
Abstract
This article aims to give an overall review of research status in hand rehabilitation robotic technology, evaluating a number of devices. The main scope is to explore the current state of art to help and support designers and clinicians make better choices among varied devices and components. The review also focuses on both mechanical design, usability and training paradigms since these parts are interconnected for an effective hand recovery. In order to study the rehabilitation robotic technology status, the devices have been divided in two categories: end-effector robots and exoskeleton devices. The end-effector robots are more flexible than exoskeleton devices in fitting the different size of hands, reducing the setup time and increasing the usability for new patients. They suffer from the control of distal joints and haptic aspects of object manipulation. In this way, exoskeleton devices may represent a new opportunity. Nevertheless their design is complex and a deep investigation of hand biomechanics and physical human–robot interaction is required. The main hand exoskeletons have been developed in the last decade and the results are promising demonstrated by the growth of the commercialized devices. Finally, a discussion on the complexity to define which design is better and more effective than the other one is summarized for future investigations.
Introduction
Over the past years, rehabilitation engineering has played a crucial role in improving the hand and finger function after stroke. The applications of robotics and mechatronic devices have rapidly expanded from the industrial environment to human assistance in rehabilitation and functional improvements. Rehabilitation engineering has increased the quality lives of individuals with disabilities, offering dedicated training that performs better than conventional methods.
In this way, there are many challenges and opportunities to integrate engineering concepts into hand rehabilitation, and increasing population wellbeing and wealth as well as reducing healthcare costs. This motivates researchers to study, design, and develop novel rehabilitative and assistive technologies and devices to help people to motor functions. Specifically, the current challenge is to transfer the research results and new knowledge to stakeholders creating a general awareness of the importance of rehabilitation engineering.
This review aims to present and discuss the main robotic technologies for hand recovery rehabilitation in stroke survivors, evaluating and comparing previous and current works and researches. This study explores the current state of art to help and support designers and clinicians make better choices among varied devices and components. The review also focuses on both mechanical design (e.g. concept), usability (e.g. setup, lightness, portability) and training paradigms (e.g. hand, hand/wrist or entire arm) since these parts are interconnected for an effective hand recovery. An overview of the main advantages and drawbacks in applying robotics to hand motor impairments is provided in order to give a general view of the relationship between hand rehabilitation devices, rehabilitation theories and results. The challenge is to restore the hand movements such as opening, closing, grasping and releasing movements. Second, a discussion on the application and new challenges of rehabilitation robotic devices is summarized for future investigations. In particular, the main challenges are to develop safe devices with less complex designs, increasing potential for portability and efficacy. In fact, future development for patient treatment should include the device portability to increase the potential applications. The preliminary results have highlighted the robot-assisted therapy currently works hand in hand rather than a replacement of traditional therapy. Therapies and rehabilitation strategies should be not only more effective but also more cost-efficient.
Stroke is one of the leading causes of long-term disability, affecting approximately 14% of world’s population.1,2 33% of survivors reports very limited or no functional use of the upper limb. 3 Rehabilitation activities based on repeated exercises have been identified suitable in recovering some degree of motion, in particular, a simple flexion and extension of fingers has demonstrated improvements in hand functionality.4,5 In this way, medical devices and robot-assisted strategies may provide a number of advantages guaranteeing the range of motion (ROM) and avoiding inappropriate movements. Nevertheless, only a limited part of the proposed devices by the literature has been clinically tested, highlighting as the design complexity and development costs may negatively impact the system implementation. The previous and current robots and devices are often too complex to be used by patients limiting any testing on the real users.
Note that the hand functional improvement may be the result of a set of compensatory strategies based on an initial support assisted by the physiotherapist. Usually, these approaches may be suggested during the first months after stroke, when the impairment reduction may be preferred to extensive functional training. In this phase of impairment, the patients show a loss of control and a decreased tactile sensation and proprioception, reducing the physical independence and social integration. The patient’s motivation associated with verbal encouragement may significantly impact the therapy efficacy.
