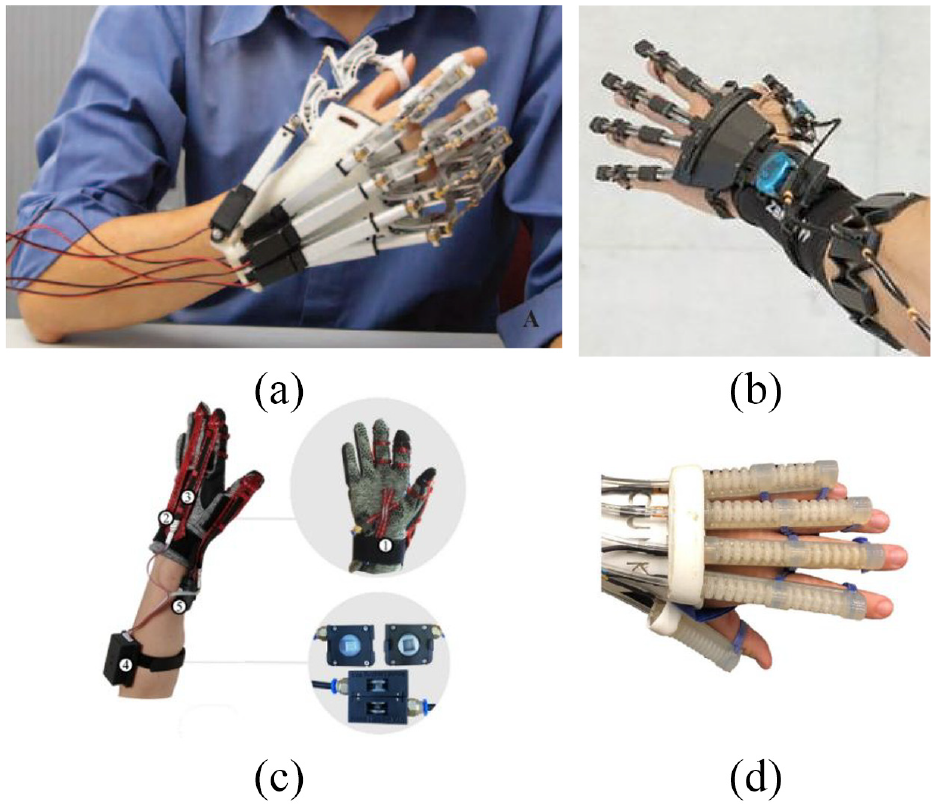
In 2021, Butzer et al. designed RELab tenoexo which is a fully wearable assistive soft hand exoskeleton for daily activities as shown in Figure 4(b). 51 It consists of a hand module attached to the hand and a backpack containing electronics, motors, and batteries. It consists of a hand module attached to the hand and a backpack containing electronics, motors, and batteries. The backpack and the hand module are connected by a force transfer system based on Bowden cables and can be connected by a clip mechanism. This soft hand exoskeleton can achieve multi-mode control, the first is the button control finger open and close, the second is the use of Myo armband to capture the arm muscle signal of the good hand to control the palm open and close. RELab tenoexo this glove is currently in the structural design part of the innovation, it cleverly combines flexible materials and rigid materials to achieve a lightweight structure, light weight, wear comfortable, grip ability adaptability, and other characteristics. However, the researchers pointed out that it still has some limitations and room for development, and in the future it is hoped that the structure and software design to completely realize the intention recognition autonomous control.
Sierotowicz et al. 30 of the German Aerospace Center (DLR) Institute for Robotics and Mechatronics designed a sEMG-driven machine learning controlled soft glove for assisted grasping and rehabilitation as shown in Figure 4(c). The glove came with a control scheme for detecting the user’s motor intention, which was estimated by a machine learning algorithm based on muscle activity. Six healthy study participants used the glove in three assistance conditions in a force reaching task. The results show that the active assistance of the glove can help the user by reducing the muscle activity required to obtain medium-high grip forces and that closed-loop control of the compliance-assisted glove can be successfully achieved by machine learning algorithms.