Over the last decades, a set of studies has evaluated the influence of the robot-assisted therapies on arm motor improvement and impairment reduction using randomized clinical controlled trials.6–12 The obtained results have not shown a complete consensus; nevertheless, the therapy assisted by robotics seems to obtain results beyond what is done by conventional methods.13–17 In particular, researchers have been slow to investigate the hand function due to the complexity of this limb.11,12,18–20
In any case, a number of studies observed that the rehabilitation training can improve the hand motor in terms of pull, push, and grip strengths, confirming that robotic training is at least as effective as conventional training.13,21–24 A significant part of the obtained outcomes have been also proved by Fugl-Meyer Assessment (FMA) and Functional Independence Measure (FIM) tests, performed after the robot treatment.25–27
Despite these promising results, the literature review shows also researches that did not observed significant difference between conventional and robotic training groups, highlighting as the conventional therapies are more effective in decreasing levels of impairment and disability.2,8,28,29 Mazzoleni et al. 29 and Colombo et al. 30 have underlined that there are other significant factors that may impact the efficacy of the training outcome, such as recovery stage, intensity, or duration of the rehabilitation therapy. This point needs to be considered to evaluate and compare different therapy treatments. In the light of these considerations, there are not evident conclusions that sustain the robot-therapy efficacy, suggesting further investigations.31,32
Advantages and limits of robot-assisted therapy
Robot-based methods may be used independently by patients in different levels of impairment. Robots permit to obtain a quantifiable measure of subjective performance, repeating treatment protocols without the need of continuous involvement of therapists saving a significant amount of the human labor that may lead to high cost.8,10 In fact, traditional therapist–based methods require several sessions of rehabilitation training, inducing impractical and unaffordable therapies for many patients. Robotic therapy techniques guarantee a safe, intensive, and task-oriented rehabilitation at relatively moderate costs.14,15–33 They may apply forces with precision, improving accuracy and reducing variance. These actions are potentially effective to strengthen muscle, ROM, and motor coordination. Advanced robots provide also tactile feedback that may correct the impaired movements. In addition, robot-assisted therapies may be quantified easily and collect a number of parameters useful to track the patient’s status (e.g. spasticity or level of voluntary control). 34
A further advantage of robotic rehabilitation consists of the possibility to be combined with other technologies (e.g. virtual reality (VR), brain computer interface (BCI) technology or haptic stimuli).35–37 This combination allows to motivate the patients to perform the rehabilitation tasks without the constant supervision, guaranteeing repetitive movements and informative feedback. On the other hand, robot-assisted therapy permits the therapist to conduct rehabilitation tasks for two or more patients at the same time, improving the service efficiency.
Finally, it has been noted that robotics may improve the accessibility to rehabilitation. In fact, a patient prefers to use the unaffected limb in daily activities, damaging the recovery of the impaired limb. 38 The possibility to perform rehabilitation in remote locations (e.g. home) using robotics devices may involve better the patient in the recovery process.
Despite these noted advantages, a number of limits and constraints of rehabilitation robot-based cannot be ignored. First, there is a significant gap between the outcomes of rehabilitation robots and people’s expectations. This element may negatively impact patient’s motivations during the therapy. In particular, the personalization is still difficult due to the design complexity of devices. Another further issue is the determination of the most efficient dosage of rehabilitation training.
Although the literature has demonstrated the main advantages and benefits of robot applications, more studies involving a large participant size are required to confirm whether robotic-assisted therapy performs better than conventional methods, evaluating and comparing the treatment dosage. In particular, a lack of robust methods to evaluate the efficacy of the robot-assisted therapy making difficult to define which design is better and more effective than the other one. A deep investigation is needed to explore whether the obtained results on the patient can be maintained in the long term and how the potential improvements can be transformed into the motor skills in performing the activities of daily living (ADL). The user’s safety needs to be guaranteed during the training, avoiding the nonlinear movement of the patient. Further limits are noted on the current robotic devices regarding their design, often complex and unconvinced for the user, or the high costs for the treatment access.39–41 The ratio between the price and performance is rather dissatisfactory due to the high cost of development combined with a relatively benefit for patients and clinics.42–44 These drawbacks need to be considered in the overall evaluation of robotic application. They represent an open challenge to improve the integration of engineering concepts into hand rehabilitation, increasing population wealth, as well as reducing healthcare costs. These issues justify the low penetration of robotics in the market and the requirements of new investigations. Only a limited number of stroke patients (5%–15%) who requires assistive devices and technologies may access to this service. On the other hand, the studies and researches on rehabilitation robots are becoming strategic for the society due to the fact that the costs of excluding people with disabilities are high and borne by community. 45
Rehabilitation robotic devices for hand recovery
A primary categorization of rehabilitation robotic technologies is based on the design concepts of the device: end-effector or exoskeleton.
An end-effector device (also called endpoint control) recreates dynamic environments corresponding to ADL, determining the movements at the joint level. Usually, the patient’s joint rotation is distally executed using a support (e.g. a table or a tripod) to facilitate the training and avoiding muscle fatigue. It means that the more proximal joints are not directly controlled by the robot. End-effector devices may be dedicated to hand rehabilitation or to be integrated in more complex structures for the arm recovery.
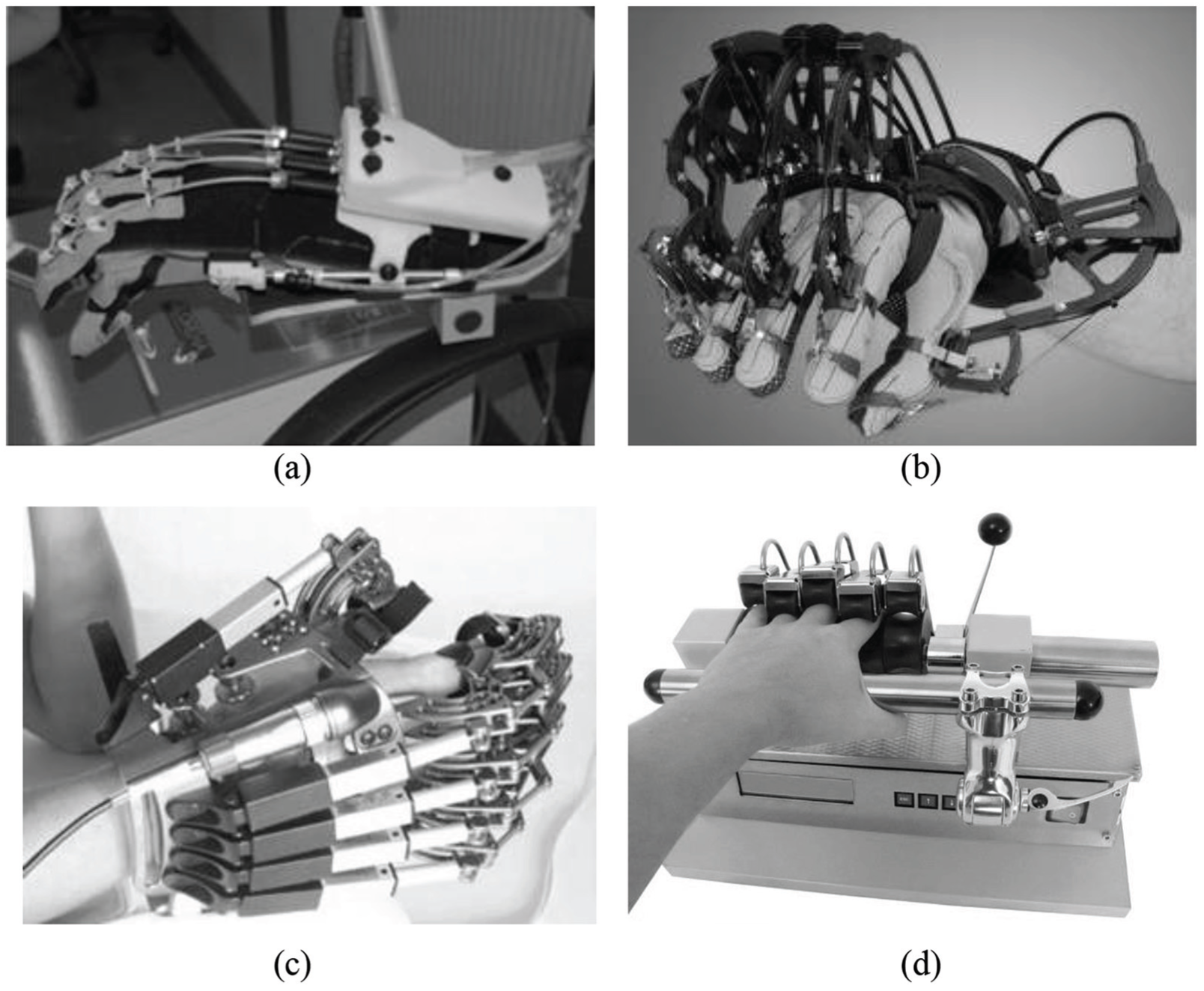
The second main logic to design a rehabilitation robotic device is the exoskeleton. An exoskeleton, from Greek “exo” = outer and “skeletos” = skeleton, is a wearable robot attached to the user’s limbs, in order to enhance their movements. It focuses on the anatomy of the subject’s hand following the limb segments, each degree of freedom is aligned with the corresponding human joint. Figure 1 illustrates a number of examples. An exoskeleton should be compliant with the user’s movements and delivers at least part of the power required by the movements. In order to guarantee the natural motor of the hand joints, their design is more complex than end-effector devices. For example, a set of components (e.g. rings, hinges, external linkages, or structures) is embedded to accomplish the alignment between the forearm axial rotation of the forearm located along an axis between the ulna and the radius50,51 to support in forearm pronation and supination.
Comparing these two different approaches, it is noted that an end-effector robot is more flexible than an exoskeleton device in fitting the different sizes of hands, reducing the setup time and increasing the usability for new patients. In addition, end-effector mechanisms are also generally ambidextrous. Exoskeletons, on the contrary, need to be adjusted to fit different sizes of hand due to its complexity, and, as a consequence, the geometric parameters also need to be updated in the controller to guarantee the accuracy of the kinematic models. However, the end-effector robots suffer from limited control of the proximal joints of the limb, which could result in abnormal movement patterns. In contrast, an exoskeleton device controls the individual joints directly, minimizing abnormal posture or movement. Due to the complexity of construction, an exoskeleton device is generally more expensive than an end-effector type. 52
Rehabilitation robotic devices may be also categorized into passive and active devices. A robot provides a passive movement when there is not voluntary muscular contraction by the individual. In this case, the robotic device has a dominant role and leads the movement during grasping, reaching, or holding objects. The active mode is adopted when the patient has some levels of control, and the robot assists the user in the correct movement execution. The patient applies the forces in a preferred path, and the robot supports the user only as much as needed to accomplish the task along the workspace. Note that active movements also have a beneficial impact to reorganize the brain neuro-connectivity.