Tang et al. 52 of the University of Hong Kong designed a probabilistic model-based learning control for hand rehabilitation, as shown in Figure 4(d). This soft pneumatic glove allows for a task-oriented sEMG intention-driven training model. The control performance of three able-bodied subjects and three stroke survivors who participated in 20 rehabilitation sessions was evaluated. With the intention-driven strategy, stroke patients could successfully trigger the system and complete the task in more than 90% of the repetitions. Their proposed approach allows the soft pneumatic glove to provide adaptive assistance for all participants to complete different tasks. The tracking error and muscle co-contraction index tended to decrease with training, while the gesture index tended to increase. All stroke survivors showed improved hand function and better muscle coordination after training. This work promotes the use of soft robotic training systems in stroke rehabilitation.
The generation of surface EMG signals is overtaken by motion generation. It allows predetermination of movement intention, which is a good advantage for patient initiative. However, because the use of sEMG to control tremor and muscle fatigue in the rehabilitation hand can greatly reduce the applicability and reliability of myoelectric control, muscle physiology models of muscle-related parameters are difficult to obtain and identify, and are significantly affected by perturbations in online identification, and the model will gradually increase the cumulative error under long time estimation, even leading to divergence. And the data-based black-box modeling methods such as neural networks are more sensitive to experimental data and experimental environment, and once the experimental environment differs from the real environment, it will lead to a large variance of the trained model and produce overfitting, resulting in a large difference between offline experimental results and online test results. Therefore, attention should be paid to environmental factors and testing accuracy when using surface EMG signals.
Electroencephalography (EEG)
Brain-machine interfaces (BMI) have attracted much interest in the field of human-computer interaction in recent years, and such interfaces can directly decode the user’s brain signals to control devices and become a new control pathway. However, unlike sEMG signals, which have a one-to-one mapping between motor intention or limb movement, EEG signals do not fully reflect this explicit and direct relationship. Therefore, extracting motor intent from EEG signals is more challenging than sEMG signals. There are many ways to acquire EEG signals, and different criteria distinguish them according to different criteria.
The common acquisition methods are implantable and non-implantable; as the name implies, implantable acquisition is the implantation of a signal acquisition device into the cerebral cortex, and the EEG signals acquired in this way are of high quality and more specific to brain regions, enabling, for example, tetraplegic patients to drink a cup of coffee. 84 However, invasive brain-computer interfaces carry the risk of surgical complications and infections, and are accompanied by additional risks associated with long-term signal instability and reduced performance in decoding intentional information, 85 so this approach is currently mostly targeted at animal experiments. In contrast, the non-implantable approach does not require the implantation of electrodes inside the brain, which is safer and more convenient, but the signal quality is relatively poor.
In the second part of this paper, it was briefly introduced that the left and right halves of the brain work together by collaborating with each other to control various functions of the human body. In the case of EEG signals, it is also necessary to study the cortical structure of the brain. There are many sulci and gyri on the surface of the brain, and it is these sulci and gyri that divide the brain into four brain regions. Specifically, the central sulcus, the parieto-occipital fissure, and the lateral fissure divide the brain into the frontal, parietal, occipital, and temporal lobes. The temporal lobe is dominated by auditory functions, the occipital lobe is dominated by visual functions, the parietal lobe is the higher center of somatosensory functions, and the frontal lobe is dominated by somatic motor functions. The contact area between the prefrontal cortex and the temporal, parietal, and occipital cortices is related to higher brain activities such as complex perception, attention, and thinking. The thickness of the cerebral cortex is very thin, only 2.5 mm on average, and its outermost layer is a dark structure, which is the cell body of the nerve cells, also called gray matter, and the area where we collect EEG signals. Since the axons are wrapped in a light-colored myelin sheath, they are also called white matter. The higher center that governs our actions is the cerebral cortex, or gray matter. The bioelectricity that can be captured by EEG is the firing of neurons in the gray matter, which allows us to explore the workings of the gray matter, as shown in Figure 5.