The literature reports different robots that are able to provide continuous passive motion (CPM). This type of robots supports and helps the patient to reduce joint stiffness of the fingers, but suffers from the possibility to develop the active movements of fingers.53,54
Over the last years, a significant number of active robotic devices have been studied and commercialized in order to train hand function with active participation of the patient. A further classification may be based on the type applications of the robot devices:
Robots dedicated to hand function rehabilitation. They aim to train specific hand functions (e.g. opening, closing, grasping, and releasing movements). HWARD (3 degrees of freedom (DOF)) 54 and Haptic Knob (2 DOF)55–57 are two examples of this type of application. Usually, these devices offer a high force and ROM; however, they are not able to move each finger independently.
Additional hand modules. They are designed to be integrated in robotic structures used for the arm rehabilitation (e.g. shoulder, elbow or wrist). Examples of this concept are the Hand Robot Alpha-Prototype II, added as the output of the MIT-MANUS, 58 or the extension of the ARMin device that uses a semi exoskeleton system, designed to insert the hand inside a device. 53
Robots focused on rehabilitation of fingers individually. These types of devices are based on gloves or robotic exoskeleton structure. For example, the Rutgers Master II, 59 or the new improved design, is based on an internal mechanism where the pneumatic direct drive actuators are placed in the palm of the user. The applied forces at the distal phalanx are propagated to all the joints. However, grasping tasks is not completely performed using physical objects for rehabilitation. A further example of this type of logic is the CyberGrasp (Figure 1b) exoskeleton which provides a full ROM of the hand without restricting movements. It exerts unidirectional forces to oppose the finger flexion fitting using a glove.60–62
End-effector robotic devices
Several robotic devices have been developed and commercialized using the end-effector logic. This approach may be used to train specific hand functions, but also to control each digit individually. This review considers the main devices that are presented in the literature with clinical tests or some experimental results. Table 1 lists a set of robotic devices, including those end-effector systems that are commercially available.
End-effector devices for hand rehabilitation.

DOF: degrees of freedom; ROM: range of motion; ADL: activities of daily living.
Commercially available.
One of the first end-effector devices was the Rutgers Master II, introduced by Bouzit et al. 59 It is a dedicated haptic device based on pneumatic actuators mounted on the hand palm to move each finger except the little finger, individually or together.
This device has 4 DOF. The internal mechanism limits the ROM of the robot, and a set of movements (e.g. grasping using physical objects) is not completely executed. This robot has been clinically tested and the results showed positive gains in movement parameters, such as movement speed and ROM. A further example of device dedicated to finger rehabilitation is the Reha Digit. Hesse et al. 63 developed this electromechanical finger trainer to move every finger except the thumb. This device is suitable to perform only passive operations. The user’s fingers are located in four plastic rollers, while other two rotors are placed on top of each finger. The robot is ambidextrous and it has 4 DOF. Although the robot is easy to use, the experimental tests have not shown significant gains of ADL performance and the clinical results have been partial.
An interesting commercial device that is capable of moving each finger in flexion and extension is Amadeo. 64 This is a passive robotic device with 5 DOF. The system is applied to the finger tips that are moved along fixed trajectories. The clinical validation highlighted promising results, the outcome of a set of studies showed an improvement in joint, grasping and pinching power of hand and wrist using FMA and Jebsen-Taylor test.6,65,66 This device is not well adapted for patients with spasticity.
In the same way, there are several devices that propose CPM using “end point control.” These types of devices may be applied to the hand by a brace and move the tips of the fingers, pulling them up to open the hand, and then reversing the movement. Examples of commercial CPM devices, including exoskeleton devices, are the Maestra Hand and the Wrist CPM, the Maestra Portable and the DigiGlide.
The end-effector approach has also been used to design the Haptic Knob. It has 2 DOF and it is able to perform a broad range of grasps, grips, and pinches. It focuses on increasing control and strength of grasping, improving forearm pronation and supination range, and training coordination of different degrees of freedom. The structure consists of two parallelograms to train opening and closing movements (such as an umbrella works). The patient’s fingers are placed to the end of the parallelogram links actuated by a motor. The design of the device does not include any support for the forearm or wrist. This element may lead to user discomfort. It has been clinically tested and the outcomes were positive. The motricity indicators of patients improved significantly at end of therapy. In particular, this device is also suitable for wrist and forearm recovery.