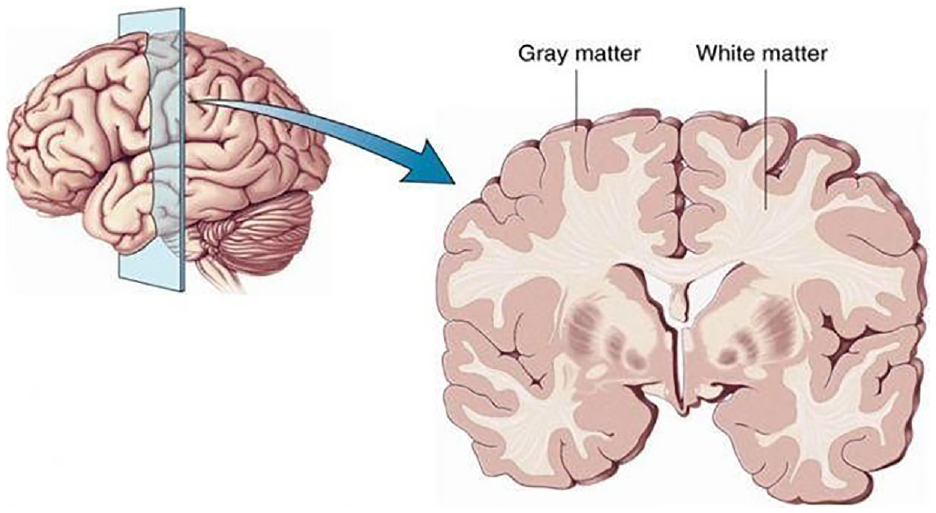
The gray and white matter of the brain.
The main modality currently used for the study of human EEG signals is non-implantable. 86 Non-implantable acquisition includes modalities such as magnetoencephalography, electroencephalography, and functional magnetic resonance imaging. The modality used in this study is EEG, which has a high temporal resolution of the acquired signal, a relatively simple acquisition process, and inexpensive equipment. 87 EEG acquisition is divided into dry electrode acquisition and wet electrode acquisition depending on the equipment, where the wet electrode acquisition has stable impedance and high signal quality, but is cumbersome and has a long preparation time due to the need to apply conductive paste. The dry electrode approach does not require the application of conductive paste, is simple to operate and has a short preparation time. For the population facing the study, dry electrode acquisition of EEG signals is commonly used in the field of EEG-controlled hand rehabilitation robots. However, the technique is highly sensitive to noise to the extent that it is difficult to filter out the interference components of the data. Also using EEG as a brain-machine interface requires a lot of training before the device can work properly and efficiently. So, the problem of EEG signal classification has been a kind of focus and difficulty in the development and design of brain-computer interfaces.
At present, EEG control strategies based on manual action pattern recognition are mainly studied at home and abroad to realize the control of multi-degree-of-freedom rehabilitation robots, 88 as shown in Figure 6.

Process based on EEG control.
Randazz et al. 49 of the Swiss federal Institute of Technology in Lausanne designed the mano flexible underdriven rehabilitation robot for daily living activities assistance and neuro-rehabilitation of patients. Patients need to wear an EEG helmet for EEG signal acquisition and use only EEG to decode the motor representations, which in turn control the exoskeleton hand. The mano exoskeleton provided an ecological way to induce natural hand movements. By coupling the device to a transparent control interface, the system can be used to translate motor intent into realistic hand movements, thus providing rich and coherent proprioceptive feedback to the wearer and thus re-establishing a closed sensorimotor circuit for the user. These approaches are promising in terms of stimulating neuroplasticity and recovery in patients with motor disorders as well as enabling transparent human-computer interaction in everyday scenarios. A rendering of a subject using Mano is shown in Figure 7(a).

Li et al. 50 of Xi’an Jiaotong University invented an attention-controlled hand exoskeleton for restoring finger extension and flexion using a combined hard-soft mechanism, as shown in Figure 7(b). Active rehabilitation was achieved by using an attentional value threshold measured by an electroencephalography (EEG) sensor as a brain-controlled switch for the hand exoskeleton. The performance of the attention value-based visually guided hand exoskeleton switch was experimentally evaluated with an overall activation rate of 95.54%. Based on the success rate of the hand exoskeleton attention-based control experiments, it is clear that the general thresholds perform as well as the customized thresholds.