In the same way, Dovat et al. 67 introduced the HandCARE, a rehabilitation robot that assists a patient in hand opening and closing movements and offers a variety of training possibilities. Thus, the objective is to train finger extension and flexion individually, improving the capacity to control the forces generated by each finger and the coordination between fingers while performing a grasping task. The device is a cable-actuated robot and it has 5 DOF. It works under the principle of the linear movement of the fingers linked to a cable. The robot assists or resists the patient in finger extension and flexion movements. The literature shows partial results of the experimental tests executed to a small group of participants. Nevertheless, the outcomes of the performed tests were promising and positive with a gain in coordination and independence of the fingers. 26 As the Haptic Knob, the HandCARE is a compact robot, easy to use and setup. It could easily be integrated into a domestic environment to provide home rehabilitation.
Other examples of devices that focus on training wrist and hand functions are the BiManu Track and the ReachMAN. 54 The BiManu Track is a commercialized device with 1 DOF that may separately assist flexion and extension of the wrist and pronation and supination of the forearm. The design is based on the principle of the bilateral training. The device is composed of two handles actuated with a master-slave system based on the motion of the healthy limb. The BiManu Track is a portable device with two motors able to perform torques of up to 5 N m. This system allows forearm and wrist movement but it is not able to train grasping and fine finger motion. Several tests have been executed to assess the device performance. A first test on a small group of patients showed an improvement of muscle tone in the major part of the participants, however, without significant functional performances in ADLs. A second study involving 44 subacute stroke patients and comparing the BiManu Track with electric stimulation therapy highlighted FMA improved in both groups.68–70
In contrast to the previously described robots, a number of devices have been designed to be integrated in more complex structures in order to create a robot capable of training the entire arm and hand function. Loureiro et al. developed the GENTLE/G system, composed of a wrist-orthosis connected to the HapticMaster robot (3 active DOF), that may train in three-dimensional virtual environment, with the possibility of compensating for the weight of the arm.
The wrist-orthosis has three passive DOFs to allow comfortable positioning during movements. A 3-DOF gripper, mounted on the structure, allows to perform key grips, power, and pinch grasps. 71 A further integration of hand devices in a complex robot is the Hand Robot Alpha-Prototype II, developed by Hogan et al. It is an extension of their arm rehabilitation device, the MIT-MANUS. The MIT-MANUS is a commercially available planar 2 DOF robot developed to train arm and shoulder and simulate arm reaching movements. The hand module is a handle fixed at the extremity of the robot. It can provide high force to train grasping and assist hand opening by progressively changing its diameter. This solution may be limited by a small ROM and the inability to train.
Hand exoskeleton robotic devices
In recent years, numerous studies and researchers have been undertaken to identify new solutions for exoskeleton applications; nevertheless, their use is still limited to specific parts of the body. The exoskeleton devices represent a new opportunities for engineering rehabilitation since their DOFs are aligned with the DOFs of the hand joints, improving the patient’s usability and portability. In addition, these devices are able to control the position or torque applied at each joint. This approach guarantees to minimize abnormal hand postures. Table 2 summarizes a number of exoskeleton devices, highlighting those systems are already available on the market. The hand exoskeletons may be passive or active devices. The passive devices do not include any actuator. An example of this application is the HandSOME 74 —a passive, lightweight, and wearable device—that opens the patient’s hand using a series of elastic cords that apply extension torques to the finger joints and compensate for the flexor hypertonia.
Exoskeleton devices for hand rehabilitation.

DOF: degrees of freedom; CPM: continuous passive motion.
Commercially available.
The active category uses a set of actuators to provide CPM or active assistance, where the user hand actively interacts with the device and the device reacts through feedback signal. In this way, the correct identification of actuators, transmission system and sensors play a fundamental role for an effective therapy of the device. In fact, a hand exoskeleton may often suffer from inaccurate torque or impedance control at individual finger joints. In addition, it is required to avoid solutions that make devices bulky, restricting the hand to a stationary device.
Several techniques may be included in the robotic system to assist, actuate, and control the user’s fingers. The literature presents a variety of solutions based on the use of servomotors, directly applied to the exoskeleton joints, 75 cable or linkage mechanisms,72,73 or pneumatic cylinders. 76
There are various criteria to categorize the hand exoskeletons, such as weight, number of active DOF, type of actuator, power transmission method, sensing and control method, or peak achievable forces and torques on the device. Table 2 summarizes and compares the main hand exoskeleton robotic devices published in the literature with the main promising results. This comparison aims at highlighting the variety of solutions that the researches have been studied in the recent years and underlines the achieved results and the challenges to be undertaken.