It is believed that the possibility of providing patients with real-time feedback about their ongoing cortical activity in neurorehabilitation scenarios may be a more effective strategy for triggering brain plasticity and promoting motor recovery by practicing and rewarding Hebbian processes.89,90 According to the above two kinds of hand rehabilitation robotic devices for intention recognition control by EEG signals, it is obvious that EEG signals can achieve the intention recognition control function, but because EEG signals have strong random and non-smooth characteristics. In order to identify the patient’s movement intention, the required effective signal needs to be analyzed and extracted, and currently, there are many methods for such problems at home and abroad, including Fourier transform EEG signal analysis, time domain analysis techniques, frequency domain analysis techniques, time-frequency analysis techniques analysis, nonlinear dynamic analysis, artificial neural networks, etc. 91 The application of brain-computer interface technology on rehabilitation platform is an interdisciplinary research field involving neuroscience, biomedicine, signal processing, circuits and systems, computer programming, communication technology, mechanical design, rehabilitation medicine, etc. It is a complex and young cutting-edge technology field.
Electrooculography (EOG)
The eye is an important organ of the human body and also the most important way in which humans and animals can obtain information about external things, and eye movements are an essential part of the eye in information processing. 92 Electrooculography (EOG) is a bioelectrical signal recorded by electrodes. It is formed by the potential difference between the retina and cornea of the eye, and its amplitude is generally between 0.4 and 10 mV. EOG is triggered by eye movements and is closely related to the thinking activity of the brain, and has the advantages of easy acquisition, easy recognition, and distinct time-domain characteristics. Compared with EEG signal acquisition, there are fewer channels used for EOG signal acquisition and the EOG signal pattern is simple, so the processing method of EOG signal is also relatively simple. The process of EEG signal processing is roughly divided into three parts: pre-processing, feature extraction, and classification recognition. The number of patients with limb movement control disorders caused by stroke, traffic accidents, and other reasons is increasing, but most of them still retain the full motor ability of the eyes. Therefore, EOG can also be a bridge for patients with limb movement control disorders to independently communicate with the outside world by their own ideas and furthermore to control the rehabilitation robotic devices to perform their daily life behaviors. In 2012, a team from Jadavpur University in India designed a single-channel detection EOG-based system that uses the horizontal movement of the eye to control the forward and steering of a motorized trolley in real time, and thus achieve the purpose of controlling a motorized wheelchair using human eye movements. 93 In the past decades, EOG-based control systems have made important progress, which not only can effectively improve the living conditions of patients with limb movement control disorders, but also have great significance for building a harmonious society. However, the system still has some limitations: in practical operation, EOG measurement requires expensive equipment; there are many external disturbances affecting EOG acquisition, and the collected EOG contains more artifacts, and the process of EOG acquisition and analysis is more complicated; most of the existing EOG techniques study the state of eye movement in the horizontal direction, and the state of eye movement in the vertical direction is easily affected by eyelid movement artifacts The existing EOG techniques mostly study the horizontal eye movement state, and the vertical eye movement state is highly susceptible to eyelid motion artifacts, so there are fewer studies, 94 and the precise problem of extracting feature information from the collected EOG remains to be solved. Therefore, although the research on EOG has made great development, further exploration and research are still needed. Fusion of bio-signals associated with eye movements and noninvasive recording of brain activity has been suggested in recent years. 95
The above three bioelectric signal control methods have their own advantages and disadvantages. In some high-level articles, researchers have combined the required functions of the hand rehabilitation robot and selected the appropriate control method or combined two of the bioelectrical signal control methods to obtain the optimal control system. For example, Soekadar et al. 31 published three papers, in 2014, 2015, and 2016, describing a novel brain/neuro-computer interaction (BNCI) system for controlling a hand exoskeleton robot that integrates electroencephalography (EEG) and electrooculography (EOG). Brain-computer interfaces (BMI) are developed to translate electronic or metabolic brain activity into control signals for machines or robots. Non-invasive BMI techniques may be a possible alternative, but do not achieve high reliability and are susceptible to signal artifacts, especially in everyday life settings. The fusion of biological signals related to eye movements works better. A hybrid system fusing biological signals from different sources (e.g., EEG and EOG) could achieve better performance in controlling the hand exoskeleton compared to a system using brain signals alone. A validation experimental paper of this system, also published in the journal science robotics, demonstrated that the use of this hybrid EEG/EOG-based BNCI system enabled the patient to regain full independence in daily life. Recent advances have shown that a transparent interface with the central and peripheral nervous system can be achieved by combining various electrophysiological signals (e.g., EEG, EMG, EEG), and this aspect is promising. Overall, future research should investigate this hybrid bioelectrical signal control system, as such systems can largely improve the applicability of assistive devices in real-life scenarios.