One of the most cited devices is the CyberGrasp (Figure 1b). The main concept is to avoid the finger flexion motion through the application of unidirectional forces with one actuated. The device is not suitable to control torque applied at finger joints individually. However, its design allows full ROM of the hand without obstructing movements. It uses cables linked to the distal phalanx of each digit and works using a mechanism applied to the back of the hand. Five remote motors control the extension force. The CyberGrasp is integrated in a glove (CyberGlove) that permits the interactions with virtual environments. 77
Schabowsky et al. introduced the HEXORR (The Hand Exoskeleton Rehabilitation Robot) that controls the individual joints of the hand allowing the training of natural joint movements. This device has 2 active DOF and consists of two modules dedicated to fingers and thumb. The finger module is linkage-based and provides the rotations of the metacarpophalangeal (MCP) and the proximal interphalangeal (PIP) joints. An electric motor actuates each module. HEXORR may be used for CPM, active unassisted movement, or force assisted movement. The experimental campaign showed promising results since the force to increase active ROM for the fingers and thumb, respectively. 78 In the HANDEXOS, each finger has three links for the phalanges that correspond with the hand joints. A slider-crank-like mechanism leads the flexion and extension of the MCP joint, while the PIP and distal interphalangeal (DIP) joints are driven by Bowden-cable based mechanisms. This device is equipped by force sensors for interaction and the transmitted force is measured by strain gauges.79,80
In the same way, Li et al. developed the iHandRehab. This device is dedicated to the rehabilitation of the index finger and thumb. It actuates the joints using a cable transmission based on two cables to guarantee the bidirectional movement. Both the index and thumb modules have 4 DOF. This device may work in passive, active, and assisted modes. The interaction forces at the tip of the fingers are measured by a set of sensors. 73
The Gloreha device, Figure 1(a), is another example of the cable application to transmit the required forces for rehabilitation tasks. It is a glove-type system, portable, and lightweight, with five independent motors that provide and combine a variety of motions performing complex exercises. It consists of two modules to transmit the forces. The first module, mounted on the wrist, drives the second module (cable mechanism) linked to the fingers. Forces and movements are transmitted through several elastic transmissions driven by the actuator. This device is particularly suitable for the CPM therapy46,81 The Hand Mentor is a further example of device based on the pneumatic actuation of wrist and fingers. It consists of 1 DOF system able to control the patient’s wrist and fingers through a resistive force. The main performed operations are flexion and extension of the hand. 82 It is commercially available on the market.
Takahashi et al. presented HWARD. This device is based on a pneumatic system able to actuate the grasping and releasing movements of the hand (3 DOF). It allows the rotation of the fingers, thumb, and wrist on their natural axes of motion, guaranteeing a large ROM and force. In fact, the pneumatic actuator delivers up to 15 N of force to open the hand. The clinical tests executed on a set of groups of stroke patients showed an improvement in all measures (FMA scores) in receiving the robotic therapy. Further positive results were noted during magnetic resonance imaging (MRI) analysis. The main drawback is a lack to train each finger independently. In addition, this device shows some issues to be integrated into more complex structures for the entire arm rehabilitation.
As discussed for the end-effector devices, the exoskeletons may be also integrated in more complex structures to assist the rehabilitation of the arm. For example, Riener et al. introduced ARMin, a rehabilitation robot comprising four active DOF allowing shoulder and elbow movement. The robot is equipped by a semi-exoskeletal structure, with the patient’s arm placed inside an orthotic shell. A 2 DOF hand module has been developed to perform rehabilitation tasks of forearm (pronation and supination) and wrist (flexion and extension). 53
Exoskeleton devices may be also applied to hand function assistance. Examples of this application are the devices designed by Hasegawa el al. (11 active DOF, using pneumatic actuators) and Takagi et al. (4 active DOF, using air cylinder with compressed air source).
Tables 2 indicates that a large number of devices uses the cable-based transmission. These solutions are designed to allow free orientation and translation of the hand movements within a large range of physical therapy. Usually, these devices are lightweight and portable due to the use of electric motors for the movement transmission. Despite these advantages, these rehabilitation systems show a number of limits and constraints. In particular, they use the force sensors to control the digit position and to compensate the resistance of friction between cable and inertia moment of finger flexion motion, ignoring other losses in cable transmission. Experimental tests have also shown that this transmission may suffer from the inaccurate measurement of the force. This limit is due to the complexity to apply the sensors that are not able to cover the contact area between the device and the finger completely. In addition, the angle change of the force application increases the control difficulty.83,84 The major part of the proposed devices uses DC electric motors to actuate the system. These motors are reliable and easy to control. However, they require a regular maintenance, with a potential increase of operating costs. They often have heavy armatures compromising the portability and home usability of the devices. An alternative solution may be represented by BLDC motors. These motors are lightweight and no regular maintenance is required.