Current status of development of commercial intelligent controlled hand rehabilitation robots
This section contains a summary of the existing intelligently controlled hand rehabilitation robots found in the literature. There are several designs, all of which contain some typical intelligent control systems to improve the technology. These designs are reviewed to highlight the features and limitations of intelligent control systems. And it contains intelligent controlled hand rehabilitation robots (e.g., non-biosignal and bioelectrical signal control approaches) and their applications and contributions, not all listed designs. Table 3 summarizes the recent representative intelligent controlled hand rehabilitation robots and their characteristics.
Overview of recent representative intelligent controlled hand rehabilitation robots and their characteristics.

These recent developments in intelligently controlled hand rehabilitation robots offer a variety of interaction methods to improve the quality of life and work for a wide range of people, and can play a major role in assistive and rehabilitation processes for a wide range of people. Unlike traditional industrial robots, the design and control of hand rehabilitation robots must take into account factors such as human safety, naturalness of operation, predictability of intent, system efficacy, operator acceptability, and active participation, while achieving basic functionality.
Jo et al
In this paper, a wearable and force-controllable hand exoskeleton system is proposed. 110 In order to apply force feedback to the fingertip while allowing natural finger motions, the exoskeleton linkage structure with three degrees of freedom (DOFs) was designed, which was inspired by the muscular skeletal structure of the finger. Kinematic performance of the proposed linkage structure was verified by comparing with functional range of motion (ROM) which is required for activities in daily living. As an actuating system, a series elastic actuator (SEA) mechanism, which consisted of a small linear motor, a manually designed motor driver, a spring and potentiometers, was applied. Friction of the motor was identified and compensated to obtain a linearized model of the actuating system. Using a linear quadratic (LQ) tuned proportional-derivative (PD) controller and a disturbance observer (DOB), the proposed actuator module could generate the desired force accurately even with arbitrary finger movement. The performance of force transmission through linkage structure was verified by simulation and experiments. The proposed exoskeleton structure, actuator modules, and control algorithms were integrated as a wearable and force-controllable hand exoskeleton system that could deliver force to the fingertips for flexion/extension motions.
Kang et al
This paper presents the development of a polymer-based tendon-driven wearable robotic hand, Exo-Glove Poly. 43 Unlike the previously developed Exo-Glove, a fabric-based tendon-driven wearable robotic hand, Exo-Glove Poly was developed using silicone to allow for sanitization between users in multiple-user environments such as hospitals. Exo-Glove Poly was developed to use two motors, one for the thumb and the other for the index/middle finger, and an under actuation mechanism to grasp various objects. In order to realize Exo-Glove Poly, design features and fabrication processes were developed to permit adjustment to different hand sizes, to protect users from injury, to enable ventilation, and to embed Teflon tubes for the wire paths. The mechanical properties of Exo-Glove Poly were verified with a healthy subject through a wrap grasp experiment using a mat-type pressure sensor and an under actuation performance experiment with a specialized test set-up. Finally, performance of the Exo-Glove Poly for grasping various shapes of object was verified, including objects needing under-actuation.
Park et al
In this paper, a hand exoskeleton system for virtual reality is proposed. 42 As a virtual reality interface for the hand, a wearable system should be able to measure finger joint angles and apply force feedback to the fingers with a simple and light design. In the proposed system, the finger joint angles are measured by a tendon-inspired cable mechanism. Also, another cable is used for force feedback to the finger. Using the measured finger joint angles and motor currents, the cable driven actuation system applies desired force to the fingers. That is, when the desired force is zero, the motor position is controlled to track the changed cable length; when the desired force needs to be applied, the motor current is controlled to generate the desired force. For a smooth transition between two control strategies, linearly changing proportions of each control strategy is applied in the transition range. A prototype of the proposed system was manufactured, and the proposed control algorithms were verified by experiments.