The actuation of a number of robotic devices consists of pneumatic cylinders, which measure the force exerted on the finger tips by estimating the pressure of the cylinder. This solution shows a few of issues to be controlled effectively. In fact, a pneumatic cylinder has only 1 DOF applied to each finger and it cannot be used to control interaction force or torque at the individual phalanges or joints of the finger. For this reason, any force applied on the distal phalanx is propagated to all the joints without any means to control it individually. This limitation may influence the hand exercise. In particular, the mechanism is located on the palmar side, limiting the rehabilitation tasks based on the grasp of physical objects.
The literature also shows devices that are equipped with geared servomotors. They may be directly located on the system joints or connected through tendons. These solutions require an accurate positioning of the sensors, in fact the control may be difficult due to the losses in the gearing or routing pulleys. These solutions risk to make the device bulky, restricting the hand movement.
In the light of these considerations, the selection of the actuator and its position may determine the device lightness and portability. These points need to be considered with a high priority in the design stage, especially for assistance application. Also, the device technical features (e.g. peak achievable forces or torques) define the application range and the related rehabilitation tasks (e.g. pathologies).
Finally, the control techniques (e.g. force-field control or assist-as-needed control) may influence the identification of the sensors (e.g. position, force) and placement.85,86 In addition, the control strategy selection needs to consider and guarantee the user’s safety, avoiding nonlinear movements of the patient and to maintain the correct trajectory and the force amount during the rehabilitation exercises. There is a variety of modes and levels to control an exoskeleton device. 38 The simplest mode is based on patient monitoring. The robot measures only the user parameters (e.g. tremors) without applying any force. This mode may be useful to understand whether the therapy has improved the hand motor. Usually, the rehabilitation devices applies passive or active control mode. In the passive control mode, the user has not any motor function and the device leads the patient to perform the expected task. In contrasts, the active mode is adopted when the patient has some levels of control, and the robot assists the user in the correct movement execution. The patient applies the forces in a preferred path, and the robot supports the user only as much as needed to accomplish the task along the workspace.
In this way, different control strategies may be implemented based on the therapy and device scope. A number of robotic systems (e.g. MIT-MANUS, MIME, GENTLE) use strategies based on position, force, proportional–integral–derivative (PID) control. These models are easy to be implemented with high reliability. However, they have some limitations in controlling upper extremity movement, lacking of cognitive abilities. Recent studies87–89 have presented other approaches that focus on high-level methods using fuzzy logics or neural network controls. The results are promising to solve the limitations of low-level control system, such as the decision-making process; nevertheless, other problems are noted in terms of adaptability and reliability.
Discussion
Developing robotic devices dedicated to rehabilitation after stroke is a challenging task that covers a broad range of domains at the interface between engineering and medicine. In particular, the hand complexity leads to many difficult decisions in terms of the device concept and design. Furthermore, it is still unknown whether the hand rehabilitation therapy that excludes the rest of the limb may offer more advantages than strategies based on the whole arm movements.
Several studies have emphasized the application of robotics to rehabilitation training, highlighting the benefits obtained by robot-assisted therapy. Nevertheless, the obtained results are still fragmented and have not shown a complete consensus due to the heterogeneity of the robotic devices and the diversity of patients’ characteristics.
One of the most critical limits is the design of the robotic device. Tables 1 and 2 present a number of devices, underlining the complexity of the design (DOF, transmission, actuation). The design complexity may make unconvincing robot for the patients and clinicians, although it may seem effective in performing the therapy tasks.
A number of studies present experimental results that are promising to improve the impairment level of the patient. However, the evaluation methods often differ from each other, making it difficult to define which design is better and more effective than the other one. 90 Only a limited part of researches have shown the evaluation of the robotic device efficacy combining in the clinical methods. For example, the use of principle of evidence-based medicine (EBM) based on the improvement of the clinical scale may be a structured method to demonstrate the capacity of robot-assisted therapy. In particular, Kwakkel et al. 12 have highlighted that the application of EBM method has underlined the weak demonstration of the robotic device usefulness although the independent researchers showed promising results. This point pushes to define more standard randomized controlled trials and blinding procedures in robot-assisted therapy assessment.
All evaluated studies underline that the robotic devices may be complement to labor-intensive interactions between therapist and stroke subjects, as they can provide high-intensity, repetitive, adaptable, and task-specific treatment of the impaired limb. In particular, a number of robots can use VR environments, or other types of feedback, to offer challenging and motivating training, although this technology should not replace the therapists, but should come hand in hand and complement each other to increase the therapy efficacy. 91 In fact, although the literature has demonstrated the main advantages and benefits of robot applications, further studies involving a large size of patients are required to demonstrate results beyond what is achieved conventional methods.
The methods to evaluate the device performance need to be applied rigorously in order to measure the expected changes during the training sessions. In particular, a further open point to be investigated is the dosage of the robot-assisted therapy. The intensity, duration of rehabilitation therapy, and the patients’ diagnosis (acute, subacute, or chronic) are critical elements that may impact the final efficacy of the rehabilitation. In this way, it is required to investigate in more detail whether the obtained results can be maintained in the long-term and how they are transformed to perform the daily activity tasks. These information may help engineers and clinicians to develop more effective devices and understand weaknesses and opportunities of the existing robots. The state of art also highlights a low number of patients (5%–10%) that have access to these technologies. This number is worrying. Researches on rehabilitation robots need to become strategic and priority for the society. In fact, the costs of excluding people with disabilities by community are higher than the costs of development and delivering robot therapy. Unfortunately, this element is only evaluated as the ratio between the price and the performance of a robotics device in terms of benefits for patients and clinics.
This article reviewed a number of devices developed using either end-effector or exoskeleton approach. Current robotic systems, in particular end-effector devices, focus mostly on supporting passive or assisted movement therapy to the proximal joints, neglecting the distal joints and haptic aspects of object manipulation. The obtained results from clinical tests have shown positive and promising achievements; nevertheless, there are still issues and constraints to improve the device ability in providing dynamic interaction simulating variable mechanical object properties. In this way, the literature shows a reduction of papers published on the end-effector concept in the last years (Scopus source), in favor of studies on exoskeleton devices. Experimental results show that distal training seems to be beneficial for the recovery of the whole upper limb, while the training and recovery of proximal joints seem to transfer only limited benefits to the distal components. From this point of view, the exoskeleton approach offers new opportunities and challenges. Nevertheless, the exoskeleton design requires a deep knowledge in physical human–robot interaction, biomechanics, rehabilitation, actuators, sensors, and control. The main scope is to design effective, lightweight, and portable robotic devices for hand rehabilitation. In particular, these devices should implement novel training methods that adapt quickly to changes in patient performance. As discussed in the previous section, there are many open challenges on hand device design related to a number of technical features (e.g. weight, active DOF, peak of force, actuators, transmission, sensors). Future developments for patient treatment should consider the portability in a rehabilitation device to increase applications. However, most of the reported hand exoskeleton rehabilitation devices, with very few exceptions, lack portability. Moreover, VR may be incorporated to do more realistic task-based exercises. The proposed classification and comparison underline how the researches are moving toward innovative solutions.
Conclusion
The main scope of this review was to explore the main technologies for hand rehabilitation. The article focused on mechanical design, training paradigms, and usability since these parts are interconnected for an effective hand recovery. Furthermore, future development for patient treatment may include the device portability to increase the potential application. A part of the reviewed devices is already commercially available demonstrating the high interest of community. The review highlighted a lack of robust methods to demonstrate the efficacy of robot-assisted therapy. Although independent researchers have shown successful results, it is still complex to identify which design is better and more effective than other one. For this reason, the effectiveness of the robotic devices has not been demonstrated completely. Further studies involving a large size of patients are required to confirm whether robot-assisted therapy allows to obtain better clinical outcome than conventional therapy, even if robots will never replace therapists. In particular, these studies need to select an appropriate patient population to allow comparisons across studies and apply blinding procedures, which may result in a positive bias in the reported effects. At the moment, it is noted that number of patients that may access to robotic-assisted therapy is very low, 5%–10% of the total stroke population. Robotics needs to be considered strategic by community because the costs of excluding people with disabilities are higher than the costs of development and delivering robot therapy. Only a limited part of the proposed devices by the literature have been clinically tested, highlighting as the design complexity and development costs may negatively impact the system implementation. The design complexity may make unconvincing robot for the patients and clinicians, although it may seem effective in performing the therapy tasks.
The main technologies adopted for the device development are end-effectors and exoskeleton devices. The end-effector robots show more clinical tests that exoskeleton devices; nevertheless, the results are often partial and do not demonstrate completely the effectiveness of the device. In this way, more standardized robot-assisted assessment are required in order to compare the obtained results with the conventional methods. An end-effector robot is in more flexible than an exoskeleton device in fitting the different size of hands, reducing the setup time and increasing the usability for new patients. In addition, end-effector mechanisms are also generally ambidextrous. As demonstrated, end-effector devices often neglect the control of distal joints and haptic aspects of object manipulation. Tests showed distal training seems to be beneficial for the recovery of the whole upper limb. In this way, exoskeleton may be a new opportunity to be investigated deeply. The exoskeleton design is more complex than end-effector devices and is required a deep knowledge in hand biomechanics, rehabilitation, control, and human–robot interaction. However, their outcomes are promising and they represent the new opportunity. There are many open challenges related to a number of technical features (e.g. weight, active DOF, peak of force, actuators, transmission, sensors). In particular, the robotic system needs to be portable for home and personal use. The review of literature highlighted several research directions and unexploited opportunities for rehabilitation robotic devices that require further investigations.
Footnotes
Handling Editor: Davood Younesian
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.