Diftler et al
The Robo-Glove is an assistive device that can augment human strength, endurance or provide directed motion for use in rehabilitation. 41 Robo-Glove is a spinoff of the highly successful Robo-naut 2 (R2) system developed as part of a partnership between General Motors and NASA. This extremely lightweight device employs an actuator system based on the R2 finger drive system to transfer part or the entire grasp load from human tendons to artificial ones contained in the glove. Steady state loads ranging from 15 to 20 lbs and peaks approaching 50 lbs are achievable. Work is underway to integrate the Robo-Glove system with a space suit glove to add strength or reduce fatigue during spacewalks. Tactile sensing, miniaturized electronics, and on-board processing provide sufficient flexibility for applications in many industries. Robo-Glove uses five sensors and supportive palm inserts inside, it is like an exoskeleton that mimics the way the hand and fingers move. The Robo-Glove covers the entire forearm, with actuators in the upper part and pressure sensors in the finger position. When it detects that the user is gripping an object and finger pressure increases, it will function as an additional artificial tendon to strengthen the grip at least two times.
Zhang et al
Zhang et al. 103 proposed an exoskeleton for the hand with the aim of rehabilitating the injured hand. The exoskeleton is designed as a wearable device and each finger has three joints named the metacarpophalangeal (MCP) joint, the proximal interphalangeal (PIP) joint, and the distal interphalangeal (DIP) joint which all employ a novel mechanism called “circuitous joint.” Adopting a symmetrical pinion and rack with a parallel sliding mechanism, the circuitous joint can cover a wide workspace of the finger and adapt to fingers of different thicknesses. And the parallel sliding mechanism ensures that the contact force between the exoskeleton and the finger is perpendicular to the finger’s bone, which can minimize the secondary injuries. Moreover, the Bowden cable driving method reduces the burden on the fingers by placing the driving and control system on the forearm. Lastly, hand fitness test and contact force experiment are conducted and the results verify the rationality and effectiveness of the exoskeleton.
Nilsson et al
This paper introduces the SEM Glove (Soft Extra Muscle Glove), a comfortable aid which automatically improves the grasping capability of a human independently of the particular task being performed. 100 The actuation unit includes a DC motor that is connected to a lead screw and nut, which in turn transmits the bending and extension of the specified fingers through a cable. The glove actuates only the thumb, middle, and ring fingers via the drive unit located in a wearable satchel on the patient’s back. The control system for the SEM glove is based on the input for the tactile sensors in the fingertips and the force sensor in the palm as well as the wearers own voluntary control of the grip.
Agarwal et al
This paper presents a novel index finger exoskeleton with Bowden cable-based tandem elastic actuation that allows bidirectional torque control of the device with high counter drive and low reflective inertia. 109 And an exoskeleton and finger joint torque controller, as well as an optimization-based offline parameter estimator, are proposed. The device can be controlled to provide minimal resistance to finger movements. In addition to its current application as an exoskeleton for hand rehabilitation, the device has the potential to be used as a haptic device for teleoperation.
Heo
This paper presents a powered finger exoskeleton with an open fingerpad, named the Open Fingerpad eXoskeleton (OFX). 107 The palm opening in the finger plate allows the user’s finger plate to come into direct contact with the object for dexterous manipulation using the wearer’s own sense of touch. The device is driven by a cylinder that applies an assisted force measured by the fingertip gripper. A load sensor is located at the tip of the distal phalanx, which is uniquely constructed to leave the user’s finger plate open. The device is characterized by actuation of the index finger and thumb. And the authors used the sEMG as a sensor to measure muscle fatigue during manipulation.
Tjahyono et al
This is a five-finger hand exoskeleton driven by pneumatic artificial muscles 101 with a unique approach to strain sensors for rehabilitation and assistive applications. The requirements of this design were to have a lightweight, low-profile, portable device. The design has 10 pneumatically actuated artificial muscles and a linear actuator to obtain an overall 19 DOF device. The design is a combination of rigid and soft elements. The artificial muscles are connected to tendon cables which in turn flex the designated fingers when actuated. A linear spring provides a counter extension force for each finger. The control of the device utilizes position and force control and regulates the pressure on the muscle via a solenoid valve. The authors created a new strain sensor that utilizes NR and PPy to measure the linear actuation of the PAMs. The position of the finger is determined by deformation. This is an innovative step in exoskeleton technology for the hand.
Discussion
The objectives of this paper are (i) to review the theoretical basis of stroke hand rehabilitation, (ii) to provide an overview focusing on the classification of intelligent control strategies, and (iii) to summarize the current status of development of commercial intelligent controlled hand rehabilitation robots in recent years. The results show that in the existing research of intelligent controlled hand rehabilitation robots, it is important to focus not only on the mechanical structure part, but most importantly on the intelligent control system aspect of hand rehabilitation robots in order to obtain the best hand rehabilitation results. We have summarized the previous discussion in order of the purpose of the review. When designing an intelligently controlled hand rehabilitation robot, it is easy to ignore the recovery phase of the patient’s hand, which leads to the separation of the device from the medical rehabilitation theory. So that the final design of the hand rehabilitation robot is not applicable to the recovery of the patient’s hand motor function. Therefore, we believe it is important to start with the theory of hand rehabilitation in stroke patients and then proceed to discuss different intelligent control strategies corresponding to different recovery stages. These recent developments in intelligently controlled hand rehabilitation robots provide multiple methods of interaction to improve the quality of life and work for a wide range of people and can play an important role in the assistive and rehabilitative process for a wide range of people. In particular, commercialized hand rehabilitation robots cannot be separated from clinical trials. A successful technology needs to undergo extensive controlled trials before it can be quickly brought to market.
In the face of the severe situation of aging population and the large number of stroke and hemiplegia patients, the research of functional hand rehabilitation robots will re-emerge as a relatively cutting-edge and popular field for in-depth exploration in recent years and in the coming decades. The current commercially available intelligent control methods remain a critical and difficult issue in this field. Based on the summary of this paper, intelligent control approaches for hand rehabilitation robots still have much to improve and enhance in future research.
1. Combine the theoretical basis of hand rehabilitation in stroke.
Combining the relevant clinical medical theories to design the hand rehabilitation robot, we designed the robot to meet the biological characteristics and kinematic features of human hand while stimulating the neuroplasticity of the brain to achieve the optimal hand rehabilitation robot training effect.
2. Combined with human bioelectrical signals.
This intelligent control not only enables the prediction of the patient’s motor intention, but also induces stimulation of neuroplasticity in the brain.
3. Fusion of different bioelectrical signals.
Future research should investigate such hybrid bioelectrical signal control systems, as such systems can greatly improve the applicability of assistive devices in real-life situations.
In order to optimize the difficult trade-off between functionality and usability of typical hand rehabilitation robots in everyday life, we have identified three future directions that are of great interest as described above. Future work should include several of these directions of development as a way to address the specific needs and desires of users of intelligent control devices.
Conclusions
The purpose of this review is to systematically review the theoretical foundations of stroke hand rehabilitation, focusing on an overview of the classification of intelligent control strategies and briefly summarizing the current state of development of commercial intelligent controlled hand rehabilitation robots in recent years. It is hoped that it will be useful to researchers in this research area. This review summarizes the techniques in this paper in a systematic way. Specifically, we provide an overview of the theoretical basis of stroke hand rehabilitation in the reviewed literature, and commercial intelligent controlled hand rehabilitation robots in recent years. Finally, we discuss the future directions of intelligent controlled hand rehabilitation robots. The results show that the development trend in recent years is more inclined to: combining the theoretical basis of stroke hand rehabilitation and studying intelligent control methods of hand function rehabilitation robots that combine human bioelectrical signals to achieve prediction of patients’ motor intentions and also induced stimulation of neuroplasticity in the brain. As well as fusing different bioelectrical signals as a way to improve the applicability of the assistive device in real life. This paper will help researchers to understand the current state of the art regarding intelligently controlled hand rehabilitation robotics after stroke in recent years.
Footnotes
Handling Editor: Chenhui Liang
Author contributions
Conceptualization, HY and KG; methodology, CL; writing—original draft preparation, CL, JL, and KG; writing—review and editing, KG and CL; supervision, HY; project administration, KG; funding acquisition, HY. All authors have read and agreed to the published version of the manuscript. CL and KG contribute the same to this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Key Research and Development Program of Jiangsu Province (Grant No. BE2021012-1) and the International Partnership Program of the Chinese Academy of Science (Grant No. 154232KYSB20200016).
Informed consent statement
Informed consent was obtained from all subjects involved in the study.
Data availability statement
The data presented in this study are available on request from the corresponding author